



Significant outcomes
-
Returning to online educational activities had a positive effect on students’ depression levels; there were no changes in anxiety levels after the return to online educational activities; there was a significant difference in the level of restriction before and after the return to online classes, and the level of restriction was not associated with depression or anxiety level.
Limitations
-
Convenience sampling strategy based on electronic forms answered voluntarily; the investigated population was not evaluated prior to the appearance of the virus; it used self-reported scales.
Introduction
A novel coronavirus, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing the coronavirus disease 2019 (COVID-19), emerged in late 2019 (Dhama et al., Reference Dhama2020; Rodriguez-Morales, Bonilla-Aldana, et al., Reference Rodriguez-Morales and Bonilla-Aldana2020). The new disease quickly spread around the world and arrived in Brazil on February 26, 2020 (Rodriguez-Morales, Gallego, et al., Reference Rodriguez-Morales and Gallego2020).
On March 11, 2020, the Brazilian Ministry of Health published social isolation guidelines for people infected or under clinical and laboratory investigation for COVID-19 (Aquino et al., Reference Aquino2020). After that, quarantine became the official position of Brazilian Ministry of Health for the entire country (Shadmi et al., Reference Shadmi2020). On March 16, 2020, the classes at Federal Universities were suspended, and the students returned to not presential classes (online classes) on July 6, 2020.
The social isolation rules affected not only the economy and society but also the mental health of individuals who had reduced social contact (Puccinelli et al., Reference Puccinelli2021). The effects became even more profound for young adults and university students (Orben et al., Reference Orben, Tomova and Blakemore2020).
A study conducted with health care students showed that only 19% of students were symptoms free of depression, anxiety and stress. The remainder (81%) had at least one of the three symptoms (Alim et al., Reference Alim2017). Moreover, the prevalence of depression and anxiety among medical students during the COVID-19 pandemic was also reported, being moderate to severe depression in 17.2% and moderate to severe anxiety in 20.3% of the students (Gupta et al., Reference Gupta, Anupama and Ramakrishna2021).
Social interactions are proposed as a basic human need, similar to other fundamental needs, such as consumption of food or sleep (Baumeister and Leary, Reference Baumeister and Leary1995). Decreasing this interaction may have increased the levels of depression and anxiety (Xiao et al., Reference Xiao2020). Studies have proposed that public health emergencies can have many psychological effects on university students, which can be expressed as anxiety, fear, and worry (Mei et al., Reference Mei2011).
Students’ anxiety levels may be related to virus’s effects on their studies, future employment and exposure to social media (Cao et al., Reference Cao2020; Wang et al., Reference Wang2020b; Cornine, Reference Cornine2020); in addition, high anxiety levels associated with the fear of being infected by the virus may be even greater among health care university students who attend university hospitals. In the same direction, constant exposure to news and information about COVID-19 is positively associated with the prevalence of mental health-related problems (Gao et al., Reference Gao2020).
However, online communication can remedy negative feelings associated with social distance (Orben et al., Reference Orben, Tomova and Blakemore2020). Therefore, evidence has shown that certain aspects of digital communication can mitigate the consequences of social distance (Orben et al., Reference Orben, Tomova and Blakemore2020). Given those findings, it is reasonable to theorise that returning to classes, even online, during the social distancing period can minimise the negative effects of social isolation on the mental health of young university students.
In order to clarify this issue, the current study compared the frequency of anxiety and depression symptoms before and after returning to online classes in a convenience sample of university students during the period of social isolation related to coronavirus pandemic. The secondary aim of the study was to verify if the restriction level adopted by the volunteers was associated with anxiety and depression symptom levels.
The hypothesis of the present study is that the return online classes would reduce the frequency of anxiety and depression symptoms among health care university students.
Materials and methods
Experimental design
This was a quasi-experimental study due to the lack of a control group. The impossibility of recruiting volunteers who were not exposed to the coronavirus pandemic, social distancing rules or online classes prevented a control group inclusion in the study. The study was based on self-administered questionnaires applied on Google Forms® at two different moments.
First, the questionnaires were applied from June 22 to 25, 2020, 98 to 101 days since the end of presential classes on March 16, 2020, and secondly from August 15 to 19, 2020, 40 to 44 days after online classes began on July 6, 2020. The students stayed a total of 112 days without presential or on-line classes (from March 16to July 6, 2020) (Fig. 1).

Fig. 1. Dates of study data collections.
In both times, the questionnaires were identical and were divided into three sections. The first session covered general information such as age (open-ended question), sex (male or female), current academic program (medicine, biomedicine or other), year of study (open-ended question) and family income (less than a minimal wage, between 1 and 2 minimal wages, between 2 and 6 minimal wages, between 6 and 10 minimal wages or more than 10 minimal wages). Currently, the minimum wage in Brazil corresponds to $213. The second section had multiple-choice questions related to their behaviour during the quarantine, regarding the level of restriction adopted (total restriction without leaving home; partial restriction, leaving only for essential non-work activities; leaving only for essential activities, including work activities; or minimal or no restriction). The third section included two questionnaires translated and validated into Portuguese, to screen for depression (PHQ-9) and anxiety (GAD-7) status. The study was approved by the Human Research Ethics Committee of the Federal University of Sao Paulo (Approval number: 4.073.442) and conformed to the principles outlined in the Declaration of Helsinki.
Assessment of risk of depression
The Patient Health Questionnaire 9 (PHQ-9) is a self-administered questionnaire that was validated for Brazilian Portuguese and is used to identify individuals at the risk of depression (Kroenke et al., Reference Kroenke, Spitzer and Williams2001; Santos et al., Reference Santos2013). When examining the reliability of the PHQ-9, high internal reliability was demonstrated, with Cronbach’s alpha of 0.81 to 0.84 (Kroenke et al., Reference Kroenke2016). The PHQ-9 is composed of nine items scored using a Likert-type scale, ranging from ‘0’ (not at all) to ‘3’ (nearly every day); therefore, the PHQ-9 final scores range from 0 to 27. By calculating a summary score, the severity of a depressive episode can be assessed (Kroenke et al., Reference Kroenke, Spitzer and Williams2001; Santos et al., Reference Santos2013). Scores ≤4 indicate minimal depression, scores from 5 to 9 indicate mild depression, scores from 10 to 14 indicate moderate depression, scores from 15 to 19 indicate moderately severe depression, and scores of 20 or greater indicate severe depression (Kroenke et al., Reference Kroenke, Spitzer and Williams2001). After the depression level was assessed for each of the participants (minimal to severe), for the purpose of analysis, scores from 0 to 4 were assigned to the levels of depression, where 0 referred to the lowest level of depression (minimal depression) and 4 to the highest level of depression (severe depression).
Assessment of risk of anxiety
The General Anxiety Disorder-7 (GAD-7) is a self-administered questionnaire that was validated for Brazilian Portuguese and is used to identify anxiety disorders (Moreno et al., Reference Moreno2016; Spitzer et al., Reference Spitzer2006). The GAD-7 was an acceptable questionnaire, with Cronbach’s alpha of 0.89 (Löwe et al., Reference Löwe2008). The GAD-7 is composed of seven items scored using a Likert-type scale, ranging from ‘0’ (not at all) to ‘3’ (nearly every day). Therefore, the GAD-7 final scores range from 0 to 21. By calculating a summary score, the severity of a depressive episode can be assessed (Moreno et al., Reference Moreno2016; Spitzer et al., Reference Spitzer2006). Scores of ≤4 indicate no anxiety disorder, scores from 5 to 9 indicate mild anxiety, scores from 10 to 14 indicate moderate anxiety, and scores of 15 or greater indicate severe anxiety (Moreno et al., Reference Moreno2016; Spitzer et al., Reference Spitzer2006). After the anxiety level was assessed for each of the participants (no anxiety disorder to severe anxiety disorder), for the purpose of analysis, scores from 0 to 3 were assigned to the anxiety levels, where 0 referred to the lowest level of anxiety (no anxiety disorder) and 3 to the highest level of anxiety (severe anxiety disorder).
Participants
Students enrolled in undergraduate health science programs at the Federal University of São Paulo (São Paulo, Brazil) were invited to participate; the invitation letters were sent by email. The invitation was sent to all students and those who responded to the invitation participated in the study, so the selection of volunteers was not random.
The inclusion criteria included being familiar with online questionnaires, being over 18 years of age, and being enrolled in an undergraduate course at the Federal University of Sao Paulo in the health field. Volunteers who did not complete both stages of the study were excluded from the survey.
Eighty-five individuals of both sexes read the consent form, voluntarily agreed to participate in the research, and answered the questionnaire in June. However, 45 of those individuals failed to answer the questionnaire again in August and were excluded. Therefore, 40 individuals who provided informed consent and completed the questionnaires in both June and August were selected to participate in the study. The characteristics of the sample (n = 30 female and n = 10 male) are described in Table 1. The students, for whom the scores of anxiety and/or depression were severe, received an email after the study was finished. In the email, the students were referred to the Federal University of Sao Paulo health service for management. This service is constituted by physicians, nurses and other health professional providers.
Table 1. Descriptive characteristics of participants.

Values were expressed as mean ± SD (minimum-maximum).
Statistical analysis
According to the Kolmogorov–Smirnov test, no variables presented a normal distribution. The Wilcoxon test was used to verify differences between June and August according to the PHQ9, GAD7 and the restriction level adopted by the volunteers. The Mann–Whitney test was used to verify differences between those who completed one (June 2020) and both surveys (June 2020 and August 2020). Fisher’s exact test was used to verify the association level between the restriction level adopted and the PHQ-9 and GAD-7 responses. Statistical analysis was performed using SPSS v. 21.0 (Chicago, Illinois, USA). In all comparisons, p values < 5% were considered statistically significant.
Results
First of all, the difference in anxiety level (GAD-7) and depression level (PHQ-9) between those who answered the questionnaires only in June 2020 and those who answered in June 2020 and August 2020 was analysed. The group that answered the questionnaires only in June had 2 (0–3) for depression and 1 (0–2) for anxiety levels (data are expressed in median and interquartile range). The group that answered the questionnaires in June and August presented 2 (1–3) for depression and 1 (1–2) for anxiety levels. There was no significant difference between groups for depression (p = 0.247) and anxiety levels (p = 0.118).
The results described below refer only to those who answered the questionnaire in June 2020 and August 2020 (n = 40).
Of all participants who answer the questionnaire twice, five per cent referred family income less than a minimum wage, five per cent referred between 1 and 2 minimal wages, 52.5% referred between 2 and 6 minimal wages, 22.5% referred between 6 and 10 minimal wages, and 15% referred more than 10 minimal wages. Forty-five per cent were medical students, 40% were biomedical, and five per cent were from other health care courses. Forty per cent were first-year students, 17.5% were second-year students, 27.5% were third-year students, five per cent were fourth-year students, five per cent were fifth-year students and five per cent were sixth-year students.
Regarding the level of restriction adopted in June, 20% of the participants (n = 8) practised social distancing and did not go out to perform any activity, 70% (n = 28) maintained partial restrictions, leaving only for essential non-work activities, 10% (n = 4) maintained partial restrictions, leaving only for essential activities including work activities, and none of them reported not taking measures of social distance.
The second time the students completed the questionnaires, in August, 12.5% (n = 5) were still practising social distancing and did not go out to perform any activity, 72.5% (n = 29) maintained partial restriction, leaving only for essential non-work activities, 5% (n = 2) maintained partial restriction, leaving only for essential activities, including work activities, and 10% (n = 4) did not take any measures of social distancing. Comparing the restriction level adopted by the volunteers in June to August, there was a significant reduction in the restriction level over time (Z = −2.07; p = 0.04).
Concerning the levels of depression, there were significant differences between the scores presented before and after the return to the online classes (Z = −2.27; p = 0.02). Fig. 2 shows a frequency histogram of PHQ9 scores before and after the return to the online classes.
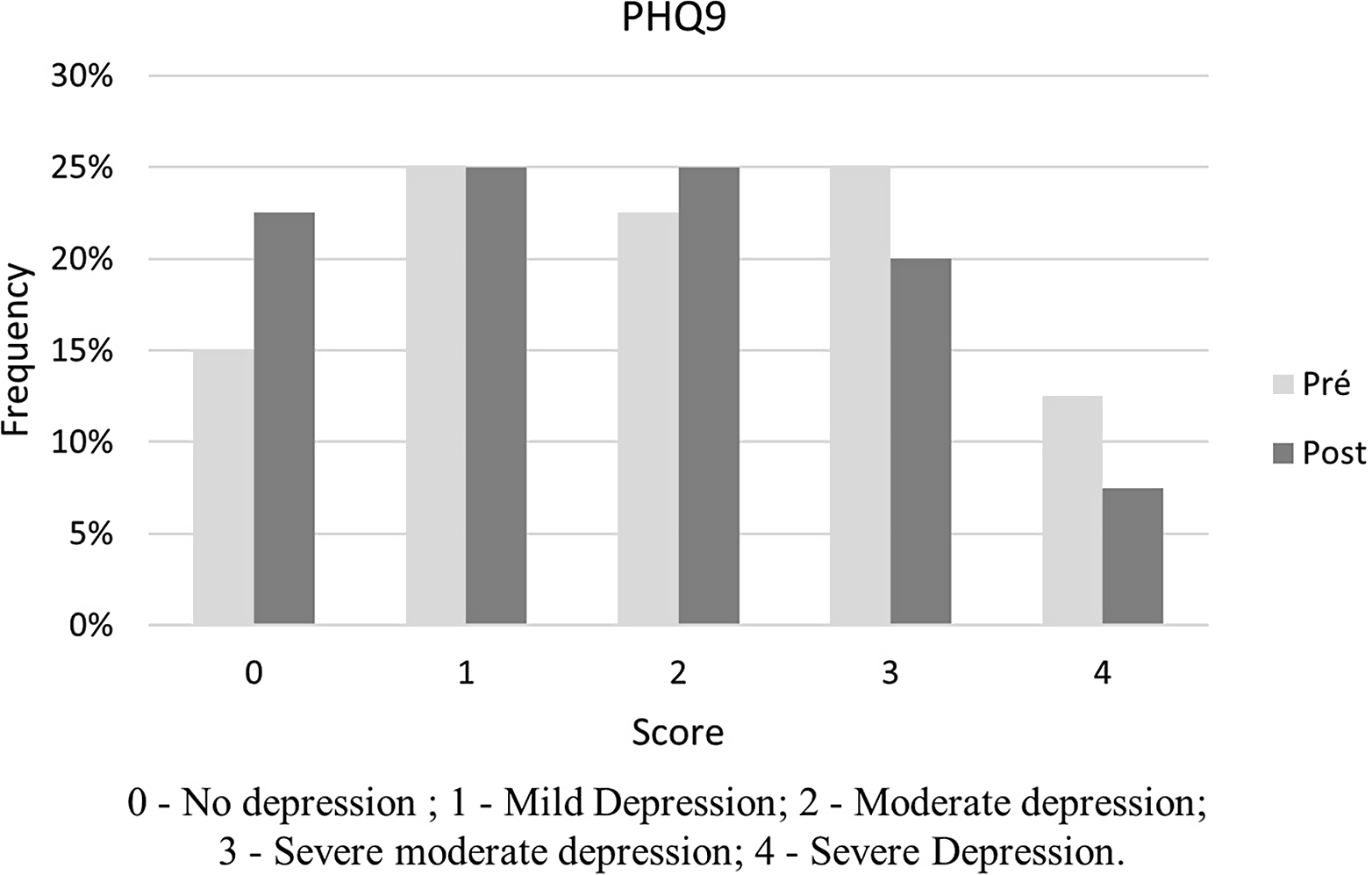
Fig. 2. Depression level score frequency histogram.
Regarding anxiety status, there was no significant difference after the return to the online classes (Z = −0.51; p = 0.61). Fig. 3 shows a frequency histogram of GAD7 scores before and after the return to online classes.
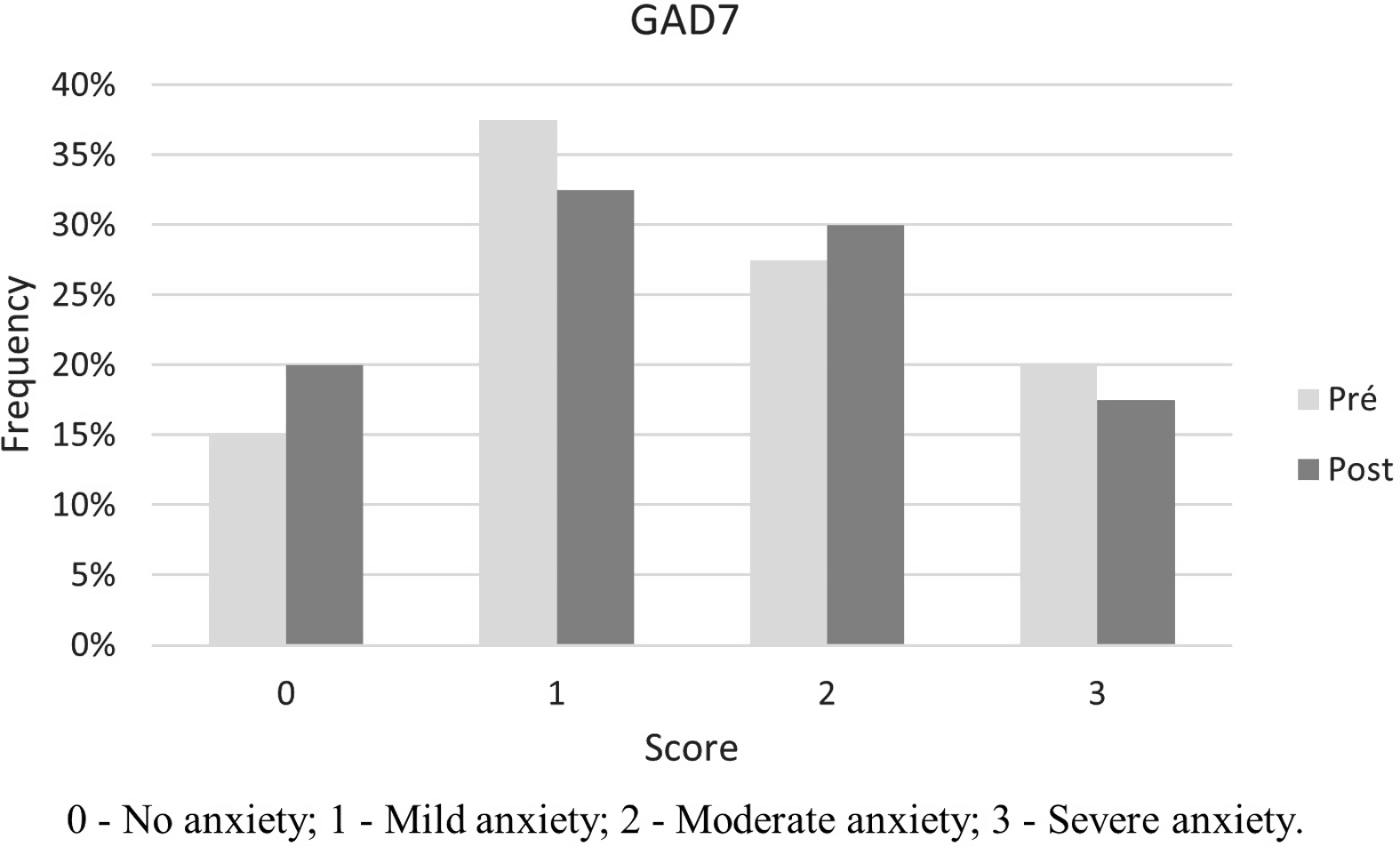
Fig. 3. Anxiety level score frequency histogram.
According to the association level between the restriction level and the depression or anxiety status, the results of Fisher’s exact test showed no significant association for PHQ9 (p = 0.25) and GAD7 (p = 0.25).
Discussion
The main findings of the present study were (i) returning to online educational activities had a positive effect on students’ depression levels; (ii) there were no changes in anxiety levels after the return to online educational activities; (iii) there was a significant difference in the level of restriction before and after the return to online classes; and (iv) the level of restriction was not associated with depression or anxiety level. These findings may help us to understand the importance of the interaction promoted by educational activities, even if they only occur online.
It is known that mental health disorders are more likely to occur and worsen in the absence of interpersonal communication (Xiao et al., Reference Xiao2020). The student population may be more vulnerable to the effects of social distancing, once they are more susceptible to stress-related anxiety and depression (Wang et al., Reference Wang2020a; Rajkumar, Reference Rajkumar2020). In addition, anxiety and depression have been shown to be very common among medical students in whom social detachment was reported with longer screen times and less healthy lifestyles (Xiao et al., Reference Xiao2020).
In the present study, 60% of the volunteers showed moderate or severe depression levels, which is comparable with previous data. It was found that the prevalence of depression among undergraduate students of health sciences in everyday situations can reach alarming levels such as 54.3% (Alim et al., Reference Alim2017) and 52.2% (Mamun et al., Reference Mamun, Hossain and Griffiths2019). During the COVID-19 outbreak, Islam et al. (Reference Islam2020), when investigating 476 university students living in Bangladesh, found that 82.4% of the students experienced a mild to severe depression. In a sample of 1134 Pakistani students, 45% of those investigated had symptoms of moderate or severe depression (Salman et al., Reference Salman2020). Medical students in Beijing and Wuhan, the epicentre of the epidemic, had a prevalence of depression symptoms of around 25.3%, mainly mild (Xiao et al., Reference Xiao2020), and a large cross-sectional online survey with 44 447 college students conducted in Guangzhou showed a prevalence of symptoms of depression in 12.2% of participants (Wang et al., Reference Wang2020c).
After the students resumed academic activities, even if not in person (only online classes), the frequency of depression symptoms decreased significantly, suggesting that the return to classes and the whole social issue that the return to activities have a positive impact on students’ mental health. In June, 60% of the students presented moderate or severe symptoms of depression, and in August, only 43% presented. The lower depression frequency observed in August more closely resembled the frequency presented by other studies from different countries.
The present results also showed an extremely high frequency of moderate and severe symptoms of anxiety (48%). Cao et al. (Reference Cao2020) indicated that 24.9% of 7143 medical students in a Chinese sample experienced anxiety because of the outbreak of COVID-19. Of these students, 0.9% experienced severe anxiety and 21.3% experienced mild anxiety (Cao et al., Reference Cao2020). Wang et al. (Reference Wang2020a) showed a lower prevalence of anxiety symptoms in Chinese students (7.7%). Salman et al. (Reference Salman2020) studied Pakistani university students and obtained values of prevalence of moderate to severe symptoms of anxiety in 35% of the students.
Nevertheless, the results of the present study did not show a significant change in anxiety levels after the return of educational activities, failing to support the hypothesis presented.
It is worth mentioning that the level of social restriction adopted by the students was significantly different between the two evaluations, and this fact might be considered a bias for the present study. In August, the students adopted less restricted behaviour than in June, and this difference may also impact their mental health. However, this concern may be alleviated because the level of restriction adopted did not show a positive association with the frequency of depression or anxiety systems. Another possible limitation of the present study is that the volunteers had to answer a questionnaire, alone, on two different occasions, and we do not know how much the level of impairment of mental health may influence the students’ lack of motivation to adhere to the study protocol. It is possible that the level of depression is even higher, but the most affected individuals may not have had the motivation to answer the questionnaire.
Strengths of the study include its originality, evaluating the return to educational activities of health students, in view of the unprecedented magnitude of this pandemic. In addition, the study may further assist in future research on the psychological aspects of the student population. Limitations include the convenience sampling strategy based on electronic forms answered voluntarily by the students; therefore, it is possible that the most depressed students did not answer the questionnaire due to lack of motivation. The investigated population was not evaluated prior to the appearance of the virus; therefore, temporal inferences are limited, and there are no more data about personal history of formal mental health diagnosis. Moreover, self-reported scales were used, and the frequency of symptoms of anxiety and depression was expected to be less reliable than those measured by a mental health professional.
The results of this study indicate that returning to online classes can mitigate the high frequency of depression symptoms observed during the social distancing measures adopted during the outbreak of COVID-19. Given these findings, we suggest evaluating the importance of maintaining a service that offers psychological interventions to students after a period of crisis, such as that presented by the COVID-19 outbreak. This can be used as an example to reinforce the need to rethink the importance of educational activities that prepare future professionals in the health workforce to cope with similar situations. In addition, there is also a need to reinforce measures to deal with stressful situations, especially the adoption of healthy habits and exercises.
Acknowledgements
The authors would like to thank all those who responded to the questionnaire.
Authors contributions
Conception and design of the work AS, PJP, LV and MSA; Data collection AS, PJP, LV; Data analysis and interpretation AS, PJP, LV RLV, CABL, PTN, TR, BK and MSA; Drafting the article AS, PJP and LV; Critical revision of the article RLV, CABL, PTN, TR, BK, MSA
Final approval of the version to be published AS, PJP, LV and MSA.
Financial support
None.
Statement of interest
None.
Ethical standards
The study was approved by the Human Research Ethics Committee of the Federal University of Sao Paulo (Approval number: 4.073.442) and conformed to the principles outlined in the Declaration of Helsinki.





 Open access
Open access