


Colorectal cancer is one of the most common cancers in the world, accounting for approximately 10 % of the incident cases of cancer(Reference Parkin, Bray and Ferlay1). In Japan, incidence of and mortality from colorectal cancer, especially of colon cancer, have increased markedly in the last few decades(Reference Kono2). Although the increasing trend seems to have ceased in the 1990s(Reference Kono2), Japan is currently among the countries with the highest rates in the world(Reference Parkin, Bray and Ferlay1). Many case–control and cohort studies have addressed the role of dietary factors in the aetiology of colorectal cancer. These studies have suggested that high intakes of red meat and alcohol are related to increased risk of colorectal cancer, while intakes of milk, Ca, garlic and foods rich in dietary fibre are probably related to decreased risk(3). The analysis of dietary patterns has recently drawn much attention regarding diet and colorectal cancer. Foods are consumed in combination, and the high correlation among intakes of individual foods and nutrients makes it difficult to separate their specific effects because of confounding and interaction(Reference Hu4, Reference Jacques and Tucker5). Furthermore, the effects of single nutrients and foods are often too small to detect.
In Western countries, several studies have reported a decreased risk of colorectal cancer associated with a prudent dietary pattern characterised by higher intakes of vegetables and fruits(Reference Flood, Rastogi and Wirfalt6–Reference De Stefani, Deneo-Pellegrini and Boffetta10) and an increased risk with a Western dietary pattern represented by higher intakes of red meat and high-fat foods(Reference Flood, Rastogi and Wirfalt6, Reference Slattery, Boucher and Caan8–Reference Fung, Hu and Fuchs12). However, such associations were not replicated in other studies(Reference Terry, Hu and Hansen13–Reference Kesse, Clavel-Chapelon and Boutron-Ruault15). While traditional foods such as rice, fish and soya products are still commonly consumed, diet has been markedly westernised in the past few decades in Japan(Reference Kono2). A Japanese study also identified dietary patterns that were similar to those observed in the Western populations, but failed to find an association of either prudent or Western dietary pattern with colorectal cancer risk(Reference Kim, Sasaki and Otani16). Another study in Japan reported a decreased risk of colorectal adenomas associated with a prudent dietary pattern characterised by high intakes of dairy foods, vegetables and fruits(Reference Mizoue, Yamaji and Tabata17). In the study reported here, we investigated dietary patterns in relation to colorectal cancer risk in a community-based case–control study, the Fukuoka Colorectal Cancer Study(Reference Kono, Toyomura and Yin18). Because the aetiology of colorectal cancer may differ by site of the colorectum(Reference Potter19), the association with dietary patterns was also examined for different sites of colorectal cancer.
Materials and methods
The details of the methodological aspects of the Fukuoka Colorectal Cancer Study have been described elsewhere(Reference Kono, Toyomura and Yin18). Both cases and controls were residents of Fukuoka City and three adjacent areas. The study protocol was approved by the ethics committees of Kyushu University Faculty of Medical Sciences and of the collaborative hospitals except two, in which no ethics committee existed at the time of the survey, and approval was given by each hospital director.
Subjects
Cases were a consecutive series of patients with histologically confirmed incident colorectal adenocarcinomas who were admitted to either of the two university hospitals or six affiliated hospitals for the first surgical treatment. Eligible cases were 20–74 years of age at the time of the diagnosis; lived in the study area; had no prior history of partial or total removal of the colorectum, familial adenomatous polyposis or inflammatory bowel disease; and were mentally competent to give informed consent and to complete the interview. Research nurses visited each hospital weekly, and determined the eligibility of the cases by referring to admission logs and medical records. They then contacted each eligible patient, and interviewed him/her if written informed consent was given. The survey was started at two university hospitals and three affiliated hospitals in September or October in the year 2000 and at another three affiliated hospitals in May 2001, and was ended in December 2003. Of the 1053 eligible cases, 840 cases (80 %) participated in the interview.
Controls were randomly selected from the community by frequency matching with respect to sex and 10-year age groups on the basis of the estimated sex- and age-specific numbers of colorectal cancer cases. Eligible criteria were the same as those for the cases except that controls did not have a history of colorectal cancer. A total of 1500 persons in fifteen geographical areas were a priori selected by two-stage random sampling using residential registry. Each candidate control was initially contacted by mail and subsequently by telephone. At the most, three further letters of invitation were mailed to non-respondents. The mail invitation revealed that 113 persons were ineligible for the following reasons: death (n 7), migration from the study area (n 22), undelivered mail (n 44), history of large-bowel resection (n 21) and mental incompetence (n 19). In addition, five persons were diagnosed as having colorectal cancer after the survey (n 5). After exclusion of these 118 persons, 833 (60 %) of the 1382 eligible candidates participated in the study.
In the present analysis, we excluded sixty subjects (eighteen cases and forty-two controls) who were less than 40 years old and further thirty-eight subjects (twenty-two cases and sixteen controls) whose energy intakes were in the lowest 1 % or the highest 1 % in each stratum of sex and age class ( < 55, 55–64 and ≥ 65 years). Finally, 800 cases and 775 controls remained. The numbers of colorectal cancer cases by subsite were as follows: proximal colon 181, distal colon 266, rectum 337 and multiple sites 16. Caecum, ascending colon and transverse colon were combined as proximal colon, and distal colon included descending and sigmoid colon. Cases of Dukes' stage A to D numbered 209, 212, 265 and 112; the stage was unrecorded for two cases.
Non-dietary lifestyle questionnaire
Information or lifestyle factors were ascertained by in-person interview using a uniform questionnaire. Interviews for cases were carried out in the hospital during admission, and those for controls were conducted mostly at public community halls or collaborating clinics. The index date was defined as the date of onset of symptoms or the screening leading to the diagnosis for the cases and the time of interview for the controls. For the cases, the interval between the index date and interview ranged from 0 to 36 months with a median of 2 months. Ever-smokers were asked about the duration of smoking in years and numbers of cigarettes smoked per day for each decade of life from the second to the last decade. The cumulative exposure to cigarette smoking until the beginning of the previous decade of age was expressed as a sum of the number of cigarettes smoked per day multiplied by years of smoking in each decade. Habitual alcohol consumption 5 years before the index date was ascertained. The amount of alcohol was expressed using the conventional Japanese units: one go (180 ml) of sake, one large bottle (633 ml) of beer and half a go (90 ml) of shochu were each expressed as one unit; and one drink (30 ml) of whisky or brandy and one glass (100 ml) of wine were each converted to half a unit. Height (cm), current body weight (kg) and body weight (kg) 10 years earlier were reported. BMI (kg/m2) 10 years earlier was used in the analysis because current BMI was unrelated to colorectal cancer risk(Reference Isomura, Kono and Moore20). Body weight 10 years earlier was not ascertained from four cases and ten controls, and was substituted with the current body weight.
Questions on physical activities elicited the type of job, activities in commuting and housework and leisure-time activities 5 years earlier. As described in detail previously(Reference Isomura, Kono and Moore20), leisure-time physical activity (including activities in commuting and housework) was expressed as a sum of metabolic equivalents multiplied by hours of weekly participation in each activity, i.e. in metabolic equivalents hours per week. The use of vitamins or mineral supplements and analgesics was recorded if these had ever been used at least once per week for a period of 6 months or longer. Parental colorectal cancer was also elicited.
Dietary assessment
Interviewers asked each participant about diet over a period of 1 year before the index date using a personal computer software, which was developed for the Fukuoka Colorectal Cancer Study. Details of the development of the software as well as the validity and reproducibility of the estimated intakes have been described elsewhere(Reference Uchida, Kimura and Shirota21). In brief, the software was designed to assess usual dietary intake on the basis of consumption frequency and portion sizes of 148 food/dish items. The collected information was the same as that obtained by the so-called semi-quantitative FFQ. As for consumption frequency, different numbers of response categories were prepared for rice at each meal, other food items and non-alcoholic and alcoholic beverages. Typical dishes were shown on the display for each food item, together with typical portion sizes. Options for serving size were 0·5, 1, 1·5 and 2 of the size displayed as a reference for most of the food items. Based on the interview data on the 148 food/dish items, intakes of 211 food items were obtained for the purpose of estimating nutrient intakes. Several items in the dietary software were mixed dishes or collective foods (such as beef/pork and ham/sausage), and such composite items were disaggregated to the ingredient level of individual foods on the basis of typical recipes and market statistics. Intakes of nutrients were calculated based on the food composition tables in Japan(22), which were supplemented by original data derived from dietary records in a validation study. The validity of the estimated intakes of nutrients and foods was evaluated among twenty-eight control participants who recorded their diet over a period of 7 d in four consecutive seasons. The dietary interview was repeated with an interval of 1 year for these twenty-eight subjects. Pearson's correlation coefficients of energy-adjusted intakes of nineteen selected food groups estimated from the first interview (and from the second interview, given in the parentheses) and diet record ranged from 0·19 (0·13) for potatoes to 0·87 (0·85) for rice with a mean of 0·53 (0·50).
In the analysis on dietary patterns, the 211 food items were aggregated into 29 food groups including 6 specific foods (rice, miso, mayonnaise, coffee, green tea and milk). The grouping was done in accordance with that used in the National Nutrition Survey in Japan(23). Intakes (grams) of these food groups and nutrients were adjusted to an energy intake of 8368 kJ/d (2000 kcal/d) by using the regression residual method.
Statistical analyses
Univariate comparisons between cases and controls were tested by unpaired t test, Wilcoxon rank sum test or χ2 test. We identified dietary patterns using principal component analysis among controls. The factors were rotated by orthogonal transformation (varimax rotation) to maintain the uncorrelated nature of the factors and greater interpretability. Dietary patterns were determined after considering eigenvalues (>1·0), scree test and interpretability of the factors. Dietary patterns were named based on the food groups with the highest loadings on each factor. The factor score for each pattern was calculated for each individual by summing the standardised intakes of the twenty-nine food groups weighted by their factor loadings. Factor scores were categorised into four categories using quartiles in the controls as cut-off points.
The potential confounding variables that were considered were sex, age (continuous value), residential area (Fukuoka City or others), BMI 10 years earlier ( < 22·5, 22·5–24·9 or ≥ 25·0 kg/m2), cigarette smoking (0, 1–399, 400–799 or ≥ 800 cigarette-years), alcohol use (0, 0·1–0·9, 1·0–1·9 or ≥ 2·0 units/d), type of job (sedentary or non-sedentary), leisure-time physical activity (0, 1–15·9 or ≥ 16 metabolic equivalents h/week), parental colorectal cancer and energy intake (quartile categories). Indicator variables were used in statistical adjustment for the categorical factors. Sex- and age-adjusted proportions and means of the covariates according to each dietary pattern score were statistically tested by using the Mantel–Haenszel method and linear regression analysis, respectively, with ordinal values of 0–3 being assigned to the quartile categories of each dietary pattern. The association between each dietary pattern and colorectal cancer risk was assessed by OR, which was estimated by multiple logistic regression. A 95 % CI of OR was estimated by the Wald method. Trend of the association was evaluated by the Wald statistic for an ordinal variable representing the categories of a specific dietary score. Statistical significance was concluded if the two-sided P value was < 0·05, or if 95 % CI did not include unity. All statistical analyses were performed using SAS version 9.2 (SAS Institut, Inc., Cary, NC, USA).
Results
Cases and controls did not differ much in terms of residence, total energy intake and most other potential confounders in either men or women, expect for age and BMI in men (Table 1). Compared with the controls, cases tended to be physically less active in job and leisure time, and to have a parental history of colorectal cancer more frequently. We identified three dietary patterns (Table 2). The first pattern was characterised by high intakes of vegetables, fruits, seafoods and soya foods, and thus was named a prudent dietary pattern. The second pattern represented high intakes of fat and oils, red meat, processed meat and mayonnaise and low intake of rice, and thus it was called a high-fat dietary pattern. High intakes of poultry, bread and noodles also contributed to the high-fat dietary pattern. The third pattern was characterised by high intakes of confectioneries of the Western and Japanese types, dairy products, bread and fruits. These foods are often served as snack or quick meal, and this pattern was named as a light-meal dietary pattern.
Table 1 Characteristics of the study subjects in the Fukuoka Colorectal Cancer Study, Japan, 2000–3†
(Mean values and standard deviations; median values and interquartile (IQR) ranges; proportions)

MET, metabolic equivalents.
Mean values were significantly different: *P < 0·05, **P < 0·01.
† Between-group comparisons were done using unpaired t test for means, χ2-test for proportions and Wilcoxon rank sum test for medians.
‡ Energy-adjusted intake per 8·4 MJ/d.
Table 2 Factor-loading matrix for the major dietary patterns identified by principal component analysis in the Fukuoka Colorectal Cancer Study, Japan, 2000–3

Table 3 shows non-dietary and dietary characteristics according to each dietary pattern score in the control group. Sex and age distributions varied substantially with the score of each dietary pattern. Thus, sex- and age-adjusted means or proportions were presented for the other potential confounding variables. Smoking was less frequent, and leisure-time physical activity was higher in those with higher scores of the prudent dietary pattern. Individuals with higher scores of the light-meal dietary pattern were much less likely to be smokers and alcohol drinkers. Total energy intake was strongly positively associated with the prudent dietary pattern, and also with the light-meal dietary pattern. These associations with total energy intake primarily resulted from adjustment for sex and age. For example, crude energy intakes for the lowest to highest category of the prudent pattern were 8·9, 9·3, 8·9 and 9·1 MJ/d. Total fat intake was progressively greater in those with higher scores of the high-fat and light-meal dietary patterns each.
Table 3 Characteristics according to quartile categories of dietary patterns among controls in the Fukuoka Colorectal Cancer Study, Japan, 2000–3

* Adjusted for sex and age class ( < 54, 55–64 and ≥ 65 years) by direct standardisation for proportions and by ANOVA for means.
† Based on the Mantel–Haenszel method for proportions and linear regression analysis for continuous variables.
‡ Leisure-time physical activity ≥ 16 metabolic equivalents h/week.
§ Geometric means.
‖ Energy-adjusted intake calculated using the regression residual method.
Of the three dietary patterns, the prudent dietary pattern showed a nearly significant association with colorectal cancer risk (Table 4). When the analysis was repeated for men and women separately, an inverse association with the prudent dietary pattern was observed only in men (P trend = 0·04) and not in women (P trend = 0·48), whereas the interaction was far from statistical significance (P = 0·72). For men, multivariate-adjusted OR for the quartile categories (from the lowest to the highest) were 1·0 (referent), 0·95 (95 % CI 0·68, 1·34), 0·79 (95 % CI 0·55, 1·15) and 0·69 (95 % CI 0·46, 1·02), respectively. The corresponding values for women were 1·0 (referent), 1·29 (95 % CI 0·74, 2·27), 0·90 (95 % CI 0·52, 1·56) and 0·98 (95 % CI 0·56, 1·70), respectively. Neither high-fat nor light-meal dietary pattern was associated with colorectal cancer risk in both sexes combined (Table 4) and in men and women separately (data not shown).
Table 4 Risk of colorectal cancer according to quartile categories of dietary pattern scores in the Fukuoka Colorectal Cancer Study, Japan, 2000–3
(Odds ratios and 95 % confidence intervals)

* Number of cases–controls.
† Adjusted for sex, age and residential area.
‡ Additionally adjusted for smoking, alcohol use, BMI 10 years earlier, type of job, leisure-time physical activity, parental colorectal cancer and energy intake.
The prudent dietary pattern was related to a decreased risk of distal colon cancer, but not to that of either proximal colon or rectal cancer, showing a statistically significant trend (Table 5). The high-fat and light-meal dietary patterns were not materially related to site-specific risks of colorectal cancer.
Table 5 Risk of site-specific colorectal cancer according to quartile categories of dietary pattern scores in the Fukuoka Colorectal Cancer Study, Japan, 2000–3
(Odds ratios and 95 % confidence intervals)
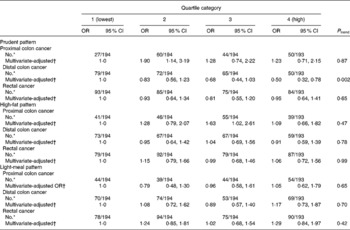
* Number of cases–controls.
† Adjusted for sex, age, residential area, smoking, alcohol use, BMI 10 years earlier, type of job, leisure-time physical activity, parental colorectal cancer and energy intake.
Discussion
The present study identified three dietary patterns, i.e. prudent, high-fat and light-meal patterns, in a Japanese population. Of these, the prudent dietary pattern was found to be associated with a decreased risk of colorectal cancer, especially of distal colon cancer. Neither of the other two dietary patterns showed a measurable association with the overall or site-specific risk of colorectal cancer.
A prudent or healthy dietary pattern has consistently been identified in different studies on the basis of different sets of food groups and items in different populations. This pattern has been characterised by high intakes of vegetables and fruits in general, and additionally, by whole grain in some Western populations(Reference Williams, Satia and Adair9, Reference Fung, Hu and Fuchs12–Reference Wu, Hu and Fuchs14), by soya foods in Asian countries(Reference Kim, Sasaki and Otani16, Reference Masaki, Sugimori and Nakamura24–Reference Nanri, Yoshida and Yamaji28) and by seafoods in both Western(Reference Slattery, Boucher and Caan8–Reference Kesse, Clavel-Chapelon and Boutron-Ruault15) and Asian countries(Reference Kim, Sasaki and Otani16, Reference Cui, Dai and Tseng25, Reference Nanri, Yoshida and Yamaji28). A high-fat or Western dietary pattern, which is characterised by high intakes of red meat and processed meat, is another dietary pattern that has been identified in many previous studies in Asian populations(Reference Kim, Sasaki and Otani16, Reference Mizoue, Yamaji and Tabata17, Reference Masaki, Sugimori and Nakamura24–Reference Nanri, Yoshida and Yamaji28) as well as in Western countries(Reference Flood, Rastogi and Wirfalt6–Reference Wu, Hu and Fuchs14). The light-meal dietary pattern, characterised by high intakes of confectioneries, bread, fruits and dairy products other than milk, was a unique dietary pattern observed in the present study, but the pattern may correspond to a Westernised breakfast pattern reported in other Japanese studies(Reference Masaki, Sugimori and Nakamura24, Reference Nanri, Yoshida and Yamaji28).
A protective association between the prudent or healthy dietary pattern and colorectal cancer has been observed in several studies(Reference Flood, Rastogi and Wirfalt6–Reference De Stefani, Deneo-Pellegrini and Boffetta10), but not in others(Reference Dixon, Balder and Virtanen11–Reference Kesse, Clavel-Chapelon and Boutron-Ruault15), in Western countries. The healthy dietary pattern was unrelated to colorectal cancer risk in Japan(Reference Kim, Sasaki and Otani16) and Singapore(Reference Butler, Wang and Koh26). The present study is the first report to describe decreased risk of colorectal cancer associated with the prudent dietary pattern in Asians. In the present study, component food items of the prudent dietary pattern were almost the same as that reported previously, except for milk and dairy products, which contributed to the prudent dietary pattern in a previous study(Reference Kim, Sasaki and Otani16). While high intakes of vegetables and fruits have been related to decreased risk of colorectal cancer in many case–control studies, prospective studies have generally failed to find a protective association with these dietary factors in both Western and Asian studies(3). However, in a recent pooled analysis of the results obtained from fourteen prospective studies in the United States and Europe, high intake of vegetables and fruits ( ≥ 800 g/d) was statistically significantly associated with a 26 % reduced risk of distal colon cancer, but not with proximal colon cancer(Reference Koushik, Hunter and Spiegelman29). These findings are in agreement with the present findings. In the present study population, high intake of fish was also related to a decreased risk of distal colon cancer specifically(Reference Kimura, Kono and Toyomura30).
The present study found no association between the high-fat dietary pattern and colorectal cancer risk. A high-fat or Western dietary pattern has been more consistently associated with increased risk of colorectal cancer in Western countries(Reference Flood, Rastogi and Wirfalt6, Reference Slattery, Boucher and Caan8–Reference Fung, Hu and Fuchs12). Of the ten studies in Western countries(Reference Flood, Rastogi and Wirfalt6–Reference Kesse, Clavel-Chapelon and Boutron-Ruault15), six studies showed a positive association between Western dietary pattern and colorectal cancer. On the contrary, neither of the two studies of Japanese(Reference Kim, Sasaki and Otani16) and Singapore Chinese(Reference Butler, Wang and Koh26) showed an appreciable association with the Western dietary pattern. High consumption of red meat and processed meat has been associated with a modest increase in the risk of colorectal cancer in Western countries(Reference Sandhu, White and McPherson31, Reference Norat, Lukanova and Ferrari32). Red meat consumption remains much lower in Japan and other Asian countries, and there has been no association between red meat and colorectal cancer(Reference Kimura, Kono and Toyomura30, Reference Lee, Shu and Yang33). It should be noted that poultry as well as red meat was a component food for the high-fat dietary pattern in Asian countries(Reference Kim, Sasaki and Otani16, Reference Mizoue, Yamaji and Tabata17, Reference Masaki, Sugimori and Nakamura24–Reference Nanri, Yoshida and Yamaji28), while high intake of poultry generally contributed to the prudent dietary pattern in Western populations(Reference Slattery, Boucher and Caan8–Reference Wu, Hu and Fuchs14).
The light-meal dietary pattern seems to have been represented by higher intakes of foods, such as confectioneries, bread and fruits, that result in a higher glycaemic load(Reference Foster-Powell, Holt and Brand-Miller34). Thus, it was expected that this dietary pattern might be related to increased risk of colon cancer, as suggested by several recent studies(Reference Gnagnarella, Gandini and La Vecchia35). The present study showed no association between the light-meal dietary pattern and colorectal cancer risk.
The healthy dietary pattern was related to a decreased risk of distal colon cancer, not to that of proximal colon or rectal cancer. The subsite analysis is of particular interest because different aetiological factors may be involved in carcinogenesis at different sites of the colorectum(Reference Potter19). Distal colon cancer shows a greater variation between high-risk and low-risk areas than proximal colon and rectal cancer(Reference Bonithon-Kopp and Benhamiche36). Chromosomal instability characterised by loss of heterozygosity at loci of APC and p53 genes was more frequent in the distal site, while microsatellite instability was almost exclusively associated with proximal colon cancer(Reference Iacopetta37, Reference Gervaz, Bucher and Morel38). However, it should be noted that the site-specific association observed in the present study may have been ascribed to chance due to a subgroup analysis.
Several strengths in the present study deserve to be discussed. In addition to the large size of the study and the use of community controls, the present study was based on a validated dietary method by a computer-assisted interview. A limitation was the retrospective assessment of dietary and other lifestyle factors. Thus, caution is needed while interpreting the present findings, as is always the case with case–control studies. Furthermore, diet in the recent past was used in the present study, and may not have represented long-term habitual consumption relevant to the development of colorectal cancer. While a high participation rate was attained among cases (80 %), the participation rate among controls was lower (60 %). However, this rate was among the highest reported in recent case–control studies using community controls(Reference Olson39). Uses of oestrogenic hormone and non-steroidal anti-inflammatory drugs, which are shown to be related to decreased risk of colon or colorectal cancer(Reference Nelson, Humphrey and Nygren40, Reference Cuzick, Otto and Baron41), were not considered in the present study. We had no information on hormone use; but the use of non-steroidal anti-inflammatory drugs was found to be rare in the study subjects; only sixty-one subjects reported the use of non-steroidal anti-inflammatory drugs. It is generally argued that the findings from the principal component analysis are difficult to extrapolate to different populations because the dietary patterns are a subjective measure specific to a study population. The so-called simplified measure of dietary pattern, which is based on a limited number of foods with the highest loadings, may be an approach to overcome this problem(Reference Schulze, Hoffmann and Kroke42).
In summary, a prudent dietary pattern characterised by high intakes of vegetables, fruits, soya products and seafoods was associated with a decreased risk of distal colon cancer in a fairly large case–control study in Japan. High-fat and light-meal dietary patterns were unrelated to colorectal cancer.
Acknowledgements
The present study was supported by a Grant-in-Aid for Scientific Research on Priority Areas (18014022) from the Ministry of Education, Culture, Sports, Science and Technology, Japan. The authors' responsibilities were as follows: K. K. was involved in data analysis and manuscript preparation; S. B., A. M. J. and G. Y. were involved in data analysis; S. K. was involved in the design of the study, data collection, data management, statistical support and manuscript preparation; K. T., R. M., M. T., Y. K., Y. M., T. O., K. I., K. F., T. M., Y. Y., K. T., H. I. and R. T. were involved in the design of the study and implementation of the survey; and all authors were involved in reading and approval of the final manuscript. None of the authors has a personal or financial conflict of interest. The authors express their appreciation to Emeritus Professor Keizo Sugimachi, and Drs Nobutoshi Imaizumi, Motonori Saku, Yoichi Ikeda, Soichiro Maekawa, Kazuo Tanoue, Kinjiro Sumiyoshi and Shoichiro Saito for conducting the survey of cases. The following physicians kindly supervised the survey of controls at their clinics: Drs Hideaki Baba, Tomonori Endo, Hiroshi Hara, Yoichiro Hirokata, Motohisa Ikeda, Masayoshi Ishibashi, Fumiaki Itoh, Yasuhiro Iwanaga, Hideki Kaku, Shoshi Kaku, Minoru Kanazawa, Akira Kobayashi, Ryunosuke Kumashiro, Shinichi Matsumoto, Soukei Mioka, Umeji Miyakoda, Osamu Nakagaki, Nobuyoshi Nogawa, Nobuyuki Ogami, Toyoaki Okabayashi, Hironao Okabe, Nishiki Saku, Masafumi Tanaka, Masahiro Ueda, Bunichi Ushio and Koheisho Yasunaga. The authors are grateful to research nurses Ms Nobuko Taguchi, Yuriko Moroe, Yuko Noda, Ryoko Tanaka, Hisako Nakagawa and Yoko Mikasa and research clerk Ms Hiroko Mizuta for their careful work.





