



Introduction
One of the major developmental tasks for preschool children is prosocial skill development, or capacities for emotional regulation, cooperation, and altruistic behavior, all of which are essential for the cultivation of successful social relationships (Eisenberg et al., Reference Eisenberg, Fabes, Spinrad, Damon and Lerner2006). Research has indicated that children with greater prosocial skills – and more positive social relationships – are better able to avoid negative developmental outcomes (Lansford et al., Reference Lansford, Malone, Stevens, Dodge, Bates and Pettit2006). In general population studies, researchers have identified great variation and distinct developmental trajectories of prosocial skills among young children (Berry & OʼConnor, Reference Berry and OʼConnor2010; Kokko et al., Reference Kokko, Tremblay, Lacourse, Nagin and Vitaro2006; Lamont & Van Horn, Reference Lamont and Van Horn2013; Takahashi et al., Reference Takahashi, Okada, Hoshino and Anme2015). However, little research has examined the variation in prosocial skills over time (e.g., decreasing, increasing, stable low) among young children exposed to intimate partner violence (IPV), despite prior cross-sectional studies suggesting exposure to IPV as a key risk factor linked to lower prosocial skills among young children (Fantuzzo et al., Reference Fantuzzo, DePaola, Lambert, Martino, Anderson and Sutton1991; Holmes et al., Reference Holmes, Voith and Gromoske2015; Howell et al., Reference Howell, Graham-Bermann, Czyz and Lilly2010). Furthermore, it is unknown whether IPV exposure and other co-occurring risk factors affect prosocial skill development over time or what potential protective factors may promote better prosocial skill development among children exposed to IPV. These are important research gaps given that identifying varying patterns of prosocial development and understanding key risk and protective factors associated with the variation in prosocial trajectories among children exposed to IPV can inform intervention design to promote prosocial behaviors among at-risk children. Therefore, this study examined the extent to which the development of prosocial skills varied, how IPV exposure explained the variation in prosocial skill development over time, and the extent to which protective factors (i.e., preschool attendance, maternal warmth, maternal responsiveness, neighborhood safety) and risk factors (i.e., maternal depression, child maltreatment) contribute to variation in the development of prosocial skills.
Heterogeneity of prosocial skill development
The developmental psychopathology perspective (Sroufe & Rutter, Reference Sroufe and Rutter1984) emphasizes that early experiences set the foundation for later development and that behavior develops through the ongoing interaction between children and their environment. According to this perspective, even when children are exposed to similar environmental experiences (i.e., child maltreatment, IPV exposure), their behavioral outcomes can differ significantly due to variation in their individual constellations of risk and protective factors. For example, it is possible that children who have been exposed to co-occurring child maltreatment and IPV may display different patterns of prosocial skill development because of multiple protective factors present throughout development (Holmes et al., Reference Holmes, Bender, Crampton, Voith and Prince2019). This would suggest that there may be individual differences in developmental trajectories of prosocial skills. Said differently, there may be distinct subpopulations within the broader population. For example, among children exposed to frequently co-occurring child maltreatment and IPV, it is possible that unique subgroups of children might be observed to share specific patterns, or trajectories, of prosocial skill development over time given the presence of multiple protective factors throughout development (Holmes et al., Reference Holmes, Bender, Crampton, Voith and Prince2019). This would evidence distinct subpopulations of prosocial skill development, despite similar adverse exposures, within the broader population. As a result of advances in statistical analyses, researchers are able to use person-centered approaches that allow for empirical identification of subgroups based on their patterns of developmental trajectories (Jung & Wickrama, Reference Jung and Wickrama2008; Muthén & Muthén, Reference Muthén and Muthén2000). Yet, to the authors’ knowledge, no research has examined the variation (e.g., decreasing vs. increasing, high vs. low) in patterns of prosocial development over time among IPV-exposed children or the potential contribution of IPV exposure and protective factors to distinct developmental trajectories of prosocial skills. A life course perspective (Elder et al., Reference Elder, Johnson, Crosnoe, Mortimer and Shanahan2003) emphasizes that human development is a long-term dynamic process and that individuals’ developmental pathways can vary by contexts within which they are embedded. Drawing from the life course perspective, examining the variation or heterogeneity in the developmental trajectories of prosocial development among children exposed to IPV can offer valuable insight into intervention efforts, by pointing out when and in what context divergent trajectories emerge over the life course. For example, if we find that involvement with the child-welfare system is associated with decreasing prosocial skills during the school-age period, then targeted social skills intervention and additional support could be provided to this population during school-age years to promote healthy patterns of prosocial development.
Earlier studies examining the general population have suggested that children’s prosocial skill development follows a curvilinear pattern, with development accelerating at different times throughout childhood, specifically between kindergarten and third grade (Berry & OʼConnor, Reference Berry and OʼConnor2010; Lamont & Van Horn, Reference Lamont and Van Horn2013). Although these studies indicate that there is heterogeneity in prosocial skill developmental trajectories from kindergarten to third grade, the researchers assumed that there was normal variability across individuals, and therefore estimated a mean trajectory of prosocial skill development. However, the observed variability in a sample may also suggest that there are multiple pathways of development (i.e., distinct subgroups).
To better examine heterogeneous patterns, researchers have more recently used a person-centered approach to identify subgroups of prosocial skill development. Kokko et al. (Reference Kokko, Tremblay, Lacourse, Nagin and Vitaro2006) identified two distinct prosocial skill development trajectories among males between ages 6 and 12; the majority (57%) were in the low declining group and the remaining in the moderate declining group. Lamont and Van Horn’s (Reference Lamont and Van Horn2013) longitudinal study examining social skills among 6,964 children from kindergarten to third grade identified three classes of social skill development: an ongoing stable trajectory included the majority of the sample (86%), a stable-then-increasing trajectory encompassed about 8% of the sample, and a stable-then-decreasing trajectory included about 6% of the sample. Both curvilinear trajectories were stable during kindergarten then either increased or decreased between first or second grade (i.e., ages 6–7 years old). Takahashi et al. (Reference Takahashi, Okada, Hoshino and Anme2015) examined prosocial skill development among 1,055 Japanese children between the ages of 2 and 5 and identified three distinct groups, including low to slight increase, sharp increase, and high increase. Interestingly, all three studies found different curvilinear trajectories, which may suggest that normative prosocial skill development may have periods of acceleration, deceleration, or stability over time.
Although general population studies have evidenced heterogeneity in prosocial skill developmental trajectories, it is unknown whether the trajectories in prosocial skill development among the general population hold in a population that has experienced adverse life events (e.g., IPV exposure, child maltreatment). At-risk populations, such as those exposed to IPV, may show a decreasing or consistently low pattern of prosocial skill development resulting from the trauma associated with adverse life experiences, but this has not been empirically investigated. Most general population studies are also limited in that they examined prosocial skill development from kindergarten on, which provides limited understanding of earlier prosocial skill development. Only one study, to our knowledge, examined prosocial skill development among 2 to 5 year olds in a sample of Japanese children (Takahashi et al., Reference Takahashi, Okada, Hoshino and Anme2015). Considering that prosocial skill development begins around the preschool years (e.g., Dunn & Munn, Reference Dunn and Munn1986) and that the primary emphasis of preschool is social development, it is important to examine prosocial skill development starting in preschool (age 3) through the early school years.
Effect of IPV exposure and other risk factors on children’s prosocial behavior
IPV continues to be a national problem, with more than 1 in 4 women (30 million) and more than 1 in 10 men (12.1 million) reported to have experienced physical violence, sexual violence, or stalking by an intimate partner at least once in their lives (Smith et al., Reference Smith, Zhang, Basile, Merrick, Wang, Kresnow and Chen2018). On average, women who said they were physically assaulted more than once reported victimization occurring over 4.5 years (Tjaden & Thoennes, Reference Tjaden and Thoennes2000). Child exposure to IPV is an equally concerning issue. A national survey showed that a quarter of all children under the age of 18 have witnessed a physical assault between caretakers in their lifetime, with more than 6% being exposed in the past year (Finkelhor et al., Reference Finkelhor, Turner, Shattuck and Hamby2015). There is also a high economic burden associated with IPV exposure, totaling $55 billion in the form of increased health care costs, increased crime costs, and reduced workforce productivity (Holmes et al., Reference Holmes, Richter, Votruba, Berg and Bender2018).
Although only a small number of studies have examined the effect of IPV exposure on child prosocial skills, these studies consistently suggest that IPV-exposed children tend to have poorer prosocial skills than non-exposed children. For example, Fantuzzo et al.s’ (Reference Fantuzzo, DePaola, Lambert, Martino, Anderson and Sutton1991) cross-sectional study found that preschool-age children (i.e., 3–5 years) residing in domestic violence shelters who had witnessed both physical and verbal aggression between their parents demonstrated significantly lower levels of prosocial skills compared with those who had not been exposed to violence. Howell et al. (Reference Howell, Graham-Bermann, Czyz and Lilly2010) studied 56 children between the ages of 4 and 6 years from low-income families, all of whom were exposed to IPV during the previous year. They found that the more frequently a child was exposed to IPV in the previous 12 months, the less likely they were to demonstrate competence in prosocial behavior and emotional regulation. Holmes et al. (Reference Holmes, Voith and Gromoske2015) found a similar, but delayed, longitudinal effect of exposure to IPV on children’s prosocial skills through aggression. Children’s exposure to IPV was related to significantly more aggression during preschool, which, in turn, was associated with decreased prosocial skills during elementary school, suggesting that exposure to IPV may affect children’s prosocial skills over time through other domains of behavior (Holmes et al., Reference Holmes, Voith and Gromoske2015).
Studies examining links between children’s exposure to violence and their social functioning and adaptation have suggested that youth exposed to violence tend to demonstrate less success in developing, navigating, and maintaining social relationships. Though limited, some family violence research has specifically explored the effects of child maltreatment on children’s prosocial skills. In general, cross-sectional studies have identified significant prosocial skills deficits in both preschool-age (Darwish et al., Reference Darwish, Esquivel, Houtz and Alfonso2001; Fantuzzo et al., Reference Fantuzzo, Weiss, Atkins, Meyers and Noone1998) and school-age children (Shonk & Cicchetti, Reference Shonk and Cicchetti2001; see also Holosko, Reference Holosko2015) with maltreatment histories. One longitudinal study, following children from birth to 9 years old, found that the more developmental periods characterized by maltreatment, the poorer a child’s prosocial skills (Jaffee & Maikovich-Fong, Reference Jaffee and Maikovich-Fong2011).
Other family-level characteristics have also been identified as risk factors for poorer prosocial skill outcomes. Maternal mental health has been identified as a significant predictor of social-emotional functioning among preschool-aged children exposed to IPV, even after controlling for violence severity or other demographic factors (Howell et al., Reference Howell, Graham-Bermann, Czyz and Lilly2010). Children of mothers with fewer depressive symptoms reported significantly higher prosocial skills than children with mothers with greater depressive symptoms (Howell et al., Reference Howell, Graham-Bermann, Czyz and Lilly2010). Poorer maternal mental health can limit the ways in which caregivers provide attuned and effective parenting (e.g., regulation or social skill modeling) that is essential for prosocial skill development (Howell et al., Reference Howell, Graham-Bermann, Czyz and Lilly2010, Reference Howell, Thurston, Hasselle, Decker and Jamison2021). Caregiver education and income, as indicators of socioeconomic status, have also been identified as predictors of child prosocial skill development (Garner, Reference Garner2006; Hosokawa & Katsura, Reference Hosokawa and Katsura2017). Lower caregiver education and income have both been associated with lower child prosocial skill development through financial stress (see Conger et al., Reference Conger, Conger and Martin2010) which may then result in more authoritarian or controlling parenting styles that are less conducive to prosocial skill development (Garner, Reference Garner2006; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021).
Although this literature is limited, results of these collective studies underscore a similar trend: children exposed to family violence (i.e., maltreatment or IPV) tend to exhibit more prosocial skills deficits than children never exposed to any type of family violence (Bevilacqua et al., Reference Bevilacqua, Kelly, Heilmann, Priest and Lacey2021; Darwish et al., Reference Darwish, Esquivel, Houtz and Alfonso2001; Fantuzzo et al., Reference Fantuzzo, Weiss, Atkins, Meyers and Noone1998; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Shonk & Cicchetti, Reference Shonk and Cicchetti2001). However, due to the limited number of studies examining the specific effect of IPV exposure on children’s prosocial skills, further research examining this relationship is warranted.
Protective factors promoting prosocial skills
Factors that promote prosocial skills among children include parent-level factors (e.g., maternal warmth, maternal responsiveness; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Oravecz et al., Reference Oravecz, Koblinsky and Randolph2008), school-level factors (e.g., preschool attendance; Moore et al., Reference Moore, Cooper, Domitrovich, Morgan, Cleveland, Shah, Jacobson and Greenberg2015), and neighborhood-level factors (e.g., neighborhood safety; Criss et al., Reference Criss, Shaw, Moilanen, Hitchings and Ingoldsby2009; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021). Each of these environments – family, school, and neighborhood – provide important experiences and opportunities for children to develop prosocial skills (Criss et al., Reference Criss, Shaw, Moilanen, Hitchings and Ingoldsby2009; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021). The role of parents in promoting resilience among children with maltreatment histories has been well studied, with a smaller body of literature focusing on parent-level protective factors related to prosocial skill development among IPV-exposed children in particular. Studies have consistently found that positive parenting characteristics (e.g., emotional support, high monitoring/supervision, maternal responsiveness) were associated with higher levels of social skills (e.g., social competence, prosocial skills) and increasing developmental trajectories of prosocial skills among young IPV-exposed children (Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Oravecz et al., Reference Oravecz, Koblinsky and Randolph2008).
Beyond the family environment, preschool also provides an important milieu in which children achieve developmental tasks, including the development of prosocial skills. While the cognitive benefits of preschool attendance are widely recognized (e.g., Bassok, Reference Bassok2010; Geoffroy et al., Reference Geoffroy, Côté, Giguère, Dionne, Zelazo, Tremblay, Boivin and Séguin2010), positive social and emotional outcomes are also associated with preschool attendance (Moore et al., Reference Moore, Cooper, Domitrovich, Morgan, Cleveland, Shah, Jacobson and Greenberg2015). Findings from a study of at-risk children ages 3 to 5 years old suggest the importance of preschool duration, coupled with preschool quality, on child social and cognitive development (Hall et al., Reference Hall, Sylva, Sammons, Melhuish, Siraj-Blatchford and Taggart2013). Children who attended higher-quality preschools for a longer period of time demonstrated improved social and cognitive development at age 5 when compared with children who attended poorer-quality preschools for a shorter period of time (Hall et al., Reference Hall, Sylva, Sammons, Melhuish, Siraj-Blatchford and Taggart2013). Preschool attendance can be particularly beneficial for children who have been exposed to IPV and other early traumatic experiences by providing safe, caring, and predictable caregiving environments necessary for promoting regulation and coping skills (Barfield et al., Reference Barfield, Dobson, Gaskill and Perry2012; Perry, Reference Perry2002). The implications of these findings are meaningful in both the short and long term; preschool attendance is associated with overall social competence and school readiness and is consequential for future scholastic success, academic achievement, and overall positive social development (Arnold et al., Reference Arnold, Kupersmidt, Voegler-Lee and Marshall2012; Clements et al., Reference Clements, Reynolds and Hickey2004).
Neighborhoods also offer important contexts for a child’s social development; neighborhood environments may directly (e.g., community violence exposure) or indirectly (e.g., via increased maternal stress) affect a child’s development (Criss et al., Reference Criss, Shaw, Moilanen, Hitchings and Ingoldsby2009; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021). Direct associations between neighborhood characteristics and child adjustment outcomes have been observed; low perceived neighborhood dangerousness in early childhood was significantly related to higher social skills during adolescence (Criss et al., Reference Criss, Shaw, Moilanen, Hitchings and Ingoldsby2009), whereas more neighborhood problems were associated with physical aggression and other externalizing behaviors among children throughout early and middle childhood (Kim & Glassgow, Reference Kim and Glassgow2018; Pei et al., Reference Pei, Yoon, Maguire-Jack and Lee2022; Romano et al., Reference Romano, Tremblay, Boulerice and Swisher2005). Neighborhood dangerousness and maternal-level factors (e.g., maternal depressive symptoms) have been found to be significantly correlated, lending support to the assertion that neighborhood factors may contribute to parenting stress and have indirect effects on child development (Criss et al., Reference Criss, Shaw, Moilanen, Hitchings and Ingoldsby2009).
Current study
Framed by the developmental psychopathology perspective, this study aimed to (a) examine the extent to which the development of prosocial skills varies in a sample of child welfare-involved children, (b) explore how IPV exposure explains the variation in prosocial skill development over time, and (c) examine the extent to which protective factors (i.e., preschool attendance, maternal warmth, maternal responsiveness, neighborhood safety) promote prosocial skill development while controlling for risk factors (i.e., maternal depression, child maltreatment, family income, maternal education). We hypothesized that distinct trajectories of prosocial skill development would be identified, that IPV exposure would be associated with group membership in the decreasing prosocial skill trajectories, and that protective factors would be related to group membership in increasing prosocial skill trajectories.
Method
For this retrospective cohort study, we conducted secondary data analyses using the National Survey of Child and Adolescent Well-Being (NSCAW-I), a United States national longitudinal study designed to examine outcomes of children referred to child protective services (CPS) for abuse or neglect between October 1999 and December 2000. Caregivers, children, teachers, and caseworkers were interviewed at five time points after the close of the CPS investigation: baseline, 12, 18, 36, and 59–96 months (Dowd et al., Reference Dowd, Kinsey, Wheeless, Thissen, Richardson, Mierzwa and Biemer2002). While all children were investigated for maltreatment, not all children had substantiated cases. This study was approved by the Case Western Reserve University Institutional Review Board.
Sample
The study sample included 1,678 children between the ages of birth and 5 years at baseline who were not removed from their home following investigation and who lived with their biological mother. At the fifth time point, children were between the ages of 5 and 10 years old.
Measures
Child prosocial skills
The Social Skills Rating System (SSRS) measured the caregiver’s perception of the child’s prosocial skills related to four domains: cooperation (e.g., follows household rules, works well with family members), assertion (e.g., asks for help from an adult, stands up for themself when treated unfairly), responsibility (e.g., respects the property of others, is well-behaved when unsupervised), and self-control (e.g., resolves disagreements calmly, makes a compromise during a conflict; Gresham & Elliott, Reference Gresham and Elliot1990). The SSRS contained 39 items for children 3 to 5 years old and 38 items for children 6 to 10 years old. Items were on a 3-point Likert scale (1 = never, 2 = sometimes, 3 = very often). Scores were summed and then standardized based on percentiles for a normative sample. Internal consistencies in the current study for children 3 to 5 years old for all time points ranged from 0.89 to 0.90, and from 0.80 to 0.88 for children 6 to 10 years old.
Exposure to IPV
IPV occurring in the home was measured by the physical assault subscale of the Conflict Tactics Scale (CTS; Straus, Reference Straus1979), which assessed the female caregiver’s experience with physical violence perpetrated by her partner (9 items; e.g., pushed, slapped, choked, threatened with a knife or gun). Response categories ranged from 0 (never) to 6 (>20 times), indicating the frequency of behavior in the past year. Internal consistency ranged from .75 to .83 across time points. We then coded IPV as either having been experienced (1) or not (0). An IPV exposure timing variable was created by recoding IPV exposure based on the child’s developmental stage in which the IPV exposure occurred. Erikson’s stages of psychosocial development were used to identify three developmental stages: infancy/toddlerhood (0–2 years); preschool (3–5 years); and school age (6–13 years). For each developmental stage, IPV exposure variables were coded as yes (1) or no (0).
Protective factors
Preschool attendance was reported by the mother who indicated the current grade of the child. For children who were ages 3 to 4 and whose mother indicated that the child was in nursery school/preschool/Head Start, the child was coded as attended preschool (1). If the caregiver indicated the child was not in school at age 3 to 4, the child was coded as did not attend preschool (0).
We measured maternal warmth as the quality and quantity of emotional support provided by the mother in the home environment of children from birth to 10 years. The Home Observation for Measurement of the Environment (HOME; Caldwell, & Bradley, Reference Caldwell and Bradley1984) was used to obtain information through observations by a member of the research team. The maternal warmth subscale included seven questions (e.g., caregiver spontaneously praised child at least twice) for children less than 3 years and seven questions (e.g., caregiver caressed, kissed, or hugged child at least twice) for children aged 3 to 5 years and 11 months. Internal consistency ranged from .62 to .68 for all maternal warmth subscales across time points. Items were scored as yes (1) if present or no (0) if not present. Items were summed and then converted to z scores. Higher z scores indicate a higher level of maternal warmth. The earliest measurement of warmth was used.
Maternal responsiveness was measured by the Cognitive/Verbal Stimulation subscale in the shorter version of the Home Observation for Measurement of the Environment (HOME-SF; Caldwell, & Bradley, Reference Caldwell and Bradley1984), which assesses the quality and quantity of cognitive stimulation that children receive in the home environment from birth to 5 years. Specific caregiver behaviors or physical conditions in the home were reported by mothers and also observed by the researchers. The Cognitive/Verbal Stimulation subscale (9 items for 0–2 year olds, 14 items for 3–5 year olds) includes questions and observations about the physical environment (e.g., Is child’s play environment safe?) and presence of stimulating materials and activities for the child (e.g., How often do you read stories to child?). All items were coded as yes (1) and not present (0). Items were summed and then converted to z scores. Higher z scores indicate a higher level of cognitive/verbal stimulation. Cronbach’s alphas ranged from .71 to .74. The first reported score (i.e., earliest measurement) of maternal responsiveness was used.
We measured mothers’ perceived community environment with the Abridged Community Environment scale (Furstenberg et al., Reference Furstenberg, Cook, Eccles, Elder and Sameroff1999) used in the National Evaluation of Family Support programs. The scale consists of nine items that ask mothers about current problems in their neighborhoods and how their own neighborhood compares with others. All nine items were reverse-coded so that higher scores on this scale indicate higher perceived neighborhood safety. We conducted an exploratory factor analysis, using principal axis factoring with Varimax rotation, to assess the dimensionality of the community environment scale. Using the Kaiser-Guttman rule (initial eigenvalues >1: factor 1 = 4.35, factor 2 = 1.26) and scree-plot inspection, two factors were retained and rotated. All nine items demonstrated acceptable primary factor loadings ≥.40 (range: .51 to .80). Based on the factor analysis results, two subscales (subscale 1: current problems and safety issues in the neighborhood, subscale 2: relative neighborhood safety) were created and used in the analysis. Cronbach’s alphas were acceptable for both subscales (subscale 1: .84, subscale 2: .78).
Risk factors
Maternal depression was assessed by the presence of a major depressive episode in the past year using the Composite International Diagnostic Interview Short Form (CIDI-SF; Kessler & Üstün, Reference Kessler and Üstün2004). Having a major depressive episode was measured by three qualifying items (i.e., whether, in the past year, the caregiver has felt sad, blue, or depressed for at least half a day, almost every day, for a total duration of 2 or more weeks) followed by five symptom questions (i.e., weight change, trouble sleeping, difficulty concentrating, feelings of worthlessness, thoughts about death) based on the DSM-IV criteria for a major depressive episode (American Psychiatric Association, 2000). Responses were coded as having a major depressive episode in the past year (0) or not having a major depressive episode in the past year (1). Concordance with clinical diagnoses has been reported to range from .76 to .84 (Janca et al., Reference Janca, Robins, Bucholz, Early and Shayka1992).
Previous CPS involvement was reported by the CPS caseworker and coded as having a previous maltreatment investigation (1) or not having a previous maltreatment investigation (0). Substantiated maltreatment was reported by the CPS caseworker regarding the outcome of the most recent maltreatment investigation. Responses were coded as the case being substantiated (1) or the case not being substantiated (0).
Control variables
Child characteristics included the child’s gender and race as reported by the caregiver at Wave 1. Caregiver/family characteristics reported by the caregiver at Wave 1 included caregiver’s age, education, and family income. We coded caregiver education into two categories: less than high school diploma (0) or high school diploma or more (1). Family income reported by the caregiver at each wave was recoded to indicate yes (1) or no (0) as to whether the family income was below the federal poverty level at any time during the study.
Analysis approach
We used a two-stage approach to test hypotheses because of the complexities of fitting cohort-sequential growth mixture models (CS-GMM) and the importance of aligning with the life course perspective of prior studies of child and human development (Li et al., Reference Li, Duncan, Duncan and Hops2001; McDermott & Nagin, Reference McDermott and Nagin2001; Muthén et al., Reference Muthén, Khoo, Francis, Boscardin, Reise and Duan2003; Muthén, Reference Muthén, Collins and Sayer2001; Nagin & Land, Reference Nagin and Land1993; Nagin et al., Reference Nagin, Farrington and Moffitt1995). First, the CS-GMM (i.e., without IPV exposure and protective and risk covariates) was fitted to determine the number of distinct trajectory groups. As an extension of latent growth curve modeling, growth mixture modeling (GMM) allows for identification of subpopulations within a larger population to examine the mean trajectories, including and testing the effect of linear, quadratic, and cubic factors, and individual variation across and within the subpopulations (Gunzler et al., Reference Gunzler, Perzynski and Carle2021; Jung & Wickrama, Reference Jung and Wickrama2008; Muthén, & Muthén, Reference Muthén and Muthén2000; Ram & Grimm, Reference Ram and Grimm2009). CS-GMM advances current GMM analyses by allowing for cohorts of children based on developmental stage to be used to determine the distinct trajectory groups. Cohort-sequential methods have important advantages in longitudinal research, particularly in research involving children (Baer & Schmitz, Reference Baer and Schmitz2000; Gunzler et al., Reference Gunzler, Perzynski and Carle2021).
Although prior work has extended latent growth curve models to include a cohort-sequential component (Muthén, & Muthén, Reference Muthén and Muthén2000), this study is the first to extend the CS-GMM framework to child development of prosocial skills, in which trajectories are estimated as a latent categorical variable (Vanhalst et al., Reference Vanhalst, Goossens, Luyckx, Scholte and Engels2013). As in prior CS-GMM studies of mental health, substance use among adults and academic functioning of maltreated children, we implemented a model using the latent class growth analysis framework (Holmes et al., Reference Holmes, Yoon, Berg, Cage and Perzynski2017; Jung & Wickrama, Reference Jung and Wickrama2008; Nagin, Reference Nagin1999). The number of latent trajectories was determined by conducting analyses with between two and six trajectories and examining classification quality (entropy), model fit, parameter estimates and visualizations of the estimated group and individual values (Bayesian information criterion; BIC; Reinecke, Reference Reinecke2006). For the second stage, we conducted multinomial logistic regression to assess whether IPV exposure and protective factors significantly predicted the log odds of prosocial skills trajectory group membership. Guided by developmental psychopathology perspective (Sroufe & Rutter, Reference Sroufe and Rutter1984) that emphasizes that early experiences set the foundation for later development and that behavior develops through the ongoing interaction between children and their environment, we compared models that had a similar starting point at age 3 but then varied in trajectory. In order to gain a better understanding of what contributes to these differences, risk and protective factors were then examined to identify the extent to which each factor contributed to the differentiation of prosocial skills across these groups of children. The model included control variables, IPV exposure variables, risk factor, and protective factor variables. For all analyses, missing data were handled using listwise deletion.
Results
Sample demographics
Child participants ranged in age from birth to 5 years old, with a mean age of 1.7 years (SD = 1.72) at baseline. Trajectories for prosocial skills were estimated between the ages of 3 to 10 years old. Over half of the children (53.00%) were male, 53.72% were white, 32.28% were Black, and 19.03% were Hispanic/Latinx. Among caregivers, the mean age at baseline was 25.86 years old (SD = 6.52) and approximately half were white (51.80%). Nearly a third (61.30%) of caregivers received a high school diploma/GED or higher level of education, and 28.10% reported a major depressive episode within the past year. A majority of participants (77.40%) reported family income below the federal poverty line. Table 1 presents the study sample demographics and Table 2 presents bivariate results for study variables and prosocial skills.
Table 1. Sample demographics (N = 1,678)

Table 2. Bivariate results for study variables and prosocial skills
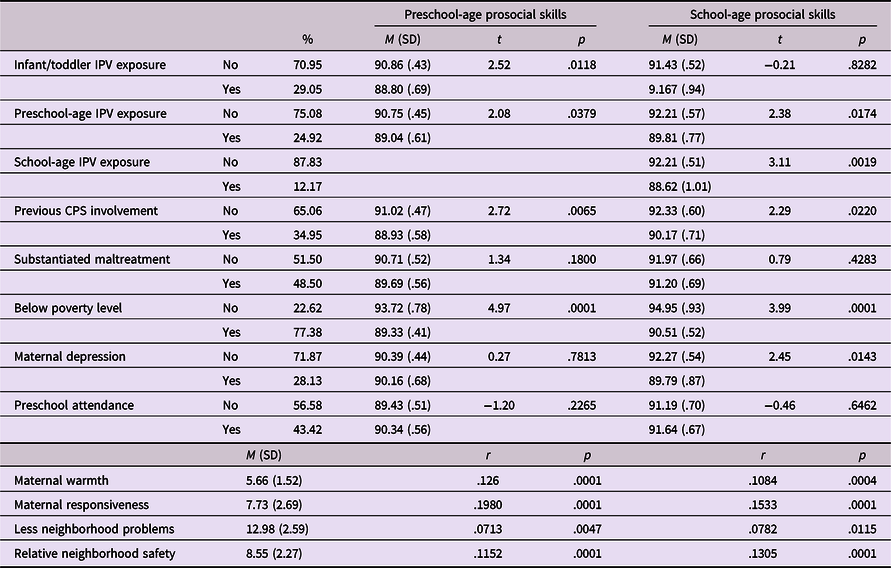
Note. Preschool age = 3 to 5 years old; school age = 6 to 10 years old; standardized scores were used for bivariate analyses of prosocial skills; raw scores were used for correlation of maternal warmth, maternal responsiveness, less neighborhood problems, and relative neighborhood safety.
Trajectories of prosocial skills
Table 3 displays the model fit comparisons for a number of prosocial skills trajectories. In the CS-GMM, entropy was greater than 0.70 for all of the models (Reinecke, Reference Reinecke2006). BIC decreased with each additional trajectory added. Although the BIC was lowest for the model with five trajectories, the addition of a fifth trajectory resulted in very small subgroup sample sizes (<5% of the total sample) and unstable solutions. Therefore, we concluded that the four-trajectory model was the optimal solution. Further analyses were based on the four-trajectory model.
Table 3. Model fit comparison for number of prosocial skills trajectories (N = 1,678)

The resulting four trajectories of prosocial skill development are shown in Figure 1. Notably, while a 5 trajectory model (see Table 3) showed improved BIC, the 5th estimated class in this model included out of range (negative) estimated parameter values, suggesting an inappropriate model solution. In addition, the shape and interpretation of the 4 classes from the 4 class model were nearly identically reproduced in the 5 class model except that the “increasing to decreasing” class separated into to nearly identical inverted-U trajectories shapes (as in Figure 1), with one of these simply shifted to the left slightly. Thus extracting trajectories beyond 4 is overfitting the underlying developmental processes in the sample (see Supplemental Table 1 for average latent class probabilities for most likely latent class).

Figure 1. Developmental trajectories of prosocial skills (N = 1,678).
Two identified groups had children who started with low prosocial skills but then diverged as the children aged. Of these, one group of children started low and remained low in prosocial skills over time (low stable group, 34.3%), and the other group of children started low but increased and then decreased in prosocial skills over time (low increasing-to-decreasing group, 15.6%). The other two groups included children who started with high prosocial skills but then diverged as they aged. One group of children started high and then subtly decreased in prosocial skills over time (high subtle-decreasing group, 33.1%) and the other group of children started high but decreased then increased in prosocial skills over time (high decreasing-to-increasing group, 17.0%). The four trajectories in the model each have a clear substantive interpretation and differ from the other classes.
Factors predicting trajectories of prosocial skills
Table 4 summarizes the results of the multinomial logistic regression analyses that examined IPV exposure timing and protective factors as focal predictors of membership in the prosocial skills trajectory groups. As a result of the natural grouping of trajectories during toddlerhood as displayed in Figure 1, the same multinomial logistic regression was run twice using a different reference group. The model was first run using the high subtle-decreasing group as the reference group. The high decreasing-to-increasing group was compared with the high subtle-decreasing group to examine the factors associated with children’s divergent paths of prosocial skills over time. The model was then run a second time using the low stable group as the reference group. The low increasing-to-decreasing group was compared with the low stable group to examine the factors associated with children’s improving then declining (versus consistently low) prosocial skills over time.
Table 4. Multinomial logistic regression results for variables predicting membership in prosocial skills trajectory groups

Note. OR = odds ratio. aNon-White is the reference group. bHigh School (HS) or less is the reference group.
High decreasing-to-increasing group compared with high subtle-decreasing group
Children with a prior history of CPS involvement had approximately 1.6 times higher odds of being in the high decreasing-to-increasing group, compared with the high subtle-decreasing group (OR: 1.58, 95% CI: 1.11−2.24, p = .012). Preschool-age IPV exposure and school-age IPV exposure also significantly predicted membership in the high decreasing-to-increasing group; children who were exposed to IPV during the preschool or school-age period had approximately 1.7 times higher odds of being in the high decreasing-to-increasing group, compared with the high subtle-decreasing group. Family income below the federal poverty level significantly increased the likelihood of membership in the high decreasing-to-increasing group, compared with the high subtle-decreasing group, while controlling for exposure to IPV and other confounders (OR: 1.79, 95% CI: 1.15−2.79, p = .010).
Low increasing-to-decreasing compared with low stable group
Children who had a mother with greater than high school education had 1.66 times higher odds of being in the low increasing-to-decreasing group, compared with the low stable group (OR: 1.66, 95% CI: 1.13−2.43, p = .010). Maternal responsiveness increased the odds of membership in the low increasing-to-decreasing group by 1.45 times, compared with the low stable group (OR: 1.45, 95% CI: 1.18−1.76, p < .001).
Discussion
This study examined the patterns (i.e., heterogeneity) of prosocial skill development in a sample of children reported to CPS for abuse or neglect, how IPV exposure may explain the variation in prosocial skill development, and the extent to which protective factors (i.e., preschool attendance, maternal warmth, maternal responsiveness, neighborhood safety) and risk factors (i.e., maternal depression, child maltreatment) contribute to variation in the development of prosocial skills.
Heterogeneity in prosocial skills
While person-centered approaches (Jung & Wickrama, Reference Jung and Wickrama2008; Muthén & Muthén, Reference Muthén and Muthén2000) are increasingly being used to examine prosocial skill development in general population research (Kokko et al., Reference Kokko, Tremblay, Lacourse, Nagin and Vitaro2006; Lamont & Van Horn, Reference Lamont and Van Horn2013), this study is the first to examine prosocial skill development in an at-risk sample starting in toddlerhood. Results of this study indicated that there is variation in the development of prosocial skills, as evidenced by our identification of distinct subgroups within a large sample of CPS-involved children. Similar to general population studies (Kokko et al., Reference Kokko, Tremblay, Lacourse, Nagin and Vitaro2006; Lamont & Van Horn, Reference Lamont and Van Horn2013; Takahashi et al., Reference Takahashi, Okada, Hoshino and Anme2015), we identified curvilinear paths that had increasing, decreasing, or stable periods of prosocial skill development. Specifically, four diverse pathways of development over time were identified. It is important to note that while four groups were identified, there were two distinct starting points for 3-year-olds. Approximately half of the sample started with high prosocial skills while the other half of the sample started with low prosocial skills. However, the two initial groupings diverged wherein some children experienced a curved developmental path and others either remained low or subtly decreased in prosocial skills over time. In order to gain a better understanding of what contributes to these differences, risk and protective factors were examined to identify the extent to which each factor contributed to the differentiation of prosocial skills across these groups of children.
Risk factors
IPV exposure and prior CPS involvement
IPV exposure was examined to determine whether certain time points of exposure during a child’s development were related to patterns of prosocial skill development. Results indicated that children who were exposed to IPV during the preschool- or school-age period had nearly two times higher odds of being in the high decreasing-to-increasing compared with the high subtle-decreasing group. Children with prior history of CPS involvement were also more likely to be in the high decreasing-to-increasing group compared with the high subtle-decreasing group. This means that while half of the children in the sample at age 3 were high functioning, about 34% of those children (16.9% of total sample) began to decrease in prosocial skills between the ages of 4 to 7 and then experienced an increase in prosocial skills between ages 8 to 10. While few previous studies have examined the effect of IPV exposure on prosocial skills, the results of the current study do align with past research; both Fantuzzo et al. (Reference Fantuzzo, DePaola, Lambert, Martino, Anderson and Sutton1991) and Howell et al. (Reference Howell, Graham-Bermann, Czyz and Lilly2010) found that children who had been exposed to IPV during the preschool years had significantly lower levels of prosocial skills compared with non-exposed children. Additionally, previous general population research has indicated that children have a curvilinear trajectory of prosocial skill development including periods of acceleration, deceleration, or stability over time (Kokko et al, Reference Kokko, Tremblay, Lacourse, Nagin and Vitaro2006; Lamont & Van Horn, Reference Lamont and Van Horn2013; Takahashi et al., Reference Takahashi, Okada, Hoshino and Anme2015).
Although limited research has examined the effects of co-occurring IPV exposure and prior CPS involvement on prosocial behavior in children, studies have indicated that children who experienced maltreatment during either the preschool-age (Bevilacqua et al., Reference Bevilacqua, Kelly, Heilmann, Priest and Lacey2021; Darwish et al., Reference Darwish, Esquivel, Houtz and Alfonso2001; Fantuzzo et al., Reference Fantuzzo, Weiss, Atkins, Meyers and Noone1998) or school-age years (Shonk & Cicchetti, Reference Shonk and Cicchetti2001) exhibit significantly fewer prosocial skills than children with no maltreatment history (see also Holosko, Reference Holosko2015). These findings corroborate the current finding that links prior CPS involvement to decreasing prosocial skills during preschool and early school years. In other words, those children in the current study who had a prior CPS case had at least two instances of alleged maltreatment. While it is unclear whether both of the cases were substantiated, it is possible that these children also experienced multiple developmental periods in which they were maltreated, aligning with the results of Jaffee and Maikovich-Fong’s (Reference Jaffee and Maikovich-Fong2011) longitudinal study finding that the greater number of developmental periods characterized by maltreatment, the poorer a child’s prosocial skills.
Trauma symptoms may be one possible explanation for the observed decrease in prosocial skills among children exposed to family violence. It is widely recognized that empathy (i.e., feeling as the other feels) and sympathy (i.e., feeling concern for the other) are major determinants of prosocial skills (Eisenberg & Miller, Reference Eisenberg and Miller1987; Yu et al., Reference Yu, Li and Zhao2020). However, young children who have been exposed to IPV may have difficulty empathizing and attending properly to social cues due to poor role modeling by caregivers, intrusive trauma symptom thoughts, and lower emotional regulation skills (Bender et al., Reference Bender, McKinney, Schmidt-Sane, Cage, Holmes, Berg, Salley, Bodell, Miller and Voith2022; Margolin, Reference Margolin2005; Rossman et al., Reference Rossman, Hughes and Rosenberg2000). This difficulty in empathizing and sympathizing, particularly during the preschool-age time period when such responses begin to develop, may explain the poorer prosocial skills in children who have been exposed to IPV.
During the preschool years, teachers tend to display more warmth to students and emphasize social development (Hatfield et al., Reference Hatfield, Burchinal, Pianta and Sideris2016; Ladd & Coleman, Reference Ladd and Coleman1997). However, starting in kindergarten and through the early school years, teachers emphasize cognitive development and may spend less time fostering social development. This shift in emphasis from social development to academic skills has been reported as one of the most challenging aspects of the preschool-to-kindergarten transition (Kiuru et al., Reference Kiuru, Aunola, Lerkkanen, Pakarinen, Poskiparta, Ahonen, Poikkeus and Nurmi2015; Ladd & Coleman, Reference Ladd and Coleman1997). For children exposed to IPV, this transition may be more difficult because of the additional demands placed on children to get along with their peers and perform academically once they enter kindergarten (Kiuru et al., Reference Kiuru, Aunola, Lerkkanen, Pakarinen, Poskiparta, Ahonen, Poikkeus and Nurmi2015).
Poverty
Results indicate that children who had family income below the federal poverty level had 1.8 times higher odds of being in the high decreasing-to-increasing group compared with the high decreasing group. Although prior research has not examined the specific interrelationships between IPV exposure, child poverty, and prosocial skills, findings from the present study regarding this initial decrease in prosocial skills do support previous research on the link between child poverty and social-emotional skills (Hosokawa & Katsura, Reference Hosokawa and Katsura2018; Lichter et al., Reference Lichter, Shanahan and Gardner2002; Webster-Stratton & Hammond, Reference Webster-Stratton and Hammond1998). Both cross-sectional and longitudinal studies have demonstrated that persistent child poverty increases a child’s risk of less social competence in preschool children (Hosokawa & Katsura, Reference Hosokawa and Katsura2018; Webster-Stratton & Hammond, Reference Webster-Stratton and Hammond1998) and exhibiting fewer prosocial behaviors in adolescence (Lichter et al., Reference Lichter, Shanahan and Gardner2002; Yao & Enright, Reference Yao and Enright2022).
Protective factors
Maternal responsiveness was a significant predictor of children being in either the high subtle-decreasing group or the low increasing-to-decreasing group. The results showed that children whose parents demonstrated responsiveness were 1.4 times more likely to be in the low increasing-to-decreasing group compared with the low stable group. This relationship between maternal responsiveness and child prosocial skill development is consistent with prior literature that underlines the significance of positive parenting in promoting healthy outcomes for IPV-exposed children (e.g., emotional regulation, prosocial skills; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021).
One possible explanation for these findings is that a positive, healthy attachment relationship with a caregiver is important for the development of prosocial skills (Levendosky et al., Reference Levendosky, Huth-Bocks, Shapiro and Semel2003; Silke et al., Reference Silke, Brady, Boylan and Dolan2018). The availability of a nurturing, supportive caregiver relationship, particularly in the early years, allows for a child to attend to important developmental tasks, including the capacity for emotional regulation and the promotion of social skills (Levendosky et al., Reference Levendosky, Huth-Bocks, Shapiro and Semel2003). However, IPV exposure may negatively affect this caregiver-child attachment relationship due to increased maternal depression and post-traumatic stress symptoms (Austin et al., Reference Austin, Shanahan, Barrios and Macy2019; Chiesa et al., Reference Chiesa, Kallechey, Harlaar, Ford, Garrido, Betts and Maguire2018). The findings in this study support earlier work suggesting that the prosocial skill development of IPV-exposed children may be indirectly bolstered by positive, attentive parenting practices (Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021).
As significant attachment figures, caregivers play an important role in modeling prosocial skills through their interactions with and behavior toward their children (Gross et al., Reference Gross, Stern, Brett and Cassidy2017; Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Levendosky et al., Reference Levendosky, Huth-Bocks, Shapiro and Semel2003). Caregivers who demonstrate higher levels of responsiveness may be more likely to offer encouragement for prosocial behavior and consistent discipline for problematic behaviors (Gross et al., Reference Gross, Stern, Brett and Cassidy2017). In addition, caregivers support children in developing the emotional regulation capacity necessary for healthy social interactions (Eisenberg et al., Reference Eisenberg, Spinrad and Eggum2010). For example, one study found that emotional coaching by parents (i.e., promoting a child’s emotion regulation skills) buffered the effects of IPV exposure on child adjustment outcomes (e.g., depression; Katz et al., Reference Katz, Gurtovenko, Maliken, Stettler, Kawamura and Fladeboe2020). This attentive parental feedback promotes a child’s emotional regulatory capacity and reinforces development of prosocial skills (Eisenberg et al., Reference Eisenberg, Spinrad and Eggum2010; Katz et al., Reference Katz, Gurtovenko, Maliken, Stettler, Kawamura and Fladeboe2020). Young children, in turn, may transfer these burgeoning understandings of emotional regulation and prosocial behavior to their interactions with peers and in relationships later in childhood (Caputi et al., Reference Caputi, Lecce, Pagnin and Banerjee2012; Levendosky et al., Reference Levendosky, Huth-Bocks, Shapiro and Semel2003).
Strengths and limitations
This secondary data analysis overcomes serious methodological limitations of prior cross-sectional and limited growth modeling approaches (e.g., those that assume a single trajectory that fits an entire population, or those that examine change by studying discrete waves as opposed to using a sequential cohort framework), by using CS-GMM. Although prior work has extended latent growth curve models to include a cohort-sequential component (Muthén & Muthén, Reference Muthén and Muthén2000), this study was among the first to extend this method to a GMM framework in which trajectories are estimated as a latent categorical variable (Hampson et al., Reference Hampson, Tildesley, Andrews, Barckley and Peterson2013; Holmes et al., Reference Holmes, Yoon, Berg, Cage and Perzynski2017; Vanhalst et al., Reference Vanhalst, Goossens, Luyckx, Scholte and Engels2013). This modeling approach extends previous studies that have been limited to using longitudinal data at data collection time points only (wave-by-wave models), which can bias results. Cohort-sequential methods have important advantages in longitudinal research by appropriately modeling child development, particularly in research involving children as tremendous growth and development occur as the child ages. This study also extends previous research on prosocial skill development by examining an at-risk sample of children. Finally, the current study fills a gap in current knowledge related to early prosocial skills by examining prosocial skill development starting at age 3. Examining younger children allowed for the identification of earlier patterns of adaptive or maladaptive development. Those divergent patterns were then explained by risk and protective factors. Examination of the potential for heterogeneity of those effects across the different trajectories is novel.
This study has several limitations. Namely, the sample consisted of CPS-involved children, making the results of this study not generalizable to the overall population. This study was also limited to maternal reports of IPV that included only physical assault. Other forms of IPV exposure, such as witnessing emotional abuse, may also have an important effect on children’s prosocial skill development, but these associations could not be tested. The majority of measures were reported by the mother, potentially biasing the results. Protective factors were estimated at baseline and could not be examined over time due to the already complicated models, and may have emerged as significant if measured at different developmental periods. This study only examined prosocial skills as a total percentile score and we are thus unable to evaluate whether there is important variation in specific subdomains over the course of development. Further work will be necessary to examine alternate measures, subdomains parameterizations of prosocial skills across developmental stages. Finally, the complexity of CS-GMM analyses and uncertainties about the underlying trajectory prevented the use of an informative a priori power simulation for this analysis. Similarly, power analyses for multinomial logistic models, even if conducted post hoc, require consideration of both events/distributions per variable and total sample size. While a post hoc power analysis is possible for the second stage regression analysis component of our approach, our sample size and the resulting events per variable are both considered large and adequate in the context of simulation studies and such an analysis is unlikely to alter the interpretation of our results (de Jong et al., Reference de Jong, Eijkemans, van Calster, Timmerman, Moons, Steyerberg and van Smeden2019), as in Table 4 where odds ratios are of moderate strength/effect size.
Research implications
This study identified the heterogeneity of prosocial skill development among children exposed to IPV. Findings illuminate areas for future research with children exposed to IPV, as prosocial skills are associated with self-regulatory capacities (e.g., emotional regulation, delayed gratification, frustration tolerance), which translate to other important functional domains (e.g., social relationships, behavioral management, cognitive functioning; Denham & Brown, Reference Denham and Brown2010; Flook et al., Reference Flook, Goldberg, Pinger and Davidson2015; Spinrad et al., Reference Spinrad, Eisenberg, Cumberland, Fabes, Valiente, Shepard, Reiser, Losoya and Guthrie2006). Multiple studies among general population and at-risk preschool-aged and elementary school-aged children have found that prosocial skills are associated with improved social relationships (Guo et al., Reference Guo, Zhou and Feng2018; Miller et al., Reference Miller, Gouley, Seifer, Dickstein and Shields2004; Shields et al., Reference Shields, Ryan and Cicchetti2001), school readiness (Fantuzzo et al., Reference Fantuzzo, Bulotsky-Shearer, Fusco and McWayne2005) and academic performance (Guo et al., Reference Guo, Zhou and Feng2018; Trentacosta & Izard, Reference Trentacosta and Izard2007). Future research should elucidate the mechanisms through which prosocial skills are associated with other domains of functioning in maltreated children, and whether children with low or decreasing prosocial skill developmental trajectories are also at risk for poorer functioning in other developmental domains.
This study examined the effects of risk and protective factors on prosocial skills development in children following trauma exposure. However, further research on how prosocial skills may also indirectly serve as a protective factor by bolstering functioning in other domains is warranted. In particular, prosocial skills may facilitate a child’s ability to access social support in the aftermath of trauma exposure (Bender et al., Reference Bender, McKinney, Schmidt-Sane, Cage, Holmes, Berg, Salley, Bodell, Miller and Voith2022). When children are able to have supportive social relationships with peers, siblings, and other family members, they may receive emotional encouragement and validation and/or tangible assistance or protection. This, in turn, may support a child’s ability to attend to their developmental tasks, promote resiliency, and improve outcomes over time (Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Lansford et al., Reference Lansford, Malone, Stevens, Dodge, Bates and Pettit2006).
Furthermore, this study’s methodological advancements have clear implications for future modeling of longitudinal data using a sequential cohort framework rather than estimating trajectories based on change across waves of data collection. Future research utilizing novel cohort-sequential data collection methodology, paired with a sophisticated analytical method (cohort-sequential growth mixture modeling analyses, CS-GMM) to identify patterns of adjustment over time, will allow for increased efficiency in examining longitudinal pathways. Specifically, future data collection anticipating the use of CS-GMM analyses can assess fewer participants at each developmental stage, thus maximizing efficiency and minimizing time and costs traditionally associated with longitudinal design.
Practice implications
The prosocial skill development trajectories observed in this sample offer important implications for clinical practice and program development. First, mental health assessments need to comprehensively address child exposure to violence and other forms of early adversity. Assessments must be constructed using a developmentally sensitive approach, examining the range of adversities experienced by children during each developmental period from the prenatal period to present (Perry, Reference Perry2009). Neural development and social interaction are deeply intertwined because early experiences occur in the context of the rapidly developing brain (van der Kolk, Reference van der Kolk2005). Research underscores the significance of the timing of violence exposure, as certain developmental windows may leave children more vulnerable to the negative sequelae of exposure to trauma (Graham-Bermann & Perkins, Reference Graham-Bermann and Perkins2010).
Assessments must also be responsive to the range of potential responses to trauma and adverse life experiences in children. Studies have demonstrated that children who exhibit more externalizing behaviors following IPV exposure may more likely be identified for intervention, while children with more internalizing behaviors often remain overlooked (Levendosky et al., Reference Levendosky, Bogat and Martinez-Torteya2013). Furthermore, some children may exhibit “sleeper effects,” or show more negative outcomes associated with trauma over time, rather than immediately following violence exposure (Holmes, Reference Holmes2013; Vu et al., Reference Vu, Jouriles, McDonald and Rosenfield2016). Briggs-Gowan et al. (Reference Briggs-Gowan, Ford, Fraleigh, McCarthy and Carter2010) found preschoolers’ exposure to violence and to non-interpersonal trauma to be significantly related, providing preliminary support that children living in families experiencing IPV may be more likely to experience other types of traumatic events. Caregiver and child psychoeducation can be provided through the assessment process as both a prevention mechanism and an initial intervention. Finally, assessments must also closely examine protective factors that promote resilience, such as maternal responsiveness and healthy caregiver-child attachment relationships. Each developmental period should be carefully assessed for the constellation of available protective factors (Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021; Perry, Reference Perry2009), offering important insight into potential points of intervention. Identifying and strengthening resources at the individual, family, and neighborhood level will support children in achieving adaptive outcomes (Howell et al., Reference Howell, Thurston, Hasselle, Decker and Jamison2021).
Because of the critical protective role of maternal responsiveness in promoting prosocial skill development, interventions for children that integrate parent training and support warrant further research and clinical application. An example of promising interventions are Pre Kids’ Club (PKC) and Kids’ Club (KC) which were designed for IPV-exposed children ages 4 to 6 years old and school-age, respectively (Graham-Bermann et al., Reference Graham-Bermann, Miller-Graff, Howell and Grogan-Kaylor2015). Through participation in these clinical programs, children work on developing skills related to emotional identification, emotional expression, and conflict resolution, while non-offending parents develop effective parenting practices and experience social support (Graham-Bermann et al., Reference Graham-Bermann, Lynch, Banyard, DeVoe and Halabu2007). Children from families receiving PKC or KC interventions have been found to exhibit reduced internalizing and externalizing symptoms, and decreased beliefs in the justifiability of violence over time compared with children in the control group (Graham-Bermann et al., Reference Graham-Bermann, Lynch, Banyard, DeVoe and Halabu2007, Reference Graham-Bermann, Miller-Graff, Howell and Grogan-Kaylor2015). Although studies have not explicitly examined outcomes related to prosocial skills, these interventions may promote the development of prosocial skills by fostering a child’s capacity for emotional identification/expression and conflict regulation and by cultivating maternal responsiveness.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579424000087.
Acknowledgements
This document includes data from the National Survey on Child and Adolescent Well-Being, which was developed under contract with the Administration on Children, Youth, and Families, U.S. Department of Health and Human Services (ACYF/DHHS). The data were provided by the National Data Archive on Child Abuse and Neglect.
Funding statement
Research reported in this publication was supported by The Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number R03HD078416-01A1.
Competing interests
The author(s) declare none.








 Open access
Open access