



Introduction
People dealing with health problems in later life often experience difficulties performing daily chores independently and therefore require need-based care. Since the expansion of the welfare state, older people in many European countries have received instrumental support from formal elder-care systems (Kuhnle and Alestalo, Reference Kuhnle, Alestalo and Kuhnle2000). However, family members, especially adult children, have remained an important source of support (Künemund and Rein, Reference Künemund and Rein1999). Population ageing and rapidly growing expenses for subsidised residential care facilities have led to a tendency for keeping older people living in their own homes as long as possible (Lewinter, Reference Lewinter2004; Davies and James, Reference Davies and James2016). However, a lack of available care-givers might create an untenable arrangement as the risk of illness and disability increases (Tang and Lee, Reference Tang and Lee2011). As a result, older adults may choose to move closer to their family for support or opt to receive institutional care services (Litwak and Longino, Reference Litwak and Longino1987).
Previous studies have demonstrated that old age and deteriorating health are important predictors of residential adjustments and institutionalisation in different countries and cultural contexts (Wilmoth Reference Wilmoth2010; Golant, Reference Golant2011; Luppa et al., Reference Luppa, Riedel-Heller, Luck, Wiese, van den Bussche, Haller, Sauder, Mösch, Pentzek, Wollny, Eisele, Zimmermann, König, Maier, Bickel, Werle and Weyerer2012). Other factors that impact the likelihood of institutionalisation relate to family structure. These usually include living without a partner (with different levels of likelihood of institutionalisation for single, divorced and widowed older people), without a co-resident child (Grundy and Jitlal, Reference Grundy and Jitlal2007; Pimouguet et al., Reference Pimouguet, Rizzuto, Schön, Shakersain, Angleman, Lagergren, Fratiglioni and Xu2015) or not having children (Larsson and Silverstein, Reference Larsson and Silverstein2004). Indeed, living with a child can offer similar protection from institutionalisation as living with a partner (McCann et al., Reference McCann, Donnelly and O'Reilly2011), especially if the co-residing child is single/never-married (Grundy and Jitlal, Reference Grundy and Jitlal2007).
In addition to the impact of parent–child co-residence, living in close proximity to a child is associated with a lower likelihood of relocation, including institutionalisation, in old age (Van der Pers et al., Reference Van der Pers, Kibele and Mulder2015). However, we still know very little about whether and how adult children's characteristics are associated with relocation into residential care facilities in older adulthood. Therefore, we address the following research questions:
• How do older people's relocations into institutionalised care relate to adult children's gender, number and proximity?
• How do the effects of these children's characteristics on older parents’ institutionalisation vary by parents’ severe health problems (operationalised as closeness to death – specifically, dying within the two-year observation period)?
Importantly, throughout the article, we use the term ‘effect’ as a technical term to denote statistical associations, without necessarily implying causal relationships.
We make several contributions to existing research. First, in addition to institutionalisation, we distinguish between immobility and relocation elsewhere to account for the qualitatively different ageing experiences of stayers – whose needs in care are potentially met – from movers, who might be changing residence in search of sufficient care. Second, we account for distance to the geographically closest child plus the gender of the child and the total number of children to capture gendered responsibilities in caring for older parents. Third, because the role of children and the amount of support that they provide might be different when the health of a parent is still relatively good versus when it deteriorates critically (Knijn and Liefbroer, Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006), we examine how the effects of children's gender, number and proximity vary by parental severe health problems. Finally, we examine whether the results hold for older mothers and older fathers separately. We study these associations in the context of Sweden, a country well-known for its generous welfare system that aims to provide each citizen with the opportunity to live independently of family members.
We employed multinomial logistic regression models for older men and women based on the Swedish register data, containing the full old-age population. We controlled for known determinants of relocation to care institution or elsewhere, such as the presence of a co-residential partner, local ties of parents, socio-demographic characteristics and urbanicity. We additionally controlled for municipal differences in the availability of institutionalised and in-home care throughout the country.
Research background and hypotheses
Need for care and the relocations of older people
Older people often need support, especially those in the fourth age – a period marked by a diminished capacity for self-care and difficulties performing daily chores (Laslett, Reference Laslett1991; Baltes and Smith, Reference Baltes and Smith2003; Lloyd et al., Reference Lloyd, Calnan, Cameron, Seymour and Smith2014). Support can range from help with housekeeping or paperwork, which tends to be provided on occasion, when the provider has the opportunity, to regular physical care that addresses specific needs (Brandt et al., Reference Brandt, Haberkern and Szydlik2009). In this study, we focus on extensive care activities that are usually provided to a person with severe health problems in the later phase of life – care that requires close geographical proximity between the recipient and provider for adequate provision (Brandt et al., Reference Brandt, Haberkern and Szydlik2009). Since older people can receive care from formal and/or informal providers, it stands to reason that they make residential adjustments in order to capitalise on available, reliable care.
Theoretically, the link between the need for care and migration in old age can be understood by the later-life migration model of Litwak and Longino (Reference Litwak and Longino1987) and Cantor's hierarchical model of support (Cantor, Reference Cantor1979, Reference Cantor1991). In their model, Litwak and Longino (Reference Litwak and Longino1987) identify three stages of migration in older adulthood. In the first stage of the model, an amenity-seeking move is usually undertaken by a couple in good health closely after retirement. In the second stage, older people acquire chronic disabilities and move closer to available care-givers, traditionally represented by their adult children. In the third stage, when older adults’ health deteriorates, they are likely to move to institutionalised residential care. According to Cantor's model, the type of care an older individual receives is determined by (a) the preferences of the individual and (b) the availability of potential care-givers. Older people first prefer to receive assistance from their family members while formal care services are less attractive. Each source of assistance can function successfully when a more-preferred source is either not available or unable to meet the needs of the care recipient (Davey et al., Reference Davey, Levin, Iliffe and Kharicha2005).
In the context of these models, moving to an institution in old age can be seen as the last resort when a need for health-related care is high and informal assistance is unavailable, insufficient or otherwise unwanted. Moving elsewhere can be seen as a strategy to remain in the community by adjusting the housing to the increasing needs or/and moving closer to children if they do not live close enough. Empirical studies from different countries confirm that, although rare, older adults’ relocations (including relocations closer to family members and institutionalised care) tend to occur in response to deteriorating health, especially among the oldest old (Zimmerman et al., Reference Zimmerman, Jackson, Longino and Bradsher1993; Pope and Kang, Reference Pope and Kang2010; Wilmoth, Reference Wilmoth2010).
The role of adult children in care and relocations to institutions in old age
For older men and women, family members remain the essential source of care, which includes both practical and emotional support (Brody, Reference Brody1981; Lloyd et al., Reference Lloyd, Calnan, Cameron, Seymour and Smith2014). Besides spouses, children are usually the emotionally closest family members and are therefore more likely than other relatives to become care-givers for frail parents (Litwak, Reference Litwak1985), largely due to intergenerational solidarity that bonds parents and children (Rossi and Rossi, Reference Rossi and Rossi1990; Bengtson and Roberts, Reference Bengtson and Roberts1991). Moreover, because they are usually younger and in better health, adult children might provide more effective care-giving than siblings or other similar-age peers (Dykstra, Reference Dykstra2009). The care that children give to their parents might enable older people to continue living in their own homes. In this case, care must be extensive enough to serve as an alternative to institutionalisation.
Geographic proximity between parents and their adult children plays one of the main roles in determining the quality and intensity of intergenerational relationships and support exchange (Lawton et al., Reference Lawton, Silverstein and Bengtson1994; Hank, Reference Hank2007; Bordone, Reference Bordone2009). One exception is the exchange of financial support, which is not linked to the distance between a parent and a child (Knijn and Liefbroer, Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006). Because distance, contact and affection between older people and their adult children are interrelated (Lawton et al., Reference Lawton, Silverstein and Bengtson1994), proximity can also be seen as an intergenerational decision that may include affection and desire to be close to each other. Some parents and children might have moved closer to each other prior to our observation period in anticipation of increasing care needs. When care is needed, the closest child – who might be also the most affectionate one – is likely to intervene, in an effort to avoid institutionalisation when death is approaching (Johansson, Reference Johansson1991).
Having a co-resident child is associated with receiving the most amount of child-based care (Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008). Non-resident children living close by can be seen as a type of location-specific capital (DaVanzo, Reference DaVanzo1981). The closer children live to parents, the more care they provide (Ikkink et al., Reference Ikkink, Van Tilburg and Knipscheer1999; Kalmijn and Dykstra, Reference Kalmijn, Dykstra, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006). Geographically distant family members are often available only for short-term, episodic or emergency help (Dykstra and Knipscheer, Reference Dykstra, Knipscheer, Knipscheer, de Jong Gierveld, van Tilburg and Dykstra1995). This partly explains why having a primary care-giver living far away is linked to more unmet care needs (Beach and Schulz, Reference Beach and Schulz2017), potentially leading to institutionalisation (Johansson, Reference Johansson1991). Therefore, we expect:
• Hypothesis 1: Older people who have a child living nearby will be less likely to move to institutionalised care facilities than those whose closest child lives far away.
Several studies have shown that while women are more likely to provide personal care to family members, men take more responsibility for providing instrumental support (Rossi and Rossi, Reference Rossi and Rossi1990; Brandt et al., Reference Brandt, Haberkern and Szydlik2009). Compared with sons, daughters usually provide more care, in general, and more support with activities of daily living, in particular (Silverstein et al., Reference Silverstein, Gans and Yang2006; Haberkern et al., Reference Haberkern, Schmid and Szydlik2015). Furthermore, having at least one daughter reduces an older person's chances of institutionalised care admission, while there is no evidence that having living sons has a similar effect (Freedman, Reference Freedman1996). Therefore, we hypothesise:
• Hypothesis 2a: The effect of having nearby daughters on relocation into institutionalised care will be greater than the effect of having nearby sons.
The gender of the parent in need of care is another important component of family care-giving. The mother–child bond is strongest (Rossi and Rossi, Reference Rossi and Rossi1990) and women not only give more support across the lifecourse (Patterson and Margolis, Reference Patterson and Margolis2019) but also get more in return (Silverstein et al., Reference Silverstein, Gans and Yang2006; Grigoryeva, Reference Grigoryeva2017). Therefore, we additionally hypothesise:
• Hypothesis 2b: The effect of the proximity of children on the likelihood of relocation into institutionalised care will be stronger for mothers than for fathers.
Number of children might be associated with the likelihood of older parents’ institutionalisation. Most of the literature about the association between number of adult children and contact with or care received from these children focuses on contact with or care received from each individual child. Having more children is associated with a lower likelihood of receiving support from each child (Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008), presumably because of the diffusion of responsibility. From a child's perspective, the more siblings someone has, the less frequent the contact with a given parent (Dykstra and Knipscheer, Reference Dykstra, Knipscheer, Knipscheer, de Jong Gierveld, van Tilburg and Dykstra1995). Those with fewer siblings also have a higher likelihood of providing support to their older parents (Kalmijn and Dykstra, Reference Kalmijn, Dykstra, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006; Stuifbergen et al., Reference Stuifbergen, Van Delden and Dykstra2008).
Yet, even though being a parent of many children does not guarantee extensive and reliable care in later life (Gillespie and Treas, Reference Gillespie and Treas2019), the total amount of care received might be greater when the number of children is greater. Children from larger families are usually more family-oriented (Marini, Reference Marini1985). If family orientation is shared among siblings, those from large families might provide reliable support to their parent(s). Having many children increases the likelihood that at least one child will live geographically close to the parents (Holmlund et al., Reference Holmlund, Rainer and Siedler2013), and it might also increase the likelihood that at least one takes up the responsibility of caring or the care is shared among the children. It is also associated with a greater frequency of intergenerational face-to-face contact (Freedman, Reference Freedman1996). We therefore hypothesise:
• Hypothesis 3: An individual's number of children will be negatively associated with their likelihood of relocation into institutionalised care in old age.
Finally, the actual or perceived need for support is a clear prerequisite for more extensive care. The degree to which children take care of their parents is a function of the needs that parents have (Soldo et al., Reference Soldo, Wolf and Agree1990; Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008). Knijn and Liefbroer (Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006) found that parents’ health was an important condition for the provision of extensive care by their children. When parents’ health problems worsen, their children might respond by providing more care. Those children who live very close to parents have opportunities to fulfil these intentions, while those who live far might not be able to provide enough care to prevent parents’ institutionalisation, even if they are willing to do so. Accordingly, we hypothesise:
• Hypothesis 4a: The effect of having the closest child nearby (relative to having the closest child living far away) on the lower likelihood of institutionalisation will be greater for parents who have severe health problems than for those who do not.
Additionally, when parents’ health deteriorates, all children might increase the amount of support that they provide. We, therefore, hypothesise:
• Hypothesis 4b: The relationship between the number of children and the likelihood of institutionalisation will be greater for parents who have severe health problems than for those who do not.
Other factors related to institutionalisation and other residential relocations
Studies demonstrate that older people with a spouse at home are less likely to utilise social services (Greene and Monahan, Reference Greene and Monahan1987; Larsson and Thorslund, Reference Larsson and Thorslund2002) or move to specialised residential care or elsewhere (Van der Pers et al., Reference Van der Pers, Kibele and Mulder2015). Single adult children provide more support to their parents than partnered children and younger children provide more than older ones (Knijn and Liefbroer, Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006).
Resources influence the quality and amount of support exchange (Knijn and Liefbroer, Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006). For example, as an alternative to institutionalisation, families from higher-income groups can draw on their financial resources to subsidise in-home care for older family members with deteriorating health. At the same time, they are perhaps better able to pay for residential care services than those from low-income families. In line with this logic, parents with lower levels of education are more likely to move very close to a child (Pettersson and Malmberg, Reference Pettersson and Malmberg2009). They also receive more support from their children than higher-educated parents (Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008), who might be more likely to use social and cultural resources for organising available services and to avoid institutionalisation (Larsson et al., Reference Larsson, Thorslund and Kåreholt2006).
For older adults with deteriorating health, the dwelling unit becomes more important, as they tend to spend more time inside (Hill et al., Reference Hill, Sutton and Cox2009). Those living in large dwellings might be more inclined to move to smaller dwellings that are more manageable (Abramsson and Andersson, Reference Abramsson and Andersson2016). Duration of residence as a form of local ties might also affect the likelihood of changing the place of residence. Those with longer residential durations are less likely to move away (Sommers and Rowell, Reference Sommers and Rowell1992). Immigrant parents are also more likely than native parents to migrate towards their children or have them migrating into co-residence (Thomas and Dommermuth, Reference Thomas and Dommermuth2020).
The degree of urbanisation of the parent's place of residence is likely associated with relocation in older age. In rural settings, the access to care services is not as great as in metropolitan areas. To compensate for this, nearby kin networks tend to provide more care in rural areas (Hogerbrugge and Dykstra, Reference Hogerbrugge and Dykstra2009).
Intergenerational care in the context of Sweden
In addition to the individual characteristics of older parents and adult children, intergenerational care-giving might be influenced by contextual factors. The availability of care services funded by the state, the legal obligation to support relatives in need, and opinions about whether the state or family members should be responsible for the care of older people are examples of contextual factors that have been found to explain differences in patterns of family care-giving in European countries (Haberkern and Szydlik, Reference Haberkern and Szydlik2010). Formal in-home and residential care alternatives to family care, minor legal obligations to provide care and low social expectations for children to be the main providers of care enable children in northern Europe – and daughters, in particular – to choose the extent of involvement in the care of their older parents (Haberkern and Szydlik, Reference Haberkern and Szydlik2010).
In light of these insights, the Swedish context provides an interesting test case for exploring the relationship between adult children's gender, number and proximity, and institutionalisation of very old parents. Swedish public services have been both affordable for the poor and attractive enough for older adults with enough resources for private care (Szebehely and Trydegård, Reference Szebehely and Trydegård2012). These services are a carryover from the ‘golden days’ of the Swedish elderly care system, when the state promoted universalism and a de-familisation of care provision. This system was designed to make every older person independent from their relatives.
Between 1950 and 1975, both in-home help services and institutional care grew rapidly. In the 1970s, Swedish elder-care experienced its greatest expansion on all fronts (Ulmanen and Szebehely, Reference Ulmanen and Szebehely2015). By 1975, about 70 per cent of those aged 80 and older – regardless of their financial situation – received support from in-home or institutional care providers (Johansson et al., Reference Johansson, Sundström and Hassing2003). In 1992, budgetary reductions due to weakening economic growth and the growing elderly population resulted in a dramatic restructuring of the long-term care system. This Elderly Reform (Ädelreformen) transferred the responsibility for providing older people with the public services to the municipalities (Johansson, Reference Johansson1997). The municipalities concentrated their resources on the frailest older people, especially those living alone (Bergmark et al., Reference Bergmark, Parker and Thorslund2000), while persons with fewer needs, younger seniors and the married often had to turn to family, friends or subsidised domestic services from the private market (Larsson et al., Reference Larsson, Thorslund and Kåreholt2006).
Even though assisting older parents was not mandatory, families felt social obligations to take responsibility for older family members by providing support or paying for extra services (Johansson et al., Reference Johansson, Sundström and Hassing2003; Szebehely and Trydegård, Reference Szebehely and Trydegård2012). As a result, the proportion of children helping their parents almost doubled during the 1990s. This trend was most pronounced among older people whose children lived nearby (Johansson et al., Reference Johansson, Sundström and Hassing2003). In fact, during these years, some municipalities even started to factor the availability of informal help in older adults’ needs assessments (Bergmark et al., Reference Bergmark, Parker and Thorslund2000). Between 2002 and 2010, the percentage of older people who received informal help – primarily from adult children – increased from 48 to 63 (Ulmanen and Szebehely, Reference Ulmanen and Szebehely2015).
Given all contextual factors, the effects of adult children's characteristics on older parents’ relocations to care institutions might be relatively modest in Sweden. However, variation between municipalities in terms of the share of older people already receiving in-home or institutionalised care might be an important source of heterogeneity worth consideration.
Data and method
Dataset
We use Swedish register data containing anonymised information about all residents of Sweden. The Population register includes such key demographic information as date of birth, sex and country of birth. Family members are linked to each other by the Multigenerational register. Annually updated socio-economic information were derived from LISA (a longitudinal integration database for health insurance and labour market studies). In total, about 2 per cent of the residents of Sweden are not registered in any dwelling in a given year (Statistics Sweden, 2014). These unregistered individuals were excluded from our analyses.
For each registered individual, we also know the SAMS area (Small Area Marketing Statistics) of residence. SAMS divisions are based on the subdivision of areas in large municipalities and on election districts in small municipalities. There are approximately 9,200 of these small areas throughout the country. SAMS codes contain municipal codes as well as identifiers within the municipalities. By adding geographical mid-point co-ordinates to the SAMS areas, we calculated Euclidean distances between non-resident family members. We also linked municipal-level information about shares of people at the age of 80 years and over receiving in-home and institutionalised care in the municipality of a parent, derived from an open-access official statistics database for elder-care (National Board of Health and Welfare, 2019).
These data enabled us to trace older people's residential locations between 2014 and 2016. The data for 2017 were used exclusively to control for the older parent's closeness to death. We observe older people across two pooled time periods: 2014 (t −1) – 2015 (t) – 2016 (t + 1); 2015 (t −1) – 2016 (t) – 2017 (t + 1). At t −1 we measured baseline characteristics of the study population. At t we tested if parents moved and t + 1 marked individuals’ closeness to death, which served as a proxy for severe health problems, at t −1. Observations were treated as censored after the first observation period if a move to a residential care institution occurred in that period.
The population at risk was represented by non-institutionalised men and women aged 80 years and older. Individuals without children and those whose children lived outside Sweden were excluded from the study. The total number of biological and/or adopted children ranged from one to 16. In total, 696,007 person-years were included in the analysis, of which 426,078 person-years (61.2%) were women.
Variables
The outcome variable ‘residential relocation’ distinguishes between three outcomes: not moving (reference category), moving to institutionalised residential care and relocation elsewhere. Individuals were considered non-movers if, according to the Internal Migration register, they did not move between t −1 and t; the dataset included 636,040 of such observations (91.4% of the total number of person-years). If the person relocated and the code of the new accommodation identified living in a specialised institution, the person was considered to have relocated to residential care (29,295 moves or 4.2% of the total number of person-years), while relocation from one ordinary dwelling to another ordinary dwelling was classified as moving elsewhere (30,672 moves or 4.4% of the total number of person-years).
The primary explanatory variables were ‘gender and distance to the closest child’ and ‘number of children’. The variable ‘gender and distance to the closest child’ differentiated between: (a) having the closest child of any gender in the same dwelling, (b) closest child is a son in the same neighbourhood, (c) closest child is a daughter in the same neighbourhood, (d) closet child is a son within 20 kilometres (km) of the parent's neighbourhood, (e) closest child is a daughter within 20 km of the neighbourhood, (f) closest children are a son and a daughter at the same distance that is less than 20 km (including those living in the neighbourhood), and (e) closest child lives further than 20 km away (reference category). We did not distinguish co-resident daughters versus sons because the categories were too small to yield meaningful analyses. We categorised the number of children into three groups: one child, two children (reference category) and three or more children.
In the absence of other health measures for this research, ‘closeness to death’ served as a proxy for severe health problems (Van der Pers et al., Reference Van der Pers, Kibele and Mulder2015) for revealing how the effects of children's characteristics on older parents’ relocations vary by parents’ health-related need for care. We use information on the parent's year of death to construct a dichotomous variable indicating whether the person died within the two-year period (1) or not (0, reference category). Although studies have shown that poor health is frequently mentioned as a reason for moving in later life (Choi, Reference Choi1996) and relocation does not bring increases in mortality in old age (Borup et al., Reference Borup, Gallego and Heffernan1979), reverse causality still could be an issue. Moving, especially to institutionalised care facilities, might be either a cause or an outcome of an individual's closeness to death.
We controlled for the parent's and closest child's age, partner in the parent's and closest child's households (reference category: living with a partner), financial resources included the older person's pension (reference category: pension below median) and whether at least one child has a high disposable income (reference category: all children with the income below median). We accounted for the financial resources of at least one child rather than the income of the closest child because financial support proved to be independent of geographical proximity between parents and adult children (Knijn and Liefbroer, Reference Knijn, Liefbroer, Dykstra, Kalmijn, Knijn, Komter, Liefbroer and Mulder2006). Disposable income (in 100,000s of Swedish crowns which was approximately €10,840 on 30 June 2015 – the middle of the observation window) was calculated by Statistics Sweden; the few registered negative incomes were recoded to 0. Other control variables included two socio-demographic characteristics of parents: ‘educational attainment’ with four categories: primary (reference category), secondary, post-secondary and no information; and ‘country of origin’ with two categories: born within or outside Sweden (reference group); and two measures of parent's local ties: ‘duration of residence’ (in years) and ‘dwelling size’ based on the median division of the dwelling area in square metres (m2) in houses and number of rooms in the apartments: a smaller-size dwelling (less than 90 m2 or up to three rooms) and a bigger dwelling (90+ m2 or four and more rooms).
Local-level controls included the ‘degree of urbanisation’ (using Eurostat's definition of the level of urbanisation), which distinguished between metropolitan areas, smaller towns or suburbs, and sparsely populated areas, and the ‘coverage of welfare system services’. The latter variable is based the share of older people at the age of 80 years and older who received (a) in-home care or (b) residential care in the municipality. The variable distinguishes between municipalities with (a) below median share of both in-home and institutionalised care coverage, (b) below median share of in-home care and above median share of institutionalised care coverage, (c) above median share of in-home care and below median share of institutionalised care coverage, (d) above median share of both in-home and institutionalised care coverage, or (e) no available information.
Summary statistics for all variables and distribution of the dependent variable across the categories of the nominal independent variables are presented in Table 1.
Table 1. Summary statistics
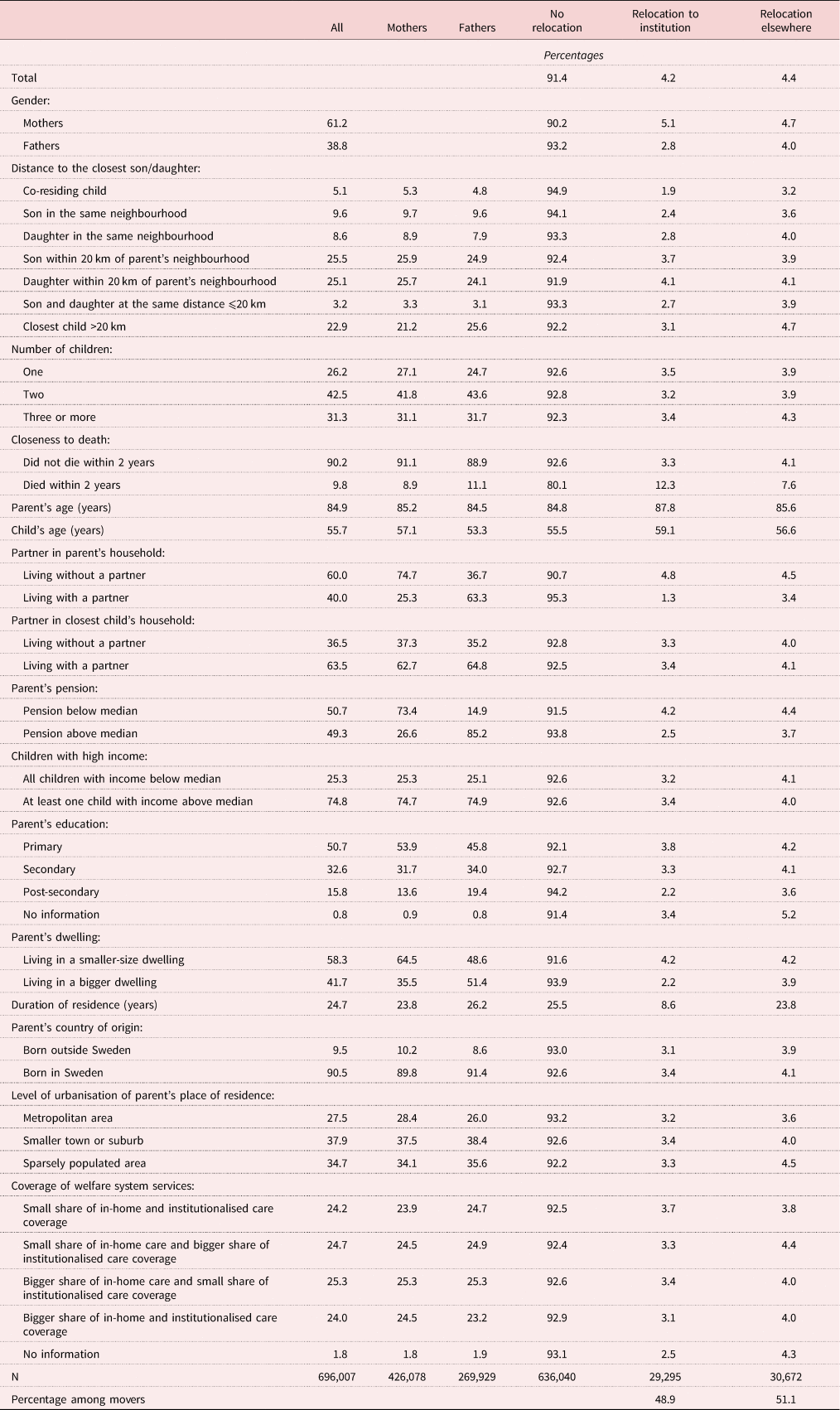
Note: km: kilometres.
Source: Swedish register data, authors’ calculations.
Analytical strategy
We employed multinomial logistic regression models, which estimated the effects of the explanatory and control variables separately for older men and women. We stratified the sample by gender to avoid double counting and correlated outcomes between partners. To account for clustering at the parent and local levels, we used two-way clustered standard errors (Cameron et al., Reference Cameron, Gelbach and Miller2011). The standard errors were adjusted for 239,025 unique clusters of women (153,461 unique clusters of men) and 290 clusters of municipalities.
In the first step, we estimated models with main effects for key explanatory variables and control variables. To compare mothers and fathers, we ran a pooled model with an interaction term between the gender of the parent and the gender plus proximity of the closest child; the model also included all controls in the main analysis. In the second step, we tested interactions between the number of children, gender and proximity of the closest child, and closeness to death. In addition to our primary findings, we also discuss the results of sensitivity and auxiliary analyses below.
Results
Descriptive findings
As shown in Table 1, on average, over 8 per cent (in person-years, 9.8% of women and 6.8% of men) relocated between 2014 and 2016. Among them, 48.9 per cent moved to an institution and 51.1 per cent relocated to another non-specialised dwelling.
As expected, co-residence with a child was relatively rare in Sweden, although 77.1 per cent of parents (78.8% of mothers and 74.4% of fathers) had the closest child within 20 km of the neighbourhood. Those who co-resided with a child or had a child living in the same neighbourhood stayed at the baseline dwelling more often than those whose closest child lived within 20 km of the neighbourhood (94.9, 93.7 and 92.2%, respectively). Those with a daughter living in the same neighbourhood moved to an institution and elsewhere somewhat more often than those who had a son living nearby (2.8 versus 2.4% to an institution and 4.0 versus 3.6% elsewhere). The same child's gender-related trend was observed for having a son or a daughter within 20 km of the neighbourhood as the closest child. For those having the closest child further than 20 km of the neighbourhood, institutionalisation was less common than for those who had the closest child of any gender within 20 km.
The majority of older people had two children. Those who had one, two, or three or more children remained in the same dwelling almost equally often.
Multinomial regression analysis of residential relocation in old age
Table 2 presents the multinomial logistic regression results separately for women and men.
Table 2. Multinomial logistic regression of relocation in old age1
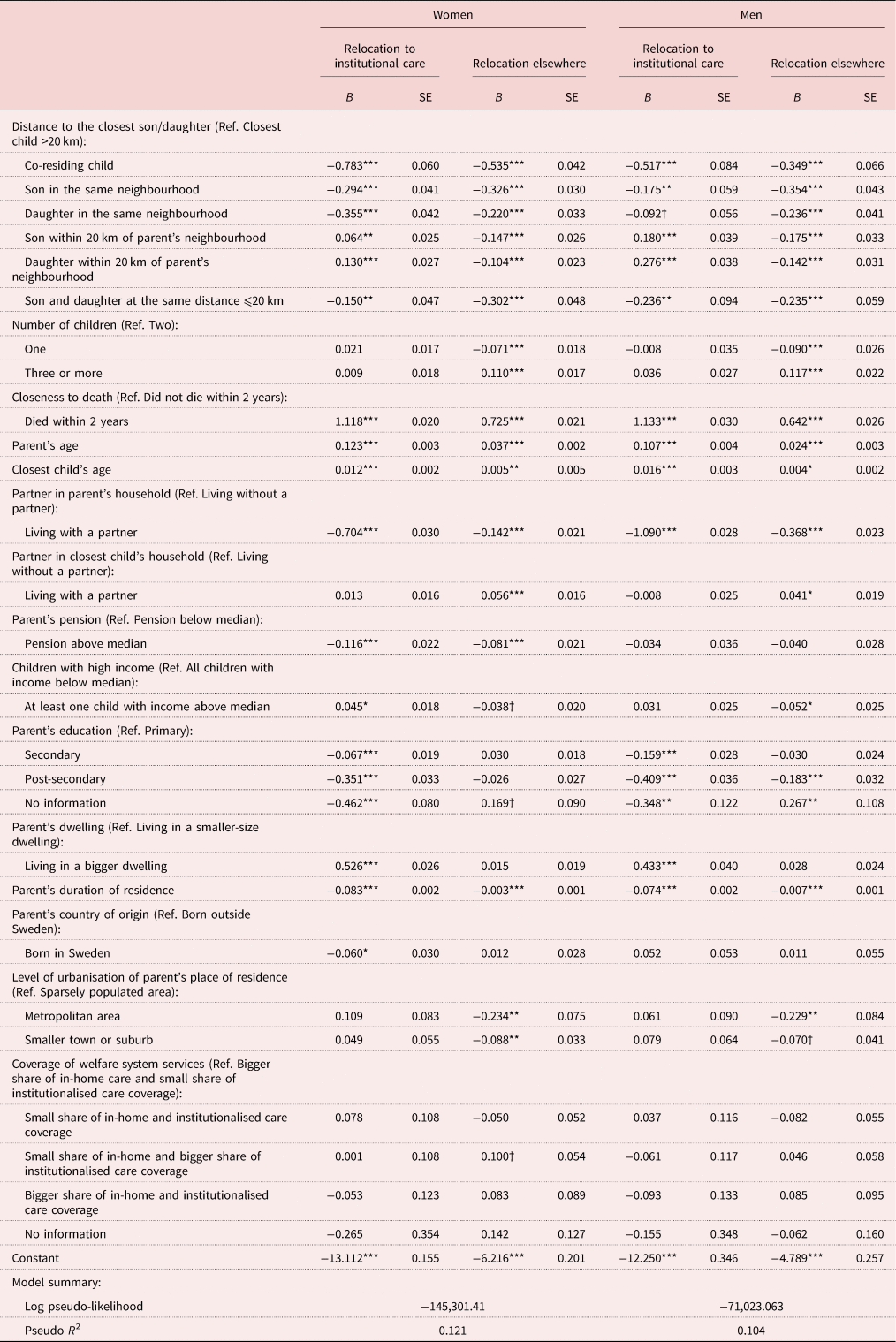
Notes: 1. Reference category (Ref.): no relocation. SE: standard error. km: kilometres.
Source: Swedish register data, authors’ calculations.
Significance levels: † p < 0.10, * p < 0.05, ** p < 0.01, *** p < 0.001.
Figure 1 presents the predicted probabilities and their 95 per cent confidence intervals of the relocation outcomes according to different categories of closest child's gender and proximity. In support of Hypothesis 1, the probabilities of moving to institutionalised care were significantly lower when the older mothers and fathers were living in the same household (0.027 for mothers and 0.016 for fathers) or the same neighbourhood (0.040 and 0.023, respectively) with adult children compared to when they lived very far from their children (0.052 and 0.025, respectively). Women and men who had the closest child within 20 km of the neighbourhood were more likely to be institutionalised than those having the closest child more than 20 km away. These statistically significant results are in line with findings from the Netherlands (Van der Pers et al., Reference Van der Pers, Kibele and Mulder2015). Considering that adult children might continue to provide support after their parents relocate to specialised care facilities (Montgomery and Hirshorn, Reference Montgomery and Hirshorn1991), one possible explanation is that older people might be more inclined to move to a nearby institution if they have a child in a relatively short distance who can visit them in institutionalised care. Another explanation might be that the children moved closer to their parent at an earlier occasion.
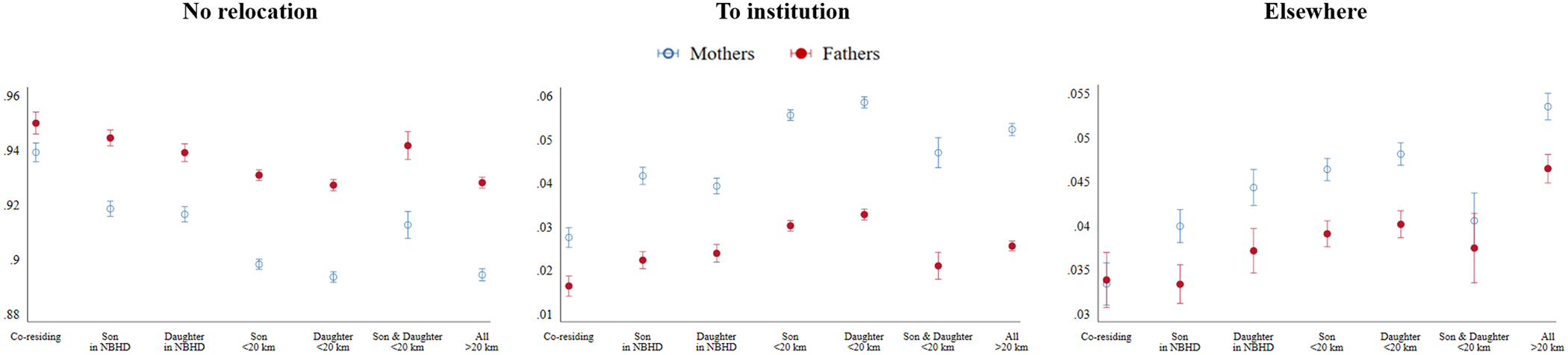
Figure 1. Predicted probability of proximity and gender of the closest child.
Notes: Estimates and 95 per cent confidence intervals are shown. NBHD: neighbourhood. km: kilometres.
However, if children live far away, parents might be more likely to relocate elsewhere instead (potentially closer to a child). The probabilities of moving elsewhere increased consistently with longer distances to the closest child. The values were lowest (0.033 for mothers and 0.034 for fathers) when the closest child was living in the same household and highest (0.054 for mothers and 0.046 for fathers) when the closest child lived more than 20 km away. Additional analyses (Table 3) indicated that when older people moved elsewhere, the most common moving distance was within 20 km of the neighbourhood (64% of all relocations elsewhere for mothers and 62% for fathers), followed by within the same neighbourhood (23% for both mothers and fathers) and further than 20 km (13 and 15%, respectively). The predicted probabilities for relocation by distance were highest when the closest child lived at the same distance, suggesting moves towards their closest children. All reported differences in predicted probabilities were statistically significant at the 0.05 level at least.
Table 3. Predicted probability of proximity and gender of the closest child (relocations and moving distances)
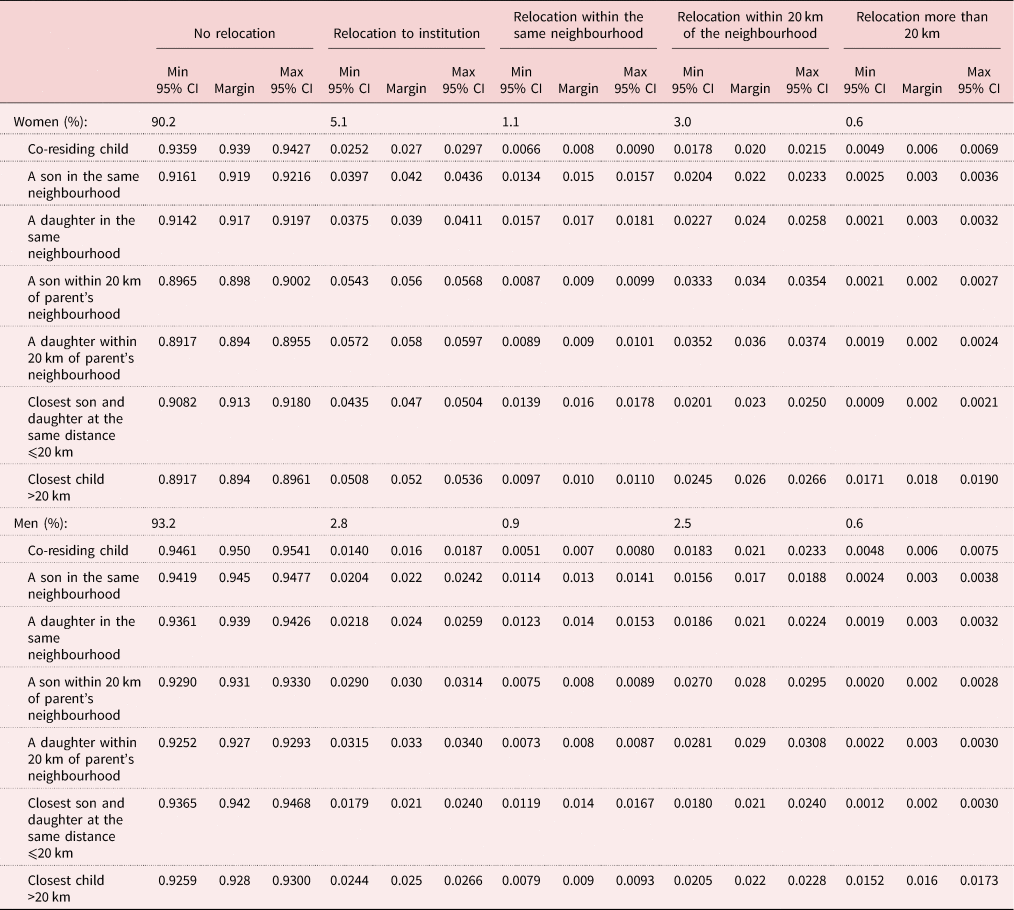
Notes: For the additional analysis, the category ‘relocation elsewhere’ was specified to distinguish between relocation (a) within the neighbourhood, (b) 20 kilometres (km) of the neighbourhood, and (c) more than 20 km. Then two multinomial logistic regression models with the same control variables as in the main models were performed and the predicted probabilities for all outcomes were calculated. Min: minimum. Max: maximum. CI: confidence intervals.
Source: Swedish register data, authors’ calculations.
Hypothesis 2a stated that the effect of having a nearby daughter would be greater than the effect of having a nearby son. Our results did not show support for this hypothesis. For older mothers, the predicted probability of relocation within the neighbourhood was significantly higher when they had a daughter in the same neighbourhood (0.017) than when they had a son there (0.015). For relocations within 20 km, the child's gender differences were found neither for mothers nor fathers.
In line with Hypothesis 2b, the effect of a co-resident child on the probability of institutionalisation was larger for older mothers than fathers. The probability of institutionalisation was, on average, 2.5 percentage points lower for those mothers who had a co-residing child (average marginal effect (AME) = −0.025, p < 0.001) relative to those mothers whose closest child lived more than 20 km away. For older fathers, this difference was 0.9 percentage points (AME = −0.009, p < 0.001). Likewise, the effect of having an adult child in the same neighbourhood on the lower likelihood of institutionalisation was stronger for older women (AME = −0.010 for sons and −0.013 for daughters, p < 0.001) than men (AME = −0.003, p < 0.01 for sons and −0.002, p = 0.16 for daughters). In further support of Hypothesis 2b, the pooled model with an interaction term between the gender of the parent and the gender plus proximity of the closest child (results not shown) had a higher value of model-fit than the pooled model without this interaction (likelihood-ratio (LR) χ2 (12) = 42.18; Prob > χ2 = 0.000). The interaction term indicated that mothers were indeed more affected by the proximity to an adult child than fathers.
Gender and proximity of the closest child seemed to be more important in preventing moves to residential care than number of children. We found no evidence of a relationship between the number of children and likelihood of institutionalisation (Hypothesis 3). Nonetheless, older mothers and fathers were more likely to relocate elsewhere when they had three or more children (B = 0.110 and B = 0.117, respectively) and less likely to do so when having only one child (B = −0.071 and B = −0.090, respectively); all coefficients were statistically significant (p < 0.001).
In general, severe health problems were associated with a higher propensity of relocation (all coefficients were positive and statistically significant, p < 0.001). The effects were greater for moving to institutionalised care (for mothers: B = 1.118; for fathers: B = 1.133) than elsewhere (for mothers: B = 0.725; for fathers: B = 0.624). The second set of models (Tables 4 and 5) test Hypotheses 4a and 4b. The interaction term between severe health problems and the gender plus proximity of the closest child improved the models’ goodness-of-fit for mothers only, not fathers. The findings did not provide support for the Hypothesis 4b that the impact of number of children on relocations to institutions would vary by the parents’ severe health problems. The interaction term in Table 5 estimates the influence of the proximity plus gender of the closest child for those mothers who had health issues compared to those who did not (the contrast category, main effects in Table 5). Figure 2 illustrates the predicted probabilities for different relocation outcomes when older women had health issues and when they did not.
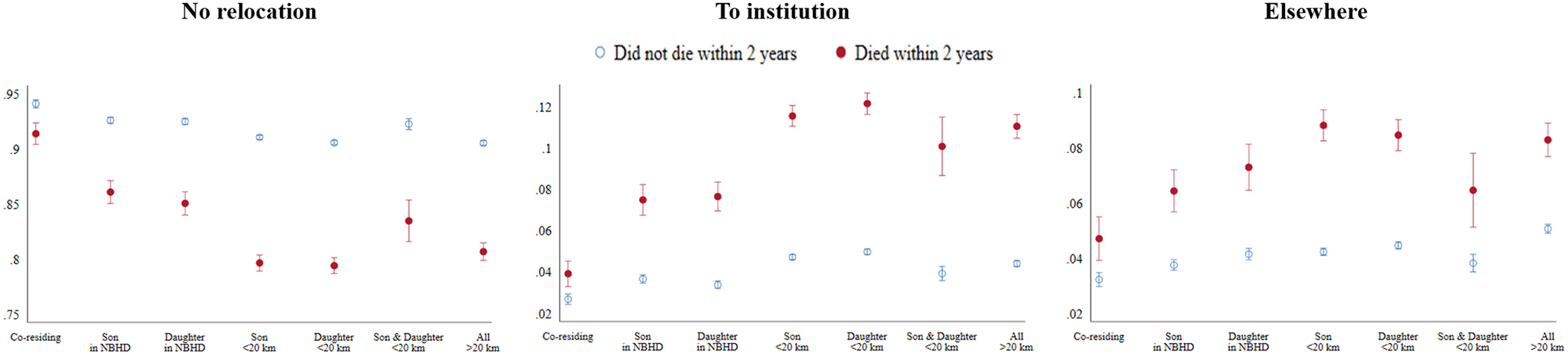
Figure 2. Predicted probability of proximity and gender of the closest child by mother's closeness to death.
Notes: Estimates and 95 per cent confidence intervals are shown. NBHD: neighbourhood. km: kilometres.
Table 4. The results of likelihood-ratio (LR) test for interaction terms
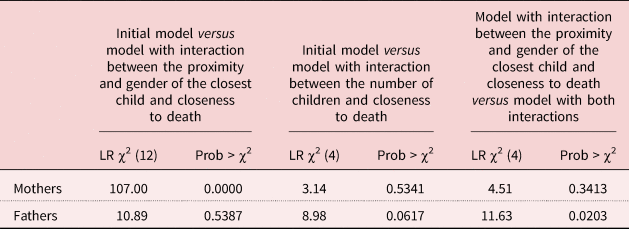
Source: Swedish register data, authors’ calculations.
Table 5. Multinomial logistic regression of relocation in old age by closeness to death (women)1
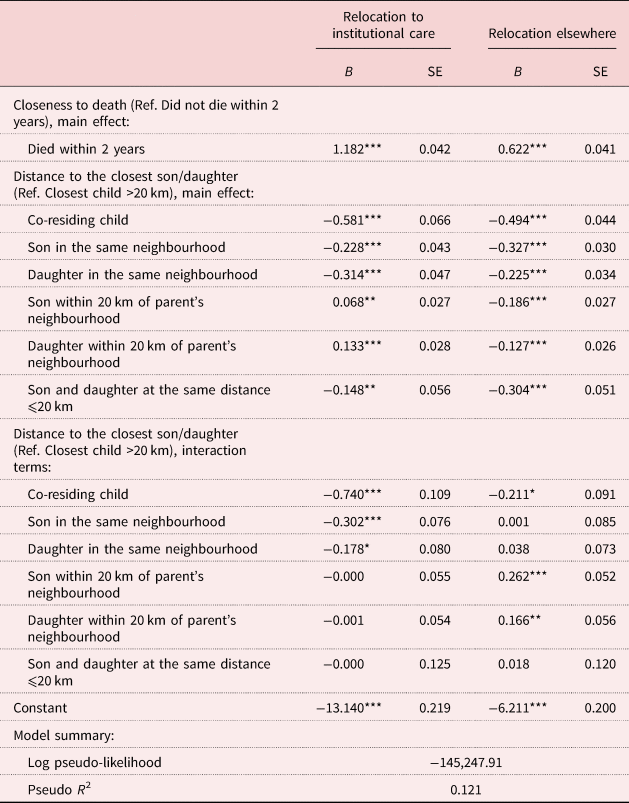
Notes: The control variables are the same as in the models presented in Table 2. 1. Reference category (Ref.): no relocation. SE: standard error. km: kilometres.
Source: Swedish register data, authors’ calculations.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
The major pattern that emerged when allowing for the association between moving to an institution and having nearby children to vary by the mother's closeness to death was that proximity to children was particularly important for women in poor health. This was visible by the larger fluctuations in the probabilities for women who had severe health problems by the proximity of the child (Figure 2). In fact, for women who did not have health issues, the probability of moving to an institution or elsewhere was almost constant across groups. As such, in support of Hypothesis 4a, our results demonstrated that for older women, having a child in the same household or neighbourhood hampered the likelihood of moving to an institution more for mothers who had severe health problems than for those with better health (statistically significant coefficients of first, second and third categories of the interaction term, first column, Table 5).
With some exceptions, the control variables showed results consistent with the findings of previous research. Parents’ old age was associated with a higher propensity of residential relocation. The older the closest child, the more likely a parent was to relocate to residential care or elsewhere. Living with a partner in older age was typically associated with lower propensities for all forms of relocation, with a stronger effect on the likelihood to be institutionalised. We did not find the effect of the presence of a partner in the closest child's household on the propensity of institutionalisation but older mothers whose closest child was living with a partner were more likely to move elsewhere than those whose children were living without a partner.
Receiving a pension above the median amount decreased the likelihood of relocation, but the effect was statistically significant only for women. Having at least one adult child with high income was associated with a higher propensity of mothers to be institutionalised and lower propensity to move elsewhere for both men and women (marginally significant). Older people with secondary and post-secondary education did have a lower propensity to move to institutionalised care compared with people who had a primary education.
From the perspective of local ties, people living in bigger dwellings had a higher likelihood of relocating to institutionalised care. The longer people lived in their home, the less likely they were to change residence. When compared with immigrant parents, women born in Sweden were less likely to be institutionalised than women born outside the country; no similar statistically significant difference was found for men.
Sensitivity and additional analyses
As an alternative approach to account for clustering of the observations (first level) at the person (second) and local (third) levels, we employed three-level mixed-effects logistic regression models of institutionalisation versus not moving. The intercept was assumed to vary randomly across these levels. The direction and magnitude of the AME values of the gender and proximity of the closest child and number of children on the likelihood of institutionalisation did not differ substantially from the estimates of the primary models.
To add context to the primary results and assess whether patterns of health-related migration differed based on the presence of children, additional analyses included older adults who did not have children. The results indicated that older women without children had similar patterns of institutionalisation as those whose closest child lived more than 20 km away. Men without children were as likely to be institutionalised as fathers whose closest child lived within 20 km. In terms of moving elsewhere, older women and men without children were similar to those whose closest child lived within 20 km. These findings are in line with the results of van der Pers et al. (Reference Van der Pers, Kibele and Mulder2015) who reported that the relocation behaviour of individuals without children was not very different from that of their peers with children.
The AME values from these models are available in the online supplementary material.
Discussion and conclusion
This paper explored (a) the role of adult children's gender, number and proximity in older parents’ moves to institutions and (b) variations in the effects of these characteristics of children by parents’ severe health problems. Our findings indicate that older people whose closest child lived in the same household or the same neighbourhood were less likely to be institutionalised.
While some studies demonstrate that daughters take care of older parents more than sons, the absence of statistically significant differences when the closest nearby child is a son or a daughter might reflect how children could give different but equally sufficient support at the end of parents’ lives. For example, daughters might give personal care while sons arrange complementary professional in-home care to avoid their older parents’ institutionalisation. Additionally, in sibling groups with sons, children are more likely to leave care responsibilities to their siblings or professional/in-home carers (Haberkern et al., Reference Haberkern, Schmid and Szydlik2015). Another explanation might support Johansson's (Reference Johansson1991) suggestion that the son's wives (daughters-in-law) help their husbands take care of frail parents. Furthermore, the non-significant differential effect of having a daughter compared to a son as the closest child on the likelihood of institutionalisation might be related to several dimensions of the context of contemporary Swedish society. Gender inequality in intergenerational care was lowest in countries with low levels of intergenerational care, high provision of professional care services, low family obligation norms and low levels of gendered division of labour (Haberkern et al., Reference Haberkern, Schmid and Szydlik2015). Sweden satisfies all these conditions.
The effect of nearby children on the likelihood of institutionalisation was stronger for mothers than fathers. This is in line with research in the United States of America, where support to mothers in good health was more common than support to fathers even in poor health (Silverstein et al., Reference Silverstein, Gans and Yang2006). This gender difference might reflect the more peripheral role of fathers in family life common in Sweden when older men in our sample were young. We also found gender differences in institutional care utilisation. Women might be more likely to be institutionalised due to longer periods of frailty and physical limitations before death than men, who more commonly face life-threatening conditions requiring hospitalisation (Oksuzyan et al., Reference Oksuzyan, Juel, Vaupel and Christensen2008; Chan et al., Reference Chan, Zimmer and Saito2011).
We did not find an effect of number of children on the likelihood of institutionalisation. One reason might be that it is usually only one person responsible for most of the care-giving work in a certain period of time while other care-givers (if any) provide sporadic assistance (Johansson, Reference Johansson1991). It can also partly explain why the interaction between severe health problems and number of children was not significant. However, we found that parents who had three or more children were more likely to move elsewhere than those with fewer children. One possible explanation is that since care-giver networks can change over time, one child can replace another in the provision of care (Szinovacz and Davey, Reference Szinovacz and Davey2007).
For older mothers, having a child in the same household reduced the likelihood of relocation to institutionalised care facilities more for those who had severe health problems than for mothers in better health. There was a similar effect for mothers whose closest child lived in the same neighbourhood. In line with Litwak's and Longino's (Reference Litwak and Longino1987) model of three stages of migration in later life and Cantor's (Reference Cantor1979, Reference Cantor1991) hierarchical model of support in old age, these findings suggest that older people's moves to institutions are primarily undertaken when care needs become substantial before death. In these circumstances, children living far away might be unable to provide sufficient care.
Our research has several limitations. First, we did not know whether older people actually preferred to age in place rather than move to an institution when a child lived nearby. We also had no way to determine whether having an adult child nearby reduced older parents’ chances of admission to a care institution. Additionally, we could not account for the actual use of in-home care by older people. Some might utilise this type of service and stay at home instead of moving into institutionalised care. Furthermore, older people might adjust their places of living to meet their needs for health-related care by moving closer to potential care-givers or to an adapted dwelling before getting close to death. Finally, there are obvious implications of our using closeness to death as a proxy for severe health problems. On one hand, it is unlikely that every death that occurred in the two-year observation window was anticipated; as such, our results likely include older people who did not have an opportunity to make residential adjustments before death. On the other hand, the sample might include older adults with long-term chronic conditions who relocated prior to our observation, potentially in search of sufficient care (in institutions or elsewhere). Our results would have more specificity given more detailed information about the health of older people and if the measure for moving to institutionalised care was available for more years.
Possible follow-up studies could address several of the limitations of the current study. It would be interesting to examine whether relocations elsewhere represent proximity-enhancing moves towards a particular child or in other directions. Future studies could also build on the register data with survey data to focus on the complex relationships between intergenerational solidarity – including geographic proximity – and older adult migration. We did not focus on the relocation of children towards their parents in response to their deteriorating health. Future studies could examine the relationship between the parent's transition to dependency and intergenerational proximity-enhancing moves by either parents or children. Another avenue for future research might be to explore how family members other than children provide informal care, particularly among older adults who do not have children. Finally, future researchers should harness the power of multilevel models (with local-level indicators) to assess variation in the relocation behaviour of older inhabitants of different municipalities.
Our study has provided deeper insight into older adults’ migration behaviours. To the best of our knowledge, it is the first study to account for institutionalisation of older parents as well as relocations elsewhere in Sweden. Revealing the role of children in this country has one important advantage. Swedish older adults are in favour of receiving care from formal sources rather than from family members (Andersson, Reference Andersson1993). They are also less likely than other Europeans to think that children should care for frail parents or move in with a parent when the partner of the parent is no longer present (Kalmijn and Saraceno, Reference Kalmijn and Saraceno2008). Our study indicated that even in these conditions, having nearby children decreases the likelihood of institutionalisation and moving elsewhere. The effects of proximity to children on the relocation behaviour of parents might be even more pronounced in less-comprehensive elder-care models or in more family-oriented societies.
In light of economic crises and ageing populations, welfare states are unlikely to master fully the older population's need for care without the informal support provided by adult children. Our study demonstrates that those who have children nearby are less likely to move to an institution. It means that informal care can be considered when planning policies for long-term care for older people. To facilitate informal care-giving, older people whose faraway children are ready, able and willing to provide them with care might receive priority access to housing in their children's area. Alternatively, children could receive support with relocation closer to their parents.
Another aspect of informal parental support that warrants consideration is the division of care among siblings. It is often the case that the distribution of intergenerational care is unequal among siblings (Haberkern et al., Reference Haberkern, Schmid and Szydlik2015). The nearest child often assumes responsibility for the lion's share while other siblings frequently use their distance to justify not providing assistance (Johansson, Reference Johansson1991). Policies might need to address this issue and ensure more equal division of care responsibilities between siblings. For example, as Haberkern et al. (Reference Haberkern, Schmid and Szydlik2015) proposed, cash-for-care could be partitioned similar to parental leave programmes, so that certain time periods are reserved for every adult child.
If governments are interested in minimising later-life institutionalisations, they should work on two fronts: (a) provide older people with access to supplemental care and (b) support family caregivers. In many cases, these measures will only work until the older person's need for care is too serious. If health-related care is not possible without professional medical assistance, a sufficient number of facilities for specialised care must be available.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X21000556
Author contributions
AA, MB, BJG and CHM developed the conception and design of this research. AA and MB prepared the dataset. AA performed statistical analyses and wrote the draft. MB supervised the data analyses. BJG, MB and CHM contributed to the revision of the draft.
Financial support
This research is part of the FamilyTies project led by Prof. Dr Clara Mulder at the Population Research Centre of the University of Groningen and the Ageing Well research programme led by Prof. Dr Gunnar Andersson at the Demography Unit of the University of Stockholm. The FamilyTies project has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation programme (grant agreement number 740113). The Ageing Well research programme has received funding from the Swedish Research Council for Health, Working Life and Welfare (Forte project number 2016-07115).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
All members of the FamilyTies project follow the ethical standards and guidelines of Horizon 2020. The processing of personal data followed the requirements outlined in the EC directive 95/46 and the European Regulation 2016/976 by the Data Protection Officer with the University of Groningen (reference number 17/04740). The Ageing Well research programme received ethical approval from the Swedish Research Council for Health, Working Life and Welfare (Dnr 2017/1623-31/5).










 Open access
Open access