


- EFSA
-
European Food Safety Authority
- NDA, EFSA Scientific Panel on Dietetic Products, Nutrition and Allergies
Health claims on foods are a means for industry to communicate health or functional benefits of foods to consumers. They constitute one of a number of ways (others include healthy eating guidelines, nutrition labelling and nutrition claims) in which information on the nutritional attributes of foods can be provided to consumers in order to assist them in choosing a healthful diet. As health claims can influence the selection of foods by consumers they are attractive to industry for marketing foods and may be an incentive to industry to innovate to develop foods with health or functional benefits. This, in turn, should lead to a wider choice of health-promoting foods for consumers. Thus, both consumers and industry stand to gain from health claims on foods.
Increasing use of health claims on foods over the past 20 years has led to the development of legislation to regulate their use in a number of global regions, including the EU( 1 – Reference Asp and Bryngelsson 3 ), USA( Reference Ellwood, Trumbo and Kavanaugh 4 , Reference Hasler 5 ), Canada( Reference L'Abbé, Dumais and Chao 6 ), Japan( Reference Shimizu 7 , Reference Yamada, Sato-Mito and Nagata 8 ), China( Reference Yang 9 ) and Australia/New Zealand( Reference Tapsell 10 ). Such legislation is needed in order to prevent the use of unsubstantiated health claims on foods, which can mislead consumers and result in unfair competition. The Codex Alimentarius Commission of FAO/WHO has also established guidelines for use and scientific substantiation of health claims on foods in order to promote a harmonised approach internationally( 11 , Reference Grossklaus 12 ).
The EU Regulation (EC) No. 1924/2006 on nutrition and health claims made on foods was adopted in 2006 and lays down harmonised rules across the EU for the use of health claims( 1 ). The main objectives are to ensure claims are truthful and not misleading for consumers, to establish common rules across EU Member States to ensure the free movement of goods and conditions for fair competition between companies, and to protect innovation in the food industry. This paper focuses on the scientific substantiation of health claims within the context of the EU Regulation.
Role of the European Food Safety Authority in evaluation of health claims
Regulation (EC) No. 1924/2006 specifies that scientific substantiation should be the main aspect to be taken into account for the use of health claims on foods( 1 ). Furthermore, scientific substantiation should be independently verified: ‘health claims should be only authorised for use in the Community after a scientific assessment of the highest possible standard’ is carried out by the European Food Safety Authority (EFSA). The evaluation of the substantiation of health claims is carried out by the EFSA Scientific Panel on Dietetic Products, Nutrition and Allergies (NDA).
For evaluation of health claims, the EFSA is required to function within the strict legal framework of Regulation (EC) No. 1924/2006, as well as the EFSA founding Regulation( 13 ) which specifies that the Authority should carry out its functions with a high level of transparency and independence. The outcomes of all evaluations, which include detailed explanations of reasons for conclusions reached, are published promptly as scientific opinions in the EFSA Journal. Independence is assured by implementation of a strict policy for avoiding any possible conflicts of interest among experts performing the evaluations( 14 ).
The EFSA role is confined to scientific assessment only; decisions on authorisation of health claims are the role of the European Commission, together with EU Member States and the European Parliament. Authorised health claims are published in the EU Register of Nutrition and Health Claims made on Food( 15 ).
Since health claims are technically complex (both scientifically and legally), the EFSA has developed, in consultation with industry and other stakeholders, extensive guidance to assist applicants in the preparation of applications for authorisation of health claims. Detailed guidance for applicants on preparation of an application( 16 ) is supplemented with guidance on the general principles applied by the EFSA NDA Panel in the evaluation of health claims( 17 ), including the scientific criteria for substantiation.
In addition, a series of guidance documents is being prepared in consultation with stakeholders, each of which addresses issues related to substantiation of specific types of health claims. These issues relate to, for example, which claimed effects are considered to be beneficial physiological effects in the context of the Regulation, and which types of studies and outcome measures are considered appropriate for the substantiation of specific health claims. The guidance documents are based on the experience gained to date by the NDA Panel with the evaluation of health claims in a range of areas, including health claims related to gut and immune function( 18 ), for which consultation has been finalised, and three others for which consultation is ongoing: claims related to bone, joints and oral health( 19 ); claims related to antioxidants, oxidative damage and cardiovascular health( 20 ); and claims related to appetite ratings, weight management and blood glucose concentrations( 21 ). Two additional guidance documents are in preparation: on claims related to neurological and psychological functions and on claims related to physical performance.
Definition of health claims in the EU Regulation
A health claim is defined as ‘any claim that states, suggests or implies that a relationship exists between a food category, a food or one of its components and health’( 1 ). There are three broad types of health claims referred to in the Regulation: (i) function claims, (ii) claims on reduction of disease risk and (iii) claims for development and health of children (see examples in Tables 1–3).
Table 1. Examples of health claims for reduction of disease risk considered substantiated by the European Food Safety Authority

Table 2. Examples of health claims for development and health in children considered substantiated by the European Food Safety Authority

Table 3. Examples of health (function) claims considered substantiated by the European Food Safety Authority
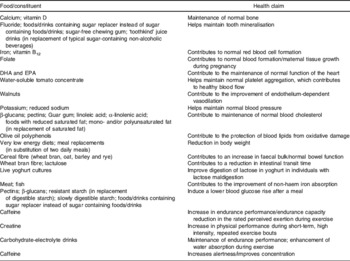
Function claims are health claims describing or referring to: (a) the role of a nutrient or other substance in growth, development and the functions of the body; or (b) psychological and behavioural functions; or (c) slimming or weight control or a reduction in the sense of hunger or an increase in the sense of satiety or to the reduction of the available energy from the diet( 1 ). Claims on reduction of disease risk are health claims referring to reduction of a risk factor in the development of a human disease( 1 ). Claims for development and health of children are health claims solely referring to the development and health of children, and where the scientific substantiation is only valid for children( 22 ). They also include health claims used on products intended exclusively for children, such as follow-on formulae, processed cereal-based foods and baby foods.
Health claims on foods are legally distinct from medicinal claims. Under EU food legislation, claims on the prevention, treatment or cure of a human disease are not allowed for foodstuffs as these constitute ‘medicinal’ claims( 23 ). However, there is potential overlap between health claims and medicinal claims and the borderline is defined partly by the wording used (e.g. health claims must not refer to the prevention, treatment or cure of a human disease) as well as the population group for which the claim is intended (e.g. if it is for patients with a disease then the claim is considered to refer to ‘treatment’)( 17 ).
The EU Regulation provides for different procedures for authorisation of different categories of health claims. Authorisation of claims on reduction of disease risk, claims for development and health of children and function claims based on newly developed scientific evidence and/or which include a request for the protection of proprietary data requires that a full application be made to a Member State for forwarding to the EFSA for evaluation. Other function claims (‘general function claims’) are to be authorised by a different procedure, i.e. following evaluation by the EFSA of claims submitted to the European Commission by Member States.
Substantiation of claims by generally accepted scientific evidence
The principal scientific criterion for scientific substantiation of health claims in the EU is ‘generally accepted scientific evidence’( 1 ). According to the EU Regulation, a health claim may only be made for a food if it has been shown to have a beneficial physiological effect, as established by generally accepted scientific evidence by taking into account the totality of the available scientific data, and by weighing the evidence( 1 ).
It is important to note that scientific criteria for substantiation of health claims vary across global jurisdictions, depending on the provisions of the specific legislation as well as on the implementation of legislation by agencies charged with assessment of claims( Reference Jew, Vanstone and Antoine 24 , Reference Jones, Asp and Silva 25 ). The Codex Alimentarius Commission of the FAO/WHO has established guidelines for the scientific substantiation of health claims on foods which sets out a common approach that should be adopted internationally( 11 , Reference Grossklaus 12 ).
The EFSA has elaborated on the meaning and application of the criterion of ‘generally accepted scientific evidence’ in its guidance( 17 ). ‘Generally accepted’ is considered to mean generally accepted by scientific experts in the field. In assessing each health claim, the NDA Panel makes a scientific judgement on the extent to which a cause and effect relationship is established between the consumption of the food/constituent and the claimed effect by weighing the evidence for its strength, consistency, specificity, dose–response and biological plausibility. This is performed with particular regard to the population group for which the claim is intended, and to the conditions of use (e.g. the quantity of food) proposed for the claim. Weighing includes only those studies considered pertinent for the claim (i.e. studies from which scientific conclusions can be drawn for the substantiation of the claim). Evidence is considered according to the hierarchy of study designs, reflecting the relative strength of evidence that may be obtained from different types of studies( 16 ).
While studies in animals or in vitro may provide supportive evidence (e.g. in support of a mechanism), human data are central for the substantiation of the claim. EFSA's requirement for studies in human subjects for substantiation of health claims is in agreement with the approach adopted by a number of other global jurisdictions( Reference Jew, Vanstone and Antoine 24 , Reference Jones, Asp and Silva 25 ), including the U.S. Food and Drug Administration( 26 ). It is also consistent with the approach recommended by Codex Alimentarius Commission( 11 , Reference Grossklaus 12 ). Accordingly, particular attention is focused on the design and quality of individual human studies.
In considering whether the human studies are pertinent for a specific claim, the NDA Panel addresses the following questions: whether the studies have been carried out with the food/constituent for which the claim is made, whether (an) appropriate outcome measure(s) of the claimed effect was used, whether the design and quality of the studies is sufficient to provide evidence from which conclusions can be drawn for the scientific substantiation of the specific claim, whether the conditions under which the human studies were performed relate to the conditions of use (e.g. quantity and pattern of consumption of the food/constituent) proposed for the claim, whether the studies have been carried out in a study group that is representative of the population group for which the claim is intended( 17 ).
Extrapolation from studies in groups (e.g. subjects with a disease) other than the target group for a claim (e.g. the general population) requires evidence to establish that such extrapolation is biologically justified( 17 ). For example, the NDA Panel has considered that for claims on reducing gastro-intestinal discomfort (in the general population) evidence in patients with irritable bowel syndrome may be accepted( 27 ). However, for claims on maintenance of normal joints (in the general population), evidence is not accepted from studies with osteoarthritis patients as their joint tissues are not considered to be representative of the general population and may respond differently to intervention with exogenous substances( 28 ).
Other considerations for substantiation of health claims
There are two other key considerations for substantiation of health claims: (i) the extent to which the food/constituent is defined and characterised, and (ii) the extent to which the claim is defined and is a beneficial physiological effect.
A food/constituent should be adequately characterised with respect to those characteristics that relate to the claim. This is required in order to establish that the studies provided for substantiation of the claim were performed with the food/constituent for which the claim is made, as well as to allow definition of appropriate conditions of use for the claim( 17 ). For example, plant products/extracts should be identified by the scientific name, the part and the preparation used, while micro-organisms (e.g. bacteria and yeast) should be identified by species, strain (genetic typing) and the name of strain according to the International Code of Nomenclature( 17 ).
The EU Regulation requires that a health claim must be a beneficial physiological effect. For example, function claims may relate to maintenance or improvement of a body function. For reduction of disease risk claims, the beneficial effect refers to the reduction (or beneficial alteration) of a risk factor for the development of a human disease (not reduction of the risk of disease)( 17 ).
A risk factor is a physiological factor associated with the risk of a disease, which may serve as an independent predictor for the development of that disease( 17 ). The relationship of the factor to the development of the disease should be biologically plausible. For example, elevated blood LDL-cholesterol concentration and elevated blood pressure are accepted as risk factors for development of CHD( 20 ). However, for other proposed risk factors, the evidence may not be as strong and these are considered on a case-by-case basis. For example, presence of dental plaque is accepted as a risk factor for dental caries only for claims on foods (e.g. sugar-free chewing gum), which have been shown to reduce both dental caries and dental plaque( 19 ).
Outcomes of evaluations of health claims by European Food Safety Authority
The implementation of the EU Regulation is still at a relatively early stage and so the overall effect on the use of health claims by industry remains unclear. However, at the scientific level, EFSA's published evaluations of a large number of claims and its extensive guidance to applicants have made an important contribution to the understanding of scientific substantiation of health claims. This will help to set new directions for research and will guide future innovation.
EFSA has published completed evaluations for over 2800 health claims (as of July, 2011). These include over 100 claims submitted to EFSA by the direct application procedure, i.e. a complete dossier of evidence from an individual applicant, as well as over 2700 ‘general function claims’ submitted by EU Member States. For most of these claims no independent evaluation of their scientific substantiation has been carried out previously and the assessment by the EFSA has defined the scientific requirements for substantiation of many claims for the first time. Based on the experience gained from these evaluations, the EFSA is consolidating these scientific requirements into extensive guidance to applicants through a process of public consultation( 18 – 21 ).
The EFSA evaluations of claims have highlighted many important issues related to the quality of studies in human subjects, as well as how different types of studies may be used for substantiation of specific claims. A review of the EFSA opinions on health claims shows that the quality of studies carried out in human subjects has frequently been the critical consideration and weaknesses in the design, execution, analysis and reporting of such studies have undermined the evidence for substantiation. The evidence on the validity and the interpretation of biomarkers of body function and of disease risk has often been weak. In addition, the lack of consideration of the validity of model systems, e.g. studies in animals and in vitro, has greatly limited the usefulness of such studies, even to explain mechanisms for claimed effects.
To date, the EFSA NDA Panel has concluded that a wide range of health claims has been substantiated (see Tables 1–3 for examples). These include claims for many well-established functions of nutrients, as well as beneficial effects of foods and food constituents on a range of body functions. In addition, claims have been substantiated on the role of nutrients in growth and development of children and on the effects of nutrients and food constituents on reduction of risk factors for disease.
The protection of proprietary data used for substantiation of claims is an important element in the Regulation. This is illustrated by the authorisation of a claim on water soluble tomato concentrate that it ‘helps maintain normal platelet aggregation, which contributes to healthy blood flow’, which can be used on water soluble tomato concentrate-containing fruit juices, flavoured drinks or yoghurt drinks and food supplements. In the authorisation, the key data required for substantiation of the claim (seven unpublished human studies claimed as proprietary by the applicant) were restricted for the benefit of the applicant for a period of 5 years( 29 ). This gives the applicant a considerable period of protection of proprietary data and is a strong incentive for innovation.
Some health claims that have been widely used in the market over recent years have not been shown to be scientifically substantiated. For example, for claims related to ‘prebiotic’ and ‘probiotic’ effects that relate to increasing numbers of specific bacteria (e.g. lactobacilli or bifidobacteria) in the gastro-intestinal tract the EFSA NDA Panel did not consider that this is a beneficial physiological effect per se. Thus, the beneficial consequences for health or body functions of increasing the numbers of such bacteria need to be demonstrated.
An important outstanding issue is the status of health claims on ‘botanicals’, many of which are supported mainly by evidence of ‘traditional use’. The EU Regulation on health claims does not make specific provision for ‘traditional use’ to be taken into account. Consequently, the assessment of many claims on ‘botanicals’ that were submitted by Member States as ‘general function claims’ has been put on hold by the European Commission pending further consideration of their status.
A key milestone in the implementation of the EU Regulation will be the adoption of the Community list of permitted ‘general function claims’. The EFSA has completed evaluation of all of these claims (except for those on ‘botanicals’, explained earlier) in June 2011 and the European Commission, together with the EU Member States and the European Parliament, is expected to adopt the list in 2012. Those ‘general function claims’ authorised on the permitted list can be used throughout the twenty-seven EU Member States; however, claims not included in the list will no longer be permitted to be used in the EU.
Conclusions
EU legislation requires that the EFSA must carry out an assessment of the scientific substantiation of health claims before they are authorised for use in the European Community. Independent evaluations by the EFSA NDA Panel of a large number of health claims have defined the scientific requirements for substantiation of many health claims for the first time. These are now being consolidated into extensive guidance to assist applicants in the preparation of applications for authorisation of health claims. EFSA opinions on health claims have also highlighted many important issues related to the quality of human studies used for substantiation, as well as how different types of studies may be used for substantiation of specific claims.
To date, the EFSA NDA Panel has concluded that a wide range of health claims has been substantiated. These include claims for many well-established functions of nutrients, as well as beneficial effects of foods and food constituents on a range of body functions. In addition, claims have been substantiated on the role of nutrients in growth and development of children and on the effects of nutrients and food constituents on reduction of risk factors for disease. Some health claims that have been widely used in the market over recent years have not been shown to be scientifically substantiated.
The EFSA published evaluations of a large number of claims and its extensive guidance to applicants have made an important contribution to the understanding of scientific substantiation of health claims. This will help to set new directions for research and will guide future innovation.
Acknowledgements
The author is currently Chair of the Scientific Panel of Dietetic Products, Nutrition and Allergies of the European Food Safety Authority. All work on the preparation of the manuscript was carried out by the author. The author declares no conflict of interest relating to this paper. No funding was received for the preparation of this paper.



