



Background
Palliative sedation (PS) is a clinical intervention of the last resort variety in end-of-life care, which is used to make tolerable the suffering caused by refractory physical, psychological, and/or existential symptoms. It can be defined as “the monitored use of medications intended to induce a state of decreased or absent awareness (unconsciousness) in order to relieve the burden of otherwise intractable suffering in a manner that is ethically acceptable to the patient, family, and health-care providers” (Cherny and Radbruch Reference Cherny and Radbruch2009, 581) A recent empirical study in 7 countries showed that PS was considered acceptable by physicians in cases of physical suffering (87–99%) and, to a lesser extent, in cases of psycho-existential suffering in the absence of physical symptoms in the last days of life (45–88%) (Heijltjes and Morita et al. Reference Heijltjes, Morita and Mori2022).
A recent French study involving 8,500 patients in palliative care units found that 0.5% of them requested PS; within this group, a psycho-existential distress item was present in 69% of the requests (Serey et al. Reference Serey, Tricou and Phan-Hoang2019). PS for existential suffering (PS-ES) is far from a consensus among physicians and palliative care experts, specifically regarding its adequacy for treating this kind of suffering and the conditions of its application (Cassell and Rich Reference Cassell and Rich2010; Rainone Reference Rainone2015; Sulmasy and Jansen Reference Sulmasy and Jansen2002). The objective and subjective assessment of existential suffering (ES) is a complex issue (Bozzaro and Schildmann Reference Bozzaro and Schildmann2018) as it has been described in a variety of ways, that is, as loss of dignity, demoralization, dependency, fear, panic, death anxiety, hopelessness, worthlessness, meaninglessness, loneliness, isolation, loss of control, lack of social support, a sense of burdening others, and being mentally exhausted or worn out. For our purposes, we assume that ES is pain, distress, or hardship due to a loss or interruption of meaning, purpose, or hope in one’s life (Kirk and Mahon Reference Kirk and Mahon2010).
A recent systematic literature review on physicians’ perceptions of PS-ES (Rodrigues et al. Reference Rodrigues, Menten and Gastmans2020) establishes some evidence regarding the conditions that physicians consider essential for implementing PS-ES, for example, regarding prognosis and refractoriness, patient request, family, and team involvement. The review also reports the possible alternatives to deep continuous PS, for example, regular palliative care, mild and intermittent sedation, psychological and spiritual care, physician-assisted suicide, and euthanasia. However, physicians remain ambivalent regarding PS-ES (Anquinet et al. Reference Anquinet, Rietjens and van der Heide2014; Cripe et al. Reference Cripe, Perkins and Cottingham2017; Rodrigues et al. Reference Rodrigues, Crokaert and Gastmans2018; Smyre et al. Reference Smyre, Yoon and Rasinski2015; Voeuk et al. Reference Voeuk, Nekolaichuk and Fainsinger2017), and a recent systematic review on practices, ethical considerations, and guidelines concludes that it is still a very controversial practice (Ciancio et al. Reference Ciancio, Mirza and Ciancio2020).
The findings reported here come from a larger study concerning Belgian palliative care physicians’ perceptions on PS-ES. In the first part of this study, which explores palliative care physicians’ perceptions regarding the ethics of PS-ES, we found that physicians are unsure whether PS is an ethical appropriate answer to ES (Rodrigues et al. Reference Rodrigues, Ostyn and Mroz2022)
Although extensive research has been done regarding decision-making in PS in general (Arantzamendi et al. Reference Arantzamendi, Belar and Payne2021; Belar et al. Reference Belar, Arantzamendi and Menten2022; Benitez-Rosario and Ascanio-Léon Reference Benitez-Rosario and Ascanio-Léon2020; Schildmann and Schildmann Reference Schildmann and Schildmann2014), to our knowledge, no empirical study has explicitly focused on what palliative care physicians take into account in their decision-making regarding PS-ES and how the decision-making actually takes place. To address this gap, we focused in the second part of our qualitative study on the content related to and the process of physicians’ decision-making regarding PS-ES. Better insight into this topic can provide important elements to inform research, policy, and practice.
Method
Study design
We used a qualitative design for this study, along with a grounded theory approach (Singh and Estefan Reference Singh and Estefan2018) and the application of the Consolidated Criteria for Reporting Qualitative Research guidelines (COREQ) (Tong et al. Reference Tong, Sainsbury and Craig2007).
Recruitment and sampling
We used a nationwide sampling method to recruit palliative care physicians practising within hospital-based palliative care units or hospices in Flanders, Wallonia, and Brussels, who met the following inclusion criteria:
(1) Palliative care doctors working within Belgian hospital-based palliative care units or stand-alone hospices;
(2) Physicians with more than 1 year of clinical experience in palliative care, including experience with the practice of PS-ES; and
(3) Individuals willing to be interviewed in English, Dutch, or French languages.
We compiled a list of potential participants (n = 66) from the membership rosters of the following organizations: the Palliative Care Federation of Flanders (n = 37), the Walloon Federation of Palliative Care (n = 19), and the Palliative and Continuing Care Federation of Brussels (n = 10). We sent an invitation letter to all potential participants by post, along with an information brochure about the study. Those willing to participate returned the informed consent form and the demographic questionnaire by post or email. Nonrespondents were sent an email reminder after 3 weeks and again after 6 weeks.
Data collection
We carried out data collection and analysis with an interdisciplinary team of 2 senior researchers in bioethics (CG) and theology (PR) and 3 master’s students in bioethics (JO, SM, and AR). We conducted semistructured interviews on campus between December 2018 and March 2019. Physicians from Brussels and Wallonia were interviewed in French (PR), and participants from Flanders could choose to be interviewed in English (SM) or Dutch (AR).
Prior to each interview, we asked the participants whether they had any questions, and they gave informed consent and permission to record their interviews. The interviews lasted from 28 to 96 minutes each (mean = 47 min), and most of these took place at the workplace of the participant. Other than the participant and the interviewer, no one else was present at the interview. We did not provide feedback or return the transcripts to the participants, and repeated interviews were not conducted.
The team developed and utilized an interview guide (Annex 1 in the Supplementary material) based on 2 literature reviews (Rodrigues et al. Reference Rodrigues, Crokaert and Gastmans2018, Reference Rodrigues, Menten and Gastmans2020) and a clinical vignette (Blondeau et al. Reference Blondeau, Roy and Dumont2005). The interview guide allowed researchers to explore participants’ perceptions of the content and the process of decision-making regarding PS-ES. We took field notes during and after each interview and transcribed and anonymized the data from the audio recordings. We concluded the data collection process when the data saturation point was reached.
Ethical considerations
This study was approved by the Ethics Committee Research of KU Leuven (MP007690) in compliance with the General Data Protection Regulation 2016/679. We collected only relevant data for the research, which was coded and stored on a KU Leuven institutional server. Codes were stored in a separate password-protected file.
Data analysis
We (JO, PR, and CG) analyzed the data using the Qualitative Analysis Guide of Leuven (QUAGOL) (Dierckx de Casterlé et al. Reference Dierckx de Casterlé, De Vliegher and Gastmans2021, Reference Dierckx de Casterlé, Gastmans and Bryon2012), which involves a continual comparison of uncovered insights with the data. The QUAGOL consists of 2 stages, namely, the preparation of coding and the coding process. Examples of a “conceptual scheme” and an “overarching conceptual scheme” are provided in Annexes 2–3 in the Supplementary material. We used NVivo (1.5.1 (940)) by QSR International to code the data. The codes emerged from the data. Detailed methods are described elsewhere (Rodrigues et al. Reference Rodrigues, Ostyn and Mroz2022).
Results
Participants’ characteristics
We contacted sixty-six (n = 66) palliative care physicians, of whom 25 (n = 25; Return Rate = 38%) were willing to participate in the study and were subsequently interviewed. The participants were from Flanders (n = 11), Wallonia (n = 11), and Brussels (n = 3). The sample had wide variability in regard to age (32–70 years), medical discipline, clinical experience (1–43 years), and experience in palliative care (1–30 years); in addition, the physicians worked in 23 different institutions (university hospitals, regional hospitals, and hospices) in Belgium (Flanders, Brussels, and Wallonia). The large majority had clinical experience within the last 12 months with receiving requests for and conducting PS-ES. Most participants were female (n = 16) and Roman Catholic (n = 17). Detailed characteristics of the participants are described elsewhere (Rodrigues et al. Reference Rodrigues, Ostyn and Mroz2022).
The content of the decision-making regarding PS-ES
When pondering PS-ES, physicians consider certain criteria. They will not initiate PS-ES until their patients have asked and have given informed consent for it, and they will perform it only after they have explored all alternatives to reduce ES and found it to be refractory. In addition, they will perform PS-ES only when patients are suffering unbearably and, in most cases, when their ES is combined with physical suffering. Almost all physicians report that only patients with a maximum life expectancy of 2 weeks can undergo PS-ES (for quotations, see Table 1).
Table 1. Themes and illustrative quotations
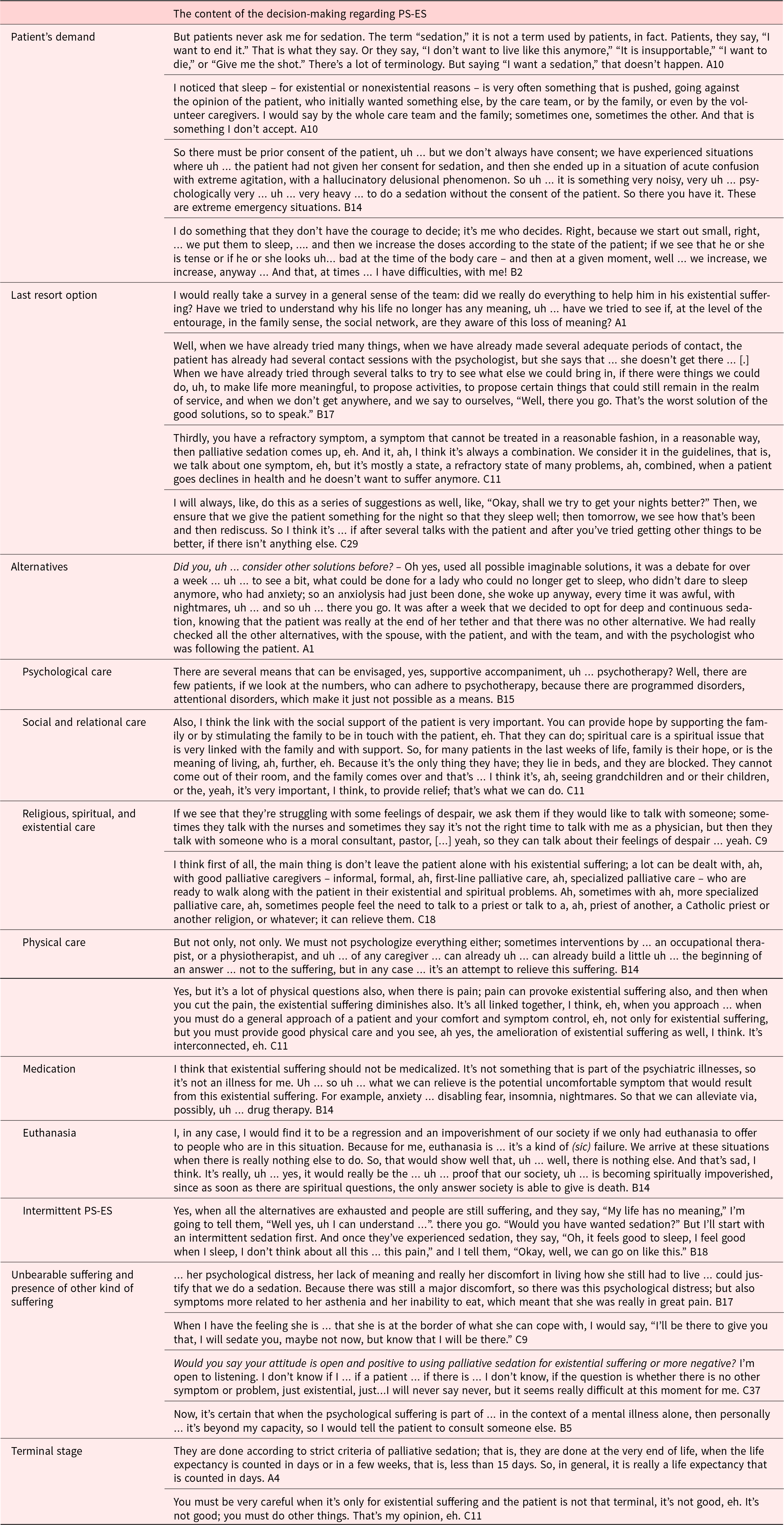
Patient’s demand
All physicians consider the patient’s demand for PS-ES a main requirement for initiating it, but they have different opinions about what a demand entails. Some physicians perceive patients’ expression of suffering as an implicit demand for PS-ES, whereas others believe this expression is insufficient and wait for the patient to prompt them to take action. They explain that patients rarely request PS-ES but ask instead for someone to end their suffering or even ask for euthanasia. These physicians usually propose PS-ES and recognize the patient’s consent as an essential requirement to start it.
When a demand is expressed, physicians discuss the demand with their patients to verify whether they truly want PS-ES or another kind of intervention. Some physicians believe it is necessary to explain PS-ES, including its drawbacks. Many physicians indicate that patients’ demand for PS-ES has to be repeated over time, as their ES may fluctuate or even disappear. In addition, some physicians require that the patient’s demand should not be driven by external factors, such as family members’ demands or caregivers’ desire to be relieved of their own suffering or fatigue. Nonetheless, physicians recall cases where the patient’s consent for PS-ES was not obtained, for example, in case of extreme urgency, or when sedatives were gradually increased from mild sedation to a level of deep sedation.
Last resort option and alternatives to PS-ES
All physicians consider PS-ES as a last resort option and thus as a response to refractory symptoms. This requires that adequate care at the physical, psychological, social, and spiritual levels has already been provided but has not brought about any satisfactory relief of the patient’s ES. One physician explained that PS-ES cannot be justified when the patient has been given non-up-to-date professional palliative care. Instead, PS-ES can be considered when optimal care has been provided but has not had a sufficient effect on the patient’s ES and no other intervention seems sufficient to make the patient feel more comfortable.
Before initiating PS-ES, physicians first consider many alternatives. A large majority of physicians view ES as a state of global suffering and consider a wide range of options for its treatment. Some emphasize the importance of global support for the patient and his or her accompaniment by a palliative care team and relatives and perceive this as an alternative to PS-ES. Almost all physicians will involve a psychologist or psychiatrist to alleviate ES. However, some mention that psychotherapy comes too late for terminally ill patients, as this intervention takes time to produce a positive effect. A majority of physicians stress the importance of accompaniment by family members and the creation of a meaningful and supportive environment by the patient and caregivers, especially by social workers; some also recontact family members and try to organize a meeting. According to some physicians, ES can also be alleviated by regularly spending time with the patient.
A majority of physicians will offer religious, spiritual, or existential care to their patients, for example, anointment of the sick, meditation, and musicotherapy. In doing so, they take the patient’s beliefs and values into account. Many physicians also try to give hope and meaning to their patients by talking with them and emphasize that this kind of care can be provided by many different health-care providers.
Some physicians point out that physical care – offered by physicians, nurses, physiotherapists, and ergotherapists – is key to reducing physical pain, which may in turn result in a reduction in ES. To a lesser extent, physicians also regard medication as a treatment for patients with ES. For instance, some physicians try to treat ES with anxiolytic drugs or antidepressants. However, some of them argue that ES cannot be treated by PS.
Some physicians perceive euthanasia as an alternative to PS-ES, but others believe that euthanasia and PS-ES are completely different from each other. Even if 2 physicians mentioned that they would allude to euthanasia during a conversation with their patient, most of them felt that such a request should come directly from the patient.
Some physicians view intermittent PS-ES as an alternative to deep continuous sedation. They will suggest or ask to try intermittent PS-ES first before allowing deep continuous PS-ES. Other physicians strongly disapprove of intermittent PS as an intervention for truly terminal patients with ES.
Unbearable suffering and the presence of other kinds of suffering
Physicians explain that PS is not performed on all patients with ES. Many physicians assert that PS-ES can only be performed when patients are in great discomfort, find their state unbearable, or are at the end of their tether. Some describe that the degree of suffering experienced by the patient is very subjective, as it differs from patient to patient. Nevertheless, physicians feel a need to determine how great the patient’s ES is and whether it requires PS, despite the difficulty of assessing ES.
Nearly all interviewees report that they will only perform PS if ES is combined with physical suffering, which they claim is mostly the case with their patients. Some physicians express difficulty with patients asking for PS when they only have ES. In that case, physicians believe either they are not competent to deal with ES or that their patients are not in the end-of-life stage.
Terminal stage
Almost all physicians state that PS-ES can only be performed if the patient is in the terminal phase of life. Some argue that this is an obvious condition because otherwise it would not be PS but rather a form of hastening death or a kind of disguised euthanasia. According to half of them, the life expectancy at this point should be less than 15 days or 1 week; however, one physician admits to having practised PS-ES outside the short-term prognosis.
The decision-making process regarding PS-ES
Based on our analysis of the interviews, we found that PS-ES decision-making is perceived by Belgian palliative care physicians as a process that is characterized by 4 aspects: 1) it appears to be a multiperspective process; 2) it takes place through interpretative dialogues; 3) it is followed by the physician’s inner conviction of its necessity preceding the final decision; and 4) it takes place over time (for quotations, see Table 2).
Table 2. Themes and illustrative quotations
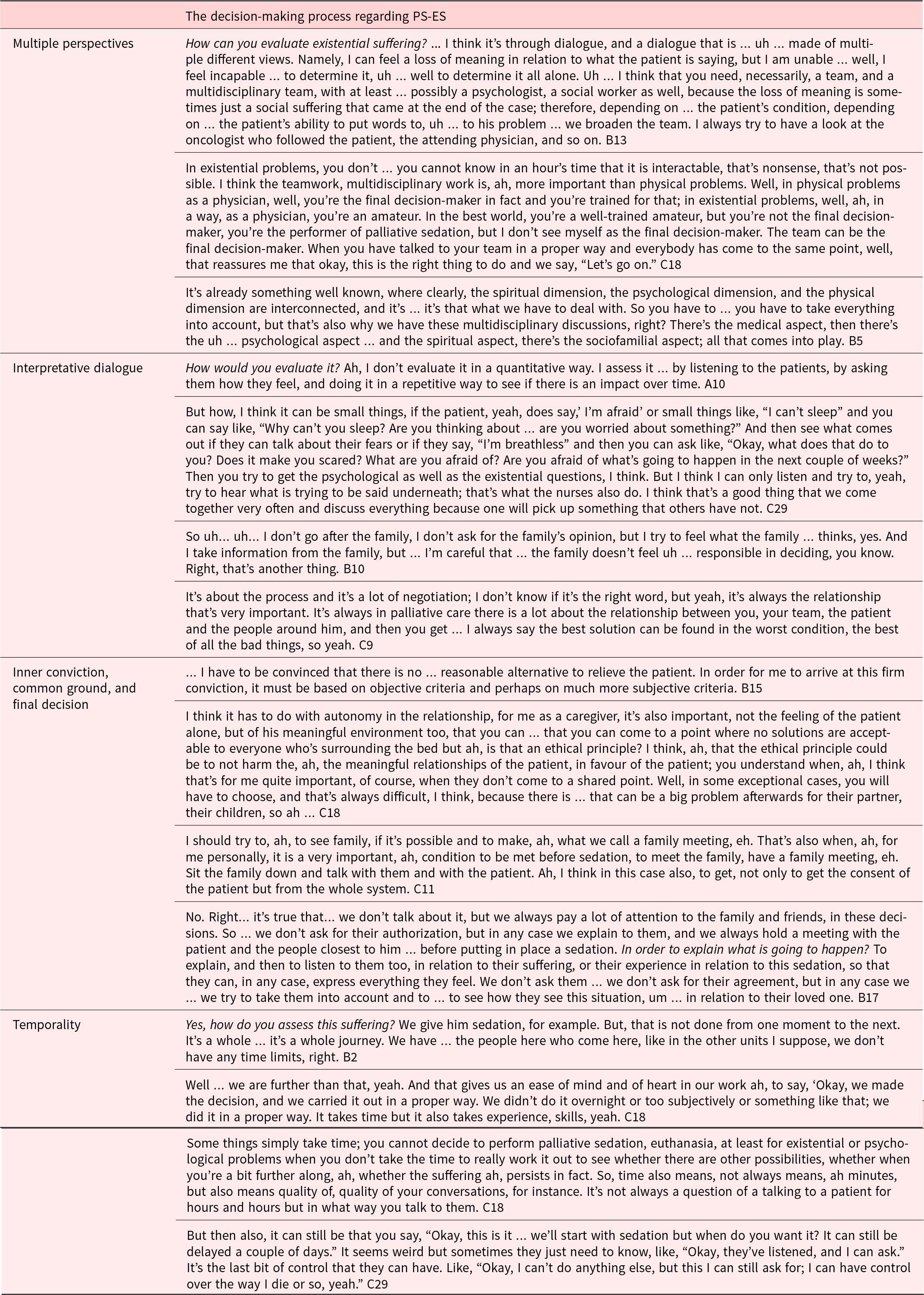
Multiple perspectives
Physicians emphasize that they never make a decision about PS-ES without consulting the relevant stakeholders, namely, the patient, the patient’s relatives, and the palliative care team, including other physicians, nurses, social workers, physiotherapists, occupational therapists, chaplains, etc.
Physicians indicate that they need input from multiple perspectives to make a decision about PS-ES, especially to assess whether the ES is unbearable and whether there are any less invasive alternatives. Some physicians explain that the decision-making process would be too subjective without this multiperspective assessment of the patient’s ES. A couple of physicians mention the danger of projecting their own feelings on their patients, while other physicians are aware they are not omniscient regarding ES and the adequacy of PS to treat it. By listening and talking to others, physicians can verify that their impression is being shared by others. Some point out that to make a decision about PS-ES, they should consider the physical, psychological, relational, and existential dimensions of the patient as a whole person. This holistic care approach calls for the active involvement and contribution of multiple stakeholders.
Interpretative dialogue
The PS-ES decision-making process, especially the evaluation of ES, is characterized by an active and iterative process of exchanging information and perceptions between the stakeholders and the understanding and interpretation thereof.
Almost all interviewees explain that they enter into dialogue with their patients multiple times and get to know them on a deeper level. Some physicians indicate that they try to follow their patients as closely as possible and emphasize the importance of a mutual trusting relationship to achieve this goal. By talking, listening to, and asking questions, physicians are able to explore their patients’ ES and actively look for ways to relieve it. One physician underlines the value of these conversations for the patients themselves because it allows patients to express what is happening to them.
Many physicians also ask their team members about their interpretation of patients’ suffering. Some physicians mention that patients express their suffering in different ways to different team members or even hide it from certain members, thereby creating complex situations that require good team communication. A few physicians also remark that they talk to patients’ relatives to gain insight into the latter’s suffering. Based on the complementary information and perceptions gathered, physicians try to reach an interpretation of the patient’s suffering, which to a certain level can be understood by the other stakeholders.
Inner conviction, common ground, and final decision
Physicians explain that at some point they arrive at the inner conviction that PS-ES can be the right course of action. Moreover, they aim to make a decision that is in accordance with their inner conviction. Some of them specify that their inner conviction is grounded in a deeper understanding of the patient’s suffering. This contains a cognitive element, namely, understanding why the patient suffers, and an emotional element, which consists of a kind of “empathy” with the patient.
Physicians report that in most cases, their inner belief is supported by the patient’s understanding of his or her suffering, as well as by the family members’ and the team’s interpretation of the situation. However, some physicians explain that relatives do not always understand the patient’s suffering because patients can hide their ES from their family. In this case, physicians say it is essential that the relatives are at least aware of the patient’s suffering in order to understand and accept the patient’s request for PS-ES. However, only a few physicians share that they will explain the suffering of their patient to the relatives if he or she is unable to do so on their own.
Although most physicians indicate that a common ground can be found within the team, some mention that team members can have different opinions regarding PS-ES for a specific case. This is why physicians consider themselves to be the ultimate decision-maker: they make a decision about PS-ES when common ground within the team is lacking. Nevertheless, some other physicians require the consent of all team members and the patient’s relatives to perform PS-ES.
A number of physicians mention the importance of clear prior communication with relatives when the final decision is made so that they know what to expect once sedation has been initiated. In addition, some physicians refer to a family gathering, that is, a time when the patient and their loved ones can say goodbye to each another. One physician points out that team members also need a moment to say goodbye to the patient they have been caring for.
Temporality
Many physicians explain that due to the required multiperspective communication and interpretation process, final decisions about PS-ES are not made quickly but instead take some time. Two physicians explicitly add that when a decision is made quickly, it is not made properly. Most doctors do not specify the amount of time it takes to make such a decision, although some say it requires a minimum of 2 days. Furthermore, many physicians refer to a qualitative way of dealing with time in end-of-life care, such as taking time to gain a deeper understanding, processing relevant information, and allowing thoughts and points of view to mature. It is also pointed out that taking time does not imply that the decision-making process should be unnecessarily extended.
A couple of physicians explain that when a decision is made to perform PS-ES, they inform their patients and give them the freedom to determine the most appropriate moment to initiate such treatment. In this way, patients can maintain control of the situation. One physician also mentions that she prefers to perform PS-ES in the evening because it is a natural time to fall asleep.
Discussion
Content of decision-making
This study shows that physicians consider the following conditions under which PS might be used for ES: 1) the patient’s demand for such treatment, 2) the presence of the condition of unbearable ES (preferably combined with physical suffering), 3) a less invasive alternative treatment cannot be found, and 4) a terminal stage condition. Even if, in general, physicians seem to agree with these conditions, the priority and interpretation given to each one is not equivalent when considering concrete complex cases of end-of-life ES.
A recent systematic review on physicians’ perceptions of PS-ES (Rodrigues et al. Reference Rodrigues, Menten and Gastmans2020) provides evidence that these conditions do not have the same weight according to all physicians. Some consider the patient’s explicit request for PS-ES to be determinant, while others consider the consultation and involvement of the family (Foley et al. Reference Foley, Johnston and Bernard2015), the decision of the primary care team (Beauverd et al. Reference Beauverd, Bernard and Currat2014), or consultation with a multidisciplinary team (Papavasiliou et al. Reference Papavasiliou, Payne and Brearley2014) to be necessary in the final decision. Our study seems to confirm the latter process, as most of the interviewed physicians place a high level of importance on the involvement of all stakeholders in the decision-making process.
The refractory nature of ES is also a condition of consideration, as some physicians find it very difficult to objectively assess ES. For most participants in our study, ES must be combined with other types of suffering for PS to be considered, which is in line with the literature indicating that physicians have a higher level of comfort using PS for refractory physical symptoms and thus prefer to wait for the combination of physical suffering or physical deterioration to initiate PS-ES (Schur et al. Reference Schur, Radbruch and Masel2015).
In our study, physicians also consider it important to verify the patient’s terminal condition; however, a comparative study with French-speaking physicians from Quebec and Switzerland found that neither the prognosis nor the interaction between the prognosis and the type of suffering influenced physicians’ attitudes toward PS-ES (Dumond et al. Reference Dumond, Blondeau and Turcotte2015). This difference in findings supports the need for further qualitative and quantitative research to confirm or refute it.
A recent scoping review (Amy et al. Reference Ciancio, Mirza and Ciancio2020) concludes that certain aspects complicate clinical decisions regarding PS-ES, namely, the lack of a precise definition of ES and clinical studies on PS-ES, difficulty assessing ES symptoms, monitoring the effectiveness of treatment, the degree of subjectivity in starting PS-ES due to the lack of guidelines, and the need for a clear understanding of the values and worldviews involved. In this review, 80% of the articles analyzed do not reach a clear consensus pertaining to whether PS-ES is acceptable or not; this finding supports our results, given that most of the physicians interviewed seem to hesitate regarding PS-ES interventions.
Process of decision-making
This study shows that PS-ES decision-making is an iterative multidisciplinary process of communication and interpretation that takes place over time. Physicians highlight the importance of consulting all relevant stakeholders to verify whether the conditions for PS-ES have been fulfilled and whether their interpretation is consensual. Belgian physicians try to reduce the risk of a subjective individual perspective by sharing their perceptions and opinions to come to some level of agreement and make shared decisions. In-depth communication between physicians, patients, relatives, and team members provides a profound understanding of the patient’s global suffering, the ability to identify what is contributing to his or her ES, and the ability to assess it in a more comprehensive way. These results are consistent with recent systematic reviews (Amy et al. Reference Ciancio, Mirza and Ciancio2020; Reich et al. Reference Reich, Bondenet and Rambaud2020), which show that diagnosing psycho-existential refractory symptoms requires a multidimensional perspective of a patient’s condition and a collaboration between different professionals (physicians, nurses, psychologists, psychiatrists, spiritual/religious advisors, and ethics committee members) to add objectivity to the decision-making process.
Methodological discussion
To our knowledge, this is the first Belgian nationwide (Flanders, Brussels, and Wallonia) qualitative study to provide in-depth insight into palliative care physicians’ decision-making regarding PS-ES. Even if theoretical sampling has not been applied, the sample reflects a wide range of gender, age, specialization, and experience in palliative care. The data were analyzed following the QUAGOL protocol, which integrated systematic team reviews and continuous dialogue. Conducting research in 3 different languages (Dutch, English, and French) was the main difficulty, but the team had the necessary skills to manage it. As our results are based on data collected within hospital-based palliative care units and stand-alone hospices, they cannot be generalized to other care settings, such as home care and nursing homes.
Conclusion
This empirical study brings to light the content related to and the process of decision-making about PS for ES by Belgian palliative care physicians. Most physicians are not sure about the precise and objective criteria regarding decision-making in PS-ES and stress the importance of participation by all stakeholders to come to acceptable solutions in complex situations involving existential refractory suffering at the end of life.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951522001547.
Data availability statement
The data for this study are kept by the first author and are available on request.
Author contributions
All authors were involved in the conception and design of this study. PR, SM, and AR carried out all the qualitative data collection. Data analysis and interpretation were performed by JO, PR, and CG, who also wrote the paper. All authors were involved in critically revising the article. All authors approved the final version of the manuscript. CG supervised the study.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
Nothing to disclose.
Ethical standards
The study was approved by the Ethics Committee Research of KU Leuven (MP007690).




