

Knowledge management sounds superficially like yet another of those topical expressions describing something that has been developed outside medicine and is possibly ill-suited for application within the field, but offering an excuse for yet more change. However, one of the distinguishing features of every profession is that it applies a body of specialist knowledge and skills to a defined purpose. Knowledge in medicine is growing exponentially. In a recent survey of just 22 general practices, the practice guidelines identified weighed 28 kg (Reference Hibble, Kanka and PencheonHibble et al, 1998)! In psychiatry, about 5500 papers which potentially have clinical relevance are published annually. Keeping pace with knowledge as it grows is a major challenge for all clinicians. This is reflected in the National Health Service (NHS) information strategy, which identifies three specific needs of clinicians (NHS Executive, 1998). These are:
-
• fast, reliable and accurate information about patients in their care;
-
• access to knowledge to inform clinical practice;
-
• access to information to underpin evaluation of clinical practice, planning and research, clinical governance and continuing professional development.
All of these include an important element of knowledge management.
Data, information and knowledge
Knowledge is built up from data and information as well as prior knowledge.
Data have no meaning or significance in themselves. Examples include individual mental symptoms shown by a particular patient or items in a computer spreadsheet. Information is data which have meaning because of a relational connection. In other words, information is data which have been processed to be useful. Information aims to provide answers to the questions ‘Who?’, ‘What?’, ‘Where?’ and ‘When?’ It is worth noting that although information is intended to be useful, it is not necessarily so. Merely aggregating data and identifying relationships between variables does not guarantee utility. Knowledge is information to which a process has been applied, which may eventually become expertise (Reference LiebowitzLiebowitz, 2000). It is ‘the collation of information for a particular purpose, intended to be useful’ (Reference Bellinger, Castro and MillsBellinger et al, 1999). Knowledge aims to answer the question ‘How?’ Developing new knowledge from that which already exists to answer the question ‘Why?’ may be defined as understanding. However, while knowledge is a necessary prerequisite for understanding, the availability of appropriate knowledge does not guarantee understanding.
The relationships between data, information and knowledge are summarised in Fig. 1. However, this is not necessarily unidirectional, but is often circular or iterative. For example, individual items in a clinical data-set constitute data. When aggregated, they can yield information, which in turn can be appraised and interpreted to give knowledge. However, designing a clinical data-set includes making a decision about which items are needed and how they should be coded. These decisions are informed by existing knowledge, but they may need revision in the light of new knowledge developed from the use of the data-set. In the same way, reviewing the formulation of an individual patient's presenting problems (knowledge) may lead to a reappraisal of individual symptoms (data).

Fig. 1 Relationships between data, information and knowledge (after Reference Bellinger, Castro and MillsBellinger et al, 1999)
Figure 1 also aims to distinguish knowledge management from data management, information management and information technologies. Information technologies, as the term is used in everyday language, are tools which support the management of data, information and knowledge. They include computer hardware and software, storage, indexing and retrieval systems, and so on. Data management and the technologies available to support this are relatively simple. An example would be a simple spreadsheet. Aggregating and analysing data from such a spreadsheet using statistical software, or bringing data together from different sources using a relational database, illustrate information management. In practice, these technologies clearly overlap. However, this overlap has been exaggerated by conceptual confusion. For example, the main purpose of the NHS strategy defined in Information for Health (NHS Executive, 1998) appears to be to optimise knowledge management, even though the document focuses on information management and does not make a clear distinction between these two areas of activity. The distinction is important because it helps to highlight the central role in health care of methodologies and technologies supporting knowledge management.
Knowledge management
A general definition of knowledge management, adapted from Macintosh (1997), is that it ‘comprises the identification and analysis of available and required knowledge, and the subsequent planning and control of actions to develop knowledge assets so as to fulfil individual and/or organisational objectives’. The processes and outcomes of knowledge management are summarised in Fig. 2.
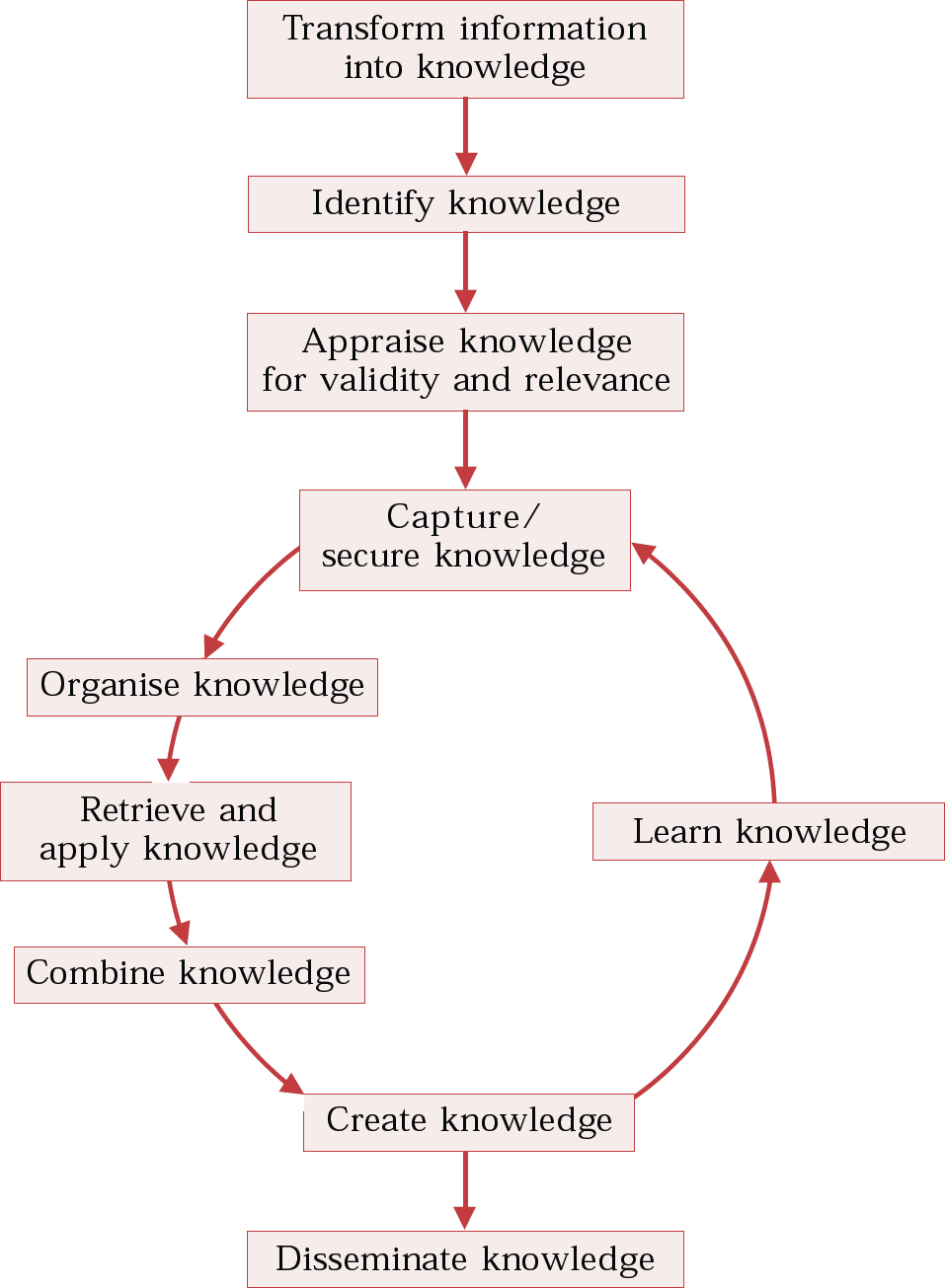
Fig. 2 Elements of knowledge management (after Reference LiebowitzLiebowitz, 2000)
Within psychiatry, knowledge management can be defined as the creation, acquisition, analysis, maintenance and dissemination of knowledge for the benefit of patient care.
The nature of knowledge
To understand the knowledge needs of an individual or an organisation and how these might best be met, it is often helpful to distinguish between different types of knowledge. Knowledge-management experts identify different types, each with its own properties and associated processes (Reference MenziesMenzies, 1999). However, simpler classifications can be very useful.
A distinction is commonly made between tacit and explicit knowledge. Consider the scenario in which a consultant is phoned in the early hours of the morning by the on-call senior house officer (SHO) asking for guidance about risk assessment for someone presenting following an overdose. If the consultant merely elicits the key features of the case that are relevant to risk and then tells the trainee what to do, this would be the application of tacit knowledge. The knowledge rests with the individual in a form which cannot be transferred for use by others. Knowledge gained through personal experience is tacit knowledge. On the other hand, if the consultant reviews the application of the principles of risk assessment in this particular case with the trainee and helps her to form her own judgement, this would be the transfer of explicit knowledge. If staff in the trust concerned had developed guidance notes on risk management of deliberate self-harm, these would also be an example of tacit knowledge, explicitly stated and readily accessible to anyone who requires it. In the literature about knowledge management, it is commonly assumed that in order to use or otherwise manage knowledge, it must be converted, where necessary, from tacit to explicit. This conversion is a major challenge to organisations, especially where expert knowledge is carried by individuals. Although these principles have been identified as pertinent to commercial organisations, they probably also apply to a large extent to medicine in general. They are also applicable in psychiatry, although there may be some exceptions such as some processes in psychotherapy supervision.
It can sometimes help to divide knowledge into that which is superficial and that which is deep. Following a simple management plan dictated by a protocol requires only superficial knowledge. Understanding the principles underlying the protocol requires deeper knowledge.
A distinction between catalogue knowledge, process knowledge and cultural knowledge may also be helpful. Catalogue knowledge is the simplest form and requires the least specialist input into its development. It is possibly the easiest form to measure. An example would be knowledge about a general psychiatry service's access to specialist services, and their relative merits. (Note that a list of addresses and telephone numbers on its own constitutes information rather than knowledge.) Process knowledge is exemplified by clinical practice guidelines, protocols and care pathways. Cultural knowledge relates to the application of the two other types in a specific setting.
These classifications of knowledge are not mutually exclusive. For example, the range of interventions used within the Care Programme Approach (CPA) by a particular community mental health team, which have to some extent been defined by the team's expertise and resources, involves cultural as well as process knowledge. The former will, in most instances, be tacit, while the latter may be explicit to some degree, depending on the extent to which the team follows care pathways or guidelines. If the team is, for example, following prescribing guidelines, the psychiatrist(s) in the team would be expected to have deep knowledge about their contents, while other team members would only need more superficial knowledge.
It becomes apparent that breaking knowledge down into its components may help to identify training as well as information needs. Conversely, by investigating knowledge itself, can we expect to gain a better understanding of its application and management in clinical practice? Knowledge and its properties have been the focus of much attention in philosophy. Other disciplines, notably anthropology, also provide valuable insights into the common features of knowledge applied in different settings (Reference D'AndradeD'Andrade, 1995).
Knowledge management and the individual clinician
The example above suggests that, although few clinicians receive formal training in this area, they have to develop sophisticated knowledge management skills in order to practise effectively. A psychiatric trainee moving from one post to another has to acquire new knowledge, much of it tacit, at all levels: catalogue, process and cultural. It could be speculated that explicitly recognising this as part of clinical practice would not only assist in the development of appropriate training, but also help to provide a better understanding of problems when they occur.
More generally, the need for personal knowledge management skills underlies the widespread acknowledgement that now, more than ever before, it is impossible for a clinician to acquire sufficient knowledge during training to equip him or her for the duration of a professional career. This is reflected not only in the importance attached to continuing professional development, but also in the change in emphasis during undergraduate medical training from the acquisition of facts to the development of skills needed for lifelong learning.
Perhaps the most obvious application of individual knowledge management is evidence-based practice. Evidence-based medicine has been defined as a process of lifelong self-directed learning in which caring for our patients creates the need for clinically important information (Reference Sackett, Richardson and RosenbergSackett et al, 1997). The process of evidence-based practice involves several steps (Box 1) which closely mirror those identified as contributing to knowledge management. This is hardly surprising, since evidence-based practice is, in effect, a systematic method of identifying and managing specific gaps in knowledge.
Box 1 Components of evidence-based practice (after Reference Sackett, Richardson and RosenbergSackett et al, 1997)
Convert information needs into answerable questions
Efficiently find the best evidence available to answer the questions
Critically appraise the evidence for its validity and its applicability to clinical practice
Apply the results, where appropriate, to the original question
Evaluate the outcome
The application of evidence-based practice to individual patients offers two important lessons about knowledge management. First, a great deal can be learned from individual cases. Second, whether or not knowledge is gained in this way depends heavily on the skills and processes applied. If inadequate attention is paid to these, commonly little or no knowledge is gained. For example, before conducting a literature search, the question must be formulated in a way which will optimise the chances of finding relevant material (the so-called four-part question) (Reference Richardson, Wilson and NishikawaRichardson et al, 1995). This is a specific skill which can be acquired by training and practice. Using predefined search terms or filters can also considerably increase the efficiency and productivity of the search. In essence, these filters are technologies supporting the search for evidence. Without these skills and technologies, literature searching often proves unproductive and, in some instances, completely unsuccessful. Other methodologies are also available to enhance learning from single cases (Box 2).
Table 1 Some resources for knowledge management and related topics on the internet
| Knowledge management | |
| The Knowledge Management Center | http://www.kmresource.com/exp.htm |
| Sveiby Knowledge Management Library | http://www.sveiby.com.au |
| Virtual Library on Knowledge Management | http://www.brint.com/km/ |
| Open Directory – Reference: Knowledge Management | http://dmoz.org/Reference/Knowledge_Management |
| Financial Times – Knowledge Management | http://www.ft.com/ftit/bsskm.htm |
| Information management and technology | |
| NHS Information Authority | http://www.nhsia.nhs.uk |
| Information for Health | http://www.nhsia.nhs.uk/def/pages/info4health/contents.asp |
| Working Together for Health Information (NHS Executive) | http://www.nhsia.nhs.uk/ppt/hc2000/etd.ppt |
| Introduction to Health Informatics for Hospital Doctors | http://www.schin.ncl.ac.uk/hicourse |
| National electronic Library for Health | http://www.nelh.nhs.uk |
Box 2 Examples of methodologies to enhance learning from single cases

| Technique | Comments | Reference |
|---|---|---|
| Clinical supervision | The most widely used methodology at postgraduate level, but not always systematically applied | Kilminster & Jolly (2000) |
| Log books or ‘progress files’ | Can be effective in enhancing learning, including self-reflection | Pee et al (2000) |
| Critical incident analysis | Developed as a method of acquiring specific knowledge and skills - applied to date in other specialities (e.g. anaesthetics) more than in psychiatry | Flanagan (1954) |
| Case-based reasoning | Application to current instances of precedents from known cases - developed by information technologists but not yet widely applied | Watson (1999) |
Expert systems to support decision-making are another example of knowledge management which have found application in other medical specialities more than in psychiatry. A decision-making algorithm is developed which takes account of the key independent variables. The clinician enters the values of the independent variables for the patient concerned and the algorithm is applied to present the best decision. Such expert systems would be extremely useful, for example, in the prediction of risk, and it is interesting that no such system is yet in common use. A key reason is that, to date, it has not proved possible to develop reliable mathematical models for important decisions, such as the probability of a patient harming someone else. This may be because the models required are extremely complex. A more radical view is that common assumptions regarding decision-making, which also underlie the development of the algorithms, are actually wrong and cannot adequately reflect real-life decision-making. Decision-making is usually modelled using Bayes’ Theorem, but there is evidence that, in real life, both clinicians and lay people tend to make at least some decisions using simpler mechanisms (Reference Gigerenzer and ToddGigerenzer et al, 1999).
Why case-based knowledge management is under-utilised
As with knowledge management in general, evidence-based medicine can be optimally applied only if it is integrated into everyday clinical practice as fully as possible. Many clinicians who have received no training in critical appraisal or the other components of evidence-based practice (Box 1) are unaware that they lack the requisite skills. Without training, their skills in this area are often not comprehensive and even when the individual makes the effort to search for and appraise evidence, lack of success and/or the excessive time taken rapidly discourage further progress. Some clinicians are wary of admitting to patients that they have gaps in their knowledge. Personal experience suggests that, far from being disconcerted, patients actually value the fact that their doctor is making the effort to seek the latest and most robust information available to contribute to their management. Telling patients that you are going to do this also acts as a powerful incentive to follow the action through, because they will usually want to know the outcome of the search at their next appointment.
Knowledge acquired from individual cases is subject to numerous pitfalls, which can discourage clinicians from pursuing this further. Perhaps the most striking example in psychiatry is the knowledge gained from independent inquiries into homicides, suicides and other serious incidents. Clinicians, like lay people, are susceptible to substantial bias in the retrospective interpretation of events. When examining the origins of a serious incident, there is a common tendency to assume that the incident was inevitable, rather than to ask the clinically pertinent question: how likely was it that this incident would occur, based on prior available information plus existing knowledge? This error, which can sometimes have very wide-ranging repercussions, is due to a specific inadequacy in knowledge management skills. Much more common is the tendency shown by some experienced clinicians to apply anecdotal evidence from past cases to current clinical problems. The problem here, as often also applies in independent inquiries, is that the most memorable cases are often the most atypical, and thus the least likely to yield knowledge that can be generalised.
Perhaps the most challenging problem facing clinicians trying to learn from individual cases is to disengage the process of learning from mistakes, from the admission of failure. This applies to other professions as much as to doctors (Reference ArgyrisArgyris, 1998). Solving this problem requires organisational as well as individual changes and it is discussed below.
Knowledge management in organisations
Many types of knowledge can help organisations fulfil their objectives more successfully. One problem with the current enthusiasm for research evidence is that randomised controlled trials, rather than being perceived as the gold standard among a host of different types of valid evidence, are sometimes considered to be the only acceptable form of evidence. Virtually all the information collected by an organisation may be useful in developing knowledge. For example, practice-based evidence, derived from systematic collection of comprehensive outcome data, is likely to contribute to the development of psychotherapy services (Reference Margison, Barkham and EvansMargison et al, 2000) as well as other mental health services.
What often works against the productive collection and application of clinical information in many NHS trusts is that their information systems are poorly integrated with clinical practice. Either the information system has been designed to meet very limited objectives (such as gathering purely administrative data) or it functions in parallel with routine clinical practice rather than being properly integrated with it. However, it follows that many clinicians are not as familiar as they should be with the sources of information available to them as starting points for knowledge. An essential prerequisite of knowledge management within an organisation is to audit the way in which information is processed (Box 3). Beyond this, a set of factors can be defined which describe how effectively an organisation manages its knowledge. Numerous descriptions of these factors are available on the internet and in ‘hard copy’ form. Box 4 offers one example. These factors can be grouped into values, behaviours and processes supported by appropriate technologies.
Box 3 Auditing information management in an organisation (Reference LiebowitzLiebowitz, 2000)
Identify the information needs of the organisation and of individuals working in it
Identify information created within the organisation and attempt to assess its value
Identify expertise and knowledge assets
Identify information gaps
Review current use of internal and external information sources
Map information flows and identify bottlenecks
Develop a knowledge map of the organisation, indicating appropriate connections
Box 4 Tests of organisational knowledge management (Reference WebbWebb, 1998)
Can we transfer knowledge easily to new staff?
Is ours an information/knowledge-sharing culture?
Do we know what and where our knowledge assets are?
Is knowledge organised and easy to find?
Do we capture and share best practice?
Do we learn from mistakes?
Do we reward knowledge-sharing?
Are we exploiting knowledge effectively and strategically?
Does our knowledge walk out of the door as staff leave?
Learning organisations
It could be argued that knowledge only realises its true value when it is integrated into learning by an individual, a team or an organisation. Learning organisations possess two characteristics (Reference GarvinGarvin, 1998). First, the organisation is skilled at creating, acquiring and transferring knowledge. In other words, it has effective knowledge management. Second, it can demonstrate changes in its behaviour in the light of new knowledge. The same two sets of characteristics apply equally to learning individuals or teams. Of these characteristics, the absolute prerequisite is the potential to show change in behaviour. Learning can be exhibited without effective knowledge management, but then it is likely to be haphazard. In practice, knowledge management and learning organisations should be closely linked.
Different levels of learning can be differentiated. At the basic level, an audit might reveal unsatisfactory performance against predefined standards, and practice is consequently changed in an attempt to improve performance. Because it resembles a simple feedback loop, this is sometimes called single-loop learning (Reference ArgyrisArgyris, 1998). Using new knowledge to develop a totally new practice reflects a more sophisticated form of learning. Organisations will also find it helpful to examine when and how they can achieve optimal learning conditions, and what barriers exist within the organisation that impede learning. This is termed meta-learning (Reference Davies and NutleyDavies & Nutley, 2000).
In essence, a learning organisation is one that values knowledge and recognises it as central to organisational development. Individuals‘ knowledge is nurtured, but it is understood that the organisation should be able to develop this into corporate knowledge.
Barriers to applying knowledge management
Although failures in knowledge management are commonly blamed on inadequate resources, the main barrier is likely to be the culture within an organisation, with other barriers commonly cited being lack of time and lack of ownership of the problem (Reference WebbWebb, 1998). The cultural values which underpin learning organisations (Reference Davies and NutleyDavies & Nutley, 2000) are precisely those likely to yield positive answers to the questions in Box 4. These include trust, openness and a tolerance of mistakes. These values need to be reflected throughout any organisation. Within NHS trusts, it is particularly important that clinical teams share these values, since most work is done within teams and the need for knowledge and learning is particularly important within these groups. Very few clinical teams or organisations have come close to the successful development of the ‘no-blame’ culture which is the cornerstone of the learning organisation and hence also of the successful application of knowledge management. Having a chief knowledge officer within an organisation (Reference GrayGray, 1998) may well be very helpful in ensuring the development of the processes and technologies necessary to support knowledge management. Although this is certainly a prerequisite for effective knowledge management, on its own it is unlikely to ensure that the organisation uses this skill to its full advantage.
Auditing knowledge management and organisational learning
Any audit must begin with a clear conceptualisation of the process to be assessed and the generation of measurable (usually operationalised) outcomes based on defined standards. The previous discussion of knowledge may assist in conceptualisation, and many of the points in Boxes 3 and 4 can be put into operation, allowing them to be audited. At present, very few NHS trusts are likely to score well in such audits. However, this is perhaps not surprising, given that for the vast majority, it appears unlikely that they have attempted to evaluate their working practices in terms of knowledge management, or even as learning organisations.
A simple audit for an NHS trust (or other organisation) wishing to examine the extent to which it has developed a learning environment is to ask staff members to identify one change in practice in the preceding 12 months that resulted from new knowledge, and to summarise that knowledge. If the audit also asked staff to identify the sources of the knowledge which proved useful, the data collected would yield information about the trust's knowledge management resources, going some way towards answering the points in Box 3.
Clinical governance: the context of knowledge management
All health care staff are keenly interested in providing the best care for their patients. Clinical governance represents a systematic approach to fulfilling this aim. As with knowledge management, clinical governance needs to be integrated into clinical work at every level. With piecemeal development there is the risk that conspicuous gaps will be left and idiosyncratic policies and procedures will develop. It is impossible for a trust or clinical service to meet the objectives of clinical governance without valid and reliable information and effective knowledge management. To optimise the effectiveness of patient care, including responding as necessary to new developments in health care and the changing environment in which it operates, an organisation must have a learning culture plus good knowledge management. An NHS trust which can endorse the points in Boxes 3 and 4 will have come a long way towards fulfilling its clinical governance objectives. Conversely, it is difficult to see how clinical governance could be pursued effectively in the absence of well-developed knowledge management systems. It could even be argued that clinical governance is no more than a specific application of knowledge management. Although this may be a provocative view, seeing clinical governance in terms of knowledge management helps to stress the vital importance of appropriate methodologies and technologies, rather than seeing these as luxuries or ‘add-ons’. As it has been expressed by one knowledge management expert, ‘knowledge management is expensive … but so is stupidity’ (Reference DavenportDavenport, 1998).
A personal reflection
Preparing this paper has itself been a useful personal experience of knowledge management. Much of the literature I found was from unfamiliar sources and it was striking that, despite the clear importance of knowledge management to medicine, most of the literature referred to business settings. In appraising this literature, I found it very difficult to apply the standard methods used in evidence-based medicine. Two main factors influenced the decisions about what to include in the paper. First, some concepts and/or authors were cited in multiple sources, suggesting that they had been appraised as useful and relevant. Second, and even more important, it was possible to identify examples from psychiatric practice, indicating that they at least had face value. This process has certainly given me new knowledge. In preparing this paper, I aimed to determine how far I could gain access to sources of appropriate information and knowledge without leaving my desk. This paper has been written entirely in this way. I identified relevant books from Amazon (www.amazon.co.uk), an internet source which includes commentaries on their contents, and then searched the on-line library catalogues of the British Medical Association (http://www.bma.org.uk/ap.nsf/content/_Hub+library) and the Royal Society of Medicine (http://rsm-hp.roysocmed.ac.uk/uhtbin/cgisirsi/) to check their availability and arrange to borrow them. All the journal articles cited (and many more) were also accessible on the internet in full-text format (including Advances in Psychiatric Treatment, at http//apt.rcpsych.org, and The British Journal of Psychiatry, at http//bjp.rcpsych.org), demonstrating the value of this resource. Several journals are currently available free of charge in full-text form on the internet. A more comprehensive list of on-line medical journals can be found at http://www.freemedicaljournals.com. I had access to a wider range of journals through an academic library than through NHS sources, highlighting the continuing need to strive to make such resources more widely available within the NHS. Websites on knowledge management and information management and technology are listed in Table 1.
Multiple choice questions
-
1. Knowledge includes:
-
a aggregated data
-
b disaggregated information
-
c all available information
-
d appraised information
-
e personal experience.
-
-
2. Knowledge management:
-
a is synonymous with information management
-
b refers to a particular application of information technology
-
c is predominantly an organisational activity
-
d is mostly dependent on valid and reliable data processing
-
e is usually difficult to audit.
-
-
3. The following are essential features of effective knowledge management:
-
a appraising information
-
b having ready access to a library
-
c having experts available who can undertake this task for the organisation
-
d appraising existing knowledge
-
e disseminating knowledge.
-
-
4. The following statements are correct:
-
a tacit knowledge is difficult to disseminate
-
b within a clinical team, where knowledge is required on a particular topic, all members should strive for deep rather than superficial knowledge
-
c process knowledge is always explicit
-
d cultural knowledge is more important than process knowledge
-
e clinical practice guidelines are examples of explicit process knowledge.
-
-
5. In an organisation effectively geared towards learning:
-
a there are mechanisms to transfer knowledge from individuals to the organisation
-
b there will usually be evidence of effective knowledge management
-
c there is always someone senior within the organisation in charge of knowledge management
-
d there will usually be evidence of effective sharing and dissemination of knowledge
-
e the importance and value of knowledge is shared by all staff, not just those in senior positions.
-
MCQ answers
| 1 | 2 | 3 | 4 | 5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| a | T | a | F | a | T | a | T | a | T |
| b | F | b | F | b | F | b | F | b | T |
| c | F | c | F | c | F | c | F | c | F |
| d | T | d | F | d | T | d | F | d | T |
| e | T | e | F | e | T | e | T | e | T |





eLetters
No eLetters have been published for this article.