



Familial Mediterranean fever is an inherited autoinflammatory disease that presents as recurring episodes of serositis of the peritoneum, pleura, synovium, and, in rare cases, the pericardium. It is characterised by clinical, laboratory, and histological evidence of localised and systemic inflammation.Reference Heller, Sohar and Sherf1 The disease is caused by a mutation in the Mediterranean fever gene.Reference Bernot, Clepet and Dasilva2–4 Colchicine is the main therapy that produces complete remission or a marked reduction in the frequency and duration of attacks in most patients.
Cardiovascular disease is a major cause of morbidity and mortality in most autoimmune diseases. However, cardiovascular involvement is uncommon in familial Mediterranean fever.Reference Knockaert5 Familial Mediterranean fever is characterised as progressing with inflammation in the attack-free period as well as during an acute attack.Reference Livneh, Langevitz and Zemer6,Reference Ben-Chetrit and Levy7 Chronic inflammation can affect the cardiovascular system by causing endothelial dysfunction. Recurrent inflammatory processes during the attacks and the potential chronic persistent subclinical inflammation among attack intervals in familial Mediterranean fever patients may lead to endothelial dysfunction, which is attributed to arteriosclerosis. Inflammation increases arterial stiffness. As a result of inflammation, cytokines increase in circulation. Increased circulating inflammatory mediators (tumor necrosis factor-alpha, interleukin-2 receptor, interleukin-1b, interleukin-6, interleukin-8, and interleukin-12) impair collagen and elastin in the aortic intima. Decreased elastin causes increased arterial stiffness.Reference Colak, Gurlek and Yegin8,Reference Gang Gang, Drenth and Langevitz9 The aortic stiffness reflects aortic elasticity. Aortic elasticity is closely associated with cardiovascular mortality. Although pericarditis is a common cardiac manifestation of familial Mediterranean fever, few studies have reported arrhythmia, atherosclerosis, ventricular dysfunctions, decreased heart rate variability, and abnormalities in aortic elasticity.Reference Baysal, Peru and Oran10–Reference Tavil, Öztürk and Üreten13 We aimed to evaluate possible cardiac involvement in children with familial Mediterranean fever during the attack-free period using electrocardiography and conventional and tissue Doppler echocardiography. Additionally, we evaluated the aortic stiffness index and time-domain heart rate variability.
Methods
Patients/participants
A single-centre, prospective study included 75 children (39 girls) with familial Mediterranean fever, and 50 healthy controls (25 girls) recruited from the outpatient clinic at Pamukkale University Faculty of Medicine. The diagnosis of familial Mediterranean fever was based on the Tel Hashomer criteria.Reference Livneh, Langevitz and Zemer6 The control group consisted of 50 healthy volunteers who were age- and sex matched with the study group.
Patients with obesity, diabetes mellitus, thyroid dysfunction, hypertension, arrhythmia, infectious disease, electrolyte imbalance, chronic renal failure, hyperlipidaemia, chronic liver disease, malignancy, congenital, or acquired heart disease, cardiomyopathy, and amyloidosis were excluded. Patients who were currently experiencing an attack period or receiving drugs that could influence the cardiac autonomic nervous system, such as antipsychotics, antidepressants, and antihistaminics, were excluded from the study. All familial Mediterranean fever patients were using regular colchicine therapy. Clinical and laboratory assessments of the patients were performed during the attack-free period and at least three weeks after the attack. The healthy controls consisted of outpatients who applied for innocent murmur, presyncope, and chest pain, but did not detect cardiologic pathology.
We recorded the epidemiological data, clinical symptoms, date of diagnosis, age at onset, age at diagnosis, family history, disease duration, clinical phenotype, attack duration and frequency, treatment duration, response to treatment, and genetic analysis of Mediterranean fever gene mutations in familial Mediterranean fever patients. Patients with familial Mediterranean fever were evaluated by dividing them into two groups according to the presence (or absence) of the M694V mutation.
Anthropometric parameters were evaluated in all patients. Body mass index was calculated as defined previously.Reference Cole, Flegal and Nicholls14 Hemogram and biochemical parameters including serum electrolytes, C-reactive protein, fibrinogen, erythrocyte sedimentation rate, triglyceride, total cholesterol, high-density lipoprotein, and low-density lipoprotein values were evaluated in the study and control groups. All subjects rested in the supine position for 15 minutes, and then their right brachial artery pressure was measured by a sphygmomanometer with the appropriate cuff. Both systolic (Ps) and diastolic blood pressure (Pd) were measured. All the patients and control subjects performed electrocardiography, conventional, and tissue Doppler echocardiography. Twenty-four-hour Holter recordings were obtained for all subjects. All data were evaluated by the same paediatric cardiologist.
This study was approved by the local ethics committee and fulfilled the ethical guidelines of the most recent Helsinki Declaration. All parents of the children gave written informed consent.
Electrocardiography
Standard resting 12-lead electrocardiogram was recorded at 25 mm/s paper speed. Heart rate was calculated from the R-R interval of the tracings. QT intervals were measured manually in a blinded fashion from the onset of the QRS complex to the end of the T wave on the iso-electric line by the same physician. For each lead, three consecutive QT intervals were measured and averaged. The QT dispersion was defined as the difference between the maximum and minimum QT intervals in one ECG record. The QT interval was corrected using the heart rate according to the Bazett’s formula (QTc=QT√RR),Reference Bazett15 and the QTc dispersion was calculated.
Echocardiography
All patients and members of the control group underwent 2D, M-mode, Doppler, and the tissue Doppler echocardiography ultrasounds using a Vivid 7 model echocardiography and multifrequency transducer (2.5–4 MHz; GE Vingmed Company, Horten, Norway). All subjects were rested and lying in the lateral decubitus position during the examinations. The means of three consecutive measurements were recorded. M-mode measurements were made at the level of the tips of the mitral valve leaflets in the parasternal long-axis view of the left ventricle.Reference Sahn, DeMaria, Kisslo and Weyman16 The standard parameters measured in the parasternal long axis by M-mode echocardiography were LV posterior wall end-diastolic thickness, left ventricular end-diastolic dimension, and interventricular septum end-diastolic thickness. LV ejection fractions and shortening fractions were calculated as defined previously.Reference Silverman and Silverman17 Left ventricular mass and left ventricular mass index were calculated using the following standard formulas:Reference de Simone, Daniels and Devereux18,Reference Devereux and Reichek19 LVM = [0.8 X1.04 ((LVEDD + IVSTd+LVPWTd)3-(LVEDD3)) + 0.6] and LVMI = LVM divided by height to the 2.7 power. Relative wall thickness was calculated using the formula:Reference Devereux and Reichek19 RWT = (IVSTd + LVPWTd)/LVEDD. Conventional Doppler blood velocities were measured for mitral and tricuspid valves using an apical four-chamber view (peak E and A waves), and the E/A ratio was determined.
Tissue Doppler echocardiography
Tissue Doppler echocardiography mode of the same machine was used by lowering the velocity range (0–30 cm/s) to determine myocardial velocities and setting the Doppler gain to achieve maximum colour information on the myocardium. Pulsed-wave tissue Doppler echocardiography was used to record myocardial contraction velocities (S), early and late relaxation velocities (Ed and Ad, respectively) in basal portions of the LV (at the level of the lateral mitral annulus), right ventricle (RV) (at the level of the lateral tricuspid annulus), and interventricular septum in the apical four-chamber view. The ratio of peak velocities in early and late relaxation (Ed/Ad) was determined for the assessment of diastolic function.
Elastic properties of the aorta
A long-axis view of the abdominal aorta of the subxiphoid area was recorded, and the maximum systolic (Ds) and minimum diastolic diameter (Dd) were measured by M-mode echocardiography. Aortic strain (S) was calculated using the changes in aortic diameters, and pressure strain elastic modules were calculated from the aortic strain and the changes in artery systolic and diastolic pressure using the formulas S = (Ds-Dd)/Dd and Ep = (Ps-Pd)/S. Pressure strain normalised (Ep*) by diastolic pressure was calculated using the following equation: Ep* = Ep/Pd. Aortic distensibility (DIS) and aortic stiffness β index (β SI) were calculated according to the previously proposed and evaluated equations as DIS = [2(Ds-Dd)/Dd(Ps-Pd)]x10−6 cm2dyne−1 and SI = ln(Ps/Pd)/[(Ds-Dd)/Dd].Reference Lage and Kopel20–Reference Lacombe, Dart and Dewar22 S and DIS represent the distensibility or elasticity of the aortic wall; Ep, Ep*, and β SI represent the stiffness of the aortic wall. Ep and Ep* are the mean stiffness of the aorta.
Twenty-four-hour ambulatory Holter monitoring
Patients and controls underwent 24-hour ambulatory Holter monitoring. Continuous ambulatory ECG monitoring was recorded using the Cardioline Walk400h Holter software Cardioline® version 1.2 for Windows. The recordings consisted of three lead configurations of electrocardiographic data. Twenty-four-hour mean RR (mean of all filtered RR intervals over the length of the analysis) and nighttime mean RR (mean of all filtered RR intervals for 5 consecutive hours during quiet sleep) were calculated. Heart rate variability was analysed using time domain indices from the Holter tapes. The following five measures23 were examined:
SDDNN: Standard deviation of all filtered RR intervals in the entire 24-hour ECG recording,
SDNN-i: Mean of the standard deviations of all filtered RR intervals for all 5-min segments of the analysis,
SDANN-i: Standard deviation of the means of all filtered RR intervals for all 5-min segments of the analysis,
RMSSD: Square root of the mean of the sum of squares of differences between adjacent filtered RR intervals over the length of the analysis,
PNN50: Percentage of differences between adjacent filtered RR intervals greater than 50 ms for the whole analysis.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 21, Inc., Chicago, IL, USA). The distribution of continuous variables was performed using the Shapiro–Wilk test. Statistical analyses included chi-square for categorised data, student t-test for parametric data, and Mann–Whitney U and Kruskal–Wallis for nonparametric data. Statistical significance was considered at p-values less than 0.05. All data were expressed as the mean and standard deviation or medians (interquartile range) for continuous variables, and categorical variables were expressed as percentages, depending on the normality distribution.
Results
The study group consisted of 75 children with familial Mediterranean fever and 50 healthy controls. The mean age was 9.8 ± 3.8 years, and 36 (48%) participants were boy in the familial Mediterranean fever group. The control group had a mean age of 9.3 ± 3.8 years, and there were 25 (50%) boys. There was no significant difference between the familial Mediterranean fever and control groups in sex, age, blood pressure, or BMI (p > 0.05). The demographic characteristics of the baseline study population are shown in Table 1.
Table 1. Demographic and clinical characteristics in the study and control groups

SD = Standard deviation; BSA = Body surface area; BMI = Body mass index; BP = blood pressure; FMF = Familial Mediterranean fever.
The mean age at diagnosis of the children with familial Mediterranean fever was 7 ± 3.6 years. The time elapsed from the onset of symptoms to diagnosis was 1.44 ± 1.35 years. The mean duration of the disease was 2.9 ± 2.5 years (0.5–12.5) (Table 1). Of the patients, 40 (53.3%) had family histories of familial Mediterranean fever.
An Mediterranean fever gene mutation was detected in at least one allele in 70 (98.5%) of the 71 patients with known mutations. Thirty-one (44.4%) variants were reported as homozygous, 25 (35.7%) as compound heterozygous, and only 14 (20%) as heterozygous. M694V was the most common homozygous variant (n: 38, 53.5%).
The hemogram results, biochemical parameters, and lipid profiles were the same in the study and control groups, except for the erythrocyte sedimentation rate levels (p > 0.05) (Table 2). Although the erythrocyte sedimentation rate was within normal values, the mean erythrocyte sedimentation rate levels were higher in the familial Mediterranean fever group than in the control group (p = 0.03, Table 2).
Table 2. Laboratory characteristics in the study and control groups
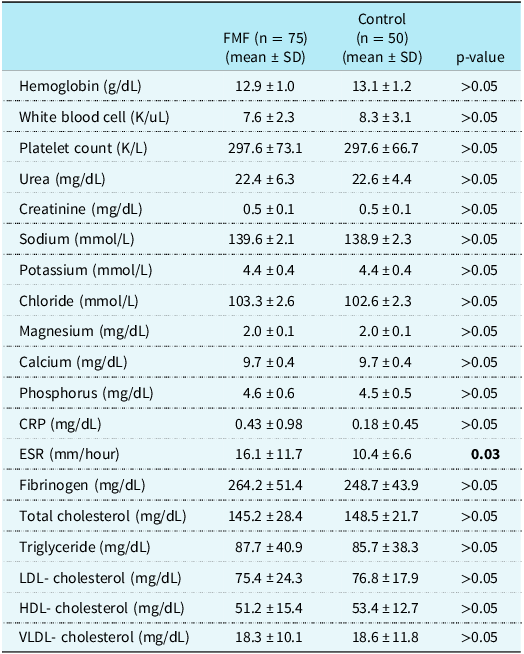
CRP = C reactive protein; ESR = erythrocyte sedimentation rate; FMF = Familial Mediterranean fever; HDL = high-density lipoprotein; LDL = low-density lipoprotein; VLDL = very-low-density lipoprotein; SD = Standard deviation.
Turning to the evaluation of ECG parameters, the mean QTd and cQTd were longer in the children with familial Mediterranean fever than in the control group, although there were no significant differences between the groups (p > 0.05). Table 3 shows the QT and cQT parameters of the groups.
Table 3. QT and QTc parameters in the study and control groups

cQT = Corrected QT; QTd = QT interval dispersion; cQTd = corrected QT dispersion; min = minimum; max = maximum; SD = Standard deviation; FMF = Familial Mediterranean fever.
When the echocardiographic parameters of the familial Mediterranean fever and control groups were compared, we detected that LVPWTd, LVd, IVSTd, LVs, LV-EF, LV-FS, LVM, LVMI, and RWT were similar in the groups. No significant difference in these parameters was found between the groups (p > 0.05, Table 4).
Table 4. Echocardiographic parameters in the study and control groups

LVPWTd = Left ventricular posterior wall end-diastolic thickness; LVd = left ventricular end-diastolic dimension; IVSTd = interventricular septum thickness diastolic; LVs = left ventricular end-systolic dimension; LA = left atrium; AA = aortic annulus; LVM = left ventricle mass; LVMI = left ventricle mass index; RWT = relative wall thickness; EF ejection fraction; FS fractional shortening; FMF = Familial Mediterranean fever; SD = Standard deviation.
In the comparison of conventional Doppler echocardiographic parameters between the familial Mediterranean fever and control groups, the peak mitral E wave velocity and mitral and tricuspid E/A ratios were lower in the familial Mediterranean fever group, whereas the peak mitral and tricuspid A wave velocities were higher in the familial Mediterranean fever group than in the healthy controls (p < 0.05) (Table 5).
Table 5. Conventional Doppler echocardiographic parameters in the study and control groups

E = peak early diastolic velocity; A = peak late diastolic velocity; IVRT = isovolumetric relaxation time; DT = deceleration time; MPI = myocardial performance index; RT = relaxation time; E′:peak early diastolic tissue Doppler velocity; S′ = peak systolic tissue Doppler velocity; A′ = peak late diastolic tissue Doppler velocity; cm/s = centimeter per second; ms = millisecond; FMF = Familial Mediterranean fever; SD = Standard deviation.
When the tissue Doppler echocardiographic parameters were evaluated, the Sd, Ed, and Ed/Ad of both ventricles were lower in the familial Mediterranean fever group than in the controls, whereas the Ad of both the ventricles and interventricular septum was higher in the familial Mediterranean fever group than in the control group (p < 0.05). The tissue Doppler echocardiographic parameters are presented in Table 6.
Table 6. The tissue Doppler echocardiographic parameters in the study and control groups

Adivs = peak atrial contraction velocity for the interventricular septum; Adm = peak atrial contraction velocity for the left ventricle; Adt = peak atrial contraction velocity for the right ventricle; Edivs = peak early relaxation velocity for the interventricular septum; Edm = peak early relaxation velocity for the left ventricle; Edt = peak early relaxation velocity for the right ventricle; Eivs = peak early mitral inflow velocity; Sdivs = peak systolic velocity for the interventricular septum; Sdm5peak systolic velocity for the left ventricle; Sdt = peak systolic velocity for the right ventricle; RTdt = relaxation time for the right ventricle; RTdivs = relaxation time for the interventricular septum; RTdm = relaxation time for the left ventricle. DTdt = Deceleration time for the right ventricle; DTdivs = Deceleration time for the interventricular septum; DTdm = Deceleration time for the left ventricle; MPIdt = myocardial performance index for the right ventricle. MPIdivs = myocardial performance index for the interventricular septum; MPIdm = myocardial performance index for the left ventricle.
While the aortic systolic and diastolic diameters were similar in the two groups (p > 0.05), the aortic strain and distensibility were lower in the study group than in the controls, and the Ep, Ep*, and aortic stiffness β index were higher in the study group (p < 0.05, Table 7).
Table 7. The aortic elasticity parameters in the study and control groups

SD = standard deviation; FMF = familial Mediterranean fever; Dd- aortic diameter in diastole; Ds - aortic diameter in systole; Ep = pressure strain elastic modulus; Ep* = pressure strain normalized by diastolic pressure; β SI - aortic stiffness β index.
The time-domain heart rate variability parameters were compared between the groups through 24-hour ambulatory Holter monitoring. There were no statistically significant differences in the maximal, minimal, or average RR intervals. SDNN-i, RMSSD, and pNN50 were significantly lower in the children with familial Mediterranean fever compared with the controls (p < 0.05). The other time-domain parameters, including SDNN and SDANN, were similar in the two groups (p > 0.05, Table 8).
Table 8. Time-domain HRV parameters in the study and control groups.

When familial Mediterranean fever patients with and without the M694V mutation were evaluated, the mean C-reactive rate and erythrocyte sedimentation rate were higher in patients with the M694V mutation than in patients without it (p < 0.05). Mean QT, QTd, and cQTd levels were higher in patients with the M694V mutation, but there were no significant differences (p > 0.05). There were also no significant differences in conventional or tissue Doppler echocardiographic parameters or 24-hour ambulatory Holter monitoring parameters between the familial Mediterranean fever children with and without M694V mutations. Aortic strain and distensibility were lower and Ep, Ep*, and aortic stiffness β index were higher in patients with M694V, although there were no statistically significant differences (p > 0.05, Table 9).
Table 9. Laboratory, electrocardiographic, conventional echocardiographic, tissue doppler echocardiographic, elastic properties of the aorta, and heart rate variability measurements in FMF patients with and without M649V mutation.

CRP = C reactive protein; ESR = erythrocyte sedimentation rate; cQT = Corrected QT; QTd = QT interval dispersion; cQTd = corrected QT dispersion; LVPWTd = Left ventricular posterior wall end diastolic thickness; IVSTd = interventricular septum thickness diastolic; LVd = left ventricular end-diastolic dimension; LVs = left ventricular end-systolic dimension; LA = left atrium; AA = aortic annulus; LVM = left ventricle mass; LVMI = left ventricle mass index; RWT = relative wall thickness; EF ejection fraction; FS fractional shortening; Adivs = peak atrial contraction velocity for the interventricular septum; Adm = peak atrial contraction velocity for the left ventricle; Adt = peak atrial contraction velocity for the right ventricle; Edivs:peak early relaxation velocity for the interventricular septum; Edm:peak early relaxation velocity for the left ventricle; Edt:peak early relaxation velocity for the right ventricle; Eivs = peak early mitral inflow velocity; Sdivs:peak systolic velocity for the interventricular septum; Sdm:peak systolic velocity for the left ventricle; Sdt:peak systolic velocity for the right ventricle; Ep = pressure strain elastic modulus; Ep* = pressure strain normalized by diastolic pressure; β SI = aortic stiffness β index.
Discussion
We showed that QT and corrected QT dispersion parameters were similar and the E wave velocity and the E/A ratio of the mitral and tricuspid valves, the Sd, the Ed, and Ed/Ad of both ventricles decreased, and the A wave velocity of the tricuspid valve, the Ad of both ventricles and the interventricular septum increased in familial Mediterranean fever patients. Aortic strain and distensibility were decreased, and Ep, Ep* by diastolic pressure, and the aortic stiffness β index were increased in the familial Mediterranean fever patients. SDNN-i, RMSSD, PNN50 significantly decreased in the familial Mediterranean fever patients, whereas SDNN and SDANN were similar in both groups in our study.
Familial Mediterranean fever is an autosomal recessive disease that is the most frequent autoinflammatory disorder and that is characterised by short, repeated, and self-limiting attacks of fever and serositis.Reference Onen24 Although familial Mediterranean fever has been observed in all age groups, it has been reported that symptoms usually begin at the age of 3–15 years.Reference Tavil, Öztürk and Üreten13 In recent years, studies have reported that increasingly younger children are being diagnosed with the disease.Reference Yalçinkaya, Özen and Özçakar25,Reference Ece, Çakmak and Uluca26 The mean age of diagnosis in children with familial Mediterranean fever was reported as 7.5 years by Yalcinkaya et al.Reference Yalçinkaya, Özen and Özçakar25 and 7.6 years by Ece et al.Reference Ece, Çakmak and Uluca26 In our study, the mean age at diagnosis was seven years, which is consistent with previous studies. We think that the reason for the decrease in the age of diagnosis of familial Mediterranean fever is that society and health professionals are becoming better informed about familial Mediterranean fever, and therefore the disease is being diagnosed at a younger age.
Acute phase reactants, including C-reactive protein, erythrocyte sedimentation rate, and fibrinogen, are known to be elevated during the acute phase of familial Mediterranean fever.Reference Cobankara and Kiraz27 The mean erythrocyte sedimentation rate was significantly higher in children with familial Mediterranean fever who were in the attack-free period compared to the control group in our study. The mean C-reactive protein, fibrinogen, and haemogram levels were similar in the two groups. The higher erythrocyte sedimentation rate detected in the attack-free period in our study also reinforces that inflammation continues even in the asymptomatic period in familial Mediterranean fever patients. Therefore, these patients are at risk for cardiovascular disease.Reference Knockaert5,Reference Cobankara and Kiraz27 We evaluated possible cardiac involvement in children with familial Mediterranean fever globally using electrocardiography, conventional and tissue Doppler echocardiography, and 24-hour ambulatory Holter monitoring during the attack-free period.
Prolonged QT dispersion indicates ventricular inhomogeneity. Although many studies have measured QT parameters in adult familial Mediterranean fever patients, only three have evaluated QT parameters in children with familial Mediterranean fever.Reference Caliskan, Gullu and Yilmaz11,Reference Canpolat, Dural and Aytemir12,Reference Farag, Sayed, Mostafa, Marzouk, Mohamed and Sobhy28–Reference Nussinovitch, Kaminer and Nussinovitch34 Studies of adults with familial Mediterranean fever have shown that QT parameters are similar in familial Mediterranean fever and control groups.Reference Topal, Tanindi and Kurtoglu32–Reference Nussinovitch, Kaminer and Nussinovitch34 However, two studies reported statistically higher values of ventricular polarisation parameters in adult familial Mediterranean fever patients.Reference Canpolat, Dural and Aytemir12,Reference Akcay, Acar and Sayarlioglu30 In the studies that evaluated paediatric familial Mediterranean fever patients, long QTc was found in only one study, conducted by Farag et al.Reference Farag, Sayed, Mostafa, Marzouk, Mohamed and Sobhy28 In contrast, KocaReference Koca, Kasapçopur and Bakari29 and Sahin et al.Reference Şahin, Kır and Makay31 showed that the QT dispersion parameters of the familial Mediterranean fever children and controls were similar. We also found longer QT dispersion parameters in children with familial Mediterranean fever, although the difference was not statistically significant. We speculate that the QT parameters of the groups in our study were similar because of the young mean age of the children, the short duration of the disease, and the minimal delay in diagnosis. Previous studies did not evaluate the relationship between the presence of the M694V mutation and QT parameters, while we evaluated QT parameters with and without the M694V mutation, finding that QT parameters were longer in the children with the M694V mutation but not significantly so.
Many studies have demonstrated the presence of diastolic dysfunction in patients with familial Mediterranean fever.Reference Baysal, Peru and Oran10–Reference Tavil, Öztürk and Üreten13,Reference Topaloglu, Ozaltin and Yilmaz35,Reference Yalçinkaya, Çakar and Misirlioğlu36 The main pathophysiologic mechanisms for diastolic dysfunction are increased cytokines in circulation, decreased nitric oxide, and atherosclerosis.Reference Panossian, Hambartsumyan and Panosyan37 Thus, the underlying mechanism of ventricular diastolic dysfunction is a subclinical, chronic, continuous inflammatory process.Reference Baysal, Peru and Oran10–Reference Tavil, Öztürk and Üreten13,Reference Nussinovitch, Kaminer and Nussinovitch34,Reference Tavil, Üreten and Öztürk38 Tissue Doppler echocardiography is able to evaluate diastolic functions because it is not affected by preload or afterload. Many studies have used conventional echocardiography with familial Mediterranean fever patients,Reference Canpolat, Dural and Aytemir12,Reference Tavil, Öztürk and Üreten13,Reference Topal, Tanindi and Kurtoglu32,Reference Ardic, Kaya and Yarlioglues39–Reference Terekeci, Ulusoy and Kucukarslan43 while tissue Doppler echocardiography has only been used in three paediatric studies.Reference Baysal, Peru and Oran10,Reference Ozdemir, Agras and Aydin40,Reference Ceylan, Özgür and Örün44 Two of these studies evaluated only the left ventricle, while the other evaluated both. Baysal et al.Reference Baysal, Peru and Oran10 evaluated only left ventricular function, finding the presence of diastolic dysfunction in children with familial Mediterranean fever. The other study of the left ventricle showed that the values for different tissue Doppler echocardiography parameters (the S and A waves of the septal mitral annulus) were lower in children with familial Mediterranean fever.Reference Ceylan, Özgür and Örün44 The third study reported that left ventricular function was preserved while right ventricular diastolic function was impaired in children with familial Mediterranean fever, which is an early sign of cardiac involvement.Reference Ozdemir, Agras and Aydin40 They speculated that right ventricular diastolic dysfunction may be more important due to the nonconcentric contraction of the right ventricle and its complex structure.Reference Ozdemir, Agras and Aydin40 In our study, we evaluated both ventricular functions to be similar to those found by Ozdemir et al.Reference Ozdemir, Agras and Aydin40 Thus, we found that the Sd, Ed, and Ed/Ad waves of both ventricles were decreased, and the Ad waves of both ventricles and the interventricular septum were increased in the familial Mediterranean fever group. We also demonstrated that both right and left ventricular function indices are impaired in children with familial Mediterranean fever.
It is known that increased aortic stiffness is an independent risk factor for cardiovascular diseases.Reference Mitchell and Izzo45–Reference Pereira, Maldonado and Pereira47 Because aortic stiffness parameters are impaired in autoimmune diseases, it is thought that these parameters may also increase in familial Mediterranean fever. While studies in adults with familial Mediterranean fever have shown an increase in aortic stiffness, one study has shown that there is no difference between the control group and adults with familial Mediterranean fever.Reference Tavil, Öztürk and Üreten13,Reference Sari, Arican and Can42,Reference Yildiz, Masathoglu and Seymen48 Only two have evaluated the aortic stiffness in children with familial Mediterranean fever. Sgouropoulou et al.Reference Sgouropoulou, Stabouli and Trachana49 found that carotid-femoral pulse wave velocities of the familial Mediterranean fever children and controls were similar. Turkuçar et al.Reference Türkuçar, Yıldız and Küme50 showed that the stiffness of descending aorta was lower. We found that aortic strain and distensibility were decreased, and aortic stiffness β index, Ep, and Ep* were increased in children with familial Mediterranean fever. We think that increased aortic stiffness indices reflect the presence of subclinical effects in patients with familial Mediterranean fever.
Heart rate variability is a simple and reliable tool commonly used to assess the autonomic nervous system. Few studies showed cardiovascular effects and autonomic dysfunction in patients with familial Mediterranean fever using heart rate variability.Reference Canpolat, Dural and Aytemir12,Reference Kaya, Suner and Koroglu51–Reference Nussinovitch, Esev and Lidar53 On the other hand, only two studies have evaluated heart rate variability in children with familial Mediterranean fever.Reference Şahin, Kır and Makay31,Reference Fidanci, Gulgun and Demirkaya54 Fidancı et al.Reference Fidanci, Gulgun and Demirkaya54 showed that SDNN values were lower; RMSSD and PNN50 values were normal in the uncomplicated children with familial Mediterranean fever during the attack-free period. Otherwise, Sahin et al.Reference Şahin, Kır and Makay31 detected that time-domain heart rate variability parameters of the familial Mediterranean fever children and healthy subjects were similar. We also demonstrated a significant decrease in the time domain of heart rate variability parameters to be similar to those found by Fidanci et al.Reference Fidanci, Gulgun and Demirkaya54 These results suggested diminished vagal and total activity.
Clinical findings are usually sufficient for the diagnosis of familial Mediterranean fever, and genetic testing is mostly performed to support the diagnosis. Although many mutations have been found so far, M694V, M680I, V726A, M694I, and E148Q mutations are responsible for 85% of cases.Reference Cobankara and Kiraz27 In our country, M694V mutation is the most common in patients with familial Mediterranean fever.Reference Cobankara and Kiraz27,Reference Touitou55,Reference Urfali, Yilmaz, Özkul and Urfali56 Although the molecular effects of the M694V mutations have not yet been understood, studies of familial Mediterranean fever patients have reported that the M694V mutation is the most deleterious in a homozygous genotype, and they also appear to be effective in heterozygous mutations.Reference Colak, Gurlek and Yegin8,Reference Touitou55,Reference Grimaldi, Candore and Vasto57 The M694V mutation is associated with a complicated clinical course and increased sensitivity to inflammatory diseases and cardiac involvement.Reference Grimaldi, Candore and Vasto57 One study showed that the heart rate recovery 1 and heart rate recovery 2 values were a negative correlation with M694V homozygous mutation in familial Mediterranean fever children.Reference Evrengül, Yüksel and Doğan58 Contrary to previous studies, we additionally also evaluated the role of M694V mutations on cardiac function in children with familial Mediterranean fever. In our study, the most common mutation was M694V. We compared the clinical effects of the M694V mutation and data of the patients with and without the M694V mutation. We found that C-reactive protein and erythrocyte sedimentation rate levels were increased in children with the M694V mutation. We think that inflammation is more prevalent in children with the M694V mutations because they have a higher acute phase response. In familial Mediterranean fever children with the M694V mutation, mean QT and QTcd were longer; mitral E was higher; tricuspid Sd, Ed, Ad were increased; Ep, Ep*, aortic stiffness β index were higher; aortic strain and distensibility were lower; SDNN and SDANN were decreased, but not significantly different. Due to the small number of cases in each group and the younger age at diagnosis of familial Mediterranean fever, we think that there are no significant difference cardiac functions in patients with the M694V mutation. Further research is needed to understand the effects of M694V mutation.
Colchicine is the mainstay of the treatment in familial Mediterranean fever and a well-developed anti-inflammatory drug. It has been used for more than 50 years for the prevention of acute inflammatory attacks and deposition of amyloid in patients with familial Mediterranean fever.Reference Imazio and Nidorf59 When used in recommended doses, colchicine reduces serum C-reactive protein values in rheumatic and cardiovascular diseases. The cardioprotective effects of colchicine in familial Mediterranean fever have been extensively studied. Colchicine prevents cardiac ischaemia and pericarditis by inhibiting the mitotic activity of neutrophils, platelets, and endothelial cells.Reference Gasparyan, Ayvazyan and Yessirkepov60,Reference Yuksel, Ayvazyan and Gasparyan61 It has been showed that colchicine also prevented recurrences of pericarditis in familial Mediterranean fever patients.Reference Adler, Finkelstein and Guindo62 A few studies have shown that colchicine may reduce the risk of coronary artery disease in familial Mediterranean fever patients by suppressing augmented atherosclerosis and preventing amyloid deposition.Reference Ambartsymian63,Reference Langevitz, Livneh and Neumann64 Sari et al.Reference Sari, Karaoglu and Can65 found regular colchicine treatment may prevent atherosclerosis and endothelial dysfunction in familial Mediterranean fever patients. Several small case-control studies showed that the familial Mediterranean fever group regularly treated with colchicine had p wave and QT dispersion values comparable to healthy people.Reference Nussinovitch, Livneh and Katz33,Reference Nussinovitch, Kaminer and Nussinovitch34,Reference Sari, Arican and Can42 Ocal et al.Reference Ocal, Ocal, Kup, Eren and Tezcan66 reported that one-year colchicine treatment in familial Mediterranean fever patients may reduce various ventricular repolarisation indices. The effect of colchicine on autonomic dysfunction is not known.Reference Canpolat, Dural and Aytemir12 Nussinovich et al.Reference Nussinovitch, Stahi and Livneh67 demonstrated that familial Mediterranean fever patients receiving colchicine treatment may have a decreased incidence of cardiac arrhythmias than recently diagnosed familial Mediterranean fever patients. All familial Mediterranean fever children were treated continuously with colchicine in this study. Therefore, we do not know the impact on outcomes in children who did not receive colchicine. Further research is necessary for the cardioprotective effect of colchicine in familial Mediterranean fever patients.
In conclusion, familial Mediterranean fever patients are at risk for cardiovascular disease because of subclinical inflammation during the attack-free period. These patients should be followed more closely. Arterial stiffness index and heart rate variability parameters of patients should also be evaluated since subclinical effects can be better understood. Therefore, cardiovascular risk can be predicted in the early stages of the disease, and necessary precautions can be taken. Arytmia, pericarditis, impairment of both right and left ventricle functions, and ıshaemic heart disease are important in the familial Mediterranean fever. We believe electrocardiography, conventional and tissue Doppler echocardiography, and 24-hour ambulatory Holter monitoring may be useful for children to be followed regularly after diagnosis. Compliance with colchicine therapy and improved disease control may help reduce the likelihood of arrhythmias in these patients. To the best of our knowledge, this is the first study in the literature that globally assesses several indices of cardiac autonomic functions using electrocardiography, conventional, tissue Doppler echocardiography, and 24-hour ambulatory Holter monitoring in children with familial Mediterranean fever.
There is a need for prospective studies in larger series in children with familial Mediterranean fever, including patients with amyloidosis, and evaluating the relationship between mutations of the Mediterranean fever gene and cardiac functions.
Authors’ contribution
SYA, DG, and SY wrote the main manuscript text and SYA prepared tables. All authors reviewed the manuscript. All authors have participated in the work and have reviewed and agree with the content of the article.
Financial support
The authors received no financial support for the research and/or authorship of this article.
None of the article contents are under consideration for publication in any other journal or have been published in any journal.
No portion of the text has been copied from other material in the literature.
I am aware that it is the authors responsibility to obtain permission for any figures or tables reproduced from any prior publications and to cover fully any costs involved.
Competing interests
None.









