



Introduction
Spontaneous regression of cancer is a rare but well-documented phenomenon that occurs in various types of malignancies. It is estimated to have an incidence of up to 1 in 100 000 cases of cancer.Reference Jessy1 In the head and neck region, spontaneous regression has been observed in Merkel cell carcinoma, melanoma and lymphoma.Reference Connelly, Cribier, Brown and Yanguas2–Reference Buckner, Dunphy, Fedoriw, van Deventer, Foster and Richards4
Squamous cell carcinoma (SCC), which constitutes more than 90 per cent of all head and neck cancers, has also been observed to regress spontaneously.Reference Marur, D'Souza, Westra and Forastiere5 Head and neck SCC commonly arises from the epithelium of the larynx, pharynx, oral cavity, nasal cavity and paranasal sinuses. In the UK, the incidence of head and neck SCC is on the rise, but the survival rates have not been improving.Reference Hunter, Parkinson and Harrison6 Understanding the potential mechanisms of spontaneous regression could guide the development of future treatments. In this study, we performed a systematic review of case reports in spontaneous regression of head and neck SCC to investigate the pattern and characteristics of this phenomenon.
Methods
Study protocol
The review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.Reference Moher, Liberati, Tetzlaff and Altman7
Search strategies and information sources
A systematic search using search strategies comprising keywords and Medical Subject Headings was carried out in Ovid Embase, Ovid Medline and Pubmed from inception through to February 2023. Reference lists of relevant articles were also searched.
Eligibility criteria
Published case reports, case series, letters to the editor and correspondence that met the following criteria were included: (1) patients with a documented histological or radiological diagnosis of head and neck SCC; (2) the primary head and neck SCC was partially or completely regressed in the absence of any substantial treatment; (3) regression were microscopically or radiologically proven; and (4) English language articles with human subjects. We excluded any conference abstracts, review articles and case series in which the analysis was pooled without description of individual primary patient data. Reports that described spontaneous regression of cutaneous SCC of the head and neck region or where spontaneous regression only occurred in a metastatic lymph node, but not the primary cancer, were also excluded.
Study selection
Using the Rayyan systematic review program,Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid8 search strategies were implemented with results imported onto the online platform. After removal of duplicates, two authors (KLL and ZF) independently screened titles and abstracts. Articles that did not meet the inclusion criteria were removed. Full texts of the remaining articles were retrieved and again independently reviewed by two authors (KLL and ZF). Articles that met the inclusion criteria were included and any disagreements over study inclusion were resolved by consensus.
Data collection and analysis
Two authors (KLL and ZF) independently extracted data from included studies using a standardised template. Discrepancies were resolved by consensus. Data included country and year of publication, patient demographics, underlying co-morbidities, primary site of head and neck SCC, time to proven regression and follow-up duration. Potential events that could have contributed to spontaneous regression were noted, such as any documented febrile illness, recent vaccinations or any significant events of interest. Descriptive statistics were used to report patient demographics and clinical characteristics. Frequency and percentages were used to describe dichotomous variables.
Methodologic quality
To assess the quality of the included studies, two authors (KLL and ZF) independently appraised the study quality with a published standardised evaluation protocol and adapted it for this study.Reference Murad, Sultan, Haffar and Bazerbachi9 Elements assessed included ascertainment of diagnosis and regression, consideration of misdiagnosis, follow-up period and overall details of reporting.
Results
Study characteristics
A total of 505 references were identified, of which 162 references were duplicates and removed. The remaining 343 references were screened on title and abstract, of which 318 were irrelevant and removed. The remaining 25 references were reviewed in full and 17 were excluded, with reasons illustrated on the PRISMA flow diagram (Figure 1). A total of eight articles met the inclusion criteria and were included in the final study. These reports described eight individual patients from seven countries (Table 1). All reports had been published since 2004. Two cases were from the USA (2020, 2022), with one case each from Japan (2004), India (2018), Brazil (2014), New Zealand (2015), Lithuania (2017) and the UK (2022).

Figure 1. PRISMA flow diagram. SCC = squamous cell carcinoma
Table 1. Details of head and neck squamous cell carcinoma spontaneous regression case reports
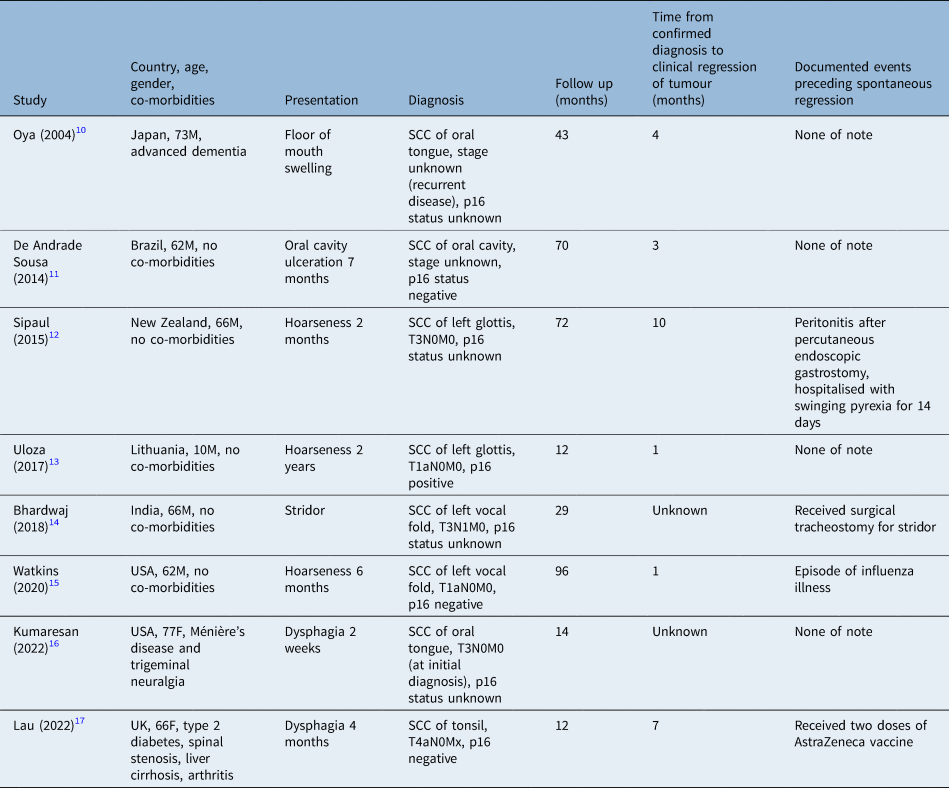
SCC = squamous cell carcinoma
Case characteristics of included studies
The median age of patients was 66 years (range, 10–77 years). Six patients were male and two were female. Hoarseness was the most common presenting symptom (n = 3) in the included reports. Other cases presented with stridor (n = 1), floor of mouth swelling (n = 1), oral cavity ulceration (n = 1) and dysphagia (n = 2). Five cases were fit and well with no significant past medical history. The primary sites of the SCC were recorded as vocal fold (n = 4), floor of mouth (n = 2), tongue (n = 1) and tonsil (n = 1).
Case 1 was a recurrent disease and the others were all first presentations of new malignancies. Two of the reports did not specify the clinical stage of disease at diagnosis and the other 6 cases were staged as T1N0M0 (n = 2), T3N0M0 (n = 2), T3N1M0 (n = 1) and T4aN0M0 (n = 1). Only one of the eight cases was p16 human papillomavirus (HPV)-positive while three cases were negative for p16 immunochemistry testing. The remainder four cases did not have a documented p16 HPV status.
Clinical course characteristics of included studies
Case 3 had a documented febrile illness prior to spontaneous regression of disease. This patient was admitted to hospital for prolonged septicaemia secondary to peritonitis after his percutaneous endoscopic gastrostomy insertion. He was noted to have a swinging fever for 14 days. Cases 6 and 8 had a possible febrile illness. Case 6 was diagnosed with influenza shortly after biopsy and treated with a course of oseltamivir. Case 8 received two coronavirus disease 2019 (Covid-19) AstraZeneca vaccinations at two and five months after diagnosis, with possible vaccination-related fever. Case 5 received surgical tracheostomy.
All cases received a surgical biopsy at presentation to obtain the initial diagnosis. No adjuvant chemotherapy or radiotherapy was administered in any included cases. Three cases received surgical resections where on subsequent histological examination the primary tumour was observed to have regressed. The mean length of time from diagnosis to proven regression was 4.3 months (range, 1–10 months).
Methodological quality
The diagnosis of head and neck SCC in all eight included reports was ascertained by histological examination (Table 2). Regression of tumour was proven by histological examination in five of eight cases, with three cases proven by radiological imaging. The possibility of misdiagnosis was considered in five of eight cases. The minimal follow-up time of the reports was 12 months (maximum, 96 months; mean, 43.5 months). All included studies reported no reoccurrence of disease at the time of publication. Cases 5 and 7 did not provide a reliable length of time between diagnoses to regression. In conclusion, seven of the eight studies were determined to have a low risk of bias and one was determined to have a moderate risk of bias.
Table 2. Methodological quality of included case reports

A total score out of 6 is given to each report: a score of 0 to 2 is regarded as high risk of bias, a score of 2.1 to 4 is regarded as moderate risk of bias and a score of 4.1 to 6 is regarded as low risk of bias
Discussion
The case report is often criticised for its heterogeneity, uncontrolled design and risk of bias. However, in rare cases where no higher-level evidence is available, case reports have proven to be a great resource for clinicians. Systematic review and meta-analysis of case reports has been performed in the literature to study uncontrolled and rare events such as emergency treatment for aortic dissectionReference Murad, Rizvi, Malgor, Carey, Alkatib and Erwin18 and, more recently, cardiac events after Covid-19 vaccines.Reference Fazlollahi, Zahmatyar, Noori, Nejadghaderi, Sullman and Shekarriz-Foumani19 The evidence inferred from these studies has proven useful in clinical decision making. In this study, we employed the same design to investigate the characteristics of head and neck SCC spontaneous regressions.
Incidences of head and neck squamous cell carcinoma spontaneous regression
Historic reviews have put the rate of spontaneous regression at between 1 in 80 000 and 1 in 100 000.Reference Jessy1 Reports of certain types of malignancies regressing are more common than for others, with 1 in 4003 in metastatic melanoma and up to 1 in 100 in metastatic clear cell renal carcinoma.Reference Buchler, Fiser, Benesova, Jirickova and Votrubova20 Other common forms of malignancies that have a higher spontaneous regression rate include leukaemia and lung cancer.Reference Radha and Lopus21 In contrast, only eight cases of head and neck SCC spontaneous regression were identified in this study. A possible explanation is that head and neck cancers have a lower incidence than the above cancers worldwide.Reference Sung, Ferlay, Siegel, Laversanne, Soerjomataram and Jemal22
Reports of spontaneous regressions of all malignancies have surged in recent years. A review performed in 2005 estimated 10 reports per year from 1987 to 2003, while a recent study revealed 89 cases were published in 2021 alone.Reference Hobohm23,Reference Žarković, Jaganjac, Žarković, Gęgotek and Skrzydlewska24 This can be explained by the shift towards evidence-based research in modern medicine, which has made clinicians aware of the importance of biomedical research and encouraged more peer-reviewed publications. Accordingly, a 9 per cent yearly increase in published scientific papers was observed over the past decade.Reference Landhuis25 This is consistent with our findings, where 7 out of 8 of the case reports of head and neck SCC spontaneous regression were published within the past 10 years.
Case characteristics: are subsets of head and neck squamous cell carcinoma more likely to regress than other subsets?
Epidemiological studies showed males are more likely to develop head and neck SCC in a ratio of 2:1 to 15:1, depending on the site of disease.Reference Mehanna, Paleri, West and Nutting26 The majority of the patients are also over 50 years old.Reference Gormley, Creaney, Schache, Ingarfield and Conway27 This is in keeping with our findings, where patients had a median age of 66 years and 6 out of 8 cases were males, reflecting that demographics are unlikely to be a factor in head and neck SCC spontaneous regression.
Head and neck SCC can present with a wide range of symptoms depending on the site of primary disease. Cancers arising from the larynx will usually present with hoarseness or stridor acutely, whereas cancers of the pharynx and oral cavity can present with dysphagia and/or oral ulcerations. Among the cases in this study, patients all presented with expected symptoms with respect to the function of the primary site of tumour. This shows that head and neck SCC which go on to regress spontaneously can often have a typical presentation.
Spontaneous regression has been documented to occur in both early and late stages of malignancies.Reference Papac28 Logically, an early-stage tumour should be more likely to regress. However, in some tumours, such as neuroblastoma, advanced stages of disease are known for their tendency to undergo spontaneous regression.Reference Brodeur29 A subset of late-stage neuroblastoma (stage 4S) has a low telomerase activity, and telomere shortening has been suggested to be an explanation for spontaneous regression in this subset of patients.Reference Hiyama, Hiyama, Yokoyama, Matsuura, Piatyszek and Shay30 This trend was not observed in any current studies in head and neck cancers. Amongst the head and neck SCCs that had been formally staged in this study, two were T1, three were T3 and one was T4, therefore our findings did not confirm that stage of head and neck SCC at diagnosis was associated with spontaneous regression.
Currently, HPV testing is performed for all new oropharyngeal cancers in the UK and USA as per the relevant guidelines.Reference Craig, Anderson, Schache, Moran, Graham and Currie31,Reference Lewis, Beadle, Bishop, Chernock, Colasacco and Lacchetti32 Routine testing for other head and neck cancer sites is not recommended. In our study, p16 immunohistochemistry was performed in two of four oropharyngeal SCCs and in two of four laryngeal SCCs. Only one spontaneously regressed laryngeal cancer was found to be HPV p16-positive. In cervical intraepithelial neoplasia, where HPV is known to be a risk factor, lesions associated with HPV16 are less likely to resolve spontaneously.Reference Trimble, Piantadosi, Gravitt, Ronnett, Pizer and Elko33 Whether the same is true in the head and neck requires larger-scale studies, and perhaps premalignant dysplastic lesions could be investigated as they have a spontaneous regression rate as high as 20 per cent.Reference Rastogi, Puri, Mishra, Arora, Kaur and Yadav34
The latest American Joint Committee on Cancer (eighth edition) guideline recommends that for metastatic p16-positive SCC in the upper jugular lymph nodes with unknown primary, staging of the disease should be on the assumption that the primary is in the oropharynx.Reference Lydiatt, Patel, O'Sullivan, Brandwein, Ridge and Migliacci35 While this represents a population of microscopic tumours not detectable by direct endoscopic visualisation or radiological imaging, some of these primary cancers could have spontaneously regressed after nodal spread. This sequence of events was observed in case 7, where the primary oral cavity SCC had spontaneously regressed but a level II node was revealed to be positive for SCC on neck dissection. The incidence of spontaneous regression is likely to be higher if a proportion of unknown primary cases was in fact spontaneously regressed head and neck SCC.
On the other hand, there are reports of head and neck SCC where only the nodal disease had spontaneously regressed.Reference Kurita, Hirano, Ebihara, Takushima, Harii and Fujino36,Reference Seo, Rooper, Seiwert and Fakhry37 In these cases, the primary tumour was still present when the cervical node metastasis had disappeared without substantial treatment. Interestingly, only the regressed lymph node had been biopsied prior to surgical resection; the primary tumours at the roof of the tongue and the inferior pole of the left tonsil in the two cases were diagnosed radiologically. This is in concordance with the current thinking that biopsy-related microtrauma to the tumour could incite an immune-modulated response.
Mechanism of spontaneous regression
Numerous mechanisms of spontaneous regression, such as epigenetics, hormonal changes and loss of telomerase activity, have been studied.Reference Bodey38 In the current literature, however, the prevailing view is that regression is modulated by a host immune response against the tumour.Reference Papac28 How this immune response is triggered remains a research area of great interest and some proposed mechanisms were demonstrated in our review.
• Eight individual patients from seven countries were reported to have a spontaneously regressed head and neck squamous cell carcinoma
• The sites of the primary were at the larynx and oral cavity, in various stages from T1 to T4, and only one case was p16 HPV positive
• Biopsy-related trauma and micro-disruption of tumour could induce an antitumour immune response, leading to spontaneous regression, and one case had a documented prolonged febrile illness as a precursor event
• Regional induced hyperthermia therapy could have a role in the treatment of head and neck cancers
• Spontaneous regression in head and neck SCC is rare but likely to be under-reported
• A better understanding of how the host immune system can instigate an antitumour response will shed light on developments of novel treatment modalities
Biopsy micro-trauma
Ablation of the primary tumour can induce regression in a distant tumour, which is termed an abscopal effect. The antitumour immune response in these cases is mediated by the upregulation of heat-shock proteins, neoantigens and cytotoxic T cells.Reference Ngwa, Irabor, Schoenfeld, Hesser, Demaria and Formenti39 This mechanism is thought to be shared by micro-disruption of a tumour in biopsies as well.Reference Lopez-Pastorini, Plönes, Brockmann, Ludwig, Beckers and Stoelben40 Operative trauma has been shown to be associated with subsequent regression of the tumour in large case series.Reference Cole41,Reference Challis and Stam42 However, these reviews were published in the last century and are largely outdated. It is difficult to determine if there is an association between spontaneous regressions and biopsy-related trauma. This is because in modern practice, suspicious lesions would almost always be biopsied in the first instance as part of the diagnostic work up. Similarly, in our review, all cases of head and neck SCC spontaneous regressions were preceded by biopsies and, in one case, partial resection of the tumour.
We should expect a much higher incidence of spontaneous regression if biopsy trauma could indeed trigger an antitumour immune response. Nowadays, treatments are always commenced expeditiously on a positive cancer diagnosis. Tumours which otherwise could have spontaneously regressed are promptly treated and the subsequent regression of disease will be attributed to the oncological treatments. In fact, six of eight cases in our review had either refused, delayed or been deemed unfit for treatment, thus allowing interval time for spontaneous regression to take place.
Febrile illness and hyperthermia
Cases of spontaneous regression are often preceded by a febrile illness.Reference Cann, Van Netten and Van Netten43 Sustained hyperthermia has been shown to inhibit tumour cell proliferation in in vitro studies.Reference Curley, Palalon, Sanders and Koshkina44 Cytotoxicity modulated by various compartments of the immune system such as CD8+ T cells, natural killer cells and MHC class ligands are all enhanced when heated at 39.5 to 45°C.Reference Gao, Zheng, Ren, Tang and Liang45 In fact, induced hyperthermia has been used as an adjunct therapy in a wide range of cancers.Reference Wust, Hildebrandt, Sreenivasa, Rau, Gellermann and Riess46 In our review, only case 3 had a documented prolonged febrile illness as a precursor event. Case 6 reported an episode of influenza but there was no mentioning of fever. Case 8 received two doses of AstraZeneca Covid-19 vaccinations, of which fever is a common side effect. Retrospectively, it is difficult to determine if these patients had any true febrile illnesses prior to tumour regression. Nonetheless, hyperthermia therapy has been adopted as standard treatment protocol in a number of centres internationally.Reference Chia, Ho, Tan, Chua and Tuan47 Randomised controlled trials have demonstrated that regional therapeutic hyperthermia, as an adjunct to chemoradiotherapy in the treatment of head and neck cancers, is associated with a higher complete response rate and longer disease-free survival.Reference Kang, Liu, Qin, Wei and Wang48,Reference Ren, Ju, Wu, Song, Ma and Ge49
Micro-organism and oral cavity microbiome
The role of micro-organisms in cancer therapy was first explored with Coley's toxin, where injection of heat-killed micro-organisms was used for the treatment of sarcomas. Modern treatment of urinary bladder cancer involves injection of Mycobacterium bovis directly into the bladder. The reason for the therapeutic effect is thought to be an increased expression of interleukins, interferons and tumour necrosis factors.Reference Kucerova and Cervinkova50 In our review, only one patient hospitalised with peritonitis had a definitive bacterial infection preceding regression of tumour. He also had a prolonged swinging fever, which in itself could have triggered an antitumour response, as discussed. How the microbiome exerts its effect on the head and neck tumour microenvironment is unclear, but it has emerged as an active research area in recent studies.Reference Hayes, Ahn, Fan, Peters, Ma and Yang51
Methodological quality
Case reports have variable levels of inferences and bias. It is imperative that the individual reports are appraised when conducting a systematic review. A major uncertainty concerning spontaneous regression of tumours is whether the lesion was malignant to begin with. In our review, all eight head and neck SCCs were confirmed by a histological diagnosis. A majority of these diagnoses were reviewed to confirm the initial diagnosis or considered for a possibility of misdiagnosis after spontaneous regression was observed. The quality appraising framework used in this study was adopted from a widely implemented instrument that considers four domains of a case report: selection, ascertainment, causality and reporting.Reference Murad, Sultan, Haffar and Bazerbachi9 The selection domain was excluded from our quality appraisal because the reporting of these cases will inherently not be representative of the whole experience of the centre. Cases of spontaneous regression are rare and could often be under-reported for reasons such as patients lost to follow up or uncertainties around this phenomenon.
Limitations
The quality of systematic review is contingent on the quality of evidence from the individual included studies. Case reports being retrospective in nature would mean some aspects of interest, such as the presence of febrile illness, were missing and susceptible to recall bias. The small case numbers also made data generalisation unreliable, but this is limited by the rarity of head and neck SCC spontaneous regression cases.
Conclusion
Management of head and neck cancer has drastically changed over the years, with the increased awareness of HPV-related head and neck SCC and the concurrent decreased incidence of tobacco-related cases. Spontaneous regression in head and neck SCC is rare but, as discussed, likely to be under-reported. We hope our review can facilitate the detection of similar cases. A better understanding of how the host immune system can instigate an antitumour response will shed light on developments of novel treatment modalities.
Acknowledgements
We would like to thank Mr Liam Flood for the invitation for a review article on such a fascinating topic and his contribution to our final manuscript.
Data availability statement
The data that support the findings of this study are available from the author KLL on reasonable request.
Competing interests
None declared



