



Child undernutrition, a condition due to energy and/or to macro- and micronutrient deficiencies, is characterised by stunting, underweight, wasting, and vitamin and mineral deficiencies(1). Worldwide, an estimated 144 million children under 5 years are stunted, 101 million are underweight and 47 million are wasted(2,Reference Black, Victora and Walker3) . The consequences of child undernutrition can be both short and long term, such as morbidities, mortality, cognitive, motor and language impairment, decreased adult stature, poor school performance, and decreased learning capacity resulting in decreased future earning potential(2). The direct and indirect cost of child undernutrition to an individual, family, nation and the world cannot be overlooked. In 2013, the cost of child undernutrition, including micronutrient deficiencies, was estimated at US$1·4 to 2·1 trillion/year, equivalent to 2 to 3 % of the global gross domestic product(4). Despite the negative consequences of child undernutrition, most of the root causes such as food insecurity, inappropriate child feeding practices and insufficient intake of energy content, vitamins and minerals are preventable(4). The pathway to prevention includes but not limited to the provision of adequate nutritious, diverse and safe diets to children, especially those who are the most vulnerable. It is globally acknowledged that this can be achieved during the complementary feeding phase, which is usually between 6 and 24 months of age. This phase starts when breast milk alone is no longer enough to meet the nutritional requirements of growing children, and thus other foods and liquids need to be introduced while breast-feeding continues(5,Reference Abeshu, Lelisa and Geleta6) . Notably, meeting the nutritional requirements of this age group is a challenge in most low- and middle-income countries (LMICs), communities, populations, and low-income households due to lack of resources to access nutritious food. Moreover, in these resource-limited settings and households, the complementary foods are often introduced too early or too late, given in smaller quantity, not given frequently enough and are of poor nutritional quality(Reference Abeshu, Lelisa and Geleta6–Reference White, Bégin and Kumapley9). A diet of poor nutritional quality has little variety in the food consumed and is low in micronutrients, particularly for Fe, Zn, vitamin A, iodine and essential fatty acids. It has been shown that the lack of dietary diversity and the poor quality of complementary foods in the short- and long-term impact negatively on the nutritional status and growth of children(Reference Dewey and Adu-Afarwuah10,Reference Onyango, Borghi and de Onis11) .
Animal-source foods such as eggs, meat, fish and dairy have been shown to be a suitable complementary food to be added to the usual diets of growing children, especially those in LMICs, communities, populations and low-income households who are vulnerable to undernutrition, because they have the potential to improve their nutritional and health status(Reference Iannotti12–Reference Grace, Dominguez-Salas and Alonso15). Foods from animal origin such as meat, eggs, fish and milk are known to be rich in nutrients such as protein, essential fats such as n-6 and n-3 fatty acids, vitamin A, Fe, Zn, choline and vitamin B12 needed to promote growth, motor and cognitive development of infants and young children, particularly those susceptible to undernutrition(Reference Iannotti12–Reference Eaton, Rothpletz‐Puglia and Dreker14,Reference Michaelsen, Dewey and Perez-Exposito16) . Despite the potential nutritional benefits of animal-source foods, it has been reported that children, particularly those in LMICs, communities, populations and low-income households are hardly given foods such as meat, eggs, fish and milk(Reference Grace, Dominguez-Salas and Alonso15). It should be noted though that previous studies from high-income countries advise against the introduction of cow’s milk in the main drinks of infants before 12 months of age due to it being a poor source of Fe; however, it was suggested that it can be added to complementary foods in small quantity(Reference Agostoni, Decsi and Fewtrell17). Hence, there is the need for high-quality studies that seeks to investigate the suitability of animal-based foods during complementary feeding on the growth, macro- and micronutrient status of children from high-income countries and resource-rich environment who may not have access to supplementation, fortified foods and/or drinks as well as well-planned vegan diet diets due to an increasing prevalence of the practice of vegetarian diets among caregivers(Reference Sutter and Bender18–Reference Louwman, van Dusseldorp and van de Vijver22). Against this background, previous and recent literature have shown that infants and young children, especially those from LMICs, communities, populations and low-income households are at high risk of growth faltering, macro- and micronutrient deficiencies due to inadequate consumption of animal-based protein-rich foods(Reference Agostoni, Decsi and Fewtrell17,Reference Alonso, Dominguez-Salas and Grace23–Reference Tang25) .
Previously, protein deficiency was considered the main determinant of undernutrition in resource-limited settings(Reference Semba26). This therefore led to the promotion of the provision of adequate energy content in the diet of children to improve their dietary protein intake(Reference Headey, Hirvonen and Hoddinott13). Proteins are needed by the body for building and maintenance of bones, muscles and skin. Dietary proteins act by promoting high circulating levels of insulin, insulin-like growth factor 1 and free triiodothyronine to stimulate bone and tissue growth(Reference Dror and Allen27). Additionally, the amino acids from dietary proteins play a role in the promotion of the synthesis of mechanistic target of rapamycin complex 1 (mTORC1), a catalytic protein that regulates cellular growth and differentiation. This catalytic protein acts on growth plates to enhance endochondral ossification, the process of bone formation. However, mTORC1 cannot be synthesised directly by the human body and so must be obtained from foods, of which the best food sources are animal-source foods such as eggs, fish, milk and meat(Reference Headey, Hirvonen and Hoddinott13,Reference Semba26) .
Thus, it is well acknowledged that the inclusion of animal-source foods to the usual complementary diets of growing children, especially those in LMICs, communities, populations and low-income households have the potential to optimise their nutritional status and thus help to alleviate child undernutrition(Reference Iannotti12,Reference Headey, Hirvonen and Hoddinott13) . Nevertheless, there is still dearth of evidence on the extent to which the addition of animal-source foods in the complementary diets of infants and young children, especially those in LMICs, communities, populations and low-income households enhance their growth and development. A recent Cochrane review published in 2019(Reference Eaton, Rothpletz‐Puglia and Dreker14) reported insufficient evidence to suggest that animal-source foods are effective complementary foods for growth and development in children aged 6 to 59 months from LMICs. Notably, the Cochrane review included only five studies(Reference He, Yang and Han28–Reference Tang, Sheng and Krebs32) in their quantitative synthesis. Additionally, recent feeding trials have focused on the effectiveness of daily consumption of an egg to improve child growth and development in LMICs, with discrepancies in linear growth outcomes(Reference Lannotti, Lutter and Stewart30,Reference Omer, Mulualem and Classen33,Reference Stewart, Caswell and Lannotti34) . Moreover, egg interventions are of great interest due to the cultural and religious beliefs associated with egg intake(Reference Lannotti, Lutter and Bunn35), especially in resource-limited settings. Recently, a systematic review on the effect of animal-based food on growth on 6 to 60 months children from LMICs pointed out a large heterogeneity among studies. This investigation resulted in the recommendation that subsequent studies should differentiate age groups. Another recommendation from this systematic review was that researchers should focus on the consistency in the definition and quantification of treatment and outcomes(Reference Shapiro, Downs and Swartz36).
Therefore, the primary objective of this systematic review and meta-analysis was to investigate whether the intake of animal-source foods accelerated the physical growth of children from LMICs, communities, populations and low-income households by using data from randomised controlled trials. Due to the availability of heterogeneous studies, we focused on previous evidence evaluating if animal-based food was a suitable complementary food that may help increase the Z-score of body size measures in children aged 6 to 24 months. The secondary objective was to ascertain the suitability of giving eggs on linear growth of children in LMIC, communities, populations and low-income household.
Methods
Eligibility criteria of included studies
Papers were selected according to the extended PICO (ST) principles. Notably, the target population (Population) was defined as children in the age range of 6 to 24 months. Papers were selected based on studies evaluating the effect of complementary animal-based food consumption of any natural origin (Intervention) with respect to no intervention or any other non-animal-based food supplementation (Comparison). We considered only studies reporting at least one measure of body size (Outcome). We included only randomised controlled trials (Study design) and was limited to papers published between 1 January 2000 and 1 August 2020 (Time) in peer-reviewed Academic Journals. We limited the literature search to papers published after 2000 to reduce methodological heterogeneity and optimise the study(Reference Cooper, Booth and Varley-Campbell37,Reference Petticrew38) . The Human Research Ethics Committee of the North-West University (NWU-00281-21-A1) approved this study.
Data sources and literature search
Medical Subject Headings (MeSH) and key terms were used to define a two-level hierarchical search string defined according to the above PICO (ST) inclusion criteria. Specifically, several MeSH items was defined for any of the above PICO (ST) elements, and the keywords search were linked by the OR/AND operators. Afterwards, several MeSH searched items, at least one for any PICO (ST) domain, were linked to the elements with the NOT operator to avoid the over selection of unwanted paper. Details of literature search strings are reported as a supplemental material, and Table 1 reports the PICO (ST) strategy. The literature search was conducted by searching electronic databases (MEDLINE, COCHRANE, EMBASE, CINAHL and Web of Science) and scanning the reference list of included studies, previous meta-analysis and systematic reviews.
Table 1. PICO (ST) criteria (participants, interventions, comparisons, outcomes and study design) used to define the research question

Study selection and risk of bias assessment
Study selection was conducted independently by two investigators (HA and CR) according to the Preferred Reporting Items of Systematic reviews and Meta-Analysis (PRISMA) guidelines (Reference Liberati, Altman and Tetzlaff39). Firstly, potential studies of interest were selected according to their titles and abstracts. Afterwards, the full text of all the potentially relevant studies were proofread for final eligibility. Papers reporting the effect of animal-source food supplementation v. no supplementation or non-animal-source supplementation on the length-for-age Z-score (LAZ), weight-for-age Z-score (WAZ), weight-for-length (WLZ), head circumference-for-age (HCAZ) and BMI-for-age (BMIZ) were further selected for the meta-analyses as secondary outcome measurements.
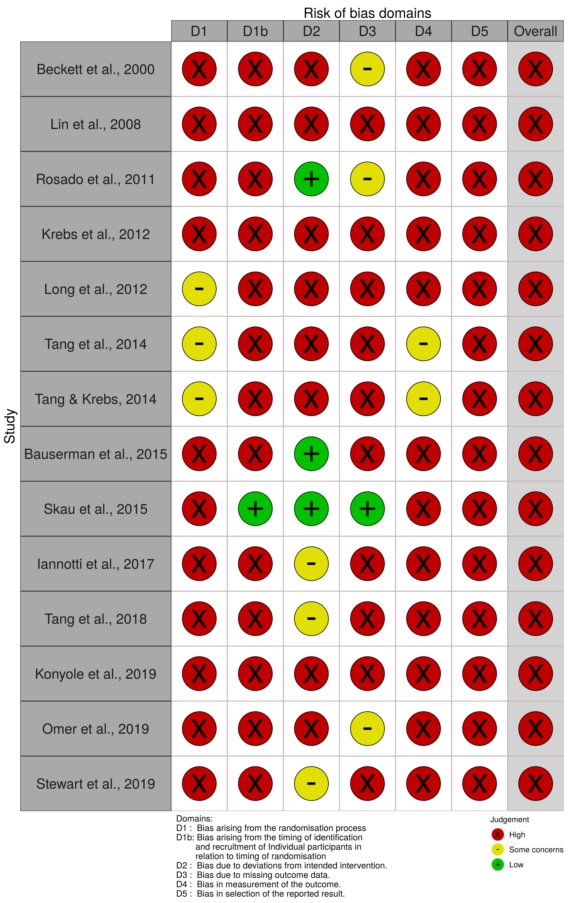
Two investigators (HA and CR) independently assessed the risk of bias according to the Cochrane Handbook for Systematic Review of Interventions. A qualitative three-level score (high, some concerns and low) was then attributed. Briefly, five different types of bias were scored. The use of a random sequence generation and allocation concealment were scored in two different sub-items to evaluate the selection bias. Performance bias (blinding of participants and operators), detection bias (blinding of outcome assessed), attrition bias (incomplete outcome data) and reporting bias (selective reporting of results) were coded by one item each. Any disagreements regarding study selection and risk of bias assessment were resolved by consensus. If no agreement was reached, a third author (CMS) was consulted to discuss and deliberate on the discrepancy or issue and to reach an agreement by all involved.
Statistical analyses
The meta-analysis for this study was based on the overall effect of the food consumption on stunting (primary outcome), underweight and wasting (secondary outcome). The values used were based on the reported difference between the treatment and the control group at the end of the study in the included papers. Specifically, unless already reported, treatment to control difference was computed as the difference between the mean Z-scores of the outcome indicator at the end of the study. The standard error was computed as the pooled standard error, s2 p = (n1-1) s2 1+ (n2-1) s2 2 /n1 + n2-2, where the subscripts 1 and 2 represent the two groups under evaluation while n and s portray the sample size and standard deviation by group. If adjusted and unadjusted effects were reported by the same study, the most adjusted outcome was used, more precisely, baseline adjusted marginal means were chosen over the unadjusted raw post-line means by group. The main meta-analysis was conducted as a meta-analysis of the above-described post-line mean differences between treatments and controls using a random effect model with inverse variance study weights computed as wi = 1/(si 2 + t 2), where si 2 was the variance estimate from the i-th study, and t 2 was the overall variance. The fix effect estimate was also reported as a secondary analysis.
Heterogeneity between studies was evaluated using the Cochrane Q test and the I 2 statistic. Sources of between-study heterogeneity (significant Cochrane Q test or I 2 > 50 %) were investigated by means of stratification and meta-regression considering potential confounders when a statistically significant random effect estimate was observed, and more than five estimates were included. Dichotomous levels were defined by medians of study duration, publication year, baseline Z-score, sample size by comparison group and baseline age. We also considered location (studies conducted in Africa v. studies conducted elsewhere) and studies having different types of animal-source food supplementation.
The comparison between studies was reported by means of the p-value for the Wald coefficient of the meta-regression. Residual heterogeneity was calculated as the difference of the between-study variance with and without the covariate(Reference Thompson and Higgins40). On the other hand, when relevant heterogeneity was found in meta-analyses based on less than five estimates stratification, study exclusion was conducted to identify it source. For the evaluation of heterogeneity by meta-regression and influence analyses, a study or a covariate were considered as relevantly associated with reduced heterogeneity if its contribution led to an I 2 below 50 %. Publication bias was assessed by visual inspection of the funnel plot and by Egger’s test(Reference Egger, Smith and Schneider41). Sensitivity analyses were conducted by means of influence analysis, excluding one study at a time and excluding outliers in the form of the higher and lower estimates included in that specific meta-analysis. All statistical evaluations were conducted using STATA vers. 12. The METAN, METANINF, METABIAS, METAFUNNEL and METAREG functions were used to perform random effect estimates, influence analyses, publication bias assessment, funnel plot and meta-regression, respectively. All statistical tests were two-tailed and type I error rate was set at 5 % (α = 0·05).
Results
Study selection
Our literature search identified 1188 records plus 6 additional records from screening the references of some relevant articles. After exclusion of duplicates, we obtained 1188 records as the 6 additional records identified were duplicates. Of these, 158 were excluded because they were either systematic reviews, protocols or letters; and an additional 1006 papers were excluded because they were not related to the topic of interest. After the paper selection phase, 24 papers were assessed for eligibility and their full texts were screened. Finally, after proofreading of the full text, 14 papers were included in the qualitative synthesis, 8 of which were also included in the meta-analysis on LAZ, WAZ and WLZ(Reference Krebs, Mazariegos and Chomba29,Reference Lannotti, Lutter and Stewart30,Reference Tang, Sheng and Krebs32–Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42–Reference Rosado, López and García44) . In addition, 5(Reference Krebs, Mazariegos and Chomba29,Reference Tang, Sheng and Krebs32,Reference Stewart, Caswell and Lannotti34,Reference Long, Murphy and Weiss43,Reference Tang, Hendricks and Krebs45) of the 14 papers were included in the meta-analysis on HCAZ and 2(Reference Lannotti, Lutter and Stewart30,Reference Rosado, López and García44) in the meta-analysis on BMIZ. The flow chart of paper selection is presented in Fig. 1.

Fig. 1. Flow chart of paper selection.
Study characteristics
The 14 studies that were included in the qualitative synthesis were published in the period 2000 to 2019 with the median publication year being 2015. Among the included studies, six where from Africa(Reference Omer, Mulualem and Classen33,Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42,Reference Long, Murphy and Weiss43,Reference Lin, Manary and Maleta46,Reference Konyole, Omollo and Kinyuru47) , four were from the American continent(Reference Lannotti, Lutter and Stewart30,Reference Tang and Krebs31,Reference Rosado, López and García44,Reference Tang, Hendricks and Krebs45) of which two were from the USA(Reference Tang and Krebs31,Reference Tang, Hendricks and Krebs45) , three were from Asia(Reference Tang, Sheng and Krebs32,Reference Skau, Touch and Chhoun48,Reference Beckett, Durnin and Aitchison49) and one study had a multicentre design being done in Zambia, Guatemala and Pakistan(Reference Krebs, Mazariegos and Chomba29). The age at baseline ranged between 5 and 24 months with a median of 6 months. Study duration ranged from 5 to 14 months with a median of 8 months. The total sample size by study ranged from 42(Reference Tang, Hendricks and Krebs45) to 1471(Reference Tang, Sheng and Krebs32), with a median of 250 children. A summary of the characteristics of the included papers is presented in Table 2. The setting for all the included papers in this meta-analysis were marginal rural communities(Reference Krebs, Mazariegos and Chomba29,Reference Lannotti, Lutter and Stewart30,Reference Tang, Sheng and Krebs32,Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42–Reference Rosado, López and García44,Reference Omer, Mulualem and Classen33) except data collected in Guatemala and Pakistan(Reference Krebs, Mazariegos and Chomba29) that were based in semirural and urban areas, respectively. Majority of the studies included in the meta-analysis did not report on the background diet of the participating children. The only three studies that gave some overview of the background diet of their participating children found little or no intake of animal-source foods(Reference Stewart, Caswell and Lannotti34,Reference Long, Murphy and Weiss43) and a high intake of sugary foods, drinks and soda(Reference Lannotti, Lutter and Stewart30), respectively, as presented in Supplementary Table 1.
Table 2. Qualitative synthesis, characteristics of included studies

DRC, Democratic Republic of Congo; M, male, F, female; NR, not reported.
* Control group.
† Comparison group.
‡ Added with germinated amaranth (71 %), maize (10.4 %), small fish (3 %) and edible termites (10 %).
§ Added with germinated amaranth (82.5 %), maize (10.2 %) and multi-micronutrient premix.
Attrition: percentage of lost to follow-up at the end of the study; groups considered for the meta-analyses.
Effect of animal-source supplementation and child growth based on measures of body size
Eight studies reported full data regarding the effect of animal-based food supplementation on LAZ and WAZ(Reference Krebs, Mazariegos and Chomba29,Reference Lannotti, Lutter and Stewart30,Reference Tang, Sheng and Krebs32–Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42–Reference Rosado, López and García44) . Five studies(Reference Tang, Hendricks and Krebs45–Reference Beckett, Durnin and Aitchison49) did not report age-specific Z-score of body size, one study reported LAZ and WAZ on a plot but numerical data were not available(Reference Tang and Krebs31). Fig. 2 depicts the effect sizes for the two outcome variables. Generally, studies showed a positive effect on children’s growth for animal-based food supplementation in comparison with the control, except for two studies for LAZ(Reference Krebs, Mazariegos and Chomba29,Reference Bauserman, Lokangaka and Gado42) and one for WAZ(Reference Krebs, Mazariegos and Chomba29). Heterogeneity between studies were observed to be 76·8 % (P Cochrane-Q < 0·001) and 89·5 % (P Cochrane-Q < 0·001) for LAZ and WAZ, respectively. We observed a homogeneous study contribution with random effect weights ranging from 6 to 19 % and 9 to 15 % for LAZ and WAZ, respectively. Based on this study’s statistical analysis, it was observed that animal-based food supplementation resulted in a higher LAZ and WAZ in comparison with the control group with random effect size estimates of 0·15 (95 % CI 0·02, 0·27) and 0·20 (95 % CI 0·03, 0·36), respectively (Fig. 2). These results are both confirmed by sensitivity analyses.

Fig. 2. Meta-analyses of length-for-age Z-score and weight-for-age Z-score comparing animal-source food supplementation v. control.
Sensitivity analyses
The random effect size estimate for LAZ conducted by excluding one study at a time ranged between 0·08 (95 % CI ( −0·01, 0·17); I 2 = 53·2 %; P Cochrane-Q = 0·046) and 0·19 (95 % CI (0·07, 0·32); I 2 = 71·2 %; P Cochrane-Q = 0·002), and when excluding the two most extreme results reported by Lannotti et al.(Reference Lannotti, Lutter and Stewart30) and by Krebs et al.(Reference Krebs, Mazariegos and Chomba29), respectively. Notably, those studies had also high risk of bias (online Supplementary Fig. S2). Furthermore, when both extreme estimates were excluded, the random effect size estimate was 0·10 (95 % CI 0·05, 0·14), with a null residual heterogeneity (I 2 = 0 %; P Cochrane-Q = 0·447). When looking at sensitivity analyses conducted on WAZ, it was observed that the exclusion of one study at a time resulted in effect size estimates ranging from 0·11 (95 % CI (−0·01, 0·23); I 2 = 74·5 %; P Cochrane-Q < 0·001) to 0·25 (95 % CI (0·08, 0·43); I 2 = 87·5 %; P Cochrane-Q = 0·001), and when excluding the studies by Lannotti et al.(Reference Lannotti, Lutter and Stewart30) and by Krebs et al.(Reference Krebs, Mazariegos and Chomba29), respectively. When both extreme observations were excluded, the random effect size estimate was 0·15 (95 % CI 0·04, 0·26) with a borderline relevant heterogeneity (I 2 = 55·7 %, P Cochrane-Q = 0·046).
Effect size estimates for animal-source food consumption on measures of body size
Among the different factors investigated in this meta-analysis, it was observed that only sample size was related to a reduction of heterogeneity. However, we observed a relevant increased effect on LAZ and WAZ when the food supplementation was based on egg. Notably, when considering studies having egg as a complementary food(Reference Lannotti, Lutter and Stewart30,Reference Omer, Mulualem and Classen33,Reference Stewart, Caswell and Lannotti34) , we reported a border-line non-statistically significant, but clinically relevant high effect size of 0·31 (95 % CI −0·03, 0·64) and 0·36 (95 % CI −0·03, 0·75) for LAZ and WAZ, respectively (Table 3).
Table 3. Stratification and meta-regression analyses
(Mean values and 95 % confidence intervals)

LAZ, length-for-age Z-score; WAZ, weight-for-age Z-score.
When looking at meta-analyses stratified by considering studies in which participants were breastfed(Reference Krebs, Mazariegos and Chomba29,Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42,Reference Long, Murphy and Weiss43) , we observed a borderline non-statistically significant larger effect size on LAZ and WAZ for studies in which children were not breastfed. Specifically, when considering LAZ, we observed an effect size of 0·31 (95 % CI (0·07, 0·56); I 2 = 81·2 %; P Cochrane-Q = 0·001) and an effect size of 0·0 (95 % CI (−0·14, 0·14); I 2 = 54·6 %; P Cochrane-Q = 0·085) for children that were not breastfed and those who were breastfed, respectively. A similar result was observed for WAZ (effect size = 0·37, 95 % CI (0·05, 0·69); I 2 = 93·0 %; P Cochrane-Q < 0·001 and effect size = 0·01, 95 % CI (−0·13, 0·14); I 2 = 59·4 %; P Cochrane-Q = 0·061, for children that were not breastfed and those who were breastfed, respectively). Finally, when considering data reported by the eight studies(Reference Krebs, Mazariegos and Chomba29,Reference Lannotti, Lutter and Stewart30,Reference Tang, Sheng and Krebs32–Reference Stewart, Caswell and Lannotti34,Reference Bauserman, Lokangaka and Gado42–Reference Rosado, López and García44) , we observed an effect size of 0·05; 95 % CI (−0·02, 0·12); I 2 = 38·7 %; P Cochrane-Q = 0·121 for WLZ (online Supplementary Fig. S1). We also observed an effect on HCAZ, based on data from five studies(Reference Krebs, Mazariegos and Chomba29,Reference Tang, Sheng and Krebs32,Reference Stewart, Caswell and Lannotti34,Reference Long, Murphy and Weiss43,Reference Tang, Hendricks and Krebs45) (effect size = −0·02; 95 % CI (0·13, 0·10); I 2 = 70·9 %; P Cochrane-Q = 0·008) and BMIZ based on data from two studies(Reference Lannotti, Lutter and Stewart30,Reference Rosado, López and García44) , (effect size = 0·13; 95 % CI ( −0·05, 0·31); I 2 = 0 %; P Cochrane-Q = 0·39).
Bias assessment
Moderate to high risk of bias was observed for most of the included studies (online Supplementary Fig. S2). Few studies gave a clear description of the randomisation technique and allocation concealment. However, all studies were randomised so that at least random allocation should not be a major source of bias. Blinding of participants was not possible for the included studies after enrolment as the intervention was based on food supplementation. However, group assignment was masked for the investigators and during statistical analysis. Also, the use of objectively assessed outcomes and the young age of the participants should have completely avoided a possible performance bias or a placebo effect. The studies that were included had low attrition rates, with similar attrition rates for the treatment and the control groups (Table 2); thus, attrition rate could not have influenced the results. Additionally, almost all studies reported full results for all considered outcomes and so we assume that selective reporting may have not affected our results because incomplete data were negligible. Finally, no indication for publication bias effect emerged in the current meta-analysis according to the reporting of a non-significant Egger test (P Egger = 0·460 and P Egger = 0·298, for LAZ and WAZ, respectively) and symmetric funnel plots for all the outcomes under analysis (online Supplementary Fig. S3).
Discussion
In this meta-analysis, it was observed that animal-source foods may be a suitable complementary food to help improve growth in children between the ages of 6 and 24 months in LMICs, communities, populations and low-income households. First and foremost, it was observed that providing animal-source foods as part of the complementary diet resulted in an increase in LAZ and WAZ values, compared with the comparison groups. The estimated effect size of 0·15 and 0·20 units for LAZ and WAZ, respectively, will correspond to a biologically relevant effect size, considering that we observed standard deviation ranging from 0·5 to 1·4 and 0·6 to 1·4 for LAZ and WAZ, respectively(Reference Tang, Sheng and Krebs32,Reference Bauserman, Lokangaka and Gado42) .
Furthermore, it was observed in this meta-analysis that children who are not breastfed might benefit from the intake of animal-source foods, compared with those that are breastfed. It is well acknowledged that the complementary feeding should be started immediately after the recommended 6 months of exclusive breast-feeding to alleviate growth faltering. Thus, children who did not benefit from the recommended 6-month period of breast-feeding may benefit from animal-source foods such as meat, eggs and milk when added to their usual diets to meet their needs for nutrients such as protein, Zn and Fe(50). It is true that there are concerns about some potential negative health consequences such as obesity, excessive intake of saturated fats, heart diseases, high blood pressure, type 2 diabetes, poor kidney function and prostate when people including children, particularly those from resource-rich environments, populations and wealthier households overindulge animal-source foods(Reference MacDonald, Brevard and Lee51–55). One cannot however disregard the potential benefits of the consumption of the same animal-source foods among children from LMICs, communities, populations and poor households who are susceptible to undernutrition during complementary feeding(Reference Grace, Dominguez-Salas and Alonso15,Reference Fewtrell, Bronsky and Campoy56,57) . The excessive intake of animal-source foods such as meat, eggs and milk by children from high-income countries, communities, populations and wealthier households should not be the basis for policymakers to put limitations on its consumption among children from LMICs, communities, populations and poorer households who could benefit nutritionally from its consumption during complementary feeding to improve their nutrition and health status(Reference Allen58–Reference Wu63).
The strength of our results was also limited by quite a substantial heterogeneity between studies. Notably, between-study heterogeneity was observed due to the study by Krebs et al.(Reference Krebs, Mazariegos and Chomba29) and Lannotti et al.(Reference Lannotti, Lutter and Stewart30). Krebs et al.(Reference Krebs, Mazariegos and Chomba29) conducted a multicentre study in 1062 children in Congo, Zambia, Guatemala and Pakistan; comparing the effect of meat v. cereal fortified with multiple micronutrients. Not only did their study obtain the lowest effect size compared with the other studies included in this meta-analysis, but they also reported a negative effect size for both LAZ and WAZ. A plausible explanation for this observed outcome might be due to the influence of environmental-related factors. Importantly, children living in settings with poor sanitation and hygiene conditions may ingest faecal bacterial through contaminated foods, drinking water and through the surrounding, and this may cause environmental enteric dysfunction. Environmental enteric dysfunction increases intestinal inflammation leading to reduces intestinal absorption of nutrients and this may cause growth faltering during nutritional interventions in children(Reference Budge, Parker and Hutchings64,Reference Syed, Ali and Duggan65) . Also, Krebs et al.(Reference Krebs, Mazariegos and Chomba29) did not report an improved growth in children, irrespective of the treatment, with the end line mean Z-score being lower than the baseline mean Z-score. A plausible explanation for this finding is the poor growth status at baseline (mean Z-score of −1·38 (sd 1·36) and −0·96 (sd 1·31) for LAZ and WAZ, respectively), for which animal-source foods alone was not sufficient to achieve a better growth outcome compared with the fortified cereal. It is also reasonable to assume that the finding of Krebs et al.(Reference Krebs, Mazariegos and Chomba29) could be ascribed, at least partly, to the high micronutrient content of the fortified cereal, as nutrients needed for growth, such as Fe, Cu, Se, Mg, niacin, biotin and folate were more concentrated in the fortified cereal compared with the meat(Reference Krebs, Hambidge and Mazariegos66), or a possible reverse causation due to the high undernutrition prevalence of the participants. The study of Lannotti et al.(Reference Lannotti, Lutter and Stewart30), on the other hand, compared egg supplementation to no-intervention in 160 children in Ecuador. They reported a larger effect on growth in children receiving egg compared with those not receiving any food supplementation. In their study, a high mean Z-score of undernutrition was also observed at baseline for LAZ (−1·9 (sd 1·0) and WAZ (−0·65 (sd 1·1)). We therefore assume that the heterogeneity observed in this meta-analysis was due to the type of supplementation for the comparison group.
It was further observed in this meta-analysis that giving egg to the treatment group could result in a higher LAZ and WAZ increase compared with the control. Most importantly, the three studies based on egg supplementation(Reference Lannotti, Lutter and Stewart30,Reference Omer, Mulualem and Classen33,Reference Stewart, Caswell and Lannotti34) had a pooled effect size of 0·31 and 0·36 for LAZ and WAZ, respectively, over the 6-month intervention period. These three studies however had no intervention as control, which could have affected the magnitude of the effect size observed. The motivation for looking specifically at the effect of providing egg on child growth was that eggs were previously not considered an acceptable food for infants aged 6 months because of possible allergy, but this view has changed, and egg is now included in the guidelines for infants and young child feeding(5,50) . Additionally, the American dietary guidelines advisory group recently recommended eggs as a first complementary food for infants and very young children(Reference Rubin67). Eggs are also indicated as complementary food from 6 months in many LMICs’ dietary guidelines for children including the South African dietary guidelines for mothers(68).
A possible explanation to why eggs might have impacted on the growth of children is that egg represents a balanced food of higher biological value compared with any other animal-based food. Egg is one of the most valuable components of the human diet(Reference Fevold69,Reference Réhault-Godbert, Guyot and Nys70) . For instance, the amino acids leucine and glutamine found in egg appears to play a role in the regulation of the mTORC1 activation pathway for muscle cell growth, by regulating skeletal muscle protein synthesis(Reference Jewell, Chul and Russell71). Leucine is an essential amino acid that can only be obtained from the diet, and it is especially very high in foods of animal origin such as the egg(Reference Réhault-Godbert, Guyot and Nys70). In comparison with other animal-source foods, egg has a high leucine content per calorie. It is also nutritionally dense in proteins and other essential micronutrients such as choline(72). Choline is needed in the body for cellular maintenance and growth throughout the life cycle. Although choline can be synthesised endogenously by the body, it is not enough to meet the human body’s requirement, and thus must be obtained from food sources(Reference Wiedeman, Barr and Green73). One large egg contains approximately 150 mg of choline v. the daily requirement for infants of 125 mg at the age of 6 months, and 150 mg at the age of 7 to 12 months(Reference Hayes74). Eggs also contain healthy fats such as phospholipids and PUFA needed for growth of infants and young children(Reference Michaelsen, Dewey and Perez-Exposito16). It has thus been argued that due to its high leucine, choline and protein content, egg can be used as an early food source to help overcome the nutritional deficiencies in the usual complementary diets and ultimately alleviate growth faltering(72,Reference Lannotti, Lutter and Bunn35) .
The current study has numerous strong points. First, we conducted a rigorous meta-analysis of randomised control trials, which actually represents the stronger form of scientific evidence(Reference West, King and Lohr75). Moreover, we adopted a commonly accepted approach to scientific evidence synthesis following the most updated evidence accumulated so far. We conducted numerous stratifications and sensitivity analyses showing the robustness of the current results. Finally, we focused on commonly accepted standardised measures of growth considering age- and sex-standardised Z-score calculated according to the WHO Child Growth Standards; therefore, biases due to children’s age, sex or ethnicity can be considered as negligible, making our results generalisable.
Our work has also certain limitations. Firstly, our research was limited because of the low number of studies reporting outcomes on physical growth, such as HCAZ and BMIZ. There were also limited studies reporting on egg as the treatment group. Thus, a low number of studies could have resulted in several false-negative results. Secondly, we may also consider the great variability of the study characteristics as a possible limitation. For example, baseline nutritional status varied between samples with high prevalence of undernutrition to samples with low prevalence of undernutrition. On the other hand, according to the results of this study, we may assume that an improved intake of animal protein would result in a further overall growth enhancement of children where undernutrition prevalence is higher. Also, due to the limited number of available randomised controlled studies, we had to include studies with a certain age variability, while focusing on a more limited age range between 6 and 12 months would have been preferable. Furthermore, although we only considered the effect of animal-source foods on children’s growth in this meta-analysis, it is possible that the growth of the children may have been influenced by other environmental and social factors such as maternal depression and poor sanitation and hygiene. We acknowledge that plant-based foods may represent an appropriate alternative to animal-based food. Specifically, we are aware of the health-related risks of the excessive intake of animal-source foods and in particularly, the long-term risks of creating taste preferences high in saturated fat and high cholesterol foods that could results in CVD such as heart attacks and stroke during adulthood(Reference Melina, Craig and Levin76,Reference Tonstad, Butler and Yan77) . Nevertheless, it is well documented that there are still some children who are susceptible to growth faltering and poor health if their usual diet does not include foods from animal origin. Also, the high protein content of animal-source foods is very important for growing children aged 6 to 24 months which is the first 1, 000 d of life where children especially those from disadvantage settings, communities and poor households are exposed to suboptimal growth due to the lack of intake of foods from animal origin in their usual diets(Reference Eaton, Rothpletz‐Puglia and Dreker14,Reference Alonso, Dominguez-Salas and Grace23) .
Finally, we cannot exclude that the limited number of available randomised controlled studies may have resulted in several false-negative results.
Conclusions
In conclusion, animal-source foods may be a suitable complementary food to help improve growth in 6 to 24 months children from LMIC, communities, populations and poor households, especially if based on eggs. Furthermore, we can speculate that the important role of micronutrients to enhance and support appropriate child growth was reinforced by our research. Our results agree with a growing body of evidence showing that livestock ownership may be related to children’s growth, a factor that should be further investigated by dedicated randomised controlled trial and implementation studies(Reference Dumas, Kassa and Young78,Reference Mosites, Rabinowitz and Thumbi79) .
There is a paucity of randomised controlled studies aimed at evaluating the effectiveness of the provision of animal-source foods as a complementary diet to support optimal growth in 6 to 24 months children. Therefore, it is important that in future studies, the battery of outcomes measures would be extended to other biometric outcomes of great interest, such as HCAZ and BMIZ. Additionally, it would be very beneficial if more high-quality randomised controlled studies would be conducted on specific target communities and populations, such as those with high undernutrition prevalence and maybe not high-income countries, communities and populations with no food scarcity and full access to fortified baby foods and supplements.
Acknowledgements
A sincere thank you to all the authors for making this work possible.
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
H. A. and C. R. were involved in the conptualization, data curation and writing the original draft of the manuscript. H. A. performed the qualitative synthesis. C. R. performed the formal statistical analyses. A. R. defined the literature search strategy and performed the search strings. A. R., M. F. and C. M. S. review and edited the first version of the manuscript. M. F., C. M. S. and C. R. equally contributed in supervising the esearch team. All the authors actively contributed to the writing, reviewing and editing of the manuscript.
None of the authors has any conflict of interest to declare.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114522000290










 Open access
Open access