



Introduction
Work stress is a serious occupational health and safety (OHS) issue for human workers and can lead to psychological distress and, in the longer term, psychological and physical disability. Under these conditions, the capacity to remain engaged at work is compromised and serious social costs can ensue (due to family breakdown, suicide, healthcare expenditure, and workers compensation). There are large costs to employers, too, primarily due to a loss in working hours and productivity, globally estimated to cost from USD 221.13 million to USD 187 billion per year (Hassard et al Reference Hassard, Teoh, Visockaite, Dewe and Cox2018). In Australia alone, from 2021 to 2022, workers psychological health compensation claims rose by 43% and 9.2% of serious claims were related to psychological health, costing AUD 58,000 per claim (Safe Work Australia, 2023). Most economic analyses of psychological health at work have emerged from macro-economics, but much less focused on the micro-economics of interest to corporations. Yet providing economic estimates at the enterprise level could provide the impetus for bottom-up progress with flow-on social effects. Providing economic evidence concerning poor OHS could provide a ground-up stimulus for organisational action to improve OHS that could be used in combination with national policy approaches. Moreover, focusing on leading rather than lag indicators (e.g., the worker’s compensation claims) is optimal to drive OHS change.
In OHS terms, psychosocial risk factors are social psychological factors at work such as high workload, low job control, poor supervisor support, and workplace bullying that cause psychological distress. To cope with psychosocial risks requires physiological and psychological effort from workers, which taxes bodily reserves, and can lead to distress and disease. These OHS risks are readily framed using an industrial relations (IR) perspective (Potter et al Reference Potter, Dollard, Lerouge, Jain, Leka and Cefaliello2024; Quinlan Reference Quinlan2023). Evidence suggest that psychosocial safety climate (PSC) is a leading indicator of these psychosocial risks (Dollard and Bakker Reference Dollard and Bakker2010, Loh et al Reference Loh, Zadow, Dollard and Theorell2020). PSC fundamentally concerns the conflict between labour and management and whether worker psychological health is valued versus productivity imperatives (Dollard and Bakker Reference Dollard and Bakker2010). Both objectives, that is, worker health and productivity, could be achieved, to an extent, if this lack of valuation was exemplified in economic terms. In this study, we quantify, in economic terms, the link between PSC and two common outcomes to stressful contexts, namely turnover and sickness absence, an issue of great concern in the post-COVID era, providing evidence at the local enterprise level for costly poor OHS consequences.
PSC in context
PSC concerns the corporate climate in relation to the organisation’s OHS safety system for worker psychological health (Dollard and Bakker Reference Dollard and Bakker2010). Corporate PSC can be understood in a wider context of regulation, policy, and unions. In recent research, national policy approaches to worker psychological health, rated by experts, were positively linked to a proxy measure of organisational PSC assessed in the European Survey of Enterprises on New and Emerging Risks (ESENER) survey, all data aggregated across 22 European countries (Potter et al Reference Potter, Dollard, Lerouge, Jain, Leka and Cefaliello2024). Over and above national policy approaches, union density was also associated with PSC, indicating that collective social action is likely important not only for the development of policy but also implementation of policy at the organisational level. The role of unions was underscored in previous research where Dollard and Neser (Reference Dollard and Neser2013) found across 31 European countries that the most important factors explaining gross domestic product (GDP) and worker self-reported health were two forms of labour protection namely macro union density (and corresponding social welfare regimes) and PSC.
At the enterprise level, PSC reflects employee perceptions of ‘policies, practices, and procedures in relation to the protection of worker psychological health’ (Dollard and Bakker Reference Dollard and Bakker2010, p.180). PSC theory proposes four functional domains: (1) management commitment to stress prevention; (2) management priority for employee psychological health and safety versus a focus on productivity and profits; (3) organisational communication throughout the organisation regarding workplace issues that may affect employee psychological health; and (4) organisational participation, consultation, and involvement of all stakeholders (i.e., employees, managers, unions, and health and safety representatives), to address workplace issues that threaten worker psychological health and wellbeing (Hall et al Reference Hall, Dollard and Coward2010; Loh et al Reference Loh, Zadow, Dollard and Theorell2020). PSC embodies the process of risk management reflecting the organisational system in addressing psychosocial risks. Knowing about how an organisation performs in these domains provides insights into how well managed psychosocial risks are, and whether they are or could be prevented. In a high PSC work context, a desirable situation, workers likely face manageable demands with adequate resources. Empirical evidence shows that PSC is ‘a cause of the causes’ (Dollard and Bakker Reference Dollard and Bakker2010), a leading indicator of task-level job demands and job resources (including job control, workload, and negative social relationships) and worker’s psychological health (Amoadu et al Reference Amoadu, Ansah and Sarfo2023; Zadow et al Reference Zadow, Dollard, Parker, Storey, Dollard, Dormann and Idris2019), as well as psychosocial safety behaviours (Weaver et al Reference Weaver, Kirk-Brown, Goodwin and Oxley2024). An organisation with high PSC is likely an effective organisation with high performance, where workers are highly engaged and psychologically healthy, and there are less costs associated with worker’s compensation, sickness absence, and turnover intention (Bailey et al Reference Bailey, Dollard, McLinton and Richards2015a; Bentley et al Reference Bentley, Teo, Nguyen, Blackwood, Catley, Gardner and Port2021).
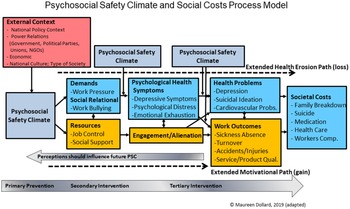
Given that PSC affects workers’ psychological health through many causal pathways (through different psychosocial risk factors), it is expected that PSC has a large role to play in modelling economic costs (Figure 1). The significance of PSC was shown in recent prospective longitudinal research (Dollard et al Reference Dollard, Loh, Becher, Neser, Richter, Zadow, Afsharian and Potter2024) showing that organisations with low PSC reported 160% more workdays off on workers compensation due to injury or illness, compared to organisations with high PSC. Employees in organisations with good PSC were quicker to return to work (Dollard et al Reference Dollard, Loh, Becher, Neser, Richter, Zadow, Afsharian and Potter2024). Again, this research is across organisations rather than within an organisation.
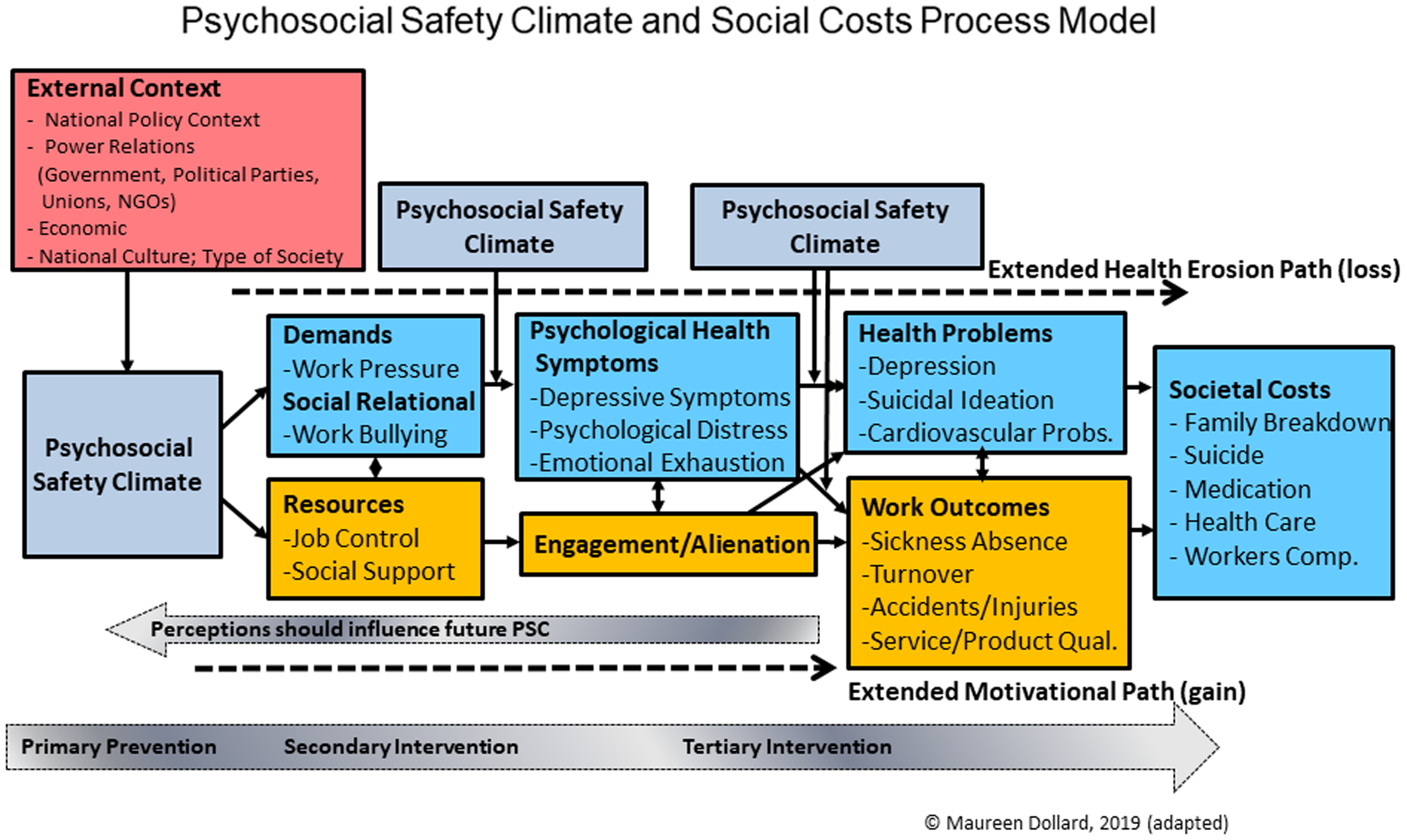
Figure 1. The theoretical framework of PSC and social costs.
In the current study, we aim to further expand the literature of PSC beyond psychological health outcomes to link to economic costs through the loss of working hours and personnels. We focus on costs related to two forms of labour loss, sickness absence and turnover. Costs associated with absence include lost days of labour through ill health, personal sickness, and work-related injuries. Costs associated with turnover include key person loss, recruiting new personnel, training, and time to replace employees. Using employees’ reported PSC and organisational registered data, we examine the relationship of PSC with sickness absence and turnover. We also conducted a cost analysis. Although organisations should move to improve PSC on moral grounds, providing insights into the extent of economic costs related to psychosocial factors could serve to enlighten and motivate organisations to focus on improving leading indicators.
PSC relationship to turnover and sickness absence
The influence of PSC on workers’ health outcomes is evident in both cross-sectional and longitudinal studies (see Zadow et al Reference Zadow, Dollard, Parker, Storey, Dollard, Dormann and Idris2019 for review). In line with the dual pathway of the PSC-extended Job Demands-Resources (JD-R) model (Dollard and Bakker Reference Dollard and Bakker2010), through the ‘health-erosion’ pathway, PSC negatively predicts demands, which in turn erode health status, and through the ‘motivational’ pathway, PSC positively relates to job resources, that in turn relate to work engagement. Through the health erosion pathway, workers in good PSC environments are less exhausted (McLinton et al Reference McLinton, Dollard and Tuckey2018). In contrary, workers in low PSC workplaces had significantly higher sickness absence and presenteeism compared to high PSC environments. This is because those suffering from psychological distress have depleted energy and require more sick days to preserve and/or recover their psychological state.Reference Becher and Dollard In addition, psychological health is closely related to physical health (Koban et al Reference Koban, Gianaros, Kober and Wager2021; Pressmen and Cohen Reference Pressman and Cohen2005; Salovey et al Reference Salovey, Rothman, Detweiler and Steward2000). Employees who are less mentally healthy are also likely to experience injuries and accidents (Kirschenbaum et al Reference Kirschenbaum, Oigenblic and Goldberg2000; Zadow et al Reference Zadow, Dollard, McLinton, Lawrence and Tuckey2017). Research showed that they took 43% more sick days per month and had a 72% higher performance loss at work, costing employers AUD 1887 per employee per year (Becher and Dollard Reference Becher and Dollard2016). Likewise, another study reported that participants in high-risk PSC work groups take 93% more unplanned leave than low-risk PSC groups (Dollard and Bailey Reference Dollard, Bailey, Dollard, Dormann and Idris2019).
By contrast, a high PSC organisation is expected to attract talent and be appealing to employees to stay and work longer for the organisation. Previous studies found that high levels of PSC fulfil human innate needs by providing them a sense of belongingness, autonomy, and competence (Deci and Ryan Reference Deci and Ryan2000; Huyghebaert et al Reference Huyghebaert, Gillet, Fernet, Lahiani and Fouquereau2018). Workers with innate need fulfilment are more psychologically healthy and more engaged. They are more likely to reciprocate the favourable treatment from organisations with pro-organisation behaviours, attitudes, and actions (i.e., Social Exchange Theory, Blau Reference Blau1964). However, if employees are dissatisfied with work and perceive that their efforts outweigh the gains, employees may start to withdraw and finally turnover (Geurts et al Reference Geurts, Schaufeli and Rutte1999). Research has found the role of PSC on workers’ turnover intention (Mansour and Azeem, Reference Mansour and Azeem2024). Hence, we expect that PSC will link to objective measures of sickness absence and turnover.
The cost of sickness absence and turnover attributable to low PSC
To calculate the cost attributable of sickness absence and turnover to poor OHS (exemplified in our study as PSC), it is necessary to calculate the risk level of exposure and compare it to those unexposed w orkers (McTernan et al Reference McTernan, Dollard and LaMontagne2013; Russo et al Reference Russo, Ronchetti, Di Tecco, Valenti, Jain, Mennini and Iavicoli2021). In the case of psychosocial risks, it is nearly impossible to have zero exposure, alternatively, a low level of psychosocial risk could reflect a low exposure. In the epidemiology and occupational safety fields, therefore risk levels are often used to assist researchers and practitioners in calculating the proportion of disease exposure or hazards exposure. Using this state of science, we used risk levels to estimate cost. We used established benchmarks proposed by Bailey et al (Reference Bailey, Dollard, McLinton and Richards2015 Reference Bailey, Dollard and Richardsb) and Dormann et al (Reference Dormann, Owen, Dollard and Guthier2018) who estimated the risk of exposure to job strain and depression with a national Australian sample from specific PSC thresholds. In estimating cost savings, we assume that PSC levels can improve, and this has been verified in a number of studies (Berglund et al Reference Berglund, Kombeiz and Dollard2024; Dollard and Bailey Reference Dollard and Bailey2021).
Methodology
Research design and sample
A study was conducted in a multinational company with a total workforce of 4437 employees in year 2019. At Time 1 (T1), a survey was distributed by the in-house personnel to collect information on PSC. A total of 1346 workers returned the survey. One year later, at Time 2 (T2), registered sickness absence and turnover data were provided by the organisation. Data matching was completed in-house by a data expert and deidentified. After omitting missing values, a total of 617 longitudinal matched responses were used to analyse sickness absence. We used all T1 available information for voluntary turnover (omitted those who were retrenched or dismissed). Ethics approval was obtained from the authors’ university Human Research Ethics Committee (approval number: 203691). Informed consent was provided by the participants to match their survey responses to company registered data (Figure 2).

Figure 2. Data collection process.
Among the 1346 workers, 49.6% were female, 87.7% were permanent workers, mostly aged between 30 and 39 years, 22.7% had worked at least one year in the organisation, and 18.4% worked more than 5 years. Around 50% of respondents worked in New Zealand, 22.7% in Australia, 10.5% in the United Kingdom, and 10.3% in the United States. Others worked in either Canada, Hong Kong, Singapore, or South Africa.
Measures
PSC was assessed by using 12 items of the PSC-12 scale (Hall et al Reference Hall, Dollard and Coward2010). An example of item is ‘Psychological well-being of staff is a priority for this organisation’. Responses ranged from 1 (strongly disagree) to 5 (strongly agree). Cronbach’s alpha in this study was α = 0.93.
Sickness absence was assessed using company registered data, assessed in days off taken due to sickness over the 12 months since the T1 survey.
Turnover was assessed by determining whether the respondents had voluntarily left the organisation at Time 2 (0 = stay; 1 = left), not due to forced resignation nor expiry of employment contract. More information about the actual reasons of employment termination can be found in the Appendix. One-way analysis of variance suggested there was no substantial differences on the levels of PSC across the groups (F [11] = 1.338, p >.05).
Analysis procedures
We conducted the analysis using IBM’s SPSS software. To test the impact of PSC on the outcomes, linear regression was used to test the relationship between PSC and future sickness absence, while binomial logistic regression was used to run a model with turnover as the outcome. For sickness absence which is a continuous variable, we specified a hierarchical linear regression model. First, we estimated the baseline model by regressing sickness absence T2 on PSC at T1, without controlling for individual demographic variables. Then in the next step, we extended the model by including control variables, including age, gender, and leadership position, as well as the sickness absence at T1. For turnover, as a categorical variable, we ran a logistic regression model computing the adjusted odds ratios with PSC T1 as the predictor and then by including age, gender, and leadership position as the control variables. In Table 2, we report the results of the final model.
Table 1. Descriptives, Cronbach’s alpha, and Spearman’s correlations of studied variables
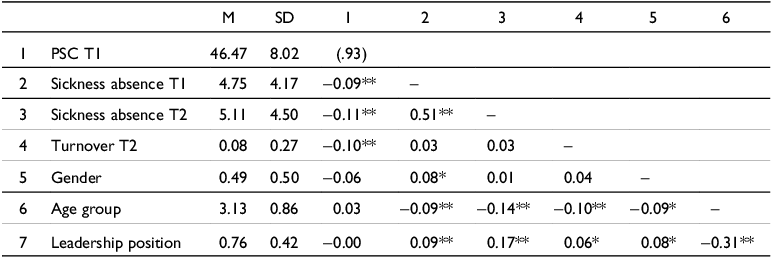
Note. N = 1346 for T1, N = 617 for T2. Missing data were pairwise deleted. PSC = psychosocial safety climate; SD = standard deviation. Values in bracket in diagonal are Cronbach’s alpha. For gender, 0 = male, 1 = female; for leadership position, 0 = non-leader; 1 = leader. * p < .01; ** p < .001.
Table 2. Linear regression analysis of PSC T1 on sickness absence T2 and logistic regression analysis of PSC T1 on turnover T2

Note. N = 617 for sickness absence, N = 1268 for turnover. PSC = psychosocial safety climate; B = unstandardised beta; β = standardised beta; SE = standard error, CI = confidence interval, LL = lower level, UL = upper level; aOR = adjusted odd ratios. * p < .05; ** p < .01; *** p < .001.
Cost estimation
To estimate the cost associated with poor PSC, we used the threshold previously established by PSC scholars (Bailey et al Reference Bailey, Dollard and Richards2015b, Dormann et al Reference Dormann, Owen, Dollard and Guthier2018), defining four risk groups (12.00–26.00 = very low PSC; 26.01 – 37.00 = low PSC, 37.01–40.99 = medium PSC; 41–60 = high PSC). Next, we followed the estimation method in Dollard and Bailey (Reference Dollard, Bailey, Dollard, Dormann and Idris2019). The cost of sickness absence was calculated using average sickness absence multiplied by the average wage of employees of the participatory organisation (NZD 494.23 per day, as provided by the organisation) and the proportion of individuals in the risk-level group. The salary of each individual was not available due to privacy concerns, and we were only provided the average as a proxy. According to the estimate provided by the participating organisation, the cost of replacing a turnover employee was estimated at 33% of their annual salary, that is, NZD 42,405 (≈USD 26,965.34). We converted the currency using an average rate in year 2022 of 1 NZD = 0.6359 USD, to ease comparison with other literature. The saved cost of improving PSC was calculated by assuming that individuals in the very low, low, and medium PSC category, through attention to improvements in the PSC domains, could theoretically be moved to the high PSC category and report similar sickness absence and turnover rates as the high PSC category (this allows for a ‘healthy rate’ of sickness absence and turnover in the total work population). We then estimated a new cost using the average sickness absence cost and turnover rate of the high PSC group with the number of people currently in the low PSC group. Next, we calculated the difference between the total cost of sickness absence and turnover and the newly estimated cost to estimate savings.
Results
Table 1 shows the correlation matrix of all variables indicating. Spearman’s bivariate correlations show that PSC T1 was negatively related to sickness absence T1 and T2, and turnover T2. Regression results are shown in Table 2. For sickness absence, using a matched sample of 617 responses, the regression model shows that PSC T1 was negatively related to sickness absence T2 (standardised coefficient β = −.10, B = −0.06, SE = 0.01, p <.001). This means that a unit increase in PSC results in a 10% reduction in sickness absence over a year. This effect remained substantial even after accounting for the variance attributable to individuals’ demographic and job position, as well as the previous health status of the individual (i.e., sickness absence at T1). This suggests that a high level of PSC is useful in protecting workers from physical and/or psychological ill health.
A binomial logistic regression was run for 1268 respondents after removing those with missing data and those who were terminated involuntarily or due to the end of their contract. The result suggests that PSC could reduce turnover one year later (B = -0.03, SE = 0.01, p <.05). Adjusted odd ratio shows that a unit increase in PSC would reduce 3% of the chance to leave the organisation. In sum, as expect PSC was related to objective measures of future sickness absence and turnover.
Estimated cost of sickness absence and saved cost
As shown in Table 3, the total of sickness absence cost was estimated at USD 9.2 million a year. From T1 to T2, an average of 6.18 sick days were taken for employees with high PSC (PSC ≥ 41), which increased to 8.39 days at high-risk PSC levels (PSC ≤ 26) (Figure 3).
Table 3. Cost estimation of sickness absence and turnover due to low PSC and the related saved cost
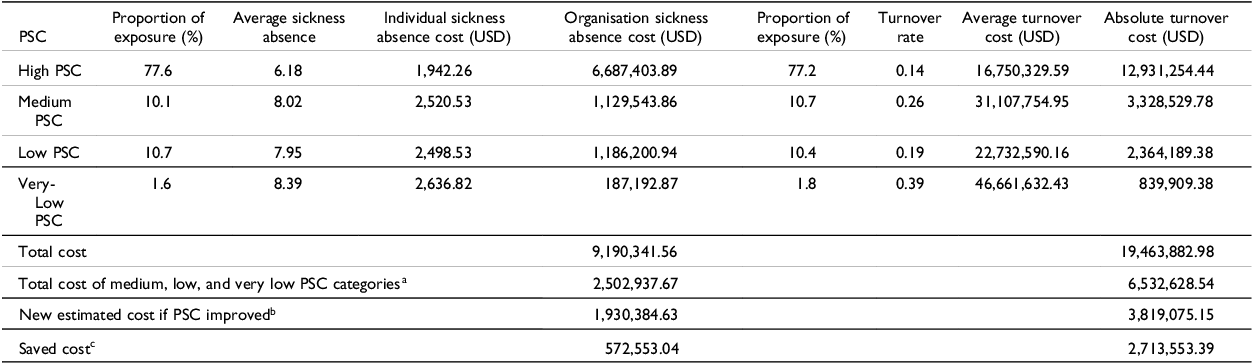
Note. All costs at USD.
a The sum of cost at medium, low, and very low PSC; bthis value is calculated by assuming individuals in the very low, low, and medium PSC category are now moved to high PSC category and reporting the similar sickness absence and turnover rate as in high PSC category; cthe differences between a and b.
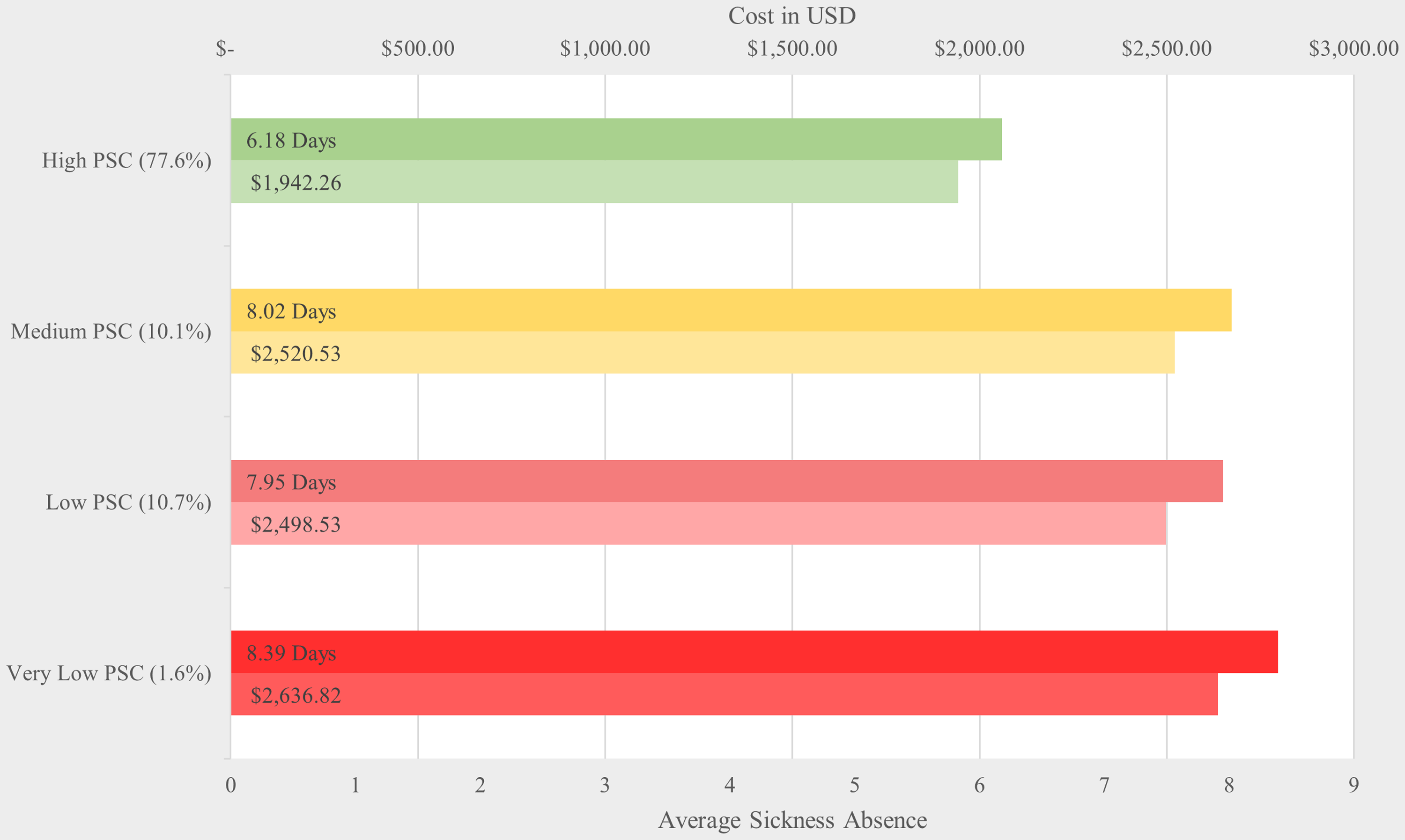
Figure 3. The average days and individual cost of sickness absence at different levels of PSC.
When PSC is lower than 41, the total organisation annual cost of sickness absence was USD 2.5 million. Savings in sickness absence would be achieved by moving those employees in the very low, low, and medium PSC categories to the high PSC category. Theorising those individuals who reported low PSC in the current data (n=994) are now experiencing high PSC and have better health, using the figure of 6.18 days (instead of 8.39), the new estimated cost is USD 1.9 million (994 x USD 1,942.26). This results in savings of USD 0.6 million per year, whilst allowing an average of 6.18 days sickness absence per person in a year.
Estimated cost of turnover and saved cost
The turnover rate for the category of high PSC was 14%, and this rate increased to 39% for the very-low PSC level. Using the organisation’s total population number (N = 4437), and assuming the same turnover rate for the entire organisation, the average turnover cost for 14% × 4437 individuals × USD 26,965.34 is USD 16.7 million if everyone reported a high level of PSC. The cost increased tremendously to USD 46.7 million if the turnover rate is 39% as reported for those at very-low level of PSC (Figure 4). However, to avoid overestimating the cost, it is necessary to consider the risk proportion in estimating an absolute cost. Using the estimated number of employees who left the company and had reported high PSC, that is, 479 (4437 × 77.2% × 14%), the absolute cost of turnover per year for this group was USD 12.9 million. For the rest of the PSC level was USD 6.5 million. Moving all other employees to high PSC will result in an estimated cost of USD 3.8 million (142 × USD 26,965.34) – thereby saving a total of USD 2.7 million with an estimated 14% turnover rate (the turnover rate for high PSC).
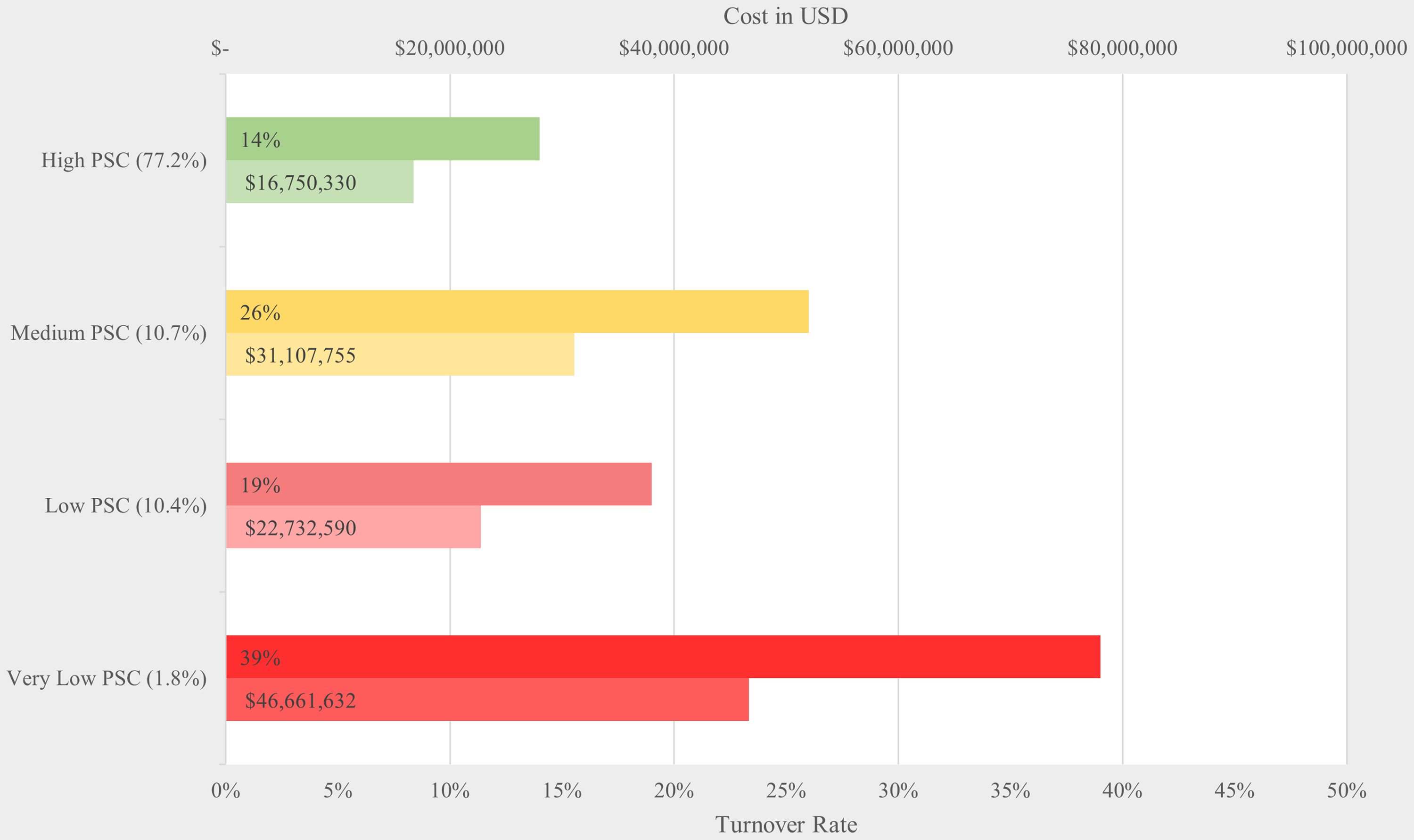
Figure 4. The rate and average organisational cost of turnover at different levels of PSC.
Discussion
The economic cost of a poor OHS system (i.e., PSC) for worker psychological health is a preventable cost if appropriate measures are taken to build the PSC system. In the current study, we argue that PSC is the leading indicator of employees’ wellbeing that protects employee’s psychological health, hence reducing sickness absence. Concurring with previous evidence, the findings suggest that PSC is indeed an important factor for workers’ health since it is negatively related to sickness absence. Additionally, PSC influenced workers’ future voluntary turnover. Importantly, we found that improving PSC has huge economic benefits for organisations. It is through establishing and building psychologically healthy workplaces that the employers could protect workers from detrimental psychosocial risks and hence also bring benefits to the organisation. Understanding the role of more distal ‘causes’ and the leading indicator of wellbeing such as PSC may provide a more effective target for intervention to prevent workplace illness and injuries and time loss, rather than attempting to treat the adverse psychosocial work conditions (e.g., job insecurity and production pressure), or remedy psychological health states once they have manifested (Zadow et al Reference Zadow, Dollard, McLinton, Lawrence and Tuckey2016). It is likely that PSC and its fundamentals (i.e., valuing psychological health versus productivity and the social relations of production within capitalistic contexts) drive traditional areas of industrial relations (IR) concern, too, such as wages, working hours, and physical safety. Noting that these issues are associated with psychosocial risks (Quinlan Reference Quinlan2023), PSC could be a bridging concept between IR and OHS fields. It would be worthwhile for future research to investigate these links more directly.
Practical implications
Addressing the root cause of sickness absence and turnover, which is identified here as low PSC, is consistent with the International Labour Organization’s agenda of decent work, the United Nation’s sustainable development goals, and the legal requirements in many countries to ensure work is safe and healthy for employees, besides being a moral good. Yet it may be necessary to pursue investment in employee wellbeing by establishing a business case for it. Researchers, practitioners, and safety representatives should be able to set up an argument from both moral and economic aspects by using the results of the current study. By protecting workers and establishing decent work, significant amounts of economic loss can be prevented. Even for an unusually high PSC organisation as in this study (PSC mean = 46.47 out of 60), savings are huge. Still given the pull of capitalistic economies in private and public organisations towards efficiencies, productivity, and profits the economic argument may have limitations, which is why national regulation regarding OHS for worker psychological health and safe levels of PSC is still important (Potter et al Reference Potter, Dollard, Lerouge, Jain, Leka and Cefaliello2024).
Limitations and future research recommendations
Our focus was on estimating cost within a single organisation, and the sample was of white-collar knowledge workers. Generalisability of the results beyond this sample may be limited accordingly. Our experience with this company and the data revealed that this global company is driving a high PSC agenda in order to increase the wellbeing of employees, and the sustainability and productivity of the organisation. Future research should assess whether providing feedback in relation to the economic costs of poor OHS yields any change in PSC. Although we used self-report data, the objective data collected in our study adds validity to the results because results concerning them overcomes subjective bias common in self-report survey approaches. In addition, since all the absence data was bundled together, we could not ascertain whether there was long-term sickness absence, which is considerable a more serious situation, from short-term absence.
Conclusion
Our findings suggest that protecting and promoting workers’ psychological health can have a significant impact on an organisation’s bottom line. There are large economic costs associated with a poor psychologically healthy OHS workplace related to sickness absence and turnover that can be prevented. Neglecting OHS for worker psychological health would lead to a tremendous cost for workers and organisations alike. Protecting worker psychological health and building psychologically healthy workplaces through PSC will assist organisation’s sustainability by reducing productivity loss due to sickness absence and turnover. Successfully increasing PSC should provide a wide range of benefits to workers’ mental and physical health, which is also reflected in a variety of productivity outcomes (reduced sickness absence and reduced turnover). The economic calibration we undertake provides researchers, practitioners, and safety representatives with evidentiary material to argue from both moral and economic perspectives, noting that national regulations for worker psychological health is likely still required to motivate the creation of safe work.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/elr.2024.42
Data availability statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Acknowledgements
MD receives an Australian Research Council Laureate Fellowship (project number FL200100025) funded by the Australian Government, provided resources for the publication. MYL thanks the Australian Government for financial support during her PhD, while the study was conducted.
Competing of interests
Authors declare no Conflict of Interests for this article. The authors’ institution received funding from the source company. The company had no role in the data analysis of interpretation of the results.
Dr. May Young Loh is a Research Associate of PSC Global Observatory, Centre of Workplace Excellence, University of South Australia. She is interested in managing psychosocial factors at work and promoting psychological health and safety through workplace intervention, positive work climate, and leadership training. Her research mainly focuses on the psychosocial safety climate (PSC), job design, and occupational health and wellbeing.
Professor Maureen Dollard is an Australian Research Council Laureate Fellow, Director of the PSC Observatory, University of South Australia, and Honorary Professor at the University of Nottingham. She is the recipient of the 2020 ARC Kathleen Fitzpatrick Award. Her applied research concerns how work affects worker mental and physical health.
Ms. Ashira Friebel is a research assistant of PSC Global Observatory, University of South Australia. Her research interest, including investigating workplace practices, the impact of policy measures on workers’ rights, vulnerability reduction, and enhanced mental health. She is also interested on investigating how senior management training, competency, and capabilities impact general staff confidence and mental health.








 Open access
Open access