



As a highly emotionally evocative task (Hajal & Paley, Reference Hajal and Paley2020), parenting poses a regulatory challenge for many individuals (Rutherford et al., Reference Rutherford, Wallace, Laurent and Mayes2015). The emotion regulation demands of parenting are unique across different stages of children’s development – when children are young (such as in infancy and toddlerhood), the demands of parenting require a hands-on, moment-to-moment involvement in the regulation of children’s emotional needs, but as children transition to the school-aged years, the parent–child relationship develops into what has been termed a “supervision partnership,” wherein children and parents share the responsibility for monitoring children’s safety and well-being (Koehn & Kerns, Reference Koehn and Kerns2021). During this latter developmental stage, the emotion regulation tasks of parenthood may be more complex if less hands-on – parents have less information regarding their children’s emotional experiences and must wait at the ready to traverse children’s highs and lows alongside them should their support be requested, yet must also know when to step back and allow children to deal with challenges independently – all while managing the feelings that emerge when this push-pull dynamic occurs (Borelli et al., Reference Borelli, St. John, Cho and Suchman2016). However, regardless of developmental stage, parents’ emotion regulation strategies have a profound impact on their well-being in the parenting role as well as on children’s emotion regulation (Kerr et al., Reference Kerr, Buttitta, Smiley, Rasmussen and Borelli2019; Nelson et al., Reference Nelson, Kushlev, English, Dunn and Lyubomirsky2013; Rutherford et al., Reference Rutherford, Wallace, Laurent and Mayes2015) and risk for psychopathology (Beauchaine, Reference Beauchaine2015; Compas et al., Reference Compas, Jaser, Bettis, Watson, Gruhn, Dunbar, Williams and Thigpen2017), making parental emotion regulation strategies an important focus of investigation.
Benefits of relational savoring as a parenting emotion regulation strategy
Use of healthy emotion regulation strategies can assist parents in accessing the benefits embedded within everyday parent-child interactions to increase their positive affect and the meaning they derive from their relationships with their children. Imagine a parent who experiences significant or frequent stressors in their parenting interactions – perhaps they do not have enough support at home or their child has learning challenges. It is easy for this parent to become overwhelmed by the difficulties they encounter throughout the day. Yet, at the end of every day, that parent’s 8-year-old son cuddles up to her and asks her to rub his back. He tells her he has been looking forward to this massage all day long because it helps him get rid of the stress he feels throughout the day. And he says to her, “There’s nobody else I love more in this world than you – you make me feel so safe.” After the child has gone to bed at night, this parent could spend time worrying about the parenting moments that were harried and stressful throughout the day (such as when they had power struggles over getting him to complete his homework or brush his teeth) and the implications his misbehavior will have for his future development, or she could spend time reflecting on those 5 min of bliss that she had with her son when he told her how much their connection meant to him. She could remember all of the details of the moment that made it special (the way he smelled, how soft his skin was, the sound of his sweet voice) and think about how much it means to both her and him that she is able to create that kind of love and relationship for him, allowing herself to become immersed in the positive emotions of the memory so that she prolongs them and reflects on their significance. One of these emotion regulation strategies is more likely to improve her emotional state than the other, and as we argue, the extent to which she engages in this positive emotion regulation strategy will have implications for her son’s emerging emotion regulation capacity and ultimately, his mental health.
The current study focuses on the emotion regulation strategy of savoring, which involves carefully attending to positive moments and deeply processing them (Bryant & Veroff, Reference Bryant and Veroff2017). As an emotion regulation strategy, savoring is positively associated with well-being and inversely associated with risk for mental health problems (Hurley & Kwon, Reference Hurley and Kwon2013; Smith & Hollinger-Smith, Reference Smith and Hollinger-Smith2015). Relational savoring (RS), an attachment-based subtype of savoring, involves recalling, re-experiencing, attending to, and processing moments of positive connection with a close other, such as with one’s child (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020). Engaging in RS helps parents step back from parenting duties and reflect on what makes a moment with their child special. It offers a chance for parents to appreciate small, yet powerful positive moments of connection they share with their children (Bond & Borelli, Reference Bond and Borelli2017; Burkhart et al., Reference Burkhart, Borelli, Rasmussen and Sbarra2015). Parents can savor a specific time when they felt connected to or in-sync with their child, ranging from something as mundane as a time spent laughing over a joke or something as major as partnering to run a 5K race together.
To effectively savor relational memories, parents must be able to focus on a specific moment when they felt close to their child, but not all parents are able to identify or recall these memories. That is, there are individual differences in parents’ ability to engage in this practice (Bond & Borelli, Reference Bond and Borelli2017). For instance, some parents experience difficulty delving into and reflecting on their emotions and thoughts, while others experience frequent interruptions from unrelated or negative thoughts (see Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020, for a review). Indeed, “certain people may be more inclined than others to mute their own joy and excitement,” which can get in the way of effective savoring (Bryant & Veroff, Reference Bryant and Veroff2017, pp. 200–220). In addition to its utility as a naturally occurring emotion regulation strategy, RS can also be taught to parents in the form of a parenting intervention program. Predictors of differences in parents’ ability to engage in RS are important to identify when using RS as an intervention to improve parents’ emotion regulation abilities; that is, understanding who is best suited for a parenting intervention involving RS and who may require additional supports will enable clinicians to best utilize this method (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020). Given the potential positive effects of RS for parents and for their relationships with their children, it is important to identify ways to adapt RS so that all parents can derive deeper meaning from this practice. In the current study, we focus on identifying predictors of individual differences of the degree to which parents are able to engage with RS, as exemplified by the quality of their RS narratives. We also examine the degree to which individual differences in savoring quality predict variability in children’s physiological emotion regulation. Doing so enables us to identify which parents may benefit from RS interventions, as well as what the potential implications of poor use of RS are for children.
Even though studies of individual differences in regulating positive affect exist (e.g., Nelis et al., Reference Nelis, Quoidbach, Hansenne and Mikolajczak2011; Quoidbach et al., Reference Quoidbach, Berry, Hansenne and Mikolajczak2010), only a handful of studies to date demonstrate individual differences in parents’ ability to recollect connected moments with their children through RS. Working with parents of school-aged children, Bond and Borelli (Reference Bond and Borelli2017) demonstrated that self-reported maternal romantic attachment insecurity and rumination were negatively associated with RS proficiency. In a sample of parents of toddlers, Borelli, Burkhart et al. (Reference Borelli, Burkhart, Rasmussen, Smiley and Hellemann2018) found that self-reported attachment avoidance was associated with less secure attachment content in RS narratives. These preliminary studies suggest that it is possible to identify individual difference factors associated with RS proficiency and that more investigation is needed. In the current study, we focus on two additional candidate factors for poorer RS – one factor that may be associated with reduced ability to experience pleasure (depressive symptoms) and one that may be associated with lower levels of proficiency in understanding the significance of the savored experience (reflective functioning).
Predictors of proficiency in RS
One possible predictor of poorer ability to engage in RS is depressive symptomatology. Parents struggling with depression might have difficulty savoring experiences with their children – compared to non-depressed parents, they report fewer positive interactions with their children (Lovejoy et al., Reference Lovejoy, Graczyk, O’Hare and Neuman2000) and greater difficulty in meeting their children’s social and emotional needs (Goodman & Gotlib, Reference Goodman and Gotlib1999). Having fewer positive experiences to draw upon, such parents may generate fewer positive relational memories to savor; in fact, people diagnosed with depression recall fewer and less specific positive autobiographical memories (Lemogne et al., Reference Lemogne, Piolino, Friszer, Claret, Girault, Jouvent, Allilaire and Fossati2006; Williams et al., Reference Williams, Barnhofer, Crane, Herman, Raes, Watkins and Dalgleish2007; Young et al., Reference Young, Bellgowen, Bodurka and Drevets2015), which could also manifest as a lower capacity to recall relational memories. Further, executive functioning skills are impaired among people with depression (see Snyder, Reference Snyder2013, for a review), which could include impaired memory functions. Even after a memory is retrieved, a parent who is higher in depressive symptoms might have difficulty savoring with as much depth and positivity as a parent with lower levels of depression. Associated features of depression include anhedonia and rumination (Beblo et al., Reference Beblo, Fernando, Klocke, Griepenstroh, Ashchenbrenner and Driessen2012; Feldman et al., Reference Feldman, Joormann and Johnson2008; Min’er & Dejun, Reference Min’er and Dejun2001), factors that might affect a parent’s ability to react to positive stimuli, including memories involving relationships with close others. Depressive symptoms could also impact parents’ ability to sustain positive emotions during the process of RS (Carl et al., Reference Carl, Soskin, Kerns and Barlow2013; Heller et al., Reference Heller, Johnstone, Shackman, Light, Peterson, Kolden, Kalin and Davidson2009). Consistent with these speculations, Bryant (Reference Bryant2003) found that among college students, those who were more depressed were less likely to reminisce about positive memories, focus on positive moments in the present, and anticipate positive events. This theorizing and preliminary research from Bryant (Reference Bryant2003) suggest that parents with higher depressive symptoms may be less likely to engage in RS, and when asked to do so, may generate memories that are of lower quality or process them less deeply.
A second possible predictor, mentalizing or one’s ability to conceptualize the self and others from the perspective of mental states (Fonagy et al., Reference Fonagy, Target, Steele and Steele1998; Slade, Reference Slade2005), could also affect one’s ability to participate in RS. Mentalizing can be operationalized as reflective functioning (Fonagy et al., Reference Fonagy, Gergely, Jurist and Target2002), or the degree to which people utilize mental states as vehicles for understanding themselves and others. The capacity to mentalize is thought to originate in one’s early attachment relationships – interactions with caregivers who promote a feeling of attachment security enable some children to be able to explore their thoughts and feelings, develop a vocabulary regarding mental states, and come to understand their own emotional experiences through contingent mirrored interactions (Fonagy et al., Reference Fonagy, Gergely, Jurist and Target2002). Adults with high reflective functioning are able to understand how emotions, thoughts, and desires motivate behaviors, as well as how one person’s mental states could affect those of another, whereas people with low reflective functioning reason about others’ behavior by focusing on behavior and personality, at times disavowing emotional states (Fonagy et al., Reference Fonagy, Target, Steele and Steele1998). In the context of parenting, parental reflective functioning (PRF) enables parents to mentalize for themselves or for their child (Slade, Reference Slade2005), drawing connections between thoughts and feelings of the self and the child. Understanding the thoughts and feelings underlying a child’s behavior and making connections between feelings experienced within the parenting role and parenting behaviors are two components of PRF that predict greater sensitivity in interactions with one’s child (Borelli et al., Reference Borelli, Hong, Rasmussen and Smiley2017; Suchman et al., Reference Suchman, DeCoste, Leigh and Borelli2010). For instance, a parent with high RF may be able to infer why a child behaves in a way that is puzzling (e.g., acting uncomfortable when a friend gives them a birthday surprise because they are embarrassed by the extra attention) and reflect on the reason for their own discomfort or annoyance at their child’s reaction. Parents with high PRF might use this as an opportunity to talk to their child about how they were feeling in that situation.
RS, whose depth is enhanced by the savorer’s ability to reflect on mental states in themselves and their child – for example, being in touch with one’s feelings related to a positive event (Bryant & Veroff, Reference Bryant and Veroff2017) – ought to be of higher quality among parents with higher PRF, because the ability to reason about the child’s thoughts and feelings should enrich the parent’s ability to experience more depth in their savoring. For instance, a parent who thinks back on a time when they helped their child achieve a goal and feels happiness about being able to be there for their child will be able to achieve only a certain depth of feeling when engaging in RS. A parent who is able to delve further, mentalizing about their child, might be able to appreciate that this milestone meant something special to the child – perhaps the parent appreciates that the child had been highly anxious about meeting the goal in the first place. The parent may also understand that their support allowed the child to take this risk and push herself further than she would have been able to on her own. Understanding her child’s mental states (anxiety, nervousness) and their contribution to the significance of this accomplishment for the child, especially in the context of the parent’s own behavior (parental support enhancing child confidence, ultimately enhancing the connection between the parent and child), will deepen the feelings associated with the event and enhance its meaning and significance. The results of one past study partially support this claim: among parents of toddlers, higher self-reported PRF was associated with more positive content in RS narratives (Burkhart et al., Reference Burkhart, Borelli, Rasmussen, Brody and Sbarra2017). However, links between coder-rated PRF, a more robust measure of PRF, and RS proficiency have not been tested, and the links between PRF and RS proficiency have scarcely been tested among parents of school-aged children, leaving a gap in the literature. As is the case with depression predicting proficiency in RS, it is important to evaluate whether PRF predicts RS because identifying factors that are associated with RS can help identify who would benefit more from savoring interventions, as well as who would need additional supports (e.g., more intervener support) within savoring interventions.
Links between parents’ emotion regulation and children’s emotion regulation
Parents’ ability to regulate their emotions is central to children’s ability to manage their own emotions (Bariola et al., Reference Bariola, Gullone and Hughes2011; Dix, Reference Dix1991; Eisenberg et al., Reference Eisenberg, Cumberland and Spinrad1998), which in turn is a key predictor of risk for psychopathology (Beauchaine, Reference Beauchaine2015; Compas et al., Reference Compas, Jaser, Bettis, Watson, Gruhn, Dunbar, Williams and Thigpen2017). Given the frequency with which emotions arise in the family context, children have ample opportunities to witness their parents’ methods of regulating emotions as well as their success in regulating them (Hajal & Paley, Reference Hajal and Paley2020). Children are thought to imitate parents’ emotion regulation strategies (using modeling and social referencing; Bridges et al., Reference Bridges, Denham and Ganiban2004; Cole et al., Reference Cole, Michel and Teti1994; Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007); internalized emotion regulation strategies then have projecting impacts onto children’s ability to regulate their own positive and negative emotion, an important developmental capacity.
In middle childhood, a period that is characterized by growth in the neurological and cognitive underpinnings of emotion regulation, emotion regulation capacity matures rapidly (Yap et al., Reference Yap, Allen and Sheeber2007). This developmental period precedes adolescence, a time when emotional experiences are frequent and intense (Larson & Lampman-Petraitis, Reference Larson and Lampman-Petraitis1989). During this phase, meta-analytic evidence suggests that stronger emotion regulation is negatively associated with psychopathology (Compas et al., Reference Compas, Jaser, Bettis, Watson, Gruhn, Dunbar, Williams and Thigpen2017), with some evidence for a more robust negative relation between emotion regulation and internalizing psychopathology as children age.
Emotion regulation can be measured by assessing expressed emotion and behavior, subjective experience, and physiological activation. One advantage of assessing physiological activation as a measure of emotion regulation is that it provides an unobtrusive measure of emotion regulation that can be measured during standardized laboratory tasks (Buske-Kirschbaum et al., Reference Buske-Kirschbaum, Jobst, Wustmans, Kirschbaum, Rauh and Hellhammer1997; Fry & Gatzke-Kopp, Reference Fry and Gatzke-Kopp2021; Wilson et al., Reference Wilson, Lengua, Tininenko, Taylor and Trancik2009); further, it sidesteps issues related to reporting biases. Respiratory sinus arrhythmia (RSA) is one such index of physiological regulation, or the ability to adapt to changes in the environment. As RSA is controlled by the parasympathetic nervous system through the vagus nerve, it is considered a measure of cardiac vagal control (Friedman & Thayer, Reference Friedman and Thayer1998; Porges, Reference Porges1995). Here we consider the maintenance of higher RSA levels during stress as a marker of a child’s ability to handle with relative ease a cognitive stressor such as the unsolvable puzzles we present to them, rather than needing to devote considerable physiological resources to attempting to withstand or overcome the challenge.
Links between children’s emotion regulation and psychopathology
In what follows, we review the research evidence on the links between RSA and both emotion regulation and psychopathology in children. When RSA is measured at baseline, higher RSA is associated with more optimal outcomes, including fewer negative responses to environmental and social stressors in adults and children (El-Sheikh et al., Reference El-Sheikh, Harger and Whitson2001; Fabes & Eisenberg, Reference Fabes and Eisenberg1997), greater self-regulatory capacity (Segerstrom & Nes, Reference Segerstrom and Nes2007), and better regulation of negative facial expressions (Demaree et al., Reference Demaree, Robinson, Everhart and Schmeichel2004, Reference Demaree, Pu, Robinson, Schmeichel and Everhart2006). However, when RSA is measured in response to laboratory tasks, findings are mixed as to whether higher or lower RSA is associated with more optimal outcomes for children. Some studies find that lower levels of RSA during stress is associated with more negative outcomes, including psychopathology (Borelli et al., Reference Borelli, Hilt, West, Weekes and Gonzalez2014; Boyce et al., Reference Boyce, Quas, Alkon, Smider, Essex and Kupfer2001; Calkins et al, Reference Calkins, Graziano and Keane2007) and other studies finding the opposite, that higher levels of RSA during stress is associated with more negative outcomes, including psychopathology (El-Sheikh et al., Reference El-Sheikh, Harger and Whitson2001; Gentzler et al., Reference Gentzler, Santucci, Kovacs and Fox2009; see Graziano & Derefinko, Reference Graziano and Derefinko2013, for a meta-analysis).
So what is unclear is the direction of the effect; though it is clear is that there is a link between RSA activity and adjustment (Beauchaine, Reference Beauchaine2015). Youth who are able to physiologically regulate in response to environmental stressors are less likely to resort to maladaptive coping, and therefore are more resilient in the face of stress and less likely to develop psychopathology across the transition to adolescence (Compas et al., Reference Compas, Jaser, Bettis, Watson, Gruhn, Dunbar, Williams and Thigpen2017). Examining the physiological correlates of emotion regulation in children is vital due to its demonstrated associations with psychopathology, especially given the increased risk for mental health problems such as depression and anxiety during this developmental phase (Costello et al., Reference Costello, Copeland and Angold2011). In line with our prior findings (Borelli et al., Reference Borelli, Hilt, West, Weekes and Gonzalez2014), we predict that higher levels of RSA during a stressor task indicate superior physiological regulation, insofar as individuals who do not exhibit RSA down-regulation are not substantially challenged by the stressor.
Parents’ proficiency in RS and children’s emotion regulation
Although the developmental psychology literature is replete with studies examining links between parents’ and children’s emotion regulation (e.g., Milojevich et al., Reference Milojevich, Machlin and Sheridan2020; Peisch et al., Reference Peisch, Dale, Parent and Burt2020; Shih et al., Reference Shih, Quiñones-Camacho and Davis2018), less work has focused on the association between parents’ use of strategies to up-regulate positive emotions and their association with children’s emotion regulation. Existing studies suggest that parental positive affectivity and the quality of parent-child relationships are linked to the development of better emotion regulation strategies in early and middle childhood (Eisenberg et al., Reference Eisenberg, Valiente, Morris, Fabes, Cumberland, Reiser and Losoya2003; Gentzler et al., Reference Gentzler, Ramsey and Black2015; Lunkenheimer et al., Reference Lunkenheimer, Olson, Hollenstein, Sameroff and Winter2011). For example, parents who can express and maintain positive emotions have school-aged children who are better able to regulate their emotions (Eisenberg et al., Reference Eisenberg, Valiente, Morris, Fabes, Cumberland, Reiser and Losoya2003). The reasons underlying these links are diverse, but likely include upward spirals of positive interactions that build upon each other in the context of secure parent-child relationships and/or the physiological undoing of negative emotion (Fredrickson, Reference Fredrickson2001; Kok & Fredrickson, Reference Kok and Fredrickson2010; Mikulincer & Shaver, Reference Mikulincer and Shaver2007; see Ramsey & Gentzler, Reference Ramsey and Gentzler2015, for a review).
Given that RS involves parents’ up-regulation of positive emotion, we expect that a parent’s proficiency in RS will be associated with their child’s physiological emotion regulation capacity. To date only one study has examined the link between RS and physiological activation – this was a study of older adults’ (ages 60–90) heart rate during a relational as compared to a personal (focused on individual experiences) savoring intervention, controlling for their heart rate during a mindfulness task. This study found that adults randomized to the RS condition exhibited significantly lower heart rates, suggestive of more adaptive emotion regulation (Borelli et al., Reference Borelli, Bond, Fox and Horn-Mallers2019). Given the preliminary nature of the field, much remains to be learned of the associations between parents’ RS proficiency and children’s physiological emotion regulation, the subject of the current investigation.
Integrated model: parents’ emotion regulation (RS proficiency) as an indirect link between their baseline psychological characteristics and their children’s emotion regulation
Finally, parents’ proficiency at RS, a measure of emotion regulation, could be a bridge by which aspects of parents’ psychological functioning, namely their depressive symptoms and PRF, are linked to children’s physiological regulation. We predict that parents’ depressive symptoms and PRF will individually predict their RS proficiency, which in turn will predict children’s physiological emotion regulation. In other words, parents’ superior ability to savor moments of positive connection with their child, predicted by low depressive symptoms and high PRF, should create a climate in which the child will develop better physiological regulation during stress (indicated by the maintenance of higher mean levels of RSA, which we contend indicates superior regulation insofar as the stressor presents less of a regulatory challenge).
Current investigation
The current study investigates the relationship between parents’ psychological functioning (depression, PRF), proficiency in RS, and children’s physiological regulation, an index of emotion regulation (see Figure 1). We focus our investigation on middle childhood, a developmental phase that has been relatively neglected within the parent-child literature. During this phase, parent-child relationships transition to a supervision partnership in which children begin to bear greater responsibility for maintaining closeness and connection with their parents (Kerns, Reference Kerns2008). Parents’ RF shifts as their direct knowledge of the child’s experiences decreases and they begin to rely more and more on children sharing important experiences with them and their history with the child to inform their understanding of the child’s perspective (Borelli et al., Reference Borelli, St. John, Cho and Suchman2016; Mayseless, Reference Mayseless2005; Rubin et al., Reference Rubin, Bukowski, Parker, Damon and Eisenberg1998). Further, as the developmental phase immediately preceding adolescence, this is an important period during which to understand children’s regulation and parents’ capacity to savor their relationships with their children. The foundation for healthy adolescent functioning is likely set during these middle childhood years.
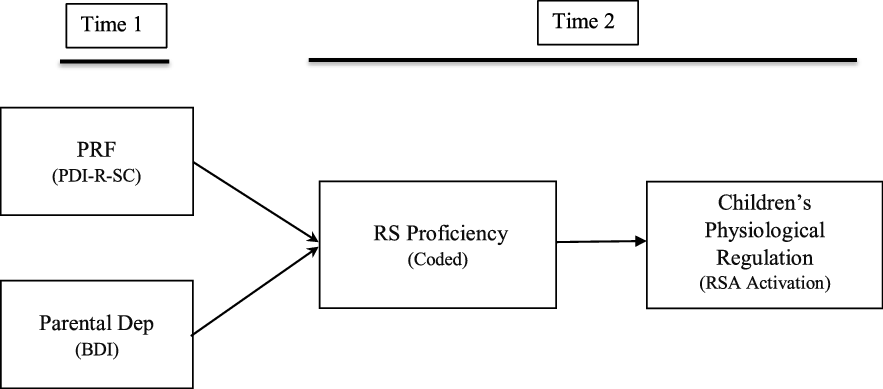
Figure 1. Proposed theoretical model of predictors and correlates of relational savoring quality. PRF = parental reflective functioning; PDI-R-SC = Parent-Development Interview-Revised for School-aged Children; RS = relational savoring; Dep = depressive symptoms; RSA: respiratory sinus arrhythmia. Note: Time 1 and Time 2 were separated by 1.5 years.
Working with an ethnically diverse and thus generalizable community sample of parents of school-aged children, we asked parents complete the Beck Depression Inventory (BDI; measure of depressive symptoms) and the Parent Development Interview-Revised for School-Aged Children (PDI-R-SC; Slade et al., Reference Slade, Aber, Berger, Bresgi, Kaplan and Borelli2009; measure of PRF) at Time 1. At Time 2 (1.5 years later), parents returned to the laboratory and completed an assessment of RS proficiency. Their children completed a laboratory stressor during which we assessed their levels of RSA activity during unsolvable puzzles. After being taught puzzle-solving strategies, children completed an initial solvable puzzle (control task) followed by four puzzles that were, unbeknownst to the children, unsolvable. Their mean levels of RSA during these four puzzles served as the measure of stressor-related change in RSA, after controlling for their RSA during the initial solvable puzzle. Higher mean levels of RSA during the stressor task indicate superior regulation, insofar as higher activation indicates less challenge from the stressor.
We tested three hypotheses in this longitudinal investigation. First, we predicted that both parental depressive symptoms and PRF measured at Time 1 (T1) would be individually predictive of savoring proficiency at Time 2 (1.5 years later; Hypothesis 1). Second, we hypothesized that parents’ proficiency in RS would be positively associated with their children’s physiological regulation, assessed as mean RSA levels during a stressful task (Hypothesis 2). Finally, we tested a mediation model, wherein T2 RS proficiency would indirectly link T1 parental depressive symptoms and T1 PRF to children’s RSA levels during a stressor at T2 (Hypothesis 3).
Method
Participants
The data presented here were collected as part of a larger, Institutional Review Board-approved investigation of children’s development at Pomona College (Child Emotion Study, 02042011JB-CS1). Participants were recruited through advertisements posted online and at local meeting spaces (e.g., coffee shops, parks) in a Southern California suburban community. Parents who self-identified as primary caregivers (N = 139; 8.9% fathers, 91.1% mothers; M age = 37.55 years, SD age = 6.25) with a child between 8 and 12 years old (43% male; M age = 9.72, SD age = 1.47) participated in this longitudinal study spanning a 1.5 year period. The sample was diverse in terms of ethnicity (38.7% Hispanic/Latino/a, 33.6% Caucasian, 18.5% African American, 1.7% Asian, 3.4% Native American, and 4.2% other) and socioeconomic status (50% of the parents reported an income of less than US $40,000 per year).
As this was a longitudinal study, we experienced attrition in our sample between Time 1 and Time 2 assessments. This was particularly the case because at Time 1, we were not anticipating conducting a Time 2 data collection, and thus we did not take steps to stay in contact with them during the time between the two assessments. At Time 1, there were N = 139 participants enrolled in the study who completed some portion of the Time 1 assessment. 123 of these provided complete Time 1 data (i.e., completing both the assessment visits at Time 1). At the Time 2 assessment (1.5 years later), n = 73 participants were available and indicated a willingness to complete the Time 2 study. We conducted independent samples t-tests and Chi-square analyses to evaluate whether there were any differences between those participants who did and did not complete the Time 2 assessment. The participants did not significantly differ on any variables assessed (PRF, parental depression scores, income, education, child age, parent age, child gender, or parent gender), enhancing our confidence in the wisdom of utilizing all data within our possession to build our models.
Procedure
Parents completed an initial assessment (T1), in which they reported on individual- and family-level demographics and their depressive symptoms. Parents also completed a semi-structured interview about their parenting experiences (Parent Development Interview-Revised for School-aged Children, PDI-R-SC; Slade et al., Reference Slade, Aber, Berger, Bresgi, Kaplan and Borelli2009), which was later transcribed verbatim and coded for PRF. Approximately 1.5 years later (Time 2), parents returned to complete the RS task (Bond & Borelli, Reference Bond and Borelli2017) while their children completed an assessment battery that included measurements of their RSA levels while completing one solvable and four unsolvable puzzles.
Measures
Parental reflective functioning
Parents completed the PDI-R-SC (Slade et al., Reference Slade, Aber, Berger, Bresgi, Kaplan and Borelli2009), a modification of the PDI-R (Slade et al., Reference Slade, Aber, Bresgi, Berger and Kaplan2003) for use with parents of school-aged children (see Borelli et al., Reference Borelli, St. John, Cho and Suchman2016; Stern et al., Reference Stern, Borelli and Smiley2015). The PDI-R-SC is a semi-structured interview consisting of 23 questions probing parents’ emotional experiences in parenting (What gives you pain or difficulty as a parent?), parent-child interactional quality (Can you tell me about a time when you and your child were not clicking?), as well as parents’ understanding of their children’s emotions (Can you tell me about a time when your child was upset?). The majority of the questions include follow-up probes regarding parents’ and children’s emotions during each situation discussed.
Standard PDI-R administration involves audio recording the interviews, transcribing them verbatim, and having trained and reliable coders rate each transcribed interview for PRF. Parents’ responses to each question receive an RF score on an 11-point scale ranging from −1 (bizarre, anti-reflective) to 9 (marked; Slade, Bernbach et al., Reference Slade, Bernbach, Grienenberger, Levy and Locker2005). Low scores indicate distortion or denial in parents’ perception of their child’s emotional experiences, whereas high scores indicate acknowledgement of their own and their child’s emotions and the effect of those emotions on behavior. Raters then consider a participant’s scores across the 23 questions on the interview and use them to assign an overall or global RF score to the interview. In the current study, two certified trainers in the coding of PRF (one of whom is the first author of this paper) trained a new coder in the RF coding scheme for the PDI-R until she achieved adequate reliability on a different sample of parent interviews. Then, this coder rated the entire sample of PDI-R-SC’s from the current study without any information about the interviews. The senior author of this paper double-coded a portion of these interviews to establish reliability within this sample: Intraclass correlation coefficients (two-way random effects ICCs, consistency) for the individual PDI questions on n = 25 interviews ranged from 0.76 to 0.94.
Depressive symptoms
Parents reported on their depressive symptoms using the BDI (Beck et al., Reference Beck, Steer and Brown1996). The BDI is a widely used, 21-item measure – for each item, participants are presented with a series of statements describing the cognitions, emotions, and behaviors associated with depressive symptomatology and are asked to select the statement that best describes them over the past two weeks. Participants receive a score ranging from 0 to 4 for each item, with higher scores indicating more severe symptomatology. The BDI yields a total score for depression ranging from 0 to 63; scores between 13 and 19 indicate mild depression and scores above 29 indicate clinical depression (Beck et al., Reference Beck, Steer and Brown1996). Psychometric properties of the scale are well documented (Beck et al., Reference Beck, Steer and Brown1996). In the current study, internal consistency of the measure was high (α = 0.88); 11.9% of participants reported mild depression and 9.2% reported clinical depression.
Coder-rated RS
Parents’ ability to savor their positive emotional connections with their children was measured using a writing task modeled after extant protocols for online or in-person administration of RS (Borelli et al., Reference Borelli, McMakin and Sbarra2010, Reference Borelli, Hilt, West, Weekes and Gonzalez2014). Parents were asked to write a narrative response to a standardized prompt asking them to describe and reflect on a moment of shared connection with their child:
For this next task, we would like you to think of a positive emotional experience you have had with your child and write about this memory. This could be something as simple as enjoying a good meal together or laughing over a funny joke, or it could be something as major as taking a vacation or accomplishing a big task together. Try to focus on a single memory of a time when things seemed at their best between you two. Using as much detail as possible, describe the situation and how you felt at the time (think about specific details and how you were feeling—What were you doing? What kinds of feelings were you feeling?). Spend a few minutes thinking about your response before beginning to write, imagining what it was like to have been there. Write as much, or as little, as you feel comfortable with.
To evaluate parents’ RS proficiency, we applied a coding system used in prior studies of RS (Bond & Borelli, Reference Bond and Borelli2017; Burkhart et al., Reference Burkhart, Borelli, Rasmussen and Sbarra2015, 2016). Raters evaluated RS proficiency in terms of three main factors: (1) degree of positivity (To what extent is the parent demonstrating a positive emotional tone when describing the memory?), (2) degree of emotional connectedness to children (To what extent does the parent appear to be emotionally connected to the memory they are describing of the child?), and (3) level of detail/vividness of the description (to what extent is the memory the parent is describing detailed, vivid, or precise? How in the moment does the parent seem when they are describing the memory?). In this study, eight trained coders rated all of the transcripts using a five-point scale, with higher numbers indicating greater savoring proficiency. Participants’ RS proficiency score was the average of all 8 raters’ scores. The coding yielded high inter-rater reliability (two-way mixed effects average measures ICCs = 0.95).
Children’s stressor task
To assess children’s emotion regulation, we adapted a laboratory stressor task previously used with younger children (Smiley et al., Reference Smiley, Coulson, Greene and Bono2010) that involved assembling two-dimensional geometric puzzles modeled after the Block Design Task on the Wechsler Intelligence Scale for Children (WISC-III-R; Wechsler, Reference Wechsler1991). For our older sample, we increased the difficulty level of the puzzles and programmed it for presentation on a 20.5” computer monitor (see Borelli et al. (Reference Borelli, Smiley, Bond, Buttitta, DeMueles, Perrone, Welindt, Rasmussen and West2015), Borelli, Burkhart et al. (Reference Borelli, Burkhart, Rasmussen, Smiley and Hellemann2018), Smiley et al. (Reference Smiley, Buttitta, Chung, Coffey, Wang and Borelli2016, Reference Smiley, Rasmussen, Buttitta, Hecht, Scharlach and Borelli2020), for examples of the use of this paradigm and modified versions of this paradigm).
Children in the present study were asked to complete a series of nine-piece (3 × 3) geometric puzzles, using two-dimensional “tiles” that were either all red, all white, or half white and half red, split on the diagonal. For each trial, a reduced-size image of the completed puzzle appeared in the upper left corner of the computer screen, an empty square outlined in black was shown in the center of the screen, and an array of nine tiles was displayed next to the square frame. Children were shown how to use a mouse to drag tiles from the array into the frame; tiles snapped into place when dragged to one of nine (unmarked) locations in the frame.
At the start of the task, experimenters trained children to complete some demonstration puzzles; more specifically, children were taught six strategies they could use for solving the puzzles (e.g., matching the corner tiles first). Children were then given a practice puzzle to solve on their own. The experimental protocol involved the presentation of six puzzles in the following order: one solvable puzzle (Solvable 1; baseline task), four unsolvable puzzles (stressor task), and one solvable puzzle. For the solvable puzzles, all nine of the necessary tiles were provided, but for the unsolvable puzzles, eight correct tiles and one incorrect tile were provided. Solvable puzzles were untimed, but unsolvable puzzles were displayed on the screen for a fixed period of time (70 seconds). At the end of the 70-second period, a cartoon “frown face” popped up on the right side of the screen to indicate that the puzzle had not been solved. For the solvable puzzles, a cartoon “smiley face” popped up to indicate successful completion of the puzzle.
Children’s physiological regulation
Children’s RSA was assessed during the puzzle task using disposable Mindware 1.5-in. foam EKG electrodes with 7% chloride wet gel, and a BioNex eight-slot chassis equipped with an impedance cardiograph (Mindware Technologies, Gahanna, OH). BioLab 2.5 acquisition software and BioLab HRV 2.0 application software were used to collect and edit the data for peak errors and noise (Mindware Technologies, Gahanna, OH).
Prior to the training phase of the puzzle task, experimenters connected electrodes to the children’s upper bodies and tested the signals to make sure electrodes had been placed accurately and were functioning well. Children were instructed to remain as still as possible. The experimental stimuli were presented using Eprime Version 2.0 (Psychology Software Tools, 2002; Schneider, Eschman, & Zuccolotto, 2007), which also sent start/stop recording signals to the physiological data collection program, Biolab (Mindware Technologies, Gahanna, OH). During the puzzle task, physiological data collection was broken into 70-second segments for each puzzle (60 segments for each puzzle with 10 seconds in between), beginning when the puzzle was first presented on the screen. Mean RSA across the four 60-second time periods for the unsolvable puzzles was utilized as the measure of physiological activation during stress. Mean RSA during an initial solvable puzzle (the first 70 seconds) was used as a control. Sixteen participants’ data were excluded from statistical analyses due to computing equipment error (e.g., Eprime malfunction during paradigm; n = 11) or unusable signals (n = 5).
Data analytic plan
Prior to hypothesis testing, we reviewed descriptive statistics, inter-item correlations, and patterns of missing data for all study variables, using SPSS version 27 (Enders, Reference Enders2010). Little’s MCAR test revealed that the data were missing completely at random, Chi-square (20) = 15.39, p = 0.76. Hypotheses were tested in a path analysis in Mplus 8.0 (Muthén & Muthén, Reference Muthén and Muthén1998-2017), using full information maximum likelihood (FIML) estimation to account for missing data. FIML uses all available data to estimate parameters and yields unbiased parameter estimates under either the missing at random or missing completely at random assumptions (Enders & Bandalos, Reference Enders and Bandalos2001). The path analysis model included parental depression and PRF as predictors of parental RS, parental RS as a predictor of children’s RSA, and two indirect effect paths: 1) the indirect effect of parental depression on children’s RSA via parental RS and 2) the indirect effect of PRF on children’s RSA via parental RS. These indirect effects were assessed using bias-corrected bootstrapped confidence intervals, with 1000 draws, as recommended by Preacher and Hayes (Reference Preacher and Hayes2008). Parent gender and child gender were included as covariates in all equations, and children’s RSA during a solvable puzzle task was included as a covariate in equations predicting children’s RSA during the unsolvable puzzle task. Before interpreting model parameters, we examined model fit using indices recommended by Kline (Reference Kline2015): the Chi-square test of model fit (where χ2 p > 0.05 indicates failure to reject the null hypothesis that the model fits the data), root mean square error of approximation (where RMSEA <0.08 indicates acceptable model fit and <0.05 indicates good model fit), comparative fit index (where CFI >0.90 indicates good model fit), and the Standardized Root Mean Square Residual (where SRMR <0.08 indicates good model fit). For ease of interpretation, standardized results are presented from the path analysis model.
Results
Descriptive statistics
Descriptive statistics and zero-order correlations for key variables are reported in Table 1.
Table 1. Descriptive statistics and correlation matrix for key variablesa

Note. P = parent; C = child; PRF = Parental Reflective Functioning; RS: Relational Savoring Proficiency; Dep = Depressive Symptoms; RSA-solvable: Children’s mean respiratory sinus arrhythmia during solvable puzzles; RSA-insolvable: Children’s mean respiratory sinus arrhythmia during insolvable puzzles.
aRaw data used in these analyses, with pairwise deletion for missing data.
bbaseline control task.
cmean score across the four puzzles, *p < 0.05.
Independent samples t-tests revealed that as compared to parents who did not identify as Latino/a, those who did were significantly younger, t(121) = 2.56, p = 0.01. No other differences emerged in key study variables between parents who did and did not identify as Latino/a. We also examined differences in key study variables as a function of child gender and parent gender. We found that parents of girls had higher parental RF, t(121) = −1.99, p = 0.04, and girls in the study were significantly older than boys, t(121) = −3.07, p = 0.003. Mothers reported higher depression scores than fathers, t(121) = −2.49, p = 0.02.
Zero-order correlations revealed that proficiency of RS was negatively associated with parental depression and positively associated with PRF and children’s RSA. Given that child gender and parent gender were associated with key study variables, we included these as covariates in subsequent analyses.
Hypothesis testing
All hypotheses were tested in a single path analysis model, which demonstrated a good fit to the data across indices (χ2 = 1.52, df = 1, p = 0.22; RMSEA = 0.06; 90% CI [0.00, 0.24]; CFI = 0.98; SRMR = 0.03).
Hypothesis 1: Are T1 depressive symptoms and PRF individually predictive of RS proficiency? As shown in Table 2, after controlling for parent and child gender, higher T1 depressive symptoms were associated with lower proficiency of RS at T2, β = −0.36, SE = 0.12, p = 0.004, and higher PRF at T1 predicted greater proficiency of RS at T2, β = 0.25, SE = 0.12, p = 0.04.
Table 2. Indirect and total effects

Note. RSA = Respiratory Sinus Arrhythmia; RF = Reflective Functioning; All analyses controlled for child and parent gender. Analyses reporting RSA during stressor controlled for baseline RSA.
Hypothesis 2: Is the proficiency of parents’ RS associated with children’s physiological regulation? After controlling for parent and child gender and children’s RSA during a solvable puzzle task, proficiency of parents’ RS at T2 was positively associated with children’s mean levels of RSA during the unsolvable puzzle task at T2, β = 0.37, SE = 0.12, p = 0.002 (see Table 2). The children of parents with greater proficiency in savoring showed evidence of better physiological regulation (i.e., high RSA levels high during the stressor task).
Hypothesis 3: Does proficiency in RS link parental depressive symptoms and PRF to children’s physiological regulation? As displayed in Table 2, after controlling for parent and child gender as well children’s RSA during the solvable puzzle task, parental depression showed an indirect effect on children’s physiological regulation (mean RSA during the unsolvable puzzle task) via parental savoring proficiency, β = −0.13, SE = 0.07, 95% C.I. [−0.04, −0.003]. There was no significant direct effect, β = 0.05, SE = 0.14, 95% C.I. [−0.02, .06] or total effect (β = −0.09, SE = 0.15, 95% C.I. [−0.05, 0.02] of parental depression on children’s physiological regulation.
Similarly, the indirect effect of PRF on children’s physiological regulation through parental savoring proficiency was significant (β = 0.09, SE = 0.06, 95% C.I. [0.01, 0.24]); there was no significant direct effect (β = −0.09, SE = 0.10, 95% C.I. [-0.35, .06]) or total effect (β = 0.002, SE = 0.11, 95% C.I. [−0.18, 0.18]) of PRF on children’s physiological regulation.
Discussion
The major aims of the study were three-fold: 1) to examine parental depression and PRF as predictors of RS proficiency, 2) to investigate the association between RS proficiency and children’s physiological regulation during a stressful task, and 3) to examine whether parental depression and PRF indirectly effect children’s physiological regulation via parental RS proficiency. If proficiency in RS, an emotion regulation strategy that parents can use to bolster their positive emotions and their relationships with their children (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020), is associated with children’s emotion regulation, understanding factors that predict proficiency in RS can help to identify parents that should be targeted for RS interventions.
Associations between depressive symptoms, PRF, and RS
Our results demonstrate that, consistent with theory, high parental depressive symptoms and low PRF each individually predict lower proficiency in RS. First, with respect to the link between depressive symptoms and RS, parents with high depressive symptoms might have had difficulty recalling positive memories at the start of the task or difficulty sustaining positivity until the end of the task. Past studies support these explanations - depressed individuals or formerly depressed people are more likely to show deficits in recalling positive memories vividly (Bergouignan et al., Reference Bergouignan, Lemogne, Foucher, Longin, Vistoli, Allilaire and Fossati2008; Lemogne et al., Reference Lemogne, Piolino, Friszer, Claret, Girault, Jouvent, Allilaire and Fossati2006), are faster to disengage from positive stimuli (Levens & Gotlib, Reference Levens and Gotlib2010), and have difficulty upregulating the neural activation circuits of positive stimuli (Heller et al., Reference Heller, Johnstone, Shackman, Light, Peterson, Kolden, Kalin and Davidson2009). It is also possible that parents with higher depressive symptoms do not recall connected moments with their children in a positive light to begin with, either because they have fewer positive interactions with their children, because they have difficulty recalling the details of positive interactions with their children (making their memories less specific and detailed), or because they experience less joy when they recall those memories. Any of these patterns could result in these parents being less proficient in RS. In the current study, participants completed an assessment of RS proficiency on their own, in which they wrote out RS narratives. In a follow-up intervention study, mothers spent with a face-to-face intervener who could help with identifying positive memories to savor (Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022); in future analyses it would be interesting to identify whether mothers with higher depressive symptoms had poorer quality savoring proficiency in this intervener-supported savoring context.
Second, parents with lower PRF also show lower proficiency in RS, as hypothesized. Parents with lower PRF may have difficulty exploring and articulating their own emotions, including the feeling of joy in parenting (Bryant & Veroff, Reference Bryant and Veroff2017), or they may have found their children’s emotional states less accessible to imagination (Slade, Reference Slade2005). These barriers may result in lower RS proficiency if parents had more difficulty with conjuring up the details of their memories, and consequently, with creating meaning from the memories they recalled. These findings add to what has previously been demonstrated with respect to self-reported PRF (Burkhart et al., Reference Burkhart, Borelli, Rasmussen, Brody and Sbarra2017); that is, in the current study, we have shown that coder-rated PRF is also associated with RS proficiency. Our interpretation of these findings is that greater precision in accessing and describing emotional experiences creates a more vivid and layered emotional tapestry – it sets the stage for a more textured memory to savor and thereby, for more meaningful savoring. For example, one participant with a high PRF score recounted an event when her son gave her a hug for letting him go sit with his friend at a baseball game. Instead of vaguely describing the scene as pleasant, the mother delves deeper, articulating how her son felt appreciated that his mother was giving him a choice to sit with his friend without making him feel guilty for wanting to leave his seat next to her, and how they felt connected and accepting of each other when they shared a hug. By describing her child’s and her own emotions in detail, the participant was able to extract more meaning from this seemingly mundane incident.
We also know that at least for some parents and as predicted by the theoretical model (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020), PRF is enhanced through RS interventions. The results of recent investigations show that RS or RS-based interventions enhance PRF for Latina mothers (Borelli, Yates et al., Reference Borelli, Yates, Hecht, Cervantes, Russo, Arreola, Leal, Torres and Guerra2020; Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022) or Latino/a parents high in attachment avoidance (Goldstein et al., Reference Goldstein, Kerr, Li, Campos, Sbarra, Smiley and Borelli2019). Taken together, these findings suggest that higher PRF predicts better quality RS, and that when exposed to an RS intervention, Latino/a parents show increases in PRF. In other words, PRF may create more opportunities to engage in meaningful RS, and engaging in RS may also result in more proficiency in mentalizing, at least for some parents. In prior work, we have argued that due to its focus on positive emotion in the context of close interpersonal connections, RS may hold particular congruence with Latino/a cultural values of familism and simpatía (Acevedo et al., Reference Acevedo, Herrera, Shenhav, Yim and Campos2020; Campos & Kim, Reference Campos and Kim2017; Senft et al., Reference Senft, Campos, Shiota and Chentsova-Dutton2020), which may in part explain the beneficial effects observed within this group (Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022).
Associations between RS and children’s RSA
As hypothesized, we found that parents’ proficiency in RS was associated with children’s higher mean levels of RSA during stress, after covarying for RSA during a lower-stress task, which has been interpreted as a marker of better autonomic regulation insofar as it indicates less need to downregulate RSA to meet the demands of a stressor (Kok & Fredrickson, Reference Kok and Fredrickson2010). To be clear, we propose that more optimal regulation is indicated by children’s maintaining a higher mean level of RSA when challenged, although as discussed earlier, it is important to keep in mind that there is evidence within the literature for both higher (Borelli et al., Reference Borelli, Hilt, West, Weekes and Gonzalez2014; Boyce et al., Reference Boyce, Quas, Alkon, Smider, Essex and Kupfer2001; Calkins et al, Reference Calkins, Graziano and Keane2007) and lower RSA levels (El-Sheikh et al., Reference El-Sheikh, Harger and Whitson2001; Gentzler et al., Reference Gentzler, Santucci, Kovacs and Fox2009; see Graziano & Derefinko, Reference Graziano and Derefinko2013, for a meta-analysis) in response to laboratory tasks is associated with more optimal outcomes. Our findings are consistent with our theoretical model that higher task-related RSA indicates reduced need to respond to a stressor; nonetheless, it is important to keep in mind that there are conflicting findings in the literature.
Very few studies have demonstrated a link between parents’ use of positive emotion regulation or co-regulation strategies and children’s physiological activation, especially in this middle childhood age range (Delgadillo-Chase et al., Reference Delgadillo, Boparai, Pressman, Goldstein, Bureau, Schmiedel, Backer, Broekman, Hian Tan, Chong, Chen, Zalta, Meaney, Rifkin‐Graboi, Tsotsi and Borelli2021: preschoolers); thus, this finding in and of itself constitutes a contribution to the literature. Savoring is one means by which parents can engage in the up-regulation of the positive emotion they experience in their relationships with their children, that in turn, may have downstream consequences for their children’s physiological regulation. These effects may be transmitted via emotion co-regulation (wherein a caregiver serves as the external regulator responding to a child’s emotional needs; Fonagy et al., Reference Fonagy, Gergely, Jurist and Target2002) or modeling (where the child learns by observing the parent’s actions; Bandura, Reference Bandura1971; Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007). That is, when parents use RS or other means to up-regulate their own positive emotion, children might benefit in terms of experiencing emotional flexibility (as a result of co-regulation) that, in turn, is reflected in physiological equanimity (Delgadillo-Chase et al., 2020; Ramsey & Gentzler, Reference Ramsey and Gentzler2015).
RS indirectly links depressive symptoms and PRF to children’s RSA
When tested within a mediated path model, we showed that the association between parental depressive symptoms and children’s RSA is indirectly, but not directly, linked via parents’ RS proficiency; similarly, the effect between PRF and children’s RSA was indirectly, but not directly, linked via parents’ RS proficiency. This pattern indicates that for parents with high depressive symptoms, low RS proficiency helps to explain why their children show lower mean levels of RSA (i.e., less optimal patterns of physiological regulation) during the stressor (unsolvable puzzles) at the Time 2 assessment, after controlling for RSA activation during the solvable puzzle (i.e., baseline), and child and mother age.
It is helpful to contextualize the parental depression and RSA finding with prior studies. Two studies that examined RSA in mother-adolescent dyads did not find a simple association between maternal depression and adolescents’ RSA (Connell et al., Reference Connell, Hughes-Scalise, Klostermann and Azem2011; van Beveren et al., Reference Van Beveren, Mueller and Braet2019). However, Connell et al. (Reference Connell, Hughes-Scalise, Klostermann and Azem2011) found that teen RSA, maternal depression, and maternal RSA interacted to predict dyadic flexibility, suggesting that the role of maternal depression in physiological regulation within dyads may be more complex than a main effect. Likewise, we did not find a direct association between parental depression or PRF with children’s RSA activation at the bivariate level (see Table 1) nor within the path model – instead, our findings indicate that the links between parental depression and children’s RSA as well as between PRF and children’s RSA were indirect, through their mutual associations with parents’ RS proficiency. Further, in past research parental depressive symptoms have been associated with other indicators of children’s emotion dysregulation: young children (infants and preschoolers) of mothers with greater depressive and anxiety symptoms show more emotion reactivity (Harden et al., Reference Harden, Panlilio, Morrison, Duncan, Duchene and Clyman2017; Olino et al., Reference Olino, Klein, Dyson, Rose and Durbin2010; Pauli-Pott et al., Reference Pauli-Pott, Mertesacker and Beckmann2004; Wu et al., Reference Wu, Feng, Hooper and Ku2017) and less adaptive responses to emotion-inducing stimuli (Glöggler & Pauli-Pott, Reference Glöggler and Pauli-Pott2008). Further, maternal depressive symptoms measured in infancy predict later depression risk for children and adolescents (Bureau et al., Reference Bureau, Easlerbrooks and Lyons-Ruth2009). Our study expands upon this body of work by suggesting one potential mechanism for this association — poorer ability to savor positive moments of connection with one’s child — that might indirectly link parental depressive symptoms and children’s RSA.
Similar to the mediational analysis between parental depression and children’s RSA, the pathway from PRF to children’s RSA via parents’ savoring proficiency was significant, whereas the total and direct effects of PRF on children’s RSA were not significant. That is, although PRF did not directly predict children’s RSA, it significantly predicted RSA through savoring proficiency. Thus, in this study, we have evidence to suggest that higher PRF predicts better physiological regulation in children during a stressor (higher RSA) through parents’ superior engagement in RS. This is the first study to examine a potential mechanism underlying the link between PRF and children’s RSA. In fact, very few studies have directly examined links between PRF and children’s emotion regulation, despite ample discussion of the theoretical rationale for their association. One prior study found that higher levels of PRF were associated with greater correspondence of distress and adaptive coping in toddlers (as distress increased, so did adaptive coping; Borelli, Lai et al., Reference Borelli, Lai, Smiley, Kerr, Buttitta, Hecht and Rasmussen2020), which the authors conceptualized as a measure of emotion regulation. To our knowledge, that is the only previous study to directly examine the links between PRF and children’s emotion regulation. Another study found that children’s own RF was associated with higher RSA in response to a laboratory task (Borelli, Ensink et al., Reference Borelli, Ensink, Hong, Sereno, Drury and Fonagy2018). Expanding upon these findings, the current study suggests that parents’ ability to savor positive, connected moments with their children can explain the link between parents’ ability to mentalize and children’s stress regulation.
Implications
In a sample of parents who were mostly mothers, the propensity to engage in higher quality positive emotion regulation (RS) is associated with school-aged children’s higher RSA, which we interpret to be evidence of better physiological emotion regulation; this propensity to savor well is predicted by parents’ lower depressive symptoms and higher PRF. Given that our sample was mostly mothers, we do not know if our findings generalize well to fathers. We had advertised for primary caregivers, but the majority of the participating parents were mothers. Likewise, although our sample was diverse in terms of ethnicity, we were underpowered to examine ethnic group differences in the associations we observed. Especially given prior research documenting impacts by parent ethnicity on savoring outcomes (e.g., Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022), the urgency of examining the role of ethnicity and culture in predicting links between RS and associated constructs is high.
The mean PRF of the PDIs in this sample was 3.5, which is lower than is often seen in community (non-clinical) samples (Sleed et al., Reference Sleed, Slade and Fonagy2020, but see Anis et al., Reference Anis, Perez, Benzies, Ewashen, Hart and Letourneau2020). In a community sample collected by our research team in the same region but comprised of mothers of younger children (ages 18-26 months) several years later, the mean PDI score was 4.99 (SD = 1.15; Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022). In this second sample, which was similarly ethnically diverse, the household income level was higher (31% had an annual household income of under $40,000 as opposed to 50% of the current sample). As we have discussed previously (Borelli et al., Reference Borelli, St. John, Cho and Suchman2016), it is difficult to ascertain whether the lower than typical scores on the PDI-R-SC are due to children’s developmental stage or to the relatively lower income status compared to many prior studies of PRF (e.g., Slade, Grienenberger et al., Reference Slade, Grienenberger, Bernbach, Levy and Locker2005). In this sample, PRF was not related to parent educational attainment or income, which has also been shown within a community sample in a recent demographic study of the PDI (Sleed et al., Reference Sleed, Slade and Fonagy2020), providing additional suggestion that lower PRF could be related to the age of the children.
These findings have implications for the intergenerational transmission of psychopathology. Specifically, our findings revealed that parental depressive symptoms and children’s physiological activation during stress were indirectly linked through parents’ poorer proficiency savoring relational memories of their children. Given the evidence base suggesting that lower resting RSA are associated with depression (Yaptangco et al., Reference Yaptangco, Crowell, Baucom, Bride and Hansen2015) and depression-related constructs (e.g., rumination: Borelli et al., Reference Borelli, Hilt, West, Weekes and Gonzalez2014) in youth and emerging adults, and the general argument that aberrant patterns of RSA functioning are a transdiagnostic risk factor for mental health problems (Beauchaine, Reference Beauchaine2015), we believe that the findings presented here may provide a window into one developmental pathway to risk for psychopathology. Specifically, parents with more depression symptoms have a reduced capacity to utilize a positive emotion regulation strategy in the context of parenting (RS), which is linked to their children having reduced physiological regulatory capacity in the context of a laboratory stressor. The ability to up-regulate positive emotion, and to do so in the context of one’s experiences with one’s child, is important because it strengthens feelings of closeness within the relationship, increases positive emotion, and increases parents’ satisfaction in the relationship (Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022; Burkhart et al., Reference Burkhart, Borelli, Rasmussen and Sbarra2015). In addition, by increasing parents’ positive emotion, it can have stress-buffering effects, thereby helping parents to be resilient in the face of challenges. Parents who cannot access this type of emotion regulation strategy may be left with fewer psychological resources to manage stressors, which could impact their behavior with their children, with negative implications for children’s developing emotion regulation. The influence of parents’ emotion regulation on children’s emotion regulation has been described as operating through many different mechanisms, through processes such as modeling, social referencing, and co-regulation (Bridges et al., Reference Bridges, Denham and Ganiban2004; Cole et al., Reference Cole, Michel and Teti1994; Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007); these results suggest that greater positive emotion and valuing of the parent-child relationship (processes that underlie proficient RS) are additional mechanisms through which parents’ emotion regulation influences children’s emotion regulation.
The findings of this study also have implications for intervention development. RS is a naturally occurring emotion regulation strategy that can also be developed into an intervention program that is used to strengthen individual and interpersonal well-being (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020). Controlled intervention trials suggest that RS increases positive emotion, relationship satisfaction, and parent-child interaction quality (Borelli et al., Reference Borelli, Hilt, West, Weekes and Gonzalez2014, Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022; Burkhart et al., Reference Burkhart, Borelli, Rasmussen and Sbarra2015). Parents who are able to regularly savor relational memories, either through their own inclination or when taught to do so through an RS intervention, may experience benefits within the parent-child relationship in the form of deepening their feelings of connectedness with their child and improving their interactions with their child (Borelli, Smiley et al., Reference Borelli, Smiley, Kerr., Hong., Hecht., Blackard., Falasiri, Cervantes and Bond.2020; Borelli et al., Reference Borelli, Kerr, Smiley, Rasmussen, Hecht and Campos2022).
Based on this research on RS and prior work suggesting that both RS and general savoring are associated with psychological benefits (e.g., Bryant & Veroff, Reference Bryant and Veroff2017), we have reason to believe that helping parents learn this emotion regulation strategy is a worthy aim. Understanding the factors that are associated with less or more RS proficiency can assist in identifying people who may benefit most from the intervention. In future work, it will be important to first test whether parents who begin with the lowest capacity to savor (e.g., parents higher in depressive symptoms and parents lower in PRF) benefit from an RS intervention to the same, greater, or lesser degree as parents without these characteristics. If they benefit to the same or greater extent as other parents, this would be an argument to prioritize their enrollment in RS intervention programs, as our data suggest they currently do not engage in high quality RS on their own. If they benefit less than other parents, then it may signal that the RS intervention needs additional modifications in order to achieve more positive outcomes with these parents. For instance, for parents higher in depressive symptoms, the intervention could be modified by asking parents to engage in a positive task with their child immediately prior to the RS (e.g., playing with bubbles, reading a book together), which would give the intervener and the parent a fresh episode of positive connectedness to savor, eliminating the difficulty of the parent having to remember an episode of positive connectedness. Additionally, if the intervener observed the episode, then even if the parent did not perceive positivity within the interaction, the intervener could more readily identify details and moments of positive connectedness that would inform the savoring exercise. For parents with lower PRF, modifications could be made to the protocol such as slowing down in sections of the intervention that involve focusing on mental states so that the parent could practice tuning into their own and their child’s thoughts and feelings. The intervener could be more active in fostering and modeling mentalizing for the child and mother in early sessions, with the goal of increasing the parent’s independence as the sessions progress. Gathering assessments of depression and PRF prior to the start of the intervention would allow the intervention team to adjust their approach based on the pre-treatment characteristics of the parents.
Strengths and limitations
Our study examines, for the first time, associations of parental depressive symptoms and PRF with parents’ RS proficiency and children’s physiological regulation. Strengths of the study include a multi-method approach, a longitudinal design, and the inclusion of a diverse sample. Limitations include the fact that the putative mediator variable (parents’ proficiency in RS) and the dependent variable (children’s RSA) were measured at the same time point. Further, we did not measure our mediator or our dependent variable at multiple timepoints, so we are unable to speak to change over time in these constructs. Thus, even though our theoretical framework assumes causal relations, we cannot draw firm causal conclusions nor conclusions about temporal ordering of the effects shown. For example, because proficiency in RS and children’s RSA were collected at the same time, different interpretations can be made. Children who are better regulated might elicit greater sensitivity from their parents, which in turn may enable parents to better savor their shared moments. Ideally, in the future, our findings will be replicated with the variables assessed at three different time points. Finally, our sample was small, contained a substantial portion of missing data, and primarily consisted of mothers (91%), limiting the definitiveness of our conclusions and the generalizability of the findings. Here it is worth noting that when analyzed just using the raw data within regression models, the pattern of findings are similar, suggesting that when missing data is treated with FIML to produce parameter estimates using the full sample, patterns are similar to those present when examining only complete cases.
Additionally, as RS was measured through narrative responses, participants’ ability to express themselves in writing might have affected our assessment of proficiency in RS. Writing fatigue could have caused participants to disengage from this task. It should be noted that response length did not differ as a function of income or educational attainment (as reported in Bond & Borelli, Reference Bond and Borelli2017). Future researchers could ask participants to speak their thoughts aloud during RS, audio record, and transcribe their responses.
Conclusion
Our findings suggest that depressive symptoms and PRF are associated with an emotion regulation strategy - savoring positive moments of emotional connectedness. Further, parents’ capacity to savor moments of connection can have important implications for children’s emotion regulation development. In particular, RS proficiency helps to explain why parents’ depressive symptoms and children’s poorer physiological regulation are linked. Further, RS proficiency helps to explain the link between PRF and better children’s physiological regulation. Parents struggling with depressive symptoms or difficulty mentalizing might benefit from interventions that focus on the skills of PRF and RS.
Acknowledgements
The authors wish to thank the families who participated in the study as well as the members of the Pomona CARE and UCI THRIVE Labs who helped to collect and process the data and Christie Phamn for her assistance with copy-editing this manuscript.
Funding statement
This work was supported by a start-up grant awarded to J. Borelli and a small research grant awarded to P. Smiley.
Conflict of interest
None.




 Open access
Open access