


Introduction
Fibromyalgia is a complex multifactorial and of unknown etiopathogenesis, characterized by spread musculoskeletal pain and specific painful points, which are specific to palpation (tender points) and, frequently, associated to tiredness, somnolence, somatic, and cognitive symptoms with psychical disturbances (Wolfe et al., Reference Wolfe, Clauw, Fitzcharles, Goldenberg, Hauser and Katz2016). The total prevalence of fibromyalgia in the general population ranges from 0.2% to 6.6% and is most frequent in women (Marques et al., Reference Marques, Santo, Berssaneti, Matsutani and Yuan2017). The fibromyalgia burden is considerable, with psychosocial consequences, as well as in the basic and instrumental activities of daily life (Antunes et al., Reference Antunes, Vertuan, Miquilin, Leme, Morales and Oliveira2016; Schaefer et al., Reference Schaefer, Mann, Masters, Cappelleri and Daniel2016; Fitzcharles et al., Reference Fitzcharles, Perrot and Häuser2018). Beyond that, fibromyalgia’s economic costs are high and are considered a public health problem (Cabo-Meseguer et al., Reference Cabo-Meseguer, Cerda-Olmedo and Trillo-Mata2017). The ideal treatment for fibromyalgia requires an interdisciplinary approach, including the association of pharmacological and nonpharmacological therapy (Braz et al., Reference Braz, Paula, Fátima and Almeida2011). The pharmacological treatment is essential and performed individually, remaining as a common element in most fibromyalgia cases, while the nonpharmacological treatments are centered on the adaptation process to face the fibromyalgia symptoms (Oliveira and Almeida, Reference Oliveira and Almeida2018).
The recommendations of the European League Against Rheumatism to Fibromyalgia management indicates that the most important strategy must be on the patient’s education. Health education is one of the main items to enable the health promotion at primary health care (Carneiro et al., Reference Carneiro, Souza, Godinho, Faria, Silva and Gazzinelli2012), and must prepare each individual to take control and responsibility for their health (Nutbeam, Reference Nutbeam2018; Oliveira et al., Reference Oliveira, Ferreira, Oliveira, Leme, Antunes and Nascimento Júnior2019). Studies carried out worldwide are still data representations of disciplinary educational interventions, without interdisciplinarity as the focus of attention (Antunes et al., Reference Antunes, Couto, Bertolini, Loures, Schmitt and Marques2021; García-Ríos et al., Reference García-Ríos, Navarro-Ledesma, Tapia-Haro, Toledano-Moreno, Casas-Barragan and Correa-Rodríguez2019). In this sense, the study objective was to develop an educational interdisciplinary program aimed at the health promotion of individuals with fibromyalgia. This study intends to bring the patient’s and the health professional’s perspectives to the design, building, and implementation of an interdisciplinary intervention aimed at improving the health and transforming the healthcare services in Brazil.
Methods
It is a study protocol with a qualitative approach. It was carried out in a Basic Health Unit in the city of São Paulo city, São Paulo State, Brazil. The study was approved by the Research Ethics Committee of the Medical Faculty of the University of São Paulo, approval number 3.197.778.
Participants received written and verbal clarification about their participation in the study. The individuals with fibromyalgia and the health professionals received and signed an informed consent form. Fibro Friends is based on integrative community therapy which is a guide to health practices. The integrative community therapy is a therapeutic model created after World War II, when an American psychosociologist, Kurt Lewin, worked through a group of people with therapeutic results. He asserts that individuals feel a therapeutic benefit when listening to people who share their problems, as they talk about how these problems can be solved. The integrative community therapy was developed in Brazil to create supportive social networks aimed at life promotion, raising resources, and the individuals, families, and communities’ competencies, to promote empowerment. This practice is interesting for the promotion of wellbeing, health, and social rights, it seeks to enhance the group’s therapeutic dimension, to value the cultural background, as well as the knowledge gathered by the life experience of each individual and is enlisted in the “Integrative and Complementary Practices on Health in Brazil” (Práticas Integrativas e Complementares em Saúde no Brasil) (Barreto, Reference Barreto2008). Fibro Friends Program presents as a goal, to guide and teach self-care techniques to individuals with fibromyalgia, and to its construction, the following steps were implemented.
First phase: requisite analysis, contents, and establishing the programs’ objectives
A total of 12 individuals with clinical fibromyalgia diagnosis were invited. The criteria were confirmed by an evaluator according to the ‘Classification Criteria of the American College of Rheumatology’, revised version of 2016 (Wolfe et al., Reference Wolfe, Clauw, Fitzcharles, Goldenberg, Hauser and Katz2016), the participants were users of the Brazilian Unified Health System (SUS – Sistema Único de Saúde), with complete elementary school grades to participate in qualitative research through group discussion. Since it is a qualitative approach, the sample is defined by the saturation of the question to be analyzed. There was not, therefore, a previous statistic estimate to define the number of subjects to compose the sample. Therefore, once we have deep and sufficient information for a scientific investigation, data collection might be ended and considered finished. The interview technique, due to the time involved and deepness of the search, limits the number of individuals to be researched. The most common and indicated group technique in qualitative researches is the focal group. The focal group is a type of interview which is generally carried out with a small and homogeneous group from 6 to 12 people (Pelicioni, Reference Pelicioni2001). The group meeting aimed at identifying, through these individuals’ speeches, the needs, and problems reported by the individuals with fibromyalgia and the possibilities for an interdisciplinary professional team to meet these requirements and to solve the problems.
Also, it was requested by the responsible physiotherapist, that they specified the number, the time length, and the frequency of meetings. At the end of this phase, the two physiotherapists responsible for the project, have listed the topics mentioned by the individuals suffering from fibromyalgia. Moreover, 10 professionals dealing with primary health care at the Unified Health System (SUS) were invited to participate in the group discussions about the program development. The choice of the number of professionals was according to the interdisciplinarity and with the possibility of a positive contribution to the aspects related to the quality of life of an individual with fibromyalgia. The invited health professionals were a Physiotherapist, a Doctor, a Psychologist, a Nutritionist, a Nurse, a Pharmacist/Druggist, a Speech Therapist, an Occupational Therapist, a Naturopath, and a Social Worker. This meeting aimed at questioning the professionals about what interdisciplinary matters are important, practical, and necessary to be approached by the program in primary health care, based on the professionals’ experience and on the current scientific evidence to fibromyalgia treatment, as well as the number, the time length, and the frequency of meetings. The project proposes to do group work rather than individual treatments. The program’s proposal is an interdisciplinary approach and all professionals that are in primary health care could participate.
Data collection
The qualitative research was carried out through spontaneous oral speeches, in which the individuals with fibromyalgia and the healthcare professionals have spontaneously spoken about the investigated theme. Qualitative research considers exclusively meanings and processes, and not measurements. The results are presented descriptively and not numerically (Salmon and Young, Reference Salmon and Young2018). It is important to highlight that, this type of research depends on the precision of the interviewer’s intuition and ability in dealing with resources and techniques to represent the phenomenon, as there are not formulated hypothesis, and also, there are no absolute criteria for data collection (Canzonieri et al., Reference Canzonieri, Pollak and Martins2009). In this study, the saturation criterion was not applied, because the purpose was to collect responses from professionals and patients who were invited to participate in the study. The questioning of the professional and the patient were executed the same way, allowing them to freely express themselves. In all the conversations, interviewers and interviewees talked in a calm voice tone and a tranquil verbal and body expression. There were no difficulties. The interview was performed using a portable digital recorder (model Zoom H4N PRO – 2018).
Data collection took place at the Basic Health Unit, in a private location, through group interviews combined with participative observation techniques, from September 3rd, 2019 to October 22nd, 2019, at days and hours previously established by the interviewer. The average data collection time with each group was 1 h and 30 min. The script elaborated by the researchers had pertinent questions to the researched problem. The average data collection time with each group was 1 h and 30 min. The orienting script, elaborated by the researchers, has contemplated pertinent questions to the researched problem.
Content analysis
For the content analysis, the data collected were transcribed, organized with Excel and Word software, and the answers were mapped, allowing a panoramic content reading. Afterward, these data were analyzed through content analysis proposed by Bardin (Reference Bardin1979), specifically the thematic content analysis (Minayo, Reference Minayo2008), which has allowed the organization of textual content, creating categorizations to enable inferences and to recognize patterns.
The different phases of content analysis have been organized around three poles:
-
1) Pre-analysis (audio hearing and checking the notes)
-
2) Material exploration (interview transcription)
-
3) Data treatment (inference and Interpretation)
In this phase, a tool was used for the visualization and mapping of the most recurrent topics in all interviews analyzed. The speeches were categorized by items in a table which considered those that refer to facing the problem, interdisciplinary information, and educational program structure. These categories were created based on Werneck et al. (Reference Werneck, Faria and Campos2009) who attribute the main criteria to the creation of healthcare protocols and organization of health services.
Second phase: program development
The program development was performed through information supplied by individuals with fibromyalgia and also by healthcare professionals, a program structure presenting in each thematic the conditions offered by the professional, the activities to be performed by the patients and the activity product, as well as the number, the time length, and the frequency of meetings. This phase was carried out by two responsible physiotherapists. The conditions refer to the main theme and the way to approach it. Concerning the activities to be carried out by the participants, in this item, there is a detailed account of which is expected that people with fibromyalgia learn and make in each meeting. The participants’ activity product refers to the knowledge that the participant of the Fibro Friend Program must have after each meeting. Those items of program creation were based on Brasil (2007).
Third phase: program validation
In this phase, after the program development, the two physiotherapists responsible for the project have presented the program structure to the 12 individuals with fibromyalgia who have participated in the first phase of the study in a group meeting. It was also realized a meeting in a group with the 10 professionals who participated in the first phase of the study to do content validation. The two meetings (patient group and professional group) were carried out on different days and hours, and the posterior meeting of patients and professionals was not carried out. This validation step sought to allow individuals with fibromyalgia and professionals, getting to know the program structure and the possibility of adjusting before starting the viability study phase.
Results
The results will be presented in the thematic category description defined by the professionals and individuals with fibromyalgia. The interdisciplinary program structure of promotion to fibromyalgia patients was conducted using a combination of activities that have followed the series of themes addressed which are based on the National Policy of Health Promotion. As a primary outcome, the study participants have chosen the ‘quality of life’, the secondary ones were: ‘level of pain’, ‘sleep quality’, and ‘self-care management’. A physical exercise program will also be carried out. To an educational program in health, directed to people with fibromyalgia, 15 weekly meetings lasting 1 h and 20 min are suggested on Tuesdays afternoon (Table 1).
Table 1 Description of Fibro Friends
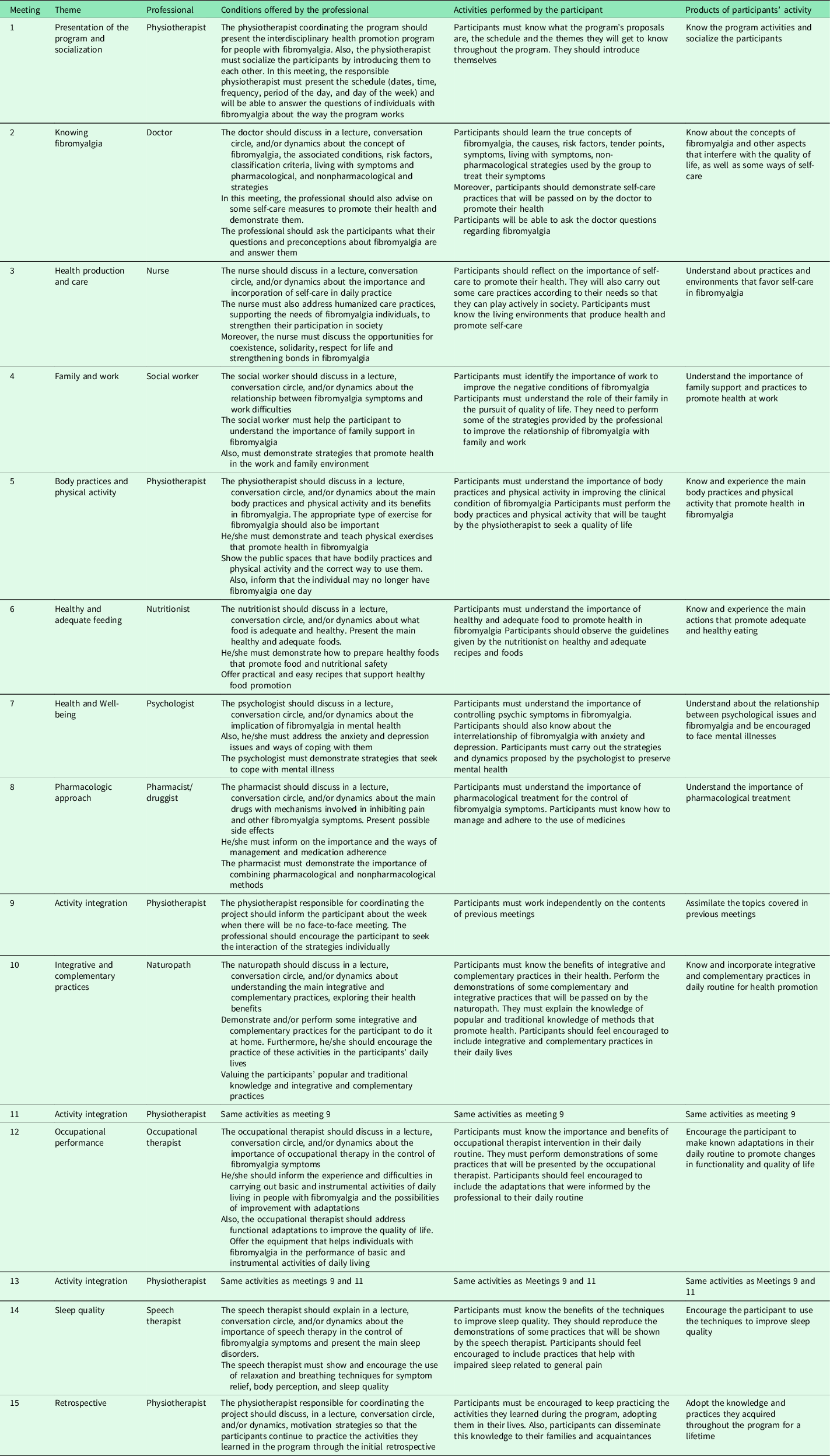
The schedule summary of Fibro Friend is described in Table 1.
Discussion
An interdisciplinary health promotion program was jointly created for the health promotion of individuals with fibromyalgia, named Fibro Friends’. The Patient’s education is considered as the first step for the self-management of symptoms of fibromyalgia (García-Ríos et al., Reference García-Ríos, Navarro-Ledesma, Tapia-Haro, Toledano-Moreno, Casas-Barragan and Correa-Rodríguez2019). A patient’s education is defined as any set of educational activities planned by qualified professionals and intended to improve health behavior and/or the patient’s health. Beyond that, the patient’s education seeks to inform and restructure the perceptions about the disease (García-Ríos et al., Reference García-Ríos, Navarro-Ledesma, Tapia-Haro, Toledano-Moreno, Casas-Barragan and Correa-Rodríguez2019). To reduce the disparity between the perception of pain that the patient and the health professional have and their treatment, it is necessary to change the maladaptive perception that patients have of the disease, reconceptualizing the pain, the disease itself, and the symptoms presented (Nijs et al., Reference Nijs, Paul van Wilgen, Van Oosterwijck, Ittersum and Meeus2011; García-Ríos et al., Reference García-Ríos, Navarro-Ledesma, Tapia-Haro, Toledano-Moreno, Casas-Barragan and Correa-Rodríguez2019).
Therefore, the patient’s education must be based on approaches that provide knowledge and information about the disease, the planned treatment, the strategies, and the expected outcomes (Hawkins, Reference Hawkins2013; Häuser et al., Reference Häuser, Ablin, Perrot and Fitzcharles2017). To develop a treatment that meets the patients’ needs, obtaining a long-term adhesion, it is essential to understand the patients’ perspectives – their expectations, their living experience of intervention, their acceptability, their lifestyle adequacy and results, and efficacy on the perceptions (Ashe et al., Reference Ashe, Furness, Taylor, Haywood-Small and Lawson2017).
The primary management must involve the patient’s education and the focus on nonpharmacologic therapies. In the case of nonresponsive treatment, other therapies must be adapted to the specific individual’s needs and might involve psychological therapies, pharmacotherapy, and/or a combined rehabilitation program (Macfarlane et al., Reference Macfarlane, Kronisch, Dean, Atzeni, Häuser and Fluß2016). To deal with the chronic pain condition, cognitive behavioral therapy is indicated to allow daily life activities and professional and social life participation (Sauer et al., Reference Sauer, Kemper and Glaeske2011; Gregório et al., Reference Gregório, Antunes, Acencio, Vissoci and Oliveira2018).
In this sense, this program will be based on cognitive behavioral therapy which is some of the therapies focused on behavior, emotions, and symptoms. This approach has an emphasis on the individual’s current situation rather than in past situations. Thoughts may represent cognitive alterations which might influence directly the individual’s health condition. In this sense, this therapy seeks to change the individual’s behavioral aspects, stimulating him/her to review inadequate attitudes and beliefs which might be negatively influencing their health condition (Bennett and Nelson, Reference Bennett and Nelson2006; Williams, Reference Williams2006; Minelli and Vaona, Reference Minelli and Vaona2012).
Qualitative studies about the fibromyalgia patient’s perspectives highlight worries, as the lack of information provided by healthcare professionals; a general lack of understanding by the family, friends, and society; trouble in adapting to fibromyalgia’s pain, fatigue, and powerlessness (Ashe et al., Reference Ashe, Furness, Taylor, Haywood-Small and Lawson2017). In this sense, it is evident that the need to continue studying the therapeutic approaches to fibromyalgia worldwide, mainly in Brazil (Cabo-Meseguer et al., Reference Cabo-Meseguer, Cerda-Olmedo and Trillo-Mata2017).
In this sense, the creation of combined programs is encouraged and, in particular, in the follow-up, the habit modification and self-efficacy, in response to some of the current limitations in the intervention with these patients (Pérez-Velasco and Peñacoba-Puente, Reference Pérez-Velasco and Peñacoba-Puente2015). Thus, the ‘Fibro Friends Program’ will have as a contribution to the health system, qualified information which will serve as a support to healguide the effectiveness, evaluation, and viability of a health promotion program to people with fibromyalgia in Brazil.
Conclusion
Fibro Friends is the first interdisciplinary program in Brazil to promote health for fibromyalgia individuals. It was created based on scientific evidence, clinical experience, and patient’s opinion. The authors suggest that healthcare professionals recommend using this program to their patients as an auxiliary resource to promote health in fibromyalgia.
Practical implications
Fibro Friends was created from the joint action of patients and healthcare professionals. It can be an effective educational tool to be implemented at primary health care centers, promoting self-care, quality of life, and health promotion in individuals with fibromyalgia. Fibro Friends is an outstanding tool for patient education and counseling in Brazil.
Future research
The next step is employing the ‘Fibro Friends Program’ through an important random clinical essay to assess the efficiency of the interdisciplinary program of health promotion in patients with fibromyalgia, and, soon, the researchers must provide new information about this subject. The protocol was registered at the Brazilian Registry of Clinical Essays (Registro Brasileiro de Ensaios Clínicos – ReBEC) under reference number: (RBR-3rh759).
Acknowledgments
We are grateful to the Coordination for the Improvement of Higher Education Personnel (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES) for encouraging research.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict(s) of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.


 Open access
Open access