



Over recent years, a number of campaigns have been developed in the UK aimed at improving the national diet by encouraging behavioural changes in society( Reference Caraher, Crawley and Lloyd 1 ). Among these strategies are the ‘Choosing a Better Diet’ framework( 2 ), the ‘Food Matters’ policy( 3 ) and the ‘Public Health Responsibility Deal’( 4 ). Despite these campaigns, average fruit and vegetable (F&V) intake, a marker of a healthy diet, remains below recommended levels( Reference Bates and Lennox 5 ), with only 26 % of adults report eating five or more portions per day in 2013 compared with 28 % in 2005( 6 ). Moreover, the percentage of overweight and obese adults remains high and has increased between 2005 and 2013 from 60·5 to 62·1 %( 6 ).
In the UK there has been a decline in cooking culture since the 1950s: home-made meals have been replaced with ready meals and convenience foods resulting in a decrease in cooking skills( Reference Caraher, Dixon and Lang 7 – Reference Caraher and Lang 9 ). Lack of cooking skills has been associated with poor diet and increased consumption of highly processed and energy-dense convenience foods of reduced nutritional quality( Reference van der Horst, Brunner and Siegrist 10 – Reference Hartmann, Dohle and Siegrist 12 ). Furthermore, high consumption of ready meals is associated with being overweight( Reference van der Horst, Brunner and Siegrist 10 ). Cooking skills are considered to be a major predictor of healthier food choices and the ability to cook in the home( Reference Caraher, Dixon and Lang 7 , Reference Hartmann, Dohle and Siegrist 12 ).
Previous UK government policy has focused primarily on increasing consumer knowledge about healthy eating; however, individuals are likely to require practical skills to utilise this knowledge. Within public health nutrition, ‘culinary nutrition’ is a newly established approach which combines aspects of nutritional principles with cooking and culinary knowledge in the form of cooking interventions( Reference Condrasky and Hegler 13 ). These programmes typically involve small groups of participants attending weekly practical sessions over a period of 4–10 weeks with main objectives to increase awareness of healthy nutrition and to increase cooking skills and confidence levels. These practical interventions provide ‘hands-on’ experience that can lead to improved dietary intake and increased food literacy( Reference Reicks, Trofholz and Stang 14 ).
Sociodemographic status and household income can influence food purchasing decisions and dietary intake; households of lower income often have poor diets and are at greater risk of diet-related disease( Reference James, Nelson and Ralph 15 , Reference Darmon and Drewnowski 16 ). In the UK, low-income populations consume diets lower in F&V, oily fish and micronutrients such as vitamin C, folate, Fe and Ca than those in the highest income quintile( Reference Bates and Lennox 5 ). Those from the lowest socio-economic levels are least likely to be confident with cooking( Reference Adams, Goffe and Adamson 17 ). By increasing food literacy, teaching better budgeting techniques and efficient food shopping strategies, and providing accessible information and skills to prepare healthy meals at a low cost, cooking interventions may help overcome economic barriers that presently prevent healthy eating( Reference Cullerton, Vidgen and Gallegos 18 – Reference Garcia, Vargas and Lam 20 ).
In 2008, Jamie Oliver, a celebrity chef, introduced a network of local food centres in the UK providing 8- to 10-week cooking courses aimed to educate individuals from lower socio-economic groups on cooking skills while incorporating simple nutritional messages. Named ‘Jamie’s Ministry of Food’, the campaign aims to eliminate common misconceptions and economic barriers, where the classes teach individuals how to prepare quick, healthy and low-cost home-cooked family meals, using fresh ingredients. The main objective of the present study was to evaluate the impact of the Jamie Oliver Ministry of Food cooking course among individuals who attended the Leeds Kirkgate Market centre from 2010 to 2014, in relation to changes in F&V and snacks consumed and confidence in cooking.
Methods
Ministry of Food cooking course
In 2010 a Ministry of Food (MoF) centre was established in Leeds, UK. The MoF centre is a fully fitted domestic kitchen fitted within a stall in Leeds Kirkgate Market. The food centre offers cooking courses which are open to all, but have the aim of teaching those with no or limited cooking skills how to prepare tasty, healthy meals on a budget. Service users attend the centre once per week over 8 weeks for 90 min per session, to learn a range of cooking skills and a variety of recipes which will teach them progressive cooking skills that they can then use to cook a range of meals for themselves and their families. Participants pay between £4·50 and £7·50 per session, based on their individual circumstances. The reduced rate applies to participants who are students or on means-tested benefits. Each cooking session promotes a key healthy eating message to educate service users on a wide range of healthy eating messages from understanding food labels to reducing salt, fat and sugar. Specific attention is given within the course to highlight the importance of the ‘Eatwell plate’ (now replaced by the ‘Eatwell Guide’), developed by the Department of Health, stressing the importance of staple food items and portion control to achieve dietary balance. The course includes the relevance of government dietary guidelines and differences in dietary requirements within different age groups of the public and vulnerable populations. The basis of the MoF was developed around outcomes from several nutritional studies including the Healthy Weight, Healthy Lives consumer insight report( 21 ).
Study participants
The MoF cooking course was advertised in a number of ways to attract participants: directly in Leeds Kirkgate Market; on Jamie Oliver’s website; by Zest Health for Life publicity; within third-sector organisations; through media coverage; and also via information leaflets distributed by Leeds City Council. The MoF received a substantial number of referrals from other organisations including support organisations for those with financial and social deprivation, weight-management problems, addictions, physical impairment, learning difficulties and mental health problems. From July 2010 to March 2014, 1210 adults over 16 years old enrolled in the MoF cooking intervention and were asked to self-complete quantitative questionnaires. These participants were also asked to complete questionnaires directly after the 8-week course and then 6 months after the course. Individuals who gave consent to be contacted up to 1 year after the course to participate in experience-focused interviews were later contacted by telephone for interview.
Design
In the current study the impact of the MoF courses, run from 2010 to 2014, on short- and long-term dietary behaviour was investigated using a pre-test/post-test design. Due to the absence of a control group, the effectiveness of the MoF cooking intervention was measured using mixed methods including both quantitative and qualitative evaluations. The evaluations were based on self-reported data.
Quantitative evaluation
The effectiveness of the MoF course was evaluated by assessing the change in self-reported number of portions of F&V consumed per day (0, 1, 2, 3, 4, 5, 6 and 7+); the change in the self-reported number of snacks consumed per day (0 to 7+); and the change in participants’ self-reported confidence in cooking a healthy meal (0 to 5; 0 being ‘not confident at all’ and 5 being ‘very confident’). This was determined by comparing responses to the self-completed questionnaires before the course with those immediately after the course and also with responses 6 months after the course. The questionnaires included examples for a portion of F&V (‘Example one handful=one portion’) and for snacks (‘Examples include: cake, biscuits, crisps, etc.’).
As part of the MoF evaluation all participants were asked to complete a general background questionnaire, issued before the beginning of the course. This included self-reported postal code (used to measure deprivation), age group, ethnicity, gender, and whether the participant considered he/she has a limiting disability, a long-term illness or a condition that limits; categorised by Learning Disabilities, Physical Impairment and Mental Health Problems.
Qualitative evaluation
A structured interview consisting of ten questions (see online supplementary material) was prepared based on specific aims of the MoF and a discussion with a health improvement specialist working within public health. Establishing contact with the participant was tried three times on three different non-consecutive days to maximise response. Each telephone interview was initiated with a brief introduction by the interviewer (J.W.) and an explanation of the purpose and procedure of the telephone call. Each telephone interview lasted for 15 to 30 min and included questions about cooking skills learned; healthy eating knowledge learned; if members felt they had improved portion control; confidence in cooking; whether they enjoyed working as a group and meeting new people; changes in eating habits since the course; and what members thought was best about this course and what could be improved. Open-ended questions were asked and responses were recorded in order to obtain details of the participant’s experiences at the MoF.
Statistical analysis
Quantitative analysis
All questionnaire data were analysed using the statistical software package Stata version 13. Student’s paired t tests were used to determine whether there were statistically significant changes between before and immediately after the MoF course (and also between before and 6 months after the course for those who completed this follow-up questionnaire) in the mean number of self-reported portions of F&V consumed per day, the mean number of self-reported snacks consumed per day and the mean change in participants’ self-reported cooking confidence levels. In the analyses the ‘7+’ responses were counted as ‘7’; this avoided exaggerated responses becoming outliers. Only 1–3 % of participants reported they ate seven or more portions of fruit and vegetables daily and only 1 % of participants ate seven or more snacks daily. A significance level of less than 0·05 was taken to represent statistical significance for all analyses.
For MoF participants who completed the questionnaires at all three data collection time points, multivariate regression analyses were undertaken to determine whether changes in self-reported F&V intake, snack intake and cooking confidence scores between before and 6 months after the course were independently associated with the sociodemographic factors. All five sociodemographic variables were included in the multivariate regression for each outcome, meaning results were adjusted for all variables. These were age group (16–19, 20–64, 65+ years), ethnicity (White, Black, Asian, mixed race, other), gender, presence of a disability (no difficulties, learning disabilities, mental health problems, physical impairment, multiple disabilities, other disabilities) and deprivation (deprived Leeds residents, non-deprived Leeds residents, living outside Leeds or had non-mappable postcodes (note: 7 % of participants had non-mappable postcodes for the purpose of classifying deprivation; about half appeared to be Leeds postal districts). Individuals were categorised as deprived if they lived at postcodes in Leeds that were classified in the top tenth of deprivation in England using the Index of Multiple Deprivation (2015). All small areas in England (of about 1000–3000 people) are mapped to postcodes which can be ranked according to their Index of Multiple Deprivation score, a relative level of overall deprivation based on deprivation scores for income, employment, health, education, crime, access to services and living environment.
Qualitative analysis
Demographic information, including disability, gender, age and ethnicity, were obtained within each individual interview to provide a background for the interviews. The answers to each question of the interview were recorded and manually typed as the interviews occurred, in order to document and analyse exact individual responses. The data were analysed in a deductive fashion using constant comparative narrative analysis, previously adopted by Symon and Wrieden( Reference Symon and Wrieden 22 ).
Data from transcripts were reviewed alongside demographic information and re-occurring themes among participants were identified. This method was then used to establish a coding framework for each individual question (see online supplementary material for questions and framework used). Specific steps of qualitative data analysis included: (i) a review of interview data and arrangement of the data into different categories, incorporating demographic background information; (ii) the classification of clear emerging common trends using quotations to support general findings; and (iii) the comparison of data and themes among different demographic groups.
Qualitative data analysis and management were carried out using Microsoft® Excel and Word; dedicated qualitative analysis software was not used in the current study.
Results
Quantitative analyses
Of 1210 who attended the MoF course between 2010 and 2014, 795 individuals completed both the baseline questionnaire and the questionnaire issued immediately after the course (a response rate of 66 %). Of these participants, 85 % were white, 57 % were female, 24 % came from a deprived area in Leeds (which were in the top 10 % deprived areas in England, i.e. 2·4 times more deprived individuals than the national average were recruited on to the course), 81 % were aged 20–64 years, 9 % were over 65 years and 9 % were under 20 years, 63 % of participants did not report a disability, 7 % had multiple disabilities, 15 % had learning difficulties, 8 % had mental health problems and 5 % had physical disabilities only (Table 1).
Table 1 Characteristics of those taking part in the Ministry of Food course, Leeds, UK, 2010–2014
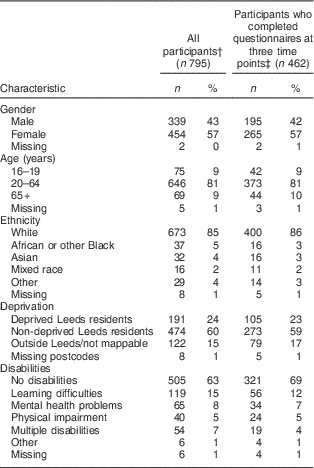
† Completed questionnaire before and immediately after the course.
‡ Completed questionnaires before, immediately after and 6 months after the course.
Of the total participants, 462 completed the 6-month follow up questionnaire (a follow-up response rate of 58 %). As observed in Table 1, their characteristics were similar to those of the full set of participants, except that there was a greater proportion who reported no disabilities (69 %).
The results of the t tests in Table 2 show there were significant increases in daily F&V consumption and cooking confidence levels and a significant decrease in the frequency of snacks consumed (P<0·001) between before the course and immediately after the course. Larger increase for these outcomes occurred from before the course to 6 months after the course for the subset who completed the follow-on questionnaires, and these results were all statistically significant (P<0·001). The increase in self-reported daily intake of F&V portions doubled from 0·7 (95 % CI 0·6, 0·8) immediately after the course to 1·5 (95 % CI 1·3, 1·6) six months after the course. Similarly, the decrease in self-reported daily intake of snacks doubled from −0·4 (95 % CI −0·2, −0·5) immediately after the course to −0·9 (95 % CI −0·8, −1·0) at 6-month follow-up. A large increase was observed in participant’s cooking confidence levels (a self-reported score between 0 and 5, 5 being very confident); this increased immediately after the course by 1·4, (95 % CI 1·3, 1·6) and the total increase after 6 months was a little higher at 1·7 (95 % CI 1·6, 1·9). The differences between immediately after the course and 6 months later were all statistically significant (P<0·001).
Table 2 Mean self-reported food intakes and cooking confidence scores, and changes in these between before, immediately afterwards and 6 months after the Ministry of Food (MoF) course, Leeds, UK, 2010–2014

F&V, fruit and vegetables.
***P<0·001.
† Where portions of F&V and number of snacks consumed were ‘7+’, these were counted as ‘7’ in the analyses.
‡ Participants were asked to score their confidence in cooking between 0 and 5.
§ For all 795 MoF participants who completed the course and the questionnaires before and immediately after the course.
|| For 462 MoF participants who completed questionnaires at three time points.
The multivariate regression analyses in Table 3 show changes between before the start to 6 months after the course by sociodemographic factors. As observed, there were no associations between changes in any of the three nutrition outcomes and deprivation or ethnicity. There were also no associations between change in self-reported snack intake and any sociodemographic variables. The increase in self-reported F&V intake was associated with age and disability: younger adults had a significantly smaller increase than the age group 20–64 years (−0·60 (95 % CI −1·00, −0·10) portions/d, P=0·02) and those with physical impairments had a smaller change than those with no disabilities (−0·69 (95 % CI −1·32, −0·07) portions/d, P=0·03). Males reported a greater increase in cooking confidence scores at 6 months after the course than females (0·29 (95 % CI 0·04, 0·55) increase, P=0·03) and those aged 16–19 years or 65 years and above had smaller increases than 20–64-year-olds (−0·57 (95 % CI −1·02, −0·13), P=0·01 and −0·46 (95 % CI −0·89, −0·04), P=0·03, respectively). Compared with participants with no disabilities, those with learning disabilities reported significantly smaller increases in cooking confidence scores 6 months after the course (−0·62 (95 % CI −1·02, −0·22), P=0·002).
Table 3 Multivariate regression showing changes in self-reported food intakes and cooking confidence scores between the start and 6 months after the Ministry of Food course, by sociodemographic factors, Leeds, UK, 2010–2014 (n 462)
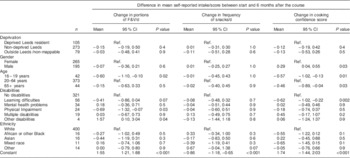
F&V, fruit and vegetables; Ref., reference category.
Only includes participants who completed questionnaires at three time points.
Qualitative analyses
Forty individuals were successfully contacted and completed the telephone interview. The characteristics of this group were different from those participating in the quantitative research: 73 % (n 29) were white, 63 % (n 25) were female, 75 % (n 30) were under 60 years of age, 53 % (n 21) came from a deprived area in Leeds and 68 % (n 27) did not report a disability.
Acquisition of cooking skills
Results across the range of participants showed that they finished the MoF programme with various cooking and preparation skills, including skills using knives, preparing vegetables, seasoning food and aspects within food hygiene:
‘It’s taught us both how to improve the quality of food using seasoning.’
‘I can now make simple meals with less ingredients and know how to stop cross contamination.’
The most valuable aspect of the course for participants from deprived areas of Leeds appeared to be learning new recipes and ways to cook from scratch (i.e. from basic ingredients).
Increased nutrition knowledge
A large proportion of participants claimed to have improved knowledge on healthy eating, being more aware of F&V nutritional value and the health consequences of saturated fat. Most participants from deprived areas in Leeds learned healthier ways to cook including using less oil and fat, with just under half of individuals gaining knowledge about the value of fresh ingredients. Those from non-deprived areas tended to learn more about nutritional value of healthy food and substitutions for unhealthy foods such as sauces. Discovering healthy alternatives for high-fat foods also appeared to be particularly present among those aged over 65 years. Within the fifteen males interviewed, most claimed to gain nutritional knowledge, learn the value of healthy food, healthier ways to cook and how to read labelling of food unhealthy ingredients:
‘They teach you how to check food labelling and how to avoid excess salt and fat.’
‘More awareness of nutritional value and I learned more about the 5-a-day campaign.’
‘I add very little fat and oil now, whereas previously I thought fat made food delicious.’
Interviews also revealed many participants made several changes within eating and cooking habits. For example, all but one participant living in deprived areas of Leeds claimed to have made changes, with most changes being eating more healthily, cooking from scratch and using less fat and oil. Within non-deprived areas 25 % claimed to have not changed eating and cooking habits, due to factors such as age, experience and already eating healthily prior to the course. Among all participants, only one male participant reported maintaining the same eating habits, with the remaining participants claiming to eat and cook more healthily. A specific finding was that attending the MoF demonstrations appeared to reduce the self-reported intake of frozen, processed and takeaway foods high in fat:
‘Yes definitely, we don’t eat ready meals anymore and myself and my dad don’t get takeaways now, we made our own pizzas because they showed us how.’
Within portion control participant feedback was varied. Among those over 65 years old, the majority of participants claimed the MoF course helped portion control, including learning how to cook batch portions, reduce wastage and how to correctly portion macronutrient groups. It was also suggested that portion knowledge helped older individuals cope with changes in household numbers, for instance when children grow up and leave home:
‘Yeah portion control definitely. I’ve got three children but they’ve all left home, so now I know how to cook for myself and not to make too much, which is helping with my weight.’
‘Yeah I learned what should be on your plate, so I learned how much should be carbohydrate, protein and fat, and the right plate size.’
Additionally, the cooking course appeared to help parents distinguish between portion sizes within the family, for example the difference and correct portion sizes for children and adults. Many participants who attended the course mentioned the ‘Eatwell plate’; however, portion control was not found to be improved for everyone with some individuals claiming to still ‘struggle’ with portion size.
There was also an increase in awareness of shopping costs, budgeting and a greater awareness of healthy food access within Leeds market. Many participants claimed to visit the market more, having an increased awareness of the healthy food available to them:
‘Yes I do because they gave us a tour and told us about a fish stall, so I now get my fish there and organic eggs, vegetables and fresh spices.’
Confidence and social aspects
The majority of the interviewees claimed to have improved confidence in cooking, with just 15 % stating no improvements due to being confident previously. In particular, through an increase in confidence, some members attending the MoF were found to cope better with illness and disability, for example:
‘Yes, it really did because that was one of the big things I couldn’t cope with before. Because I’m disabled, preparing food was something I’ve always struggled with and never really done before. So starting off on the cooker at the hob was really useful and means I’m more confident at home.’
In addition to confidence, most individuals declared other social benefits; for example, participants suffering from disabilities and living in deprivation saw a clear decrease in social isolation:
‘Yes before the Ministry of Food I wouldn’t really start conversations with people because I’m really shy. But by going there I learnt how to speak for myself and now I socialise more.’ (Male aged 20–64 years, deprived Leeds area, learning difficulties and mental health problems)
‘It got me out of the flat. I’m disabled so that was always a fear and I’d just stay in before.’ (Female aged 20–64 years, deprived Leeds area, physical impairment and mental health problems).
Within the MoF structure all but four participants claimed to enjoy working as a group and meeting new people:
‘Of course one of the participants hardly spoke to anyone, but after a few lessons he started talking and chatting so it has a social value to break an isolation barrier, talking about cooking and enhancing social aspects and the teachers were so energetic and social, they presented a feeling of relaxation and they made you want to talk.’ (African male, aged 20–64 years, deprived Leeds area)
‘Yes I do because I had only recently moved to Leeds and I got the email from the MoF, and it was really beneficial because it got me out and about and meant I met loads of new people.’ (White female, aged over 65 years, non-deprived Leeds area)
Suggested course improvements
All forty interviewees spoke positively about their MoF experience. Suggestions to improve the course were clustered mainly within wanting more recipes, advanced sessions, longer and flexible timings. Of participants from deprived areas of Leeds, 50 % stated no improvements were needed and others suggested more recipes, dessert options and longer sessions. Among those from non-deprived areas, many people would have liked a more advanced class and found the course ‘too basic’; however, 25 % of those from non-deprived Leeds suggested no changes.
Discussion
Despite the focus on recruiting deprived groups for the intervention, the baseline response to the questionnaire was 66 %. This is a good response for such a relatively hard-to-reach group( Reference Pearson, Russell and Campbell 23 ).
Dietary changes, nutrition knowledge and cooking skills
Results from the current study present the effectiveness of the MoF community-based cooking programme for facilitating medium-term changes in dietary behaviour. Quantitative analysis revealed that after the MoF course there was a significant increase in self-reported portions of 5-a-day F&V consumed and a decrease in snacks consumed. These positive changes emerged immediately following the course and had increased further by 6 months after the course. This suggests that the MoF programme may encourage short-term changes in dietary behaviour which can be maintained and improve over longer periods of time. The course did not produce inequalities in dietary changes by deprivation; however, participants under 20 years of age showed smaller increases in self-reported F&V intake. Many interviewed in the current study said they now cook more from scratch and consume less frozen food, ready meals and takeaways. The results from the current study appear to be consistent with the Australian MoF intervention which had a similarly large sample( Reference Flego, Herbert and Waters 24 ) and a recent Scottish cooking programme by the National Health Service( Reference Garcia, Vargas and Lam 20 ). In these two studies cooking from basic ingredients and cooking confidence increased, the number of takeaway or ready meals reduced and the intake of F&V increased after the intervention( Reference Garcia, Vargas and Lam 20 , Reference Flego, Herbert and Waters 24 ). There were also significant differences between the intervention group and the waiting-list control group in the Australian study for all but fruit and ready meal intake( Reference Flego, Herbert and Waters 24 ). Some differences in the intervention group remained at the further follow-up; however, there was little change in self-reported vegetable intake between post-intervention and follow-up( Reference Garcia, Vargas and Lam 20 , Reference Flego, Herbert and Waters 24 ). The increases in outcome between post-intervention and 6-month follow-up in our study may reflect the MoF ethos from Jamie Oliver about passing on skills learnt or it could be a result of response bias. Our qualitative and quantitative results, combined, suggest that learning ‘hands-on’ cooking skills while being educated about diet and health in an informal group atmosphere may reduce barriers that prevent dietary change.
Both participants from deprived areas and those from non-deprived areas stated in the interviews that the MoF taught them new aspects about nutrition. The qualitative results of the study also suggest that the cooking education provided could increase the ability to control and differentiate between healthy and unhealthy ingredients and portion sizes of food. This outcome may offer advantages within health and weight management, and may support individuals who are managing long-term conditions like obesity or diabetes( Reference Evert, Boucher and Cypress 25 ).
The cost of healthy foods has been perceived to be a barrier to the consumption of a healthful diet among individuals with low income( Reference Ploeg, Breneman and Farrigan 26 , Reference Cox, Anderson and Lean 27 ). In the UK, access to supermarkets remains extremely high( Reference Dibsdall, Lambert and Bobbin 28 ) and supermarkets have successfully used a variety of marketing strategies promoting the purchase of energy-dense, extra value convenience foods, which may be partly responsible for the UK’s current health and social inequality gap( Reference Lawrence, Skinner and Haslam 29 ). Results from the current study, also the MoF intervention evaluated in Australia( Reference Herbert, Flego and Gibbs 30 ) and other cooking interventions( Reference Foley and Pollard 31 , Reference Winkler and Turrell 32 ) suggest new knowledge and practical skills acquired can substantially influence food purchasing decisions, helping to overcome detrimental perceptions and influences that are current barriers to heathy eating. Through the convenient location of the UK MoF, and the market tours that are provided by partner organisations, the MoF increased the awareness and accessibility of affordable healthy ingredients.
Confidence and social benefits
The confidence to cook has been shown to be a major predictor of dietary intake, where a lack of confidence can make an individual less likely to purchase F&V( Reference Winkler and Turrell 32 ). Our evaluation did not measure changes in purchasing patterns and whether this was linked to cooking confidence. However, the quantitative results show that cooking confidence increased dramatically following the 8-week MoF course and was maintained at 6 months after the course, providing both short- and medium-term benefits. While only one question was used in our study, four to five questions assessing cooking confidence were used in the Australia MoF and Scottish studies, and significant increases were observed for all questions after the intervention, but these did not increase further at the follow-up( Reference Flego, Herbert and Waters 24 ).
The results of the interviews in our study also provide evidence of increases in general confidence as well as cooking confidence. Confidence gains were particularly valued among those from deprived areas, those suffering from disabilities and individuals aged over 65 years. Although some with disabilities reported benefiting from reduced social isolation, the quantitative results showed that participants specifically with learning difficulties reported smaller increases in cooking confidence than others. Nevertheless, from the interviews, it appeared that staff interaction and group atmosphere enhanced learning ability and confidence levels of participants with few prior skills and low literacy levels who may struggle to follow formal instructions. General increases in confidence following the MoF may be due to both the acquisition of culinary skills and knowledge, and the numerous social benefits offered within the course resulting from a relaxed, enthusiastic group atmosphere. Collectively, the community interaction and skill acquisition of the MoF may provide a mechanism to increase self-value. This important finding is supported by Foley et al.( Reference Foley, Spurr and Lenoy 33 ), where group dynamics were seen to encourage community discussions while increasing the trust and confidence to share advice and life experiences.
Cooking interventions have tended to primarily target females, rather than males, in the household; in a systematic review of UK cooking interventions over half of the studies (7/13) focused on all or a very high proportion of women( Reference Rees, Hinds and Dickson 34 ). In comparison, the proportion of males attracted to the current study was relatively high; it is possible that this may be due to the Jamie Oliver branding. Despite the majority of women sharing working responsibilities within couples, a considerably higher proportion of women than men are still responsible for food preparation in the UK( Reference Adams, Goffe and Adamson 17 , Reference Lake, Hyland and Mathers 35 ). Not surprisingly, men report being less confident at cooking than women( Reference Adams, Goffe and Adamson 17 ). Within the quantitative results of the current study, the male participants reported significantly greater increases in cooking confidence, while interviews revealed an increase in nutritional awareness, home-made cooking, enjoyment in cooking and confidence in males. The recent nationally representative UK nutrition survey also found that young people (19–34 years) have less confidence with cooking than other age groups in the UK( Reference Adams, Goffe and Adamson 17 ); therefore they have more scope for improvement. However, in our study, younger people (16–19 years) improved in confidence less than 20–64-year-olds. Additionally their F&V intake improved less than 20–64-year-olds’. This indicates that interventions targeting age-specific groups may be more appropriate.
Limitations
The present study adopted a pre-test/post-test design, focusing on a single treatment group with no control group, unlike the Australian MoF intervention which had a non-randomised waiting-list control group( Reference Flego, Herbert and Waters 24 , Reference Flego, Herbert and Gibbs 36 ). Leeds City Council wanted to ensure public health targets were met by maximising numbers on the intervention and did not want a waiting-list control; the study was not intended to be a trial. However, lack of randomisation to a control group means that measured differences between the pre- and post-questionnaire responses cannot be causally related to the intervention. The self-selecting nature of the participants in our study is also a limitation; these individuals may be more health conscious than those who did not apply to the course or follow up a referral from other organisations. Similarly, recent systematic reviews concluded that the evidence on the effectiveness of cooking courses for adults is limited because of limitations of the study designs( Reference Reicks, Trofholz and Stang 14 , Reference Rees, Hinds and Dickson 34 ). Only five out of the thirteen UK studies reviewed used a control group and only one of these randomised participants( Reference Rees, Hinds and Dickson 34 ). That was a study of individuals aged 65 years or older in sheltered housing in socially deprived areas( Reference Moynihan, Moynihan and Zohoori 37 ), these results therefore may not be relevant to other groups. The findings of a recent pilot study to determine the feasibility of evaluating the MoF in the UK using a randomised controlled trial methodology to recruit those most in need of cooking skills suggest it is feasible using community recruitment( Reference Halligan, O’Brien and Purves 38 ).
Another limitation of the current and many other studies in the reviews is that dietary intake and cooking confidence were self-reported and therefore prone to reporting bias. Within the qualitative analysis interviewees may have failed to remember important aspects of the MoF course they attended up to a year before. Furthermore, we assumed reported snacks were unhealthy, and although unhealthy snacks were given as an example, we did not provide guidelines on the questionnaires about whether fruits or other health foods should be included as snacks. Additionally, qualitative results may have been limited by a sample size of forty participants, and it may have been difficult to contact individuals suffering from severe disabilities due to poor communication skills. Nevertheless, quantitative findings in our study are supported by the qualitative results and are consistent with previous literature; however, in order to increase confidence and imply causality, a further study incorporating a control group would be necessary.
As suggested by participants, the course might be improved by including more recipes and longer and flexible course timings. Although the latter may make the course accessible by more people, it may not be feasible. While some individuals, especially from non-deprived areas, wanted advanced classes, it is important to offer the basic course as provided for the majority with lower confidence in cooking. As previously suggested, a booster class could be offered later to help sustain the intervention effects( Reference Garcia, Vargas and Lam 20 , Reference Flego, Herbert and Waters 24 ) and teaching more advanced skills and recipes could be part of this.
Future implications
Cooking interventions are designed to increase the ability to cook and the consumption of healthy home-prepared meals and nutritional knowledge among those who attend. In the current study, the MoF demonstrated the ability of cooking programmes to increase cooking confidence, culinary skills and effect positive dietary changes while also offering a wider range of social outcomes, including an increase in self-efficacy, personal control and general confidence in adults. This suggests that the incorporation of community-based cooking interventions such as the MoF’s as part of government strategy may present an effective mechanism to facilitate positive dietary changes without widening socio-economic inequalities. However, to confirm this further, studies incorporating a control group and participant randomisation are required.
Acknowledgements
Acknowledgements: Thanks to Zest Health for Life (the provider of Ministry of Food Leeds) for sharing the quantitative performance data from the Ministry of Food Service. Thanks to the team at Ministry of Food Leeds in supporting the researchers to access attendees of the service to conduct the qualitative research. Financial support: Ministry of Food has been commissioned by Public Health England since June 2010 to engage vulnerable adults, those at risk of ill health as a result of poor diet and those who are less able or motivated to prepare healthy food at home. It delivers a high-quality cooking skills programme tailored to meet their needs. The Ministry of Food project is a high-profile project for the city of Leeds and serves to promote Leeds Kirkgate Market and show the commitment within the city to tackling the growing national obesity issue and to provide a range of adult learning opportunities. Conflict of interest: There were no conflicts of interest. Authorship: E.K.S. and J.E.C. designed the study, J.F.W. carried out the interviews and qualitative analysis, J.F.W. and J.H. undertook the quantitative analysis, all authors were involved with writing the article. Ethics of human subject participation: This project was covered under part of a block ethics approval MEEC 10–040 for the MSc student project module. The Ministry of Food evaluation form included a section for participants to consent to their details being stored for monitoring purposes and to consent to the University of Leeds contacting them.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1368980016001476





