


Cost-effective strategies are needed to reduce the impact of unhealthy diets, one of the most important risk factors for non-communicable diseases(1). One of the approaches that can be used to reduce the impact of unhealthy diets is to encourage citizens to re-assess their eating habits and shift their choices towards healthier foods(Reference Hawkes, Smith and Jewell2). Several strategies have been implemented worldwide to increase the importance attached to healthiness in the daily food choices of citizens, including national dietary guidelines, nutrition education programmes, mass media communication campaigns and labelling policies(Reference Mozaffarian, Angell and Lang3).
Healthiness has long been recognised as one of the characteristics of foods that underlie purchase and consumption decisions(Reference Grunert4,Reference O’Brien, McConnon and Hollywood5) . However, an in-depth understanding of how people conceptualise healthy food and how they make their judgements about food healthiness is still lacking(Reference Paquette6–Reference Bucher, Müller and Siegrist8).
Food healthiness is a complex and dynamic concept, which has evolved over time as new scientific evidence emerged(Reference Mozaffarian, Rosenberg and Uauy9,Reference Monteiro, Cannon and Moubarac10) . People should give meaning to the conflicting and dynamic information they receive from a diversity of sources, including official nutritional recommendations, health professionals, the food industry, the press and social media, to shape their perception of food healthiness(Reference Grunert4,Reference Paquette6,Reference Nestle11–Reference Carolina Demonte14) . Based on the information they receive, people create a rich store of generic knowledge and preconceptions about food healthiness or ‘knowledge structures’ that provide the basis for making judgements(Reference Nisbett and Ross15). Healthy foods tend to be defined, sometimes incorrectly, in relation to specific food groups (e.g., fruit, vegetables and meat), specific nutrients (e.g., low in fat, low salt content and rich in vitamins and minerals), preparation or production methods (e.g., organic, home-made and natural) or the absence of potentially hazardous substances (e.g., toxins, pesticides and additives)(Reference Paquette6,Reference Provencher and Jacob7,Reference Bisogni, Jastran and Seligson16,Reference Mete, Shield and Murray17) .
Up to date, most research has focused on people’s perception about healthy eating and healthy food. However, an in-depth exploration of how healthiness is judged in relation to ultra-processed foods has not yet been performed. The contribution of ultra-processed products to the diet has largely increased worldwide and has paralleled the rise in obesity prevalence(Reference Vandevijvere, Jaacks and Monteiro18). These products are frequently marketed using textual and visual references to healthiness, such as nutrition marketing claims and references to specific ingredients, which are expected to largely influence healthiness perception(Reference Christoforou, Dachner and Mendelson19,Reference Schermel, Emrich and Arcand20) .
A large amount of information is included on the packages of ultra-processed products(Reference Christoforou, Dachner and Mendelson19–Reference Gil-Pérez, Rebollar and Lidón21). Considering that human beings have a limited capacity to process information, people are not expected to invest a large amount of time or to engage in deep processing to make their healthiness judgements(Reference van’t Riet, Sijtsema and Dagevos22,Reference Kahneman23) . Instead, such judgements are expected to be made without much deliberation and based on heuristic strategies(Reference Kahneman23). In particular, people tend to give more relevance to simple, concrete and imagery-provoking information that easily attracts attention, such as the visual and salient information on food labels(Reference Nisbett and Ross15). Thus, people may not rely on more complex information, such as nutritional information or ingredient lists for judging the healthiness of ultra-processed products. These simplified cognitive strategies can lead to misleading judgements about the healthiness of these products, which may influence purchase and consumption decisions(Reference Paquette6). Understanding the heuristics that guide healthiness perception of ultra-processed foods can contribute to the design of policies and communication strategies to discourage their consumption.
In this context, the aim of the present work was to qualitatively explore the conceptualisation of healthy food by citizens and, particularly, how they judge the healthiness of ultra-processed foods.
Materials and methods
Participants
A total of fifty-two participants were involved in the study, conducted in Montevideo, the capital city of Uruguay (South America). Participants were recruited using a Facebook advertisement targeted at Uruguayan adult users, posted by the institutional Facebook account of the research group who authored the study. The advertisement invited participants to join a group discussion about foods in exchange for a voucher worth 70 $US. Interested participants clicked on the advertisement and were directed to an online questionnaire, where they registered their name, provided their contact details, answered a series of questions related to their socio-demographic characteristics: gender, age, educational level and socio-economic level(24) and indicated their self-reported weight and self-reported height.
A total of four focus groups with 9–15 participants were conducted. Initially, three focus groups were planned. Interested participants were randomly selected and contacted to check their availability to attend the focus group discussions, scheduled on different days of the week during a 3 weeks period. Within each focus group, the authors set quotas for gender, age and socio-economic level to achieve similar groups of participants in all discussions. The final number of focus groups was selected based on saturation(Reference Carlsen and Glenton25). During the third focus group, new topics emerged from the discussions, and therefore, an additional focus group was conducted. Additional participants were selected for the fourth focus group using the list of registered participants. During the fourth group, no new topics emerged, indicating that saturation was reached.
Data collection
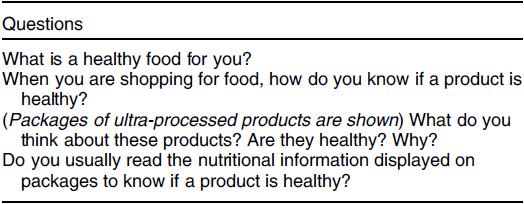
Focus groups lasted 60–90 min and were conducted by a researcher with ample experience in the moderation of focus group discussions. A semi-structured discussion guide was used, which included questions related to the concept of healthy food, the characteristics that define a healthy product, healthiness perception of packaged products and use of the nutritional information displayed on packages to judge product healthiness (Table 1). Commercial ultra-processed products (cookies, crackers, granola, instant soup, flavoured water, mayonnaise and yogurt) were used to trigger discussion about healthiness perception of packaged products. The selected products were positioned as healthy in the Uruguayan marketplace and included textual and visual elements that have been reported to influence healthiness perception.
Table 1 Questions included in the discussion guide of the focus groups
The discussions were audio-recorded and then transcribed. Participants signed an informed consent form. The study was approved by the Ethics Committee of the School of Chemistry of Universidad de la República (Uruguay).
Data analysis
Transcripts of the focus group discussions were analysed in Spanish using content analysis, following an inductive coding approach(Reference Krippendorff26). In this approach, research findings emerge from the raw data as researchers interpret the transcripts to identify recurrent themes and categories(Reference Boyatzis27). In the present work, one of the researchers performed an initial coding of the data by repeated examination of the transcripts of the four focus group discussions. The main themes discussed in the focus groups discussion as well as categories of concepts within the themes were identified. Two additional researchers verified the coding and proposed modifications(Reference Hennink, Hutter and Bailey28). Disagreements among the researchers were resolved through open discussion until agreement about the best coding was reached. Examples of quotes for each theme and category were selected and translated from Spanish to English.
Results
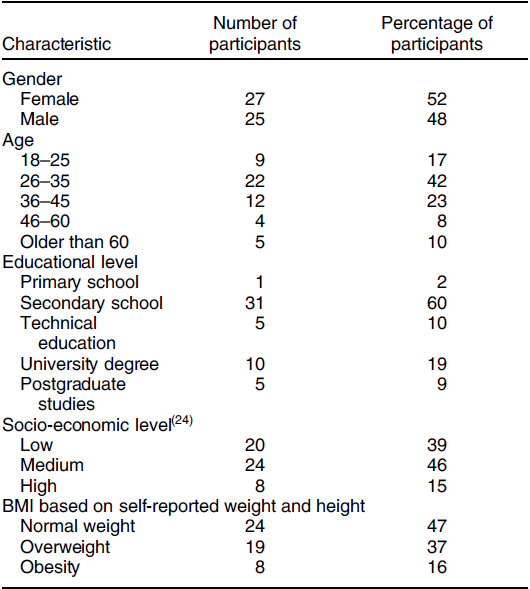
The socio-demographic characteristics of the participants of the focus groups are presented in Table 2. Compared with the Uruguayan population, the sample had a similar distribution in terms of gender and socio-economic status(24,29) . However, it underrepresented older citizens (45 years and older) and citizens with low educational level (primary school only).
Table 2 Socio-demographic characteristics of the participants of the focus groups (n 52)
In the following, the themes and categories identified in the content analysis of the focus group discussion for the two objectives of the present research are presented: the conceptualisation of healthy food and how the healthiness of ultra-processed products is judged. Results are summarised in Figs 1 and 2.
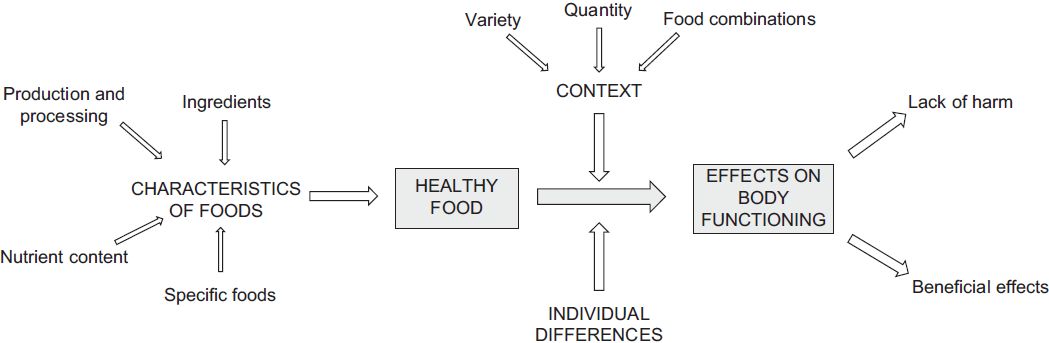
Fig. 1 Themes (capital letters) and categories (sentence case) related to the conceptualisation of healthy food, identified in the content analysis of the focus group discussions
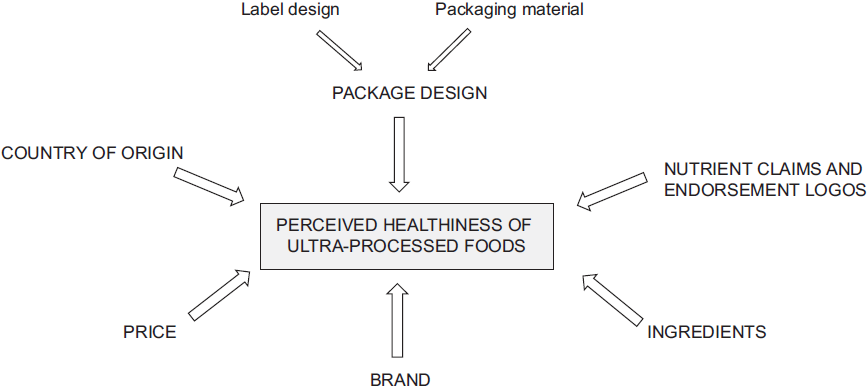
Fig. 2 Themes (capital letters) and categories (sentence case) related to how participants judged the healthiness of ultra-processed foods, identified in the content analysis of the focus group discussions
Conceptualisation of healthy food
Four main themes were identified in the discussion in relation to participants’ conceptualisation of healthy food: characteristics of foods, context, individual differences and effects on body functioning. Figure 1 provides a visualisation of the themes and categories that emerged when participants discussed the concept of healthy food. In general, healthy foods were defined in relation to their effects on body functioning: they were regarded as those that do not cause any harm on health and, if possible, have a positive effect on body functioning.
The characteristics of foods were the most frequently mentioned theme that emerged from the discussion as a determinant of food healthiness. Four main categories were identified within this theme: specific foods, nutrient content, production and processing, and nutrient content (Fig. 1). First, participants associated food healthiness with specific food groups; in particular fruits, vegetables and meat: ‘Something healthy would be meat, fruits and vegetables’.
Then, they referred to the content of specific nutrients. Participants stated that healthy foods had low content of salt, fat, cholesterol and should not contain trans fats. Positive nutrients were infrequently mentioned, and participants mainly referred to vitamins and antioxidants: ‘It should provide beneficial things, such as antioxidants and vitamins’.
Production and processing were important parts of the discussion in relation to healthy foods. Participants identified organic food as healthy, in contraposition to foods with pesticides or genetically modified (GM) foods. Industrial processing was regarded as a negative contributor to food healthiness. In particular, a couple of participants referred to the concept of ultra-processed foods or the number of ingredients as a rule to judge food healthiness. In the following, examples of quotes within this category are provided:
It shouldn’t be too industrially processed, something ultra-processed
I use the rule of the 5 ingredients. If it has more than 5 it is not good
Everything that comes from the earth, from nature… It is for a reason… I don’t think that anything you take from a package and it is ready to eat can be healthy
References to specific ingredients frequently emerged from the discussion. Participants stated that products with sugar, glucose syrup or hydrogenated fat were unhealthy, as well as those with additives (preservatives, colourings), as exemplified in the following quotes:
It is good to check the ingredient list to know if it has glucose syrup
It shouldn’t contain chemicals, colorings
Everything that has preservatives and colorings
Several participants stated that food healthiness is not an absolute concept as the effect on health depends on contextual factors, such as the quantity consumed, and the variety of the diet. Participants stressed that most foods are not harmful if consumed infrequently and in small quantities, and if they are part of a healthy diet. In this line of reasoning, one of the participants stated that healthy foods can have a negative effect on health if consumed excessively. Examples of quotes related to this theme are:
There is something that is not much talked about and is the dose. The definition of poison is any substance that in a specific quantity can be harmful. Water, for example, is pure but it can kill. For me, one of the keys in nutrition is the portion
It depends on the quantity you consume. It is not the same to eat a package than only eat 2 or 3 crackers
As I consume it once in a while, I won’t die
One of the participants also mentioned that certain food combinations are not healthy and referred to the belief that meat and potatoes cannot be consumed together in the same meal: ‘You have certain foods that cannot be simultaneously consumed, meat and potatoes, because they can make you absorbed certain things and not others’.
Another factor that participants regarded as a moderator of the effects of food on body functioning is individual differences. Participants referred to the fact that some foods are harmful for people with specific health problems, such as celiac disease or diabetes.
Healthiness depends on the person, on what he or she needs, because we all have different bodies
What is excessive content of salt or sugar? What is the limit? It is not the same for a 60 years old person than for a 20 years old
There are things that are healthy for everyone and others aren’t
There are certain things that kill celiac people
Perceived healthiness of ultra-processed products
Although participants mentioned that processing had a detrimental effect on healthiness and specifically referred to ultra-processed products, it did not emerge from the discussions that they regarded every ultra-processed product as unhealthy in their everyday life. Some categories were classified as unhealthy (e.g., mayonnaise, potato chips), whereas others tended to be classified as healthy (e.g., yogurt, granola). In some categories, participants recognised the existence of healthy and unhealthy products. This was the case of cookies, crackers, flavoured water and instant soup.
Several simplified decision-making strategies were mentioned to categorise an ultra-processed product as healthy or unhealthy. Interestingly, participants seemed to be aware of the fact that these strategies usually lead to inaccurate conclusions on food healthiness. Lack of time, difficulties for accessing to the information and the complexity of the information were highlighted as barriers for not engaging in an in-depth processing of the information available on food packages. Examples of quotes are provided below:
For me it’s a social phenomenon. It is impossible with our life-style… We are running all day long and everything has to be quick. We lost the habit of thinking and choosing the best food. We lost interest.
It is complicated. If you don’t sit down to read the package…. and you don’t go to the supermarket to study
Sometimes it is difficult to find the ingredients. They are hidden. When they are bad, they are hidden on the package fold. They are not accessible
You have all those numbers. I really don’t know what they mean
I think it is great to be informed but you can’t read and compare everything all the time….Otherwise, you don’t eat anything
Six main themes were identified in the discussion in relation to the cues that guide healthfulness perception of ultra-processed foods: package design, ingredients, nutrient claims and endorsement logos, brand, price and country of origin (Fig. 2). Package design was identified as a relevant cue for judging food healthiness, both unprompted and prompted by the packages exhibited in the focus group. Within this theme, two main categories were identified: label design and packaging material. Regarding label design, several features were associated with healthiness, including colours, font, references to nature, textual or graphical elements related to natural foods, and references to sustainability, as exemplified in the following quotes:
Foods in green packages are healthy. That catches my attention. When you see a food in a green package you think it is healthy, or at least that is what they try to communicate. And you don’t look at anything else
The bottle with the leaves, the colors, the font, the pictures. They look healthy
A lemon, the little thing of wheat, the fruit, natural things
Fruit on the package, in the front…shows that it is good
Specific packaging materials were also perceived as a healthiness and naturalness cue. In particular, participants referred to recyclable or biodegradable: ‘Products in recyclable materials like this one (are healthy)’, ‘Now they usually come in a biodegradable package, or cardboard. On the contrary, potato chips come in a metallized package’.
References to specific ingredients on the package were recognised as a relevant element for judging healthiness. In particular, participants referred to whole grains, cereals and fruit, as exemplified in the following quotes: ‘It says 20 % dried fruit, fresh fruit. You never know. You don’t check if what is written there is true’, ‘It has whole flour, fiber, and cereals’, ‘It has a lot of seeds. I like that a lot and I think it is healthy, right?’. In addition, the presence of specific ingredients, such as preservatives, colourings and hydrogenated fats, was perceived as indicators of unhealthiness, although participants recognised that they do not spend much time reading the ingredient lists.
Nutrient content claims were regarded as indicators of product healthiness, including ‘0 % trans fats’, ‘0 % cholesterol’, ‘contains omega 9’, reduced nutrient content claims or references to vitamins. Endorsement logos from health-related societies were perceived as a trustful sign of healthiness: ‘I trust in ADU (Uruguayan Diabetics Association) because even if they are healthy we (referring to people with diabetes) can’t consume some products, and reading everything is tiring’.
Participants indicated that they associate specific brands with healthy products, mainly due to the positioning of products in the marketplace or even the name of the brand: ‘People associate some brands with healthiness. For example, I see (brand name blinded for publication) crackers and I think they are healthy, even if I know that some of the products have even more fat than (brand name blinded for publication). There are very intelligent brands. Once they are associated with healthiness, they launch a lot of products that are not healthy’. Another participant stated that leading brands are usually associated with less healthy products ‘For me, big brands don’t work. I don’t think they care about making something healthy’.
Price was regarded as an indicator of quality and healthiness. Participants shared the belief that the cheaper the product, the less healthy it is: ‘I generally take into account price. An expensive product is not necessarily good but if it is too cheap, they didn’t put too much effort’ and ‘And price… Because they are the most expensive and expensive products are always the healthiest’. Country of origin also emerged as a simplified strategy for judging product healthiness. Uruguayan products were perceived as healthier compared with imported products, as exemplified in the following quotes:
In general, the national industries are trustworthy
I take into account the country of origin. There are a lot of packaged products from China. I don’t trust some countries
I always prioritize products made in Uruguay. It’s not only to support the national industry. It is because the products are better
Interestingly, none of the participants in the focus groups mentioned the nutritional information included on food packages as a cue for judging the healthiness of ultra-processed foods. When specifically asked about this information, they stated to be aware of it but highlighted difficulties to find it on packages and to understand it. Participants tended to read the ingredient list instead of the nutritional information, as exemplified in the following quotes: ‘How do you know if a product has too much sugar? I read the ingredient list and the taste is unmistakable’.
Discussion
Results from the present work provide additional evidence about people’s conceptualisation of healthy food. In agreement with previous studies on lay perceptions of healthy eating, the conceptualisation of healthy food was mainly focused on food characteristics(Reference Margetts, Martinez and Saba30,Reference Vizireanu and Hruschka31) . Healthy foods were defined in relation to their effects in body functioning, specific food groups (fruits, vegetables and meats), specific nutrients (e.g., vitamins, low fat content), production or processing (e.g., not processed, organic and not GM) and lack of specific ingredients (e.g., preservatives and colourings)(Reference Paquette6,Reference Provencher and Jacob7,Reference Bisogni, Jastran and Seligson16,Reference Mete, Shield and Murray17,Reference Margetts, Martinez and Saba30,Reference Vizireanu and Hruschka31) . Emphasis was placed on the consumption of natural foods, and particularly on fruits and vegetables, in contraposition to highly processed foods. This is in agreement with the recommendations included in the national dietary guidelines(32).
The concepts of balance, variety and moderation emerged from the discussion. Some participants stated that food healthiness is a relative concept, as the effect of foods on the body is moderated by the characteristics of the diet. In particular, emphasis was placed on the quantity and consumption frequency. Previous studies have identified the concept of moderation in response to confusion and inconsistencies around healthy eating(Reference Lupton and Chapman12,Reference Havala33) . Participants mentioned that products may not be harmful if consumed infrequently and in small quantities. This belief can be used to justify any food choice and particularly the consumption of products that are regarded as unhealthy, as previous studies suggest(Reference Paquette6). Moderation has relevant implications for health communication as it can weaken nutritional recommendations. For example, Peruvian regulations state that nutritional warnings highlighting products with high content of sugar, Na and saturated fat should include the expression ‘Avoid excessive consumption’(34). This expression could trigger the idea that products do not cause any health harm if they are not consumed excessively. Further research should explore people’s perception of the quantities and consumption frequencies of ultra-processed foods that are regarded as harmless.
Individual-related characteristics also emerged as a moderator of food healthiness. Participants referred that foods may not be healthy for everyone, particularly due to age differences and specific health conditions (diabetes, celiac disease). Perceived likelihood of suffering the negative conditions of a behaviour and perceived severity of its negative consequences have been reported to be predictors of health-related behaviours (e.g., alcohol use, smoking)(Reference Weinstein35). In the context of the promotion of healthy eating, the moderator effect of individual differences and context stresses the importance of increasing the perceived risk associated with the consumption of ultra-processed foods.
In this sense, results from the present study showed that although participants regarded lack of processing as a cue for healthiness, they did not categorise all ultra-processed products as unhealthy. Albeit some categories were automatically categorised as unhealthy, participants considered that other categories could include healthy and unhealthy products. In such cases, they explicitly referred to several simplified cognitive strategies to judge whether an ultra-processed product is healthy or not, particularly at the time of purchase. Lack of time, lack of cognitive effort and the complexity of the information available were identified as the main motives for not performing an in-depth analysis before taking a decision. This result evidences that judging the healthiness of ultra-processed foods is perceived as a task that requires time and cognitive effort. Similarly, previous research has reported that shoppers believe that making healthy choices requires cognitive effort, particularly at the point of purchase(Reference O’Brien, McConnon and Hollywood5,Reference Mai and Hoffmann36) . Lack of in-depth processing of the information included on the packages of ultra-processed products was mentioned as a strategy to avoid conflictive information. Participants indicated that they prefer not to be aware of information about negative characteristics of the products they usually buy, so that they can keep on consuming them. Consumer tendency to ignore potential risks and to focus on positive characteristics has been reported in other areas of consumer behaviour, such as purchase intention of smart home devices(Reference Wang, McGill and Klobas37).
Decisions that require high cognitive load are expected to be made based on heuristics, particularly if they are repeatedly taken in short time frames(Reference Kahneman23). This is the case of food-related decisions, which has been reported to be habitual in nature(Reference van’t Riet, Sijtsema and Dagevos22). The focus group discussions evidenced a series of heuristics that underlie healthiness judgements of ultra-processed products. Participants seemed to rely on simple cues to categorise ultra-processed products. In particular, package design seems to provide vivid, simple and concrete cues for judging product healthfulness. Participants reported to frequently rely on package colour and images to categorise a product as healthy. Several studies have reported the relevance of visual attributes of food packaging in shaping healthiness perception(Reference Marques da Rosa, Spence and Miletto Tonetto38,Reference van Rompay, Deterink and Fenko39) . Participants seemed to rely on other simple cues, such as nutrient claims, endorsement logos from scientific societies and brand, which have been previously reported to influence perceived healthiness(Reference Lähteenmäki40–Reference Cavanagh and Forestell42).
Several heuristics seem to play a relevant role in shaping the perceived healthiness of ultra-processed foods, being salience bias and the representative heuristic the most relevant. Participants seem to take salient features of the products to judge their healthiness based on the resemblance of those features with other products(Reference Nisbett and Ross15). In addition, persuasion heuristics(Reference Rucker, Petty, Briñol and Stewart43) also seem to play a relevant role, as participants seemed to trust on specific brands or countries of origin, as they were expected to be likely to produce healthy products.
Perceived healthiness has been reported to influence product purchase, consumption and portion size(Reference O’Brien, McConnon and Hollywood5,Reference Provencher, Polivy and Herman44,Reference Lusk45) . The simplified cues identified in the present work seem to increase healthiness perception of ultra-processed foods and could contribute to encourage their consumption. Therefore, multifaceted strategies seem necessary to raise consumer awareness of the negative health consequences associated with the consumption of ultra-processed products and reduce their perceived healthiness. In this sense, educational strategies and communication campaigns could stress the importance of being critical about the information displayed on the packages of ultra-processed products. However, considering that people rely on heuristics for making their decisions, regulatory approaches seem necessary. One of the regulatory approaches that could contribute to reducing the perceived healthiness of ultra-processed products is the inclusion of health warnings or nutritional warnings highlighting excessive content of nutrients associated with non-communicable diseases on the packages of ultra-processed products(Reference Khandpur, Swinburn and Monteiro46,Reference Taillie, Hall and Popkin47) . Recent research has shown that the inclusion of nutritional warnings on food packages can create a salience bias, encouraging people to focus their attention on the negative health consequences of sugar, fat and sodium(Reference Ares, Antúnez and Otterbring48). A similar mechanism has been reported for the inclusion of pictorial warnings on tobacco packages. Such warnings have been reported to make the negative health effects of smoking salient, increasing intention to quit(Reference Brewer, Parada and Hall49). Moreover, experimental research has shown that the inclusion of nutritional warnings can override the positive effect caused by nutrition-related claims and other label features, decreasing perceived healthiness(Reference Nobrega, Ares and Deliza50–Reference Centurión, Machín and Ares52). Another regulatory approach that can contribute to reducing healthiness perception of ultra-processed products is the removal of textual and visual elements conveying health-related associations from packages, such as images of natural foods, nutrient content claims and endorsement logos.
Limitations and strengths of the study
The present research is not free from limitations. First of all, the study was conducted with a small sample of citizens from a single country (Uruguay), suggesting that further research is needed to confirm and extend the findings. However, it should be highlighted that the study involved participants with diverse characteristics in terms of gender, age, educational level and socio-economic status. Considering the qualitative nature of the research and the fact that saturation was reached during the focus group discussions, the findings of the study are expected to be extended to the Uruguayan population. Considering that transnational food companies dominate the global food system(Reference Monteiro, Cannon and Moubarac10,Reference Nestle11) , the insights gained from the discussions are expected to be applicable to the international context.
The qualitative nature of the study was one of its main strengths, as it enabled the identification of a wide range of product characteristics that shape how citizens perceive ultra-processed products. However, results do not provide insights on what characteristics are the main drivers of perceived healthiness. In this sense, further research is needed to assess the relative importance of the identified cues on the perceived healthiness of ultra-processed products.
Conclusions
Results from the present work suggest that the perceived healthiness of several categories of ultra-processed products seems to be largely determined by heuristics based on simple cues, such as package design and brand. On the contrary, objective information related to the nutritional composition of the products does not seem to play a relevant role in shifting healthiness perception. These results stress the need to implement multifaceted strategies that raise consumer awareness of the negative health consequences associated with the consumption of ultra-processed products and reduce perceived healthiness.
Acknowledgements
Acknowledgements: N/A. Financial support: The authors disclose receipt of the following financial support for the research, authorship and/or publication of this article: Comisión Sectorial de Investigación Científica (Universidad de la República, Uruguay), Espacio Interdisciplinario (Universidad de la República, Uruguay) and Instituto Nacional de Alimentación (Ministerio de Desarrollo Social, Uruguay). Conflict of interest: The authors declare no conflict of interest. Authorship: All authors contributed to the development of the research. L.M. moderated the focus groups. G.A., L.M. and L.A. analysed the data. G.A. prepared a first version of the paper, to which all other authors contributed substantially. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects. The experimental protocol was approved by the Ethics Committee of the School of Chemistry of Universidad de la República (Uruguay). Informed consent was obtained from all participants in an online form and formally recorded.




