


Introduction
In the event of a large-scale disaster resulting in a large number of sick and wounded people at health care facilities, and in particular, at disaster base hospitals that are expected to play a key role in the most acute phase of a disaster event, it is vital that hospital functions, or business continuity, of the disaster base hospitals are maintained, even immediately following a disaster.Reference Schultz, Koenig and Lewis 1 - Reference Kudo, Furukawa and Nakagawa 3 In the case of the Great East Japan Earthquake of March 11, 2011, water supply systems, and other critical social infrastructure, were disrupted over a wide area around the disaster zone. In Miyagi Prefecture (Japan), up to 22,362 households had their water service interrupted, 4 and a number of prefectural medical facilities were also adversely affected. 5
There have been several studies on disruptions and damage to water supply systems of hospitals in the event of disasters,Reference Ukai 2 , 6 , Reference Kobayashi, Uda and Yamashita 7 but there have been very few studies that examine both facilities and operation.Reference Kobayashi, Uda and Yamashita 7 In this study, damage and disruption to water supply facilities and operation of water resources at Miyagi Prefectural disaster base hospitals at the time of the Great East Japan Earthquake were investigated, with the general aim of examining the issue of operational continuity of hospitals in the event of a disaster.
Methods
In this study, as part of a series of surveys of all secondary and tertiary medical institutions in Miyagi Prefecture (72 facilities) regarding accidental hypothermia at the time of the Great East Japan Earthquake (including: (1) a survey regarding the incidence of accidental hypothermia; (2) a survey regarding means of information and communication; and (3) a survey on heating in hospitals), with permission of the Medical Research Ethics Committee of the Faculty of Medicine of Tohoku University (Sendai, Japan), a written survey of the disaster medical centers located within the jurisdiction of the Miyagi Disaster Management Headquarters, and the 14 medical facilities, was conducted on the two items below.Reference Kudo, Furukawa and Nakagawa 3 In Miyagi Prefecture, a total of 14 medical facilities are designated as disaster base hospitals.
First, an analysis of the event chronology at the 14 disaster base hospitals and the disaster medical centers located within the jurisdiction of the Miyagi Disaster Management Headquarters, and a written survey of the 14 disaster base hospitals, were conducted.
The survey questions concerned the disruption and restoration of water facilities at each hospital, as well as the supply and operation of water resources. On the disruption and restoration of water supply facilities, inquiries were made about the main configuration of water piping, pumps, elevated water tanks, and hospital plumbing that make up the water supply facility (Figure 1); on the supply and operation of water resources, inquiries were made about whether or not water supply services from water utilities were interrupted, how many days it took for water service to be restored (in case it was interrupted), and about the quantity of water used under normal conditions and during an earthquake disaster. Note that buildings not directly used for medical treatment, such as staff dormitories and research blocks, were excluded from the current investigation. Assessment of water quantities used for different purposes under normal conditions was also examined, and whether or not any plans were formulated to allocate available water strategically in the event of an emergency.
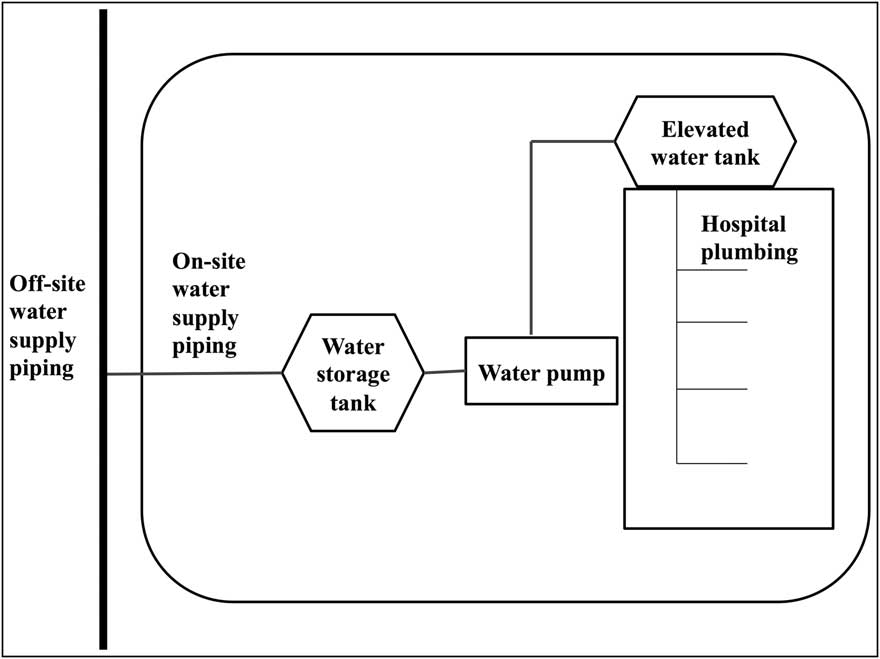
Figure 1 General Water Supply System of a Hospital. A water-storage-tank-style water supply facility is composed of water supply piping, water storage tank, water pump, elevated water tank, and hospital plumbing.
Second, a detailed interview survey on medical treatment work impacted by water supply disruptions was also conducted.
A survey of Tohoku University Hospital (Sendai, Japan) regarding water usage applications under normal conditions found that the greatest consumption of water—as far as can be determined—is for bathing (24%), followed, in order, by meal services, dialysis, and sterilization (which together account for approximately 13% of consumption). Consumption for applications other than meal services—that is, for different kinds of sanitation-related use, including lavatories and toilets—is difficult to determine. In fact, including these applications, the specific use of a full 62% of water consumed cannot be determined.
Interview surveys of representatives at each hospital were also conducted on a total of five items—the four activities for which consumption was highest in the survey mentioned above (dialysis, sterilization, sanitation, and meal services), plus outpatient care, which is an essential requirement for a disaster base hospital. The impact on each activity of water supply interruption and water system damage was ranked using one of three levels: (A) 100% (operation as usual); (B) partial operation; and (C) 0% (no operation possible).
Results
Disruption and Restoration of Water Supply Facilities
Damage or disruption to water supply facilities was confirmed at 14 locations (seven hospitals). Table 1 shows the number of damage points and the number of days needed to restore service for different structures. For nine points of damage (four hospitals), 30 or more days were needed to restore service, with a maximum value of 133 days.
Table 1 Damage to Water Supply Facility and Number of Days for Recovery

This table shows the number of points of damage for each part of the water supply facility as well as the range in values of the number of days needed to restore operation. There was a total of 14 points of damage at seven hospitals that suffered damage. Two points needed less than 10 days for water supply restoration, two points needed 10 to 30 days, and nine points needed 30 days or more.
State of Water Resource Supply and Operation
In relation to the supply of water resources, water supply was interrupted to nine out of 14 hospitals following the disaster, with a median value of three days (range = one to 20 days) for service to be restored (Figure 2). For the nine hospitals that experienced water supply interruptions, the volume of water supplied per day under normal conditions was compared with the water volume supplied in the wake of the Great East Japan Earthquake (Figure 3). At hospitals where water supply was interrupted, the main water supply source was fed with an emergency supply of water, transported by truck; however, at Hospitals A, B, and C, where the available water supply service amounted to less than 10 m3 per day, due to insufficient emergency water supply, the only available water supply after the disaster was the water remaining in water storage tanks and elevated water tanks. Hospitals D, E, F, and G, which had well water supply facilities, were able to obtain water from their wells after the disaster, and apart from Hospital D, which did not make any detailed records, the volume of water supplied from the well was quite comparable to the volume supplied under normal operating conditions.
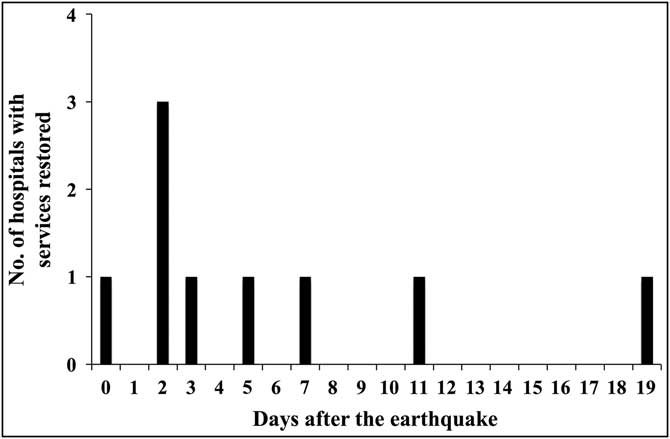
Figure 2 Trend in Recovery from Water Supply Interruption. Median value for number of days for recovery was three, with a minimum of one day and a maximum of 20 days.
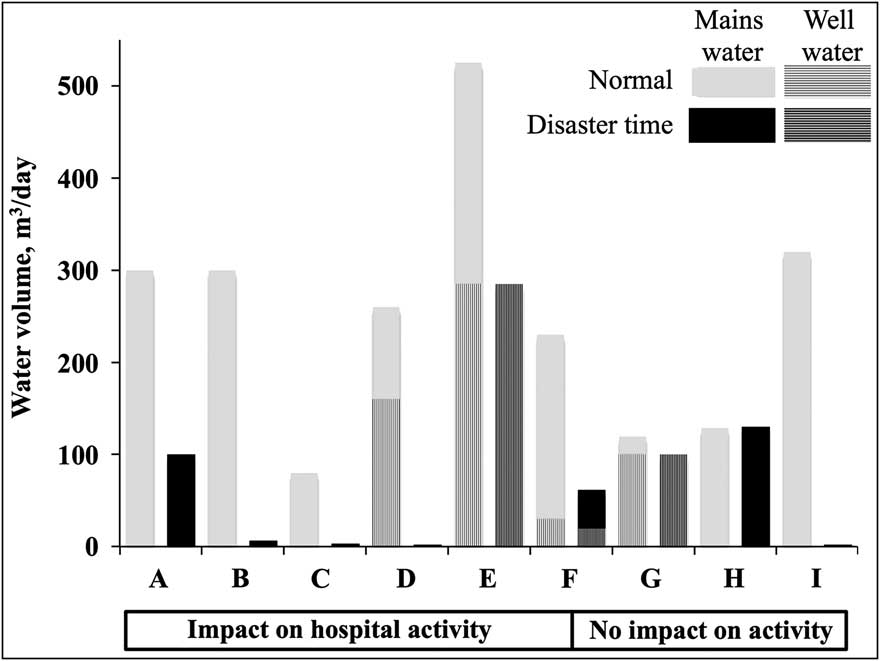
Figure 3 Water Volume by Water Source During Normal Operation and Water Supply Interruption. Left: water volume by water source in normal operation. Right: water volume by water source during water supply interruption. At hospitals where medical care activities were impacted, total water volume was greatly reduced. At Hospital I, water service was recovered on the same day as the disaster. The water supply was greatly reduced, but there was hardly any change in the volume of well water. There was no data on well water for Hospital D.
At the six hospitals that responded that their medical care activities were impacted, total available water was reduced. On the other hand, at the three hospitals that reported no impact to their medical care activities, Hospital I was able to restore water service on the day of the disaster, while Hospitals G and H managed to maintain approximately the same level of water as normal, by accessing well water and through frequent deliveries of emergency water.
The relationship between whether or not there was a water service interruption and whether there was any damage to water supply facilities, and the impact on medical care activities that require large amounts of water, was tabulated, as described above (Table 2). Of the facilities that responded that their medical care activity was impacted, all except Hospital E experienced damage to their water supply facilities. Dialysis was disrupted at three hospitals; meal services were disrupted at five hospitals; sterilization was disrupted at two hospitals; and outpatient care was disrupted at three hospitals. Two hospitals answered “C” (0%: no operation possible) for one or more types of activity, and both of these experienced massive damage to water supply facilities within the hospital. At Hospital J, the elevated water tank on the roof of the building was destroyed, making water distribution difficult and causing a deterioration of sanitation conditions; at Hospital D, outpatient care and continuity of medical care within the hospital were difficult due to the damage to the hospital's plumbing. For these reasons, both of these hospitals had to evacuate inpatients.
Table 2 Impact on Medical Care Activities of Damage to Facility and Water Supply Interruption
Including: (A) no impact; (B) partial impact; and (C) no operation possible. If B or C was the answer for even one item, medical care had been impacted. Whether or not there was an impact is more closely correlated with facility damage than whether or not water supply was interrupted.
In terms of water resource operations, none of the hospitals had ascertained how much water they used for different purposes under normal conditions, and none had formulated a plan for strategic water allocation in the event of a disaster.
Discussion
In this study, the importance of not only ensuring a reliable water supply, including emergency water supply and well water, but also preventing the decline of hospital functionality by properly maintaining water supply facilities, was demonstrated. In addition, it took, on average, about three days for interrupted water supply services to be restored, whereas it took an average of 52 days to repair damaged water supply facilities. This suggests that the impact on medical care activities can be potentially very long lasting.
Since the Great East Japan Earthquake, the Ministry of Health, Labour, and Welfare has taken initiatives to enhance the earthquake-resistance of disaster base hospitals, and as of 2012, a full 73.0% of disaster base hospitals and critical care centers were earthquake-proof;Reference Takei, Ikeuchi, Tokuno, Yamada and Ukai 8 however, this figure is still not high enough. Until water supply services can be restored fully, it is necessary to obtain emergency water supplies from external sources (eg, deliveries by water trucks). In view of this, it is necessary to take precautionary countermeasures, such as: earthquake-proofing the whole series of structures, from the water storage tank used, to store supplied water, to the internal water piping of the hospital; setting up a water distribution system that does not include an elevated storage tank, which uses water pumps, and is not easily affected by an earthquake, by adopting a direct water supply system that utilizes a pressurized water supply pump; or installing multiple water piping circuits within the hospital.Reference Kobayashi, Uda and Yamashita 7 The current survey showed that well water is able to provide almost the same amount of water as during normal operation, proving that wells are an effective source of water in the event of an emergency. Securing a well water supply facility is incorporated into the requirements of disaster base hospitals and it should be given a high priority as a disaster countermeasure. At the same time, this survey showed that regardless of whether well water supplies the same volume of water as the normal water supply service, the risk that the quality of groundwater is changed by an earthquake means that some hospitals may not be able to use well water until the water quality has been checked. Therefore, instead of just diversifying water supply options, it is also important to properly maintain water supply facilities and devise effective countermeasures to the risks posed by disasters.
The results of this survey show that it is desirable to conclude water supply agreements and to formulate water allocation plans in anticipation of the possibility of water supply interruptions that last for a long time. The results of a study by Kudo et al that examined the requests for supply of materials from disaster base hospitals to the Miyagi Medical Headquarters during four days from March 11 (the day of the disaster) to 14, 2011, and the frequency of inquiries on the progress after requests, showed that multiple hospitals made inquiries aimed at securing water supplies.Reference Kudo, Furukawa and Nakagawa 3 The disaster base hospitals surveyed in this study use approximately 50 m3 to 300 m3 of water per day, but since water delivery trucks can only deliver three to four m3 of water at a time, it is not realistic to expect that, in a disaster, it will be possible to obtain the same amount of water as under normal conditions by receiving numerous deliveries of water each day. For this reason, it is necessary to determine the minimum volume of water necessary to carry out essential hospital activities. Each base hospital needs to determine clearly the activities that it must perform in the event of an emergency and the minimum quantities of water required for each activity. Based on this, the hospital then needs to format a detailed plan for allocation of water. It is also important to know the total amount of water that can be stockpiled at the hospital. When the normal water supply is interrupted, the water remaining in the water storage tanks plays an important role until emergency supplies of water can be obtained. Some hospitals have installed large water storage tanks after an earthquake to ensure a large volume of water, as a disaster countermeasure; 9 however, according to a survey conducted in 2011 by the Ministry of Health, Labour, and Welfare, the water storage capacity at disaster base hospitals around Japan was most typically just half a day or one day of normal usage, with 42.3% of all surveyed hospitals having this amount of reserves.Reference Yutani and Nakatani 10 It would be difficult to immediately adopt high-capacity water storage tanks at all disaster base hospitals, so it is more important to devise a clear water allocation plan, and to be able to judge the necessary timing of emergency water delivery requests based on total storage capacity and usage volume.
Many private businesses formulate a business continuity plan (BCP) in preparation for a disaster or other unexpected occurrence, in order to decide in advance the methods and means to be used to ensure a quick recovery with minimal disruption to business activities. Originally, BCPs were used principally in specific sectors, like manufacturing and finance, but they have become increasingly widespread in a wide variety of industries, including government and public agencies, and regional and local public bodies. However, the number of medical facilities that have formulated BCPs is relatively small, so it cannot be said that the concept of BCPs is penetrating medical service providers. 11 Since the Great East Japan Earthquake, though, the importance of formulating a BCP is being recognized by medical institutions, and the public demand for BCPs for disaster base hospitals is growing. 12 , Reference Nakagawa, Furukawa and Abe 13 In formulating a BCP for a disaster base hospital, the designated requirements of a disaster base hospital issued by the Ministry of Health, Labour, and Welfare are defined by a single indicator; however, based on the lessons of major earthquakes, these designated requirements are modified,Reference Nakagawa, Furukawa and Kudo 14 and with regard to water supply facilities, these are: “possession of water storage tanks of suitable capacity, the provision of well water supply facilities that can be used when electric power is cut off, and ensuring a supply of water necessary for medical care in the event of a disaster by the conclusion of preferential water supply agreements.” 15 The results of this study back up these requirements.
Limitations
First, this study was based on survey results obtained from disaster base hospitals, and each hospital referred to data elicited from process records (event chronologies), reports, and other materials at the time of the Great East Japan Earthquake. Consequently, these data may not be exhaustive, owing to confusion at the time of disaster. Second, medical care activities (dialysis, sterilization, sanitation, meal services, and outpatient care) impacted by water supply disruptions were examined in the current study, but it is difficult to prove actual or perceived harm to patients because a control group did not exist in the same hospitals in the event of the disaster. Finally, it is also difficult to quantify the impact on each medical care activity of water supply interruption and water system damage, thus, it was assessed by ranking scale using one of three levels: (A) 100% (operation as usual); (B) partial operation; and (C) 0% (no operation possible).
Conclusion
Through the proper maintenance of water supply facilities and securing alternative sources of water, such as well water, it is possible to minimize the disruption or reduction of hospital functions in the event of a disaster. At the same time, to address the risk of long-term water service disruption, it is desirable to conclude water supply agreements and to formulate water allocation plans.
Acknowledgements
The chronology of events was collected from Miyagi Prefecture's Department of Medical Development, and the 14 disaster base hospitals in Miyagi (Sendai Medical Center, Katta General Hospital, South Miyagi Medical Center, Sendai City Hospital, Tohoku University Hospital, Sendai Red Cross Hospital, Tohoku Rosai Hospital, Tohoku Pharmaceutical University Hospital, Saka General Hospital, Osaki Citizen Hospital, Kurihara Central Hospital, Tome Citizen Hospital, Ishinomaki Red Cross Hospital, and Kesen-numa City Hospital.) Valuable comments were given by Masayuki Kobayashi, head of the Facility Planning Office, as well as Yayoi Okano and other neurosurgery research administrators.





