


Heatwaves are predicted to increase in intensity and severity during the coming century and are expected to have significant consequences for human health. Reference Confalonieri, Menne, Akhtar, Ebi, Hauengue, Kovats, Parry, Canziani, Palutikof, van der Linden and Hanson1 Hot weather generally, and heatwaves more specifically, have been shown to increase mortality in the short term, Reference Keatinge, Donaldson, Cordioli, Martinelli, Kunst and Mackenbach2,Reference McMichael, Wilkinson, Kovats, Pattenden, Hajat and Armstrong3 and risk factors for death during these periods include old age, living in institutional care, pre-existing cardiovascular or respiratory illness and urban living. Reference Kovats and Hajat4 There is limited evidence that people with severe mental illness may be at particular risk of premature death during periods of hot weather, Reference Bouchama, Dehbi, Mohamed, Matthies, Shoukri and Menne5–Reference Page, Hajat and Kovats7 but studies to date have mostly been case reports or have relied on case–control methodology.
The current study seeks to use a large, well-validated, longitudinal, primary care data-set to determine the risk of mortality in people with psychosis, dementia and substance misuse during hot weather. It also seeks to identify the regions of England where heat risk is greatest and to determine whether individual-level risk factors (e.g. age, type of mental illness, medication use) confer increased risk for heat-related death. Our primary hypothesis was that patients with psychotic illness would be at greatest risk of heat-related mortality; a secondary hypothesis was that those taking antipsychotic medication would show elevated risk compared with those taking other medications.
Method
Sample
People with primary diagnoses of psychosis, dementia, alcohol misuse and other substance misuse, who had died between 1 January 1998 and 31 December 2007 in England, were identified from the UK General Practice Research Database (GPRD). The GPRD contains detailed, longitudinal, clinical information on 4 million primary care patients living in the UK, is subject to a high level of quality control and has been used widely to investigate epidemiological and clinical questions relevant to primary care (www.gprd.com). Participating practices are subject to a rigorous quality control and only practices that reach a sufficient standard are retained in the database. All data are fully anonymised at source, and GPRD has a well-established consent procedure in place for participating practices. In order to ascertain an exact date of death for each patient, this sample was cross-linked with death registration records held by the UK Office for National Statistics (ONS); to protect patient anonymity, this linkage procedure was undertaken using a protocol specially designed by ONS and GPRD.
For this study, we were interested in people with mental illness that was severe and enduring and for this reason included the following diagnostic groups in our sample: psychoses, dementia, alcohol misuse and other substance misuse. There is some existing evidence that these groups may be at particular risk during hot weather. The diagnoses were made clinically and were recorded using Oxford Medical Information System (OXMIS) or READ codes that were cross-referenced to ICD-10. Diagnosis was hierarchical, such that patients could only be counted in one diagnostic group. Previous publications have demonstrated the validity of the GPRD database when recording psychotic illness. Reference Howard, Kumar, Leese and Thornicroft8 Levels of current alcohol or substance misuse consumption were not known, although use would have been clinically and/or functionally significant in order to be recorded by the general practitioner. See online Table DS1 for further details of how diagnostic groupings were coded.
Health data
Basic demographic data including age at death, gender and region of residence were available for each patient. Details of prescribed medication were available and patients were presumed to be taking psychotropic medication at the time of their death if they had been prescribed that medication within the year prior to their death. Psychotropic medication was classified into the following categories in line with the British National Formulary: 9
-
(a) antipsychotics
-
(b) antidepressants
-
(c) hypnotics/anxiolytics
-
(d) other.
Region of residence referred to the region of England in which the patient usually resided according to GPRD records.
Exposure data
The effect of temperature on mortality was assessed across the temperature range and throughout the year – not just during isolated heatwave periods. Daily temperature data for 1998–2007 from all monitoring stations in England were downloaded from the British Atmospheric Data Centre. Data were processed to obtain an average daily series for each government region of England, and imputing any missing values using the method from the Airgene study (i.e. a missing value on day i from monitor j is replaced by the period average of monitor j plus a standardised value of day i over all monitors, multiplied by the period standard deviation of monitor j). Reference Rückerl, Greven, Ljungman, Aalto, Antoniades and Bellander10 Temperature series from individual monitors were highly correlated within regions, and station means also varied little within regions. We also collected information on relative humidity, as well as daily temperature measures from the Central England Temperature (CET) series to represent national level data. Reference Parker, Legg and Folland11 England is divided into ten government regions, which have some differences in terms of prevailing weather, with Southern and Eastern regions tending to have higher temperatures in summer. All analyses were conducted on daily mean temperature, as this reflects high daytime as well as high night-time temperatures.
Analysis
To assess the short-term relationship between mortality levels and daily fluctuations in temperature, the mortality data were first collapsed by date of death to provide a daily count of the number of deaths between 1998 and 2007. Counts were subdivided by region, age group, diagnosis, and pharmacological therapy. Each series was then examined in relation to daily temperature using Poisson regression models with scale over-dispersion. Each model controlled for trends and broad intra-annual seasonal patterns using cubic smoothing splines of date. Also, all models controlled for any confounding effects of relative humidity and any day-of-week patterns.
Initially, natural cubic splines of temperature were used to visualise the adjusted relationship between temperature and the risk of death. Then, to quantify the heat effect, a linear threshold model was assumed, whereby the relationship between high temperature and mortality risk is assumed to be linear once temperatures have reached regionally specific threshold values. Statistical diagnostics indicated that the best-fitting models were obtained using a zero-day lag only of the temperature measure (i.e. temperature levels on the same day as the date of death), indicating therefore that there is little delayed effect of heat exposure.
Nationally aggregated mortality data were first analysed in relation to the CET series, but then also by region in conjunction with region-specific temperature data. As with previous work, Reference Armstrong, Chalabi, Fenn, Hajat, Kovats and Milojevic12 statistical model fit indicated that a heat threshold was evident at approximately the 93rd percentile of the annual temperature distribution specific to each region. Finally, cluster-specific heat risks were combined in a meta-analytic model to provide a mean effect of heat exposure. This assumed a fixed effect between clusters, although a random effects model gave very similar results. All results presented for subgroups are derived from the meta-analytic models. All analyses were conducted using STATA version 11 for Windows.
Results
In total, data on 22 562 deaths were available for analysis and there was a mean daily count of 6.18 deaths. As with the general population, mortality counts were broadly highest in the winter months (see Fig. 1 for an example year). However, on plotting all deaths against same-day temperature, while adjusting for trends and any seasonal patterns, an increase in relative risk of death could be seen at temperatures above a heat threshold. This is shown for national data against CET (Fig. 2), where a threshold is evident at about 18°C – this corresponds approximately to the 93rd percentile of the annual CET distribution. Splines for relative humidity were included in all models by default, although they were not significant.
Regional analyses showed that, with the exception of the North West and South Central regions, all clusters demonstrated an increased risk of death at high temperature. Figure 3 shows the relative risk of death per 1°C increase in temperature above the 93rd percentile of the annual distribution of regional-specific temperature data. There was variation in risk by region, with the East Midlands and the South East regions of England
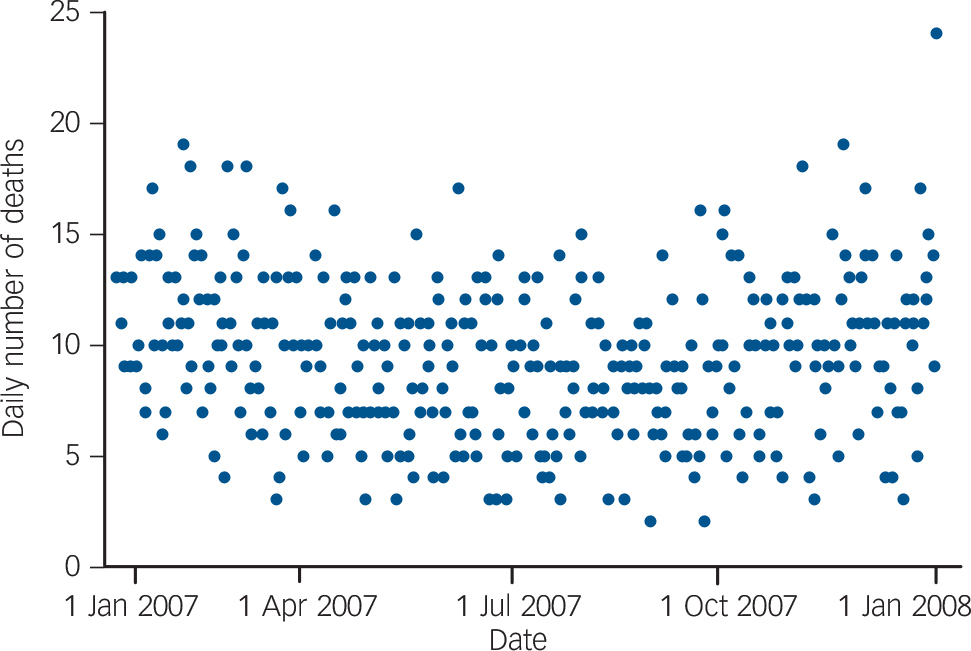
Fig. 1 Annual distribution of total daily deaths in England in a typical year in patients with psychosis, dementia and substance misuse.
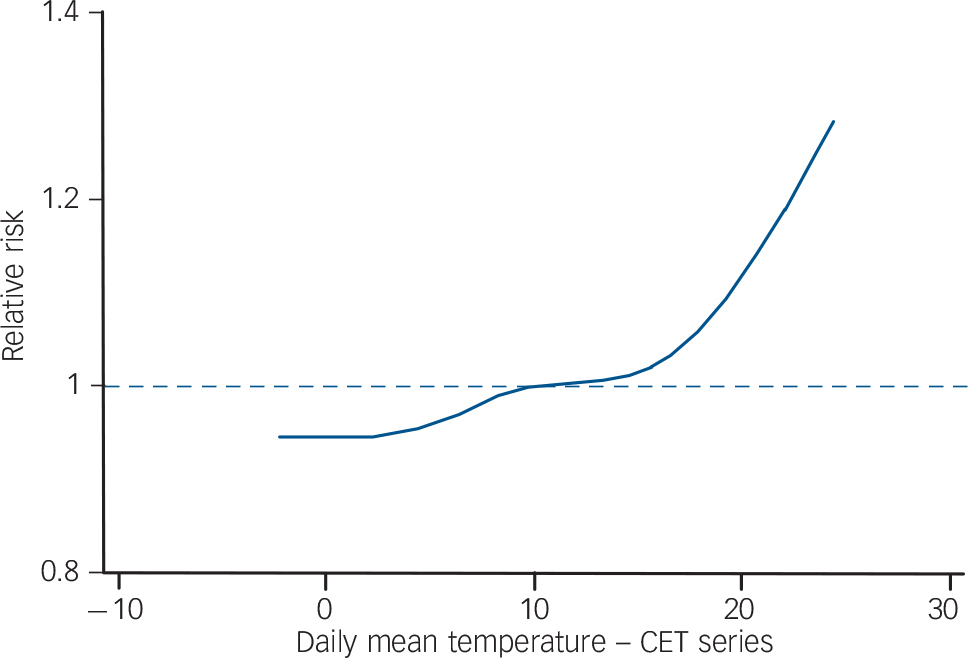
Fig. 2 Seasonally adjusted relationship between risk of death and central England temperature (CET) series in patients with psychosis, dementia and substance misuse.
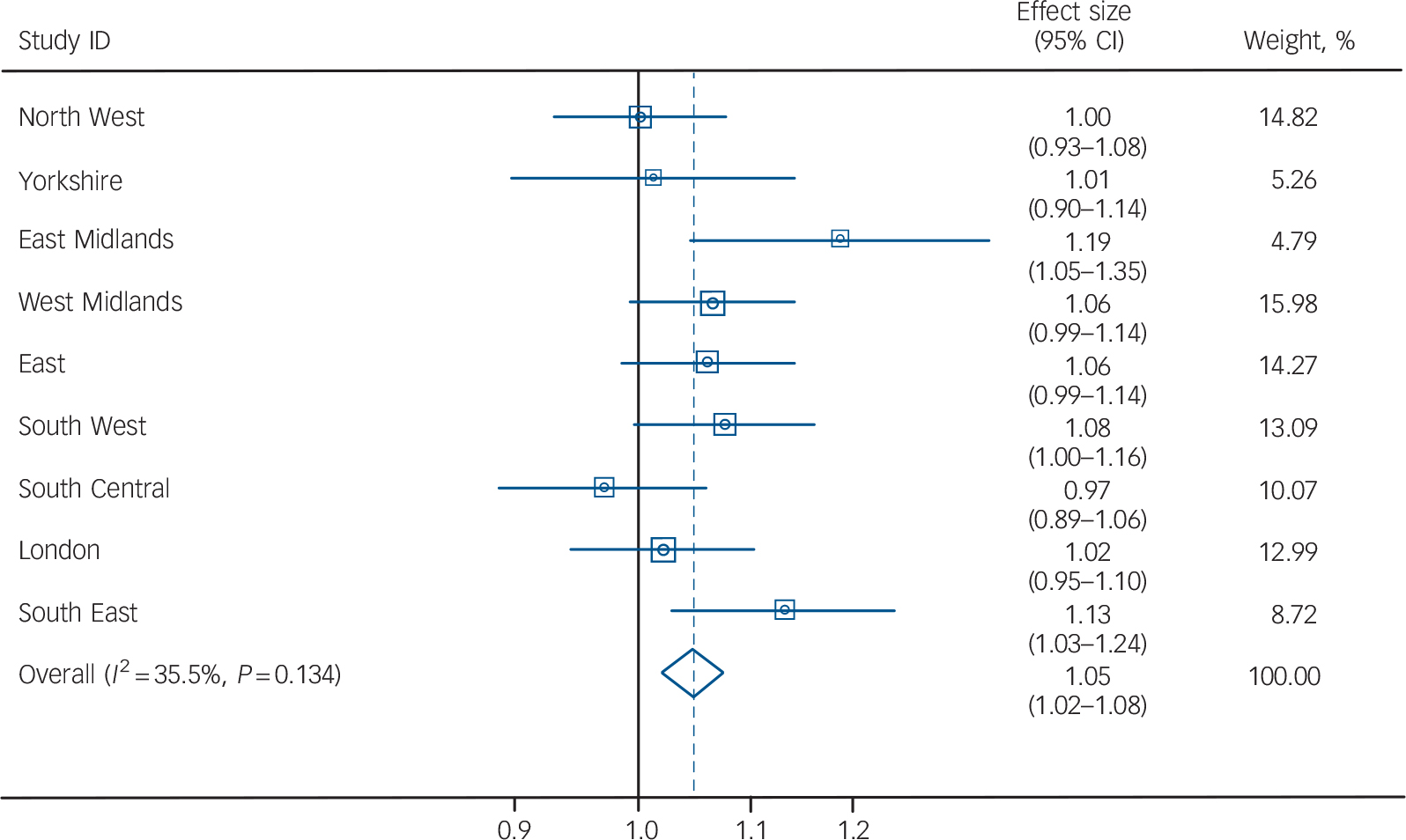
Fig. 3 Forest plot of effect of temperature on relative risk of death by regiona in patients with psychosis, dementia and substance misuse.
93rd percentile by cluster: 15.86 North West; 17.06 Yorkshire; 17.74 East Midlands; 17.22 West Midlands; 18.38 East; 17.32 South West; 17.70 South Central; 19.36 London; 18.18 South East.
a. Death count in North East cluster too low to be analysed.
demonstrating the greatest effect of high temperature on mortality. Meta-analyses of all deaths by region demonstrated an overall 4.9% (95% CI 2.0–7.8) increase in deaths per 1°C increase in temperature above the 93rd percentile of temperature.
Effect modifiers
Age and diagnosis acted as effect modifiers in the relationship between temperature and relative risk of death. Specifically, patients aged less than 65 years were at greater risk of death than those aged over 65 years during hot weather – 10% v. 4% (P = 0.06) increase in relative risk per 1°C increase in temperature (above 93rd percentile). Those patients with a primary diagnosis of alcohol misuse or other substance misuse were at elevated risk of death compared with patients with other diagnoses (Table 1). Prescribed psychotropic medication was found to modify the relationship between temperature and relative risk of death. Hypnotic/anxiolytic and antipsychotic medications were associated with elevated risk during hot weather (8% and 7% increase in relative risk per 1°C increase in temperature respectively), while antidepressant medication was not. Hypnotics/anxiolytics continued to be associated with elevated risk even after all individuals with a primary diagnosis of alcohol
TABLE 1 The effect of age and diagnosis on the relationship between relative risk of death and temperature (combined effect shown for all regional clusters)
| Effect modifier | % of all deaths | Relative risk per 1°C increase | Lower confidence interval | Upper confidence interval | P |
|---|---|---|---|---|---|
| Age, years | |||||
| <65 | 17.9 | 1.10 | 1.05 | 1.16 | |
| 65+ | 82.1 | 1.04 | 1.01 | 1.07 | 0.06 |
| Diagnosis | |||||
| Dementia (reference group) | 50.4 | 1.03 | 1.00 | 1.07 | |
| Psychoses | 13.9 | 1.02 | 0.95 | 1.09 | 0.77 |
| Alcohol misuse | 32.6 | 1.08 | 1.04 | 1.13 | 0.07 |
| Other substance misuse | 3.2 | 1.20 | 1.08 | 1.35 | 0.02 |
or drug misuse were excluded (11% increase in relative risk per 1°C increase) (Table 2).
Discussion
To our knowledge, this is the first study to assess the effect of high ambient temperature on mortality in a national sample of patients with mental illness. Using a representative and well-validated primary care sample, we found a marked increase in relative risk of death during hot weather. A classic ‘hockey stick’ plot was demonstrated within the sample, whereby a sharp increase in the risk of death was observed above a certain temperature threshold (defined as the 93rd percentile) – this corresponded to an increased risk of death of around 5% per 1°C increase in temperature above this threshold. This is greater than the effect seen in general population samples using similar methodology, where an increased risk of around 2% per 1°C increase has been identified in England and Wales. Reference Armstrong, Chalabi, Fenn, Hajat, Kovats and Milojevic12 We also found specific demographic and illness factors associated with elevated risk: patients from the East Midlands and South East regions of England showed the greatest risk of death during hot weather, while being of younger age, having a primary diagnosis of
TABLE 2 Effect of pharmacological therapy on the relationship between relative risk of death and temperature a

| n b (%) | Relative risk per 1°C increase | Lower confidence interval | Upper confidence interval | |
|---|---|---|---|---|
| All patients | 13988 (100) | 1.04 | 1.00 | 1.08 |
| Patients prescribed antipsychotics | 4449 (31.8) | 1.07 | 1.01 | 1.13 |
| Patients prescribed antidepressants | 3987 (28.5) | 1.02 | 0.96 | 1.09 |
| Patients prescribed hypnotics/anxiolytics | 4546 (32.5) | 1.08 | 1.02 | 1.15 |
| Patients prescribed hypnotics/anxiolytics (but excluding those with primary diagnosis of alcohol or drug misuse) | 2731 (19.5) | 1.11 | 1.02 | 1.20 |
a These results are the combined effect for five clusters only where counts were high enough to subdivide patients by therapy type (North West, Yorkshire, West Midlands, South West, and London). This is why the ‘all patients’ estimate is slightly different to previously.
b Percentages add up to >100 as patients could be prescribed more than one type of medication.
drug or alcohol misuse and being prescribed hypnotics or antipsychotics also conferred greater risk.
There are several biological and social factors that may plausibly increase mortality among people with mental illness during hot weather. Reference Page and Howard13 People with mental illness are more likely to be socially isolated or living in institutional care, both of which are risk factors for heat-related death. Reference Kovats and Hajat4,Reference Kovats, Johnson and Griffiths14 Case reports have suggested that maladaptive behaviours, such as wandering and psychomotor agitation, make people with mental illness especially vulnerable during hot weather. Reference Mann and Boger15 Putative biological risk factors include the use of psychotropic medication, Reference Bouchama, Dehbi, Mohamed, Matthies, Shoukri and Menne5,Reference Mann and Boger15,Reference Nordon, Martin-Latry, de Roquefeuil, Latry, Bégaud and Falissard16 poor physical health Reference Basu and Samet17 and substance misuse. Reference Marzuk, Tardiff, Leon, Hirsch, Portera and Iqbal18 A study from New York City, found that individuals receiving psychiatric in-patient care were twice as likely to die during heatwaves as the general population. Reference Bark19 However, prior to the current study, there have been few attempts to quantify the extent of increased risk to people with mental illness during periods of hot weather.
Cause of death
We did not have information on cause of death for our sample, so are unable to comment on this in any detail. Research from general population samples would suggest that death due to cardiovascular and respiratory causes is more frequent during hot weather and it is uncommon for death to be recorded as a direct result of ‘heat stroke’. There is emerging evidence, from the UK Reference Page, Hajat and Kovats7 and elsewhere, Reference Kim, Kim and Kim20,Reference Likhvar, Honda and Ono21 that death by suicide is associated with higher ambient temperature. Suicide is known to be a relatively common cause of death in patients with psychosis and substance misuse; unfortunately, we were unable to examine suicide as a specific cause of death in this study.
Alcohol and drug misuse
Alcoholism has previously been linked to heat-related mortality, but never beyond the setting of isolated heatwaves. Reference Mirchandani, McDonald, Hood and Fonseca22 The mechanism by which alcohol exerts this effect is probably via depression of the central nervous system, diuresis and dehydration. Reference Keatinge23 One previous study showed an association between fatal cocaine overdoses and hot weather, Reference Marzuk, Tardiff, Leon, Hirsch, Portera and Iqbal18 but otherwise the strikingly elevated risk of death we observed among patients with substance misuse has not previously been noted and has potential implications for public health strategies. Patients with a primary diagnosis of substance misuse were mostly opiate users and it is not clear whether their increased risk was conferred by the use of opiate drugs themselves or the physical comorbidities related to chronic drug misuse.
Medication
A few studies have previously identified psychosis as a risk factor for mortality during hot weather. Reference Stafoggia, Forastiere, Agostini, Biggeri, Bisanti and Cadum24–Reference Hansen, Bi, Nitschke, Ryan, Pisaniello and Tucker26 However, the present study suggests that antipsychotic and hypnotic medication are more strongly associated with risk of death than the diagnosis of a psychotic illness per se. One strength of the present study was the ability to examine these medications as potential effect modifiers, but unfortunately numbers precluded us from assessing the effect of first-generation v. second-generation antipsychotics; neither were we able to examine the effect of anticholinergics or mood stabilisers on mortality.
Further work is needed to understand how medications such as hypnotics, antipsychotics and opiates may impair physiological response to extreme heat. Mechanisms probably vary depending on the medication under consideration. For example, antipsychotics may alter the temperature regulation set point via anti-dopaminergic action and impair sweating via anticholinergic action. Reference Kwok and Chan27 Opiates may interfere with the usual physiological responses to heat within the skin vasculature; Reference Romanovsky and Blatteis28 while hypnotics depress the central nervous system leading to dehydration and haemoconcentration. The absence of a lag effect in the relationship between temperature and mortality suggests that the pathophysiological effect of heat in people with mental illness is rapid. The implied adverse effect of certain medications – both prescribed and non-prescribed – suggests that patients other than those with mental illness could also be at increased risk during hot weather. For example, hypnotics and opiates are commonly prescribed post-surgically and in palliative and intensive care settings; further work is needed to investigate temperature–mortality effects in these contexts.
Age effects
Our finding that patients aged under 65 years were at greater relative risk than older patients was surprising, given that the elderly are often associated with high death rates during heatwaves and high temperatures generally. Reference Kovats and Hajat4,Reference Stafoggia, Forastiere, Agostini, Biggeri, Bisanti and Cadum24,Reference Hansen, Bi, Nitschke, Ryan, Pisaniello and Tucker26 The majority of elderly patients in our sample had dementia and it may be that their care was better during periods of hot weather relative to younger patients with alcohol or substance misuse. Certainly, elderly patients would have been more likely to be in institutional care, although we were not able to look at the effect of place of death in this study. The lack of extremely old patients (e.g. > 90 years of age) in our sample may also have influenced our findings, as this age group is better represented in general population samples. Overall, we conclude that the finding of higher relative risk amongst younger patients is likely to be driven by the substantially greater risk that those with a primary diagnosis of drug and alcohol misuse demonstrated.
Region
Living in the East Midlands and South East region of England may have conferred greater risk than other regions because of the relative urbanicity of these regions. The ‘urban heat island effect’ refers to the finding that temperatures are consistently higher within cities than outside. Characteristics of the urban environment are likely to magnify night-time temperatures and therefore lead to increased mortality during hot weather. Reference Kovats and Hajat4 There is a need for this study to be repeated in other settings and geographical areas.
Study strengths
To our knowledge, this is the first study to use a representative, community sample of patients with defined mental illnesses to study heat-related mortality. Many of the studies that have previously identified psychiatric illness as a risk factor for heat-related mortality have used a case–control method following a single heatwave event, whereas the present study used a longitudinal design to quantify the effect of temperature on mortality across the temperature range over a 10-year period. Therefore, our findings are not just relevant to extreme heatwave events, as we were able to demonstrate that people with mental illness were at increased risk of death above regionally defined thresholds corresponding to the 93rd centile, thereby confirming that excess mortality in this group occurs outside of defined heatwave events. Additional strengths included the minimisation of misclassification of outcome by cross-linking the primary care data with nationally held death records (based on death certificates) to ensure that date of death was accurate. Misclassification of exposure was also reduced by assigning regional (as opposed to national) temperatures to each death. Given the lack of air conditioning in England, it is likely that in the summer months measured external temperature corresponded closely with temperatures experienced inside residential and institutional environments.
Study limitations
There were several limitations to this study. First, we assumed that if a patient had been prescribed a psychotropic medication in the year prior to their death, they were still taking it at the time of their death. This approach may have led to inaccuracies, as patients may not take their prescribed psychiatric medication; likewise, it is possible that additional psychiatric medications were prescribed directly from secondary care and not recorded by primary care. Second, despite using a nationally derived sample, there were insufficient numbers to evaluate the role of some effect modifiers of interest (e.g. first-generation v. second-generation antipsychotics or mood stabilisers). Insufficient numbers and information on cause of death also precluded detailed evaluation on cause of death. Third, the temperature series used for the South Central cluster was derived by taking the simple average of the South East and South West regions (due to the fact that this cluster is the only one that does not map directly to a government region, which is the unit of area used to create averaged temperature series), so there may have been exposure misclassification. This may explain the negative risk obtained for the South Central cluster. The sample was too small to reliably assess the impact of any heatwaves that occurred during the study period, such as that of the 2003 heatwave.
Public health implications
The current study adds to the accumulating evidence that people with mental illness constitute a vulnerable group during hot weather. Some public health strategies, such as that outlined by the English ‘Heatwave Plan’, already identify patients with mental health problems as being a ‘high risk’ group, 29 but more attention may need to be paid to patients with primary alcohol and substance use problems, who are commonly not under the care of mental health services. Indeed, patients with substance use disorders are often hard to reach using public health interventions, and are often out of contact with professional health services entirely, Reference Garland, Aarons, Brown, Wood and Hough30 meaning that novel tactics may need to be employed if mortality risk is to be reduced in these groups during hot weather. It is likely that the multiple physical comorbidities experienced by people with mental illness substantially contribute to their vulnerability during hot weather. Optimising physical care for these patients has become a clinical priority Reference Citrome and Yeomans31 and general improvements to their physical health could reduce their risk of heat-related mortality.
The importance of regionally defined thresholds and analyses is emphasised by the present study. Identifying areas (such as the East Midlands and South East region of England) in which there is an especially increased risk of temperature-related mortality may be helpful when scarce resources are being targeted at the most vulnerable.
We found that primary care patients with psychosis, dementia, alcohol or substance misuse experienced significant heat-related mortality above regionally defined temperature thresholds. This effect was more marked for younger patients, those living in Southern and Eastern parts of England and in those with a primary diagnosis of alcohol or substance misuse. Prescription of hypnotics and antipsychotics were also associated with higher risk of death. Given that global temperatures will continue to rise and the frequency of heatwaves is predicted to increase in the years to come, Reference Meehl and Tebaldi32 these findings suggest that consequences of climate change may be felt disproportionately by people with mental illness.
Funding
This study was made possible by the MRC-GPRD access to data initiative (reference 08_002) and was funded by the BUPA Foundation (grant reference ). MRC-GPRD and BUPA Foundation had no role in the design and conduct of the study; collection, management, analysis or interpretation of the data. The funders were not involved in the preparation, review or approval of the manuscript.
Acknowledgements
L.M.H. is supported by the NIHR Biomedical Research Centre based at South London and Maudsley NHS Foundation Trust/King’s College London, and has received grants from the UK Medical Research Council and the Wellcome Trust. S.H. is funded by the Wellcome Trust. L.A.P. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.







eLetters
No eLetters have been published for this article.