


An important aspect influencing patients’ satisfaction with hospital stay is their relationship to food, nutrition being a part of hospital care. Moreover, the role of the hospital foodservice has become increasingly important because of problems associated with malnutrition(Reference Lassen, Kruse and Bjerrum1–Reference St-Arnaud-McKenzie, Paquet and Kergoat4).
Food should meet patients’ needs, help to eat and drink should be provided when necessary and food should be presented appropriately and consumed in a pleasant environment(Reference Ruxton, Gordon and Kirkwood5). Hospital menus should be planned according to patients’ preferences, focusing on variety, quality and taste, as well as hospital environment and pleasant helpfulness of nursing staff. This is a new qualitative approach to a complex problem(Reference Hickson, Fearnley and Thomas6–Reference O'Flynn, Peake and Hickson8). Context, including indirect environmental/cultural factors, indirect personal factors and socio-cultural aspects occurring before, during and after hospitalization, has also been identified as an important factor in understanding acceptance of food and in predicting food consumption(Reference Dube, Trudeau and Belanger9–Reference Quercioli, Marianelli and Conti13). However, few instruments to measure customer satisfaction exist and it is difficult to convert results into protocols and practices. Surveys usually have the limitation of asking very few general questions about foodservice, which are insufficient to obtain detailed feedback about objective and interpersonal aspects from patients and to investigate patients’ desire for personalized service. However, knowledge of these features seems to be an important basis from which to measure the impact of foodservice innovations or patients’ foodservice satisfaction outcomes in time(Reference King, Meiselman and Hottenstein14, Reference Wright, Capra and Aliakbari15). Several studies concerned with influences on foodservice satisfaction have been published, especially in the USA and Canada, but the relationships between consumer satisfaction, perceived quality and foodservice characteristics are largely unexplored(Reference Dube, Trudeau and Belanger9, Reference Donini, Castellaneta and De Guglielmi16, Reference Wright, Connelly and Capra17).
Evidence in this field is still lacking in our country (Italy); to our knowledge, only a few studies(Reference Donini, Castellaneta and De Guglielmi16, Reference Donini, Castellaneta and Magnano18) have raised these aspects. Therefore the aims of the present study were to: (i) measure patient satisfaction with foodservice in a big Italian university hospital; and (ii) study the influence of variables related to patient characteristics, hospital admission and food catering on overall perceived satisfaction.
Methods
Setting
The survey was carried out in Careggi Hospital, a publicly financed university hospital in Florence, Tuscany, central Italy. It is a highly specialized centre with 1500 beds and about 60 000 ordinary admissions and 73 000 day admissions per year. Patients are from the Province of Florence (population about 970 000), other Tuscan provinces and other Italian regions. Mean hospital stay is about 8 d(19). The study period was 1 November to 15 December 2009, and involved in-patients of fifty-five wards. The hospital has pavilion architecture and the food is prepared in a centralized kitchen. The foodservice is ‘cook–hot hold’ type. The type and quantity of food for each ward is loaded into (refrigerated and heated) food containers and is transported to the wards from the central kitchen by electric indoor buses. In the wards, nurses/nursing assistants load the container into trolleys, wheel them to all the rooms and serve an appropriate portion at every bedside. When no food restrictions apply, patients may choose between two or three hot first courses (mainly pasta, rice or soup), two or three main courses (mainly chicken, beef or fish) and two or three vegetables (mainly mashed potatoes or steamed vegetables) plus fresh fruit.
Meals are served three times daily: breakfast at 07.30–08.30 hours, lunch at 12.00–12.30 hours and dinner at 19.00–19.30 hours. Nurses do not distribute other food outside mealtimes, except fruit or yoghurt (late morning) and hot tea in the afternoon in some wards.
The food is ordered by the nurse responsible for the ward on the basis of the medical prescription on the clinical chart (without restrictions, modified texture, dysphagic, diabetic, high energy, high protein, etc.). Nutritional risk is evaluated and managed by doctors and nurses using a Malnutrition Universal Screening Tool(Reference Todorovic, Russell and Stratton20) chart which identifies three nutritional levels (low, medium, high) of patients. In the case of high risk, a dietitian is consulted and the diet is prescribed by the doctor and dietitian.
The estimated cost per meal may vary (preparation in/out of hospital, type of meal, etc.). The estimated cost of a meal in Careggi Hospital is about €11 ($US 15·98).
The questionnaire
Data were collected using a slightly modified version of the Acute Care Hospital Foodservice Patient Satisfaction Questionnaire (ACHFPSQ)(Reference Wright, Capra and Aliakbari15, Reference Theurer21) (see Table 2). Most nutritional screening tools do not measure various aspects that influence poor food intake and undernutrition. Since the ACHFPSQ differentiates foodservice into several detailed aspects, it is considered more effective in identifying specific areas in need of correction(Reference Wright, Connelly and Capra17, Reference Lau and Gregoire22). It was administered by nurses who could answer any questions patients might have. The ACHFPSQ is a reliable validated tool which gathers general information on the patients’ age, gender, length of hospital stay, appetite status (measured as food intake quantity), diet type (standard, high energy, high protein, modified for clinical reasons, texture modified) and need for help to answer the questionnaire(Reference Wright, Capra and Aliakbari15, Reference Ferguson, Capra and Bauer23). It comprises sixteen questions investigating the following dimensions: Food Quality (FQ), Meal Service Quality (MSQ), Staff/service Issues (SI) and Physical Environment (PE), plus two questions not included in these dimensions and one question investigating overall satisfaction (OS). We decided to include three more questions related to a fifth dimension, ‘Hunger and Food Quantity’ (HQ), which are not part of the published ACHFPSQ, but are part of the survey, because: (i) in the guidelines of the ACHFPSQ, this fifth dimension – hunger and food quantity – is described and it is identified by three additional questions; (ii) we felt that the three questions could be pertinent to the study; and (iii) we found that they have been used also in other research(Reference Theurer21). Patients could also write comments on the questionnaire(Reference Theurer21, Reference Capra, Wright and Sardie24).
We translated the questionnaire into Italian and then asked a translator whose mother tongue was English to translate it back into English again to check for errors, distortions and misinterpretations in the English–Italian translation. Finally, using other Italian questionnaires(Reference Donini, Riti and Castellaneta25, Reference Firenze, Morici and Calamus26) which investigate patient satisfaction with food, and to better adapt the ACHFPSQ to the Italian hospital context, we rephrased the item ‘The crockery and cutlery are chipped and/or stained’ to ‘I am satisfied with crockery and cutlery’ to make the question more direct and we changed the item ‘The cold drinks are just at the right temperature’ to ‘I am satisfied with meal distribution time’ because there were other questions related to the temperature aspects and this one, from a prior discussion with dietitians, emerged to be less important, at least in the Italian context, while a question regarding the meal distribution time was missing and was of interest also to other research. The questionnaire took approximately 15 min to fill in (alone or with nursing staff help). Patients rated each statement on a 5-point scale (always/often/sometimes/rarely/never) and expressed overall satisfaction with foodservice from very good to very poor. Adult patients (18+ years) were enrolled using non-probability sampling (convenience sampling)(Reference Ferber27). Patients were excluded if nursing staff considered their condition too poor or if they were not served food (no oral diet) or were too confused to answer or provide consent. Patients who did not wish to participate in the study returned a blank questionnaire. Patients’ names were not recorded.
Data collection and management
The authorization by and support of the hospital health management enabled good organization in distributing the questionnaire and the project was explained to nurses.
Questionnaires were distributed by nurses or other hospital staff according to the guidelines. The questionnaires were brought to patients on the food tray. Nurses explained that it was anonymous and authorized by the hospital administration for the purpose of improving catering. Questionnaires could be returned to nurses or other hospital personnel. Nurses had access to the completed questionnaires but it is unlikely that they influenced patient’ choices because questionnaires were anonymous and filled in by patients. Moreover, nurses were not responsible for food preparation. Finally, the questionnaire guidelines stated that health-care personnel could provide assistance in cases of difficulty in filling in the questionnaire.
All of the questionnaires were processed using the optical mark recognition software Remark Office version 7·0 (Gravic Inc., Malvern, PA, USA), which allowed us to standardize questionnaire reading methods in an efficient way. In cases of possible misinterpretation of marks, the software alerts the user so that the correct choice can be selected manually. All questionnaires were automatically stored in a database and later exported for statistical analysis.
Statistical analysis
Descriptive analysis (mean and percentages) was used to describe patients’ characteristics and answers to questionnaire items. To account for possible selection bias between respondents and non-respondents to all ACHFPSQ items, we conducted χ 2 tests for statistical significance. Factor analysis was then carried out to reduce multiple variables and the number of underlying factors describing catering and food characteristics. We used an intercorrelation matrix to account for collinearity of variables. Bartlett's test of sphericity was used to assess factorability of the intercorrelation matrix. Factors were extracted based on eigenvalues >1 (that explain more variance than a single variable)(Reference Dube, Trudeau and Belanger9). We chose varimax rotation to maximize the items in factor patterns. Items that did not fit any factor but had explanatory power were considered and analysed independently; indeed, factors were only included in the analysis if they contained at least three items(Reference Norman and Streiner28). Items scoring less than 0·4 on the factor were not included. Items grouped within a factor but also highly correlated with one or more factors (making factor interpretation ambiguous) were omitted(Reference Norman and Streiner28). To determine the factor score, also in accordance with the ACHFPSQ guideline, all items had to be answered. In fact, to maximize the validity of our results we opted for listwise deletion, excluding records lacking answers to even a single item, rather than creating predictors for distribution of missing values, which make it impossible to verify the consistency of derived models depending on the imputation method chosen(Reference King, Honaker and Joseph29). Missing answers have to be dealt with cautiously as they may introduce distortions(Reference O'Reilly, Jolley and Cameron30). The reliability of the questionnaire and the internal consistency of factors were evaluated by Cronbach's alpha coefficient (α C). Statistical significance was assessed at the 5 % level. Univariate and multiple ordinal regression analyses were used to investigate the influence of the factors obtained, age, gender, appetite status, patients’ diet type and length of hospital stay on overall perceived satisfaction measured on a 5-point scale (from very poor to very good). The multiple ordinal regression models only included variables that proved to be associated with the outcome at univariate analysis level. Descriptive analysis, as well as univariate and multiple ordinal regression, were conducted with the STATA statistical software package version 8 (StataCorp LP) and factor analysis was conducted with the SPSS statistical software package version 10 (SPSS Inc.).
Ethics
The study was conducted with the permission of the administration of Careggi University Hospital. The information about patients was anonymous and was obtained on a voluntary basis.
Results
A total of 1288 questionnaires were distributed and 927 were collected (overall response rate 72 %). Questionnaires were not returned by Orthopaedics, Urology, Gastroenterology and Day Hospital. After screening for missing answers to items included in factors, the total of questionnaires eligible for analysis was 603. The χ 2 tests for statistical significance did not highlight differences in characteristics of respondents and non-respondents to all ACHFPSQ items (Table 1).
Table 1 Characteristics (%) of the study population, overall and according to response to all ACHFPSQ items: hospital patients aged 18+ years, Florence, Italy, November–December 2009
ACHFPSQ, Acute Care Hospital Foodservice Patient Satisfaction Questionnaire.
Regarding the sample of respondents, the mean age was 54·0 (sd 18·0) years, with almost 25 % in the age group >70 years; 50·6 % were males. Of the sample, 57·4 % recorded ‘normal appetite’, 66·1 % had a standard/diabetic/cardiac diet and 56·9 % stayed in hospital for less than 1 week. Survey results are shown in Table 2. Items investigating staff/service issues were the most positively rated (83·4 % answered that staff who delivered meals were always neat and clean; 70·7 % that staff who took away finished meals were friendly and polite; 60·0 % that staff who delivered meals were helpful). Some items investigating food quality were the least positively rated (56·6 % answered that hospital food was sometimes/rarely/never as good as expected; 64·3 % answered that they sometimes/rarely/never liked the way vegetables were cooked; 60·0 % answered that meals had sometimes/rarely/never excellent and distinct flavours). Overall satisfaction was rated very good/good by one-third of the sample; one-third rated it sufficient and one-third as poor/very poor.
Table 2 Percentage distributions of the ACHFPSQ items answered (n 603) and factor scores of the factors obtained by factor analysis: hospital patients aged 18+ years, Florence, Italy, November–December 2009
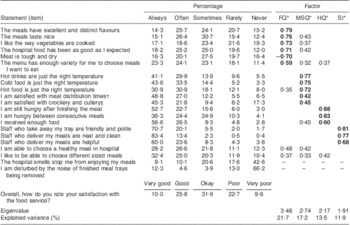
ACHFPSQ, Acute Care Hospital Foodservice Patient Satisfaction Questionnaire; FQ, food quality; MSQ, meal service quality; HQ, hunger and quantity; SI, staff/service issues.
*Items with value <0·40 were not shown except for specific items. In bold, values of items used in factors.
†Original version: ‘The cold drinks are just the right temperature’.
‡Original version: ‘The crockery and cutlery are chipped and/or stained’.
We found an association between the item ‘I am still hungry after meals’ and type of diet (P = 0·003). In particular, a majority of patients on special texture (minced/pureed) and high-protein diets answered that they were always hungry after meals.
Four dimensions of foodservice satisfaction were found by factor analysis: ‘food quality’ (FQ), ‘meal service quality’ (MSQ), ‘hunger and food quantity’ (HQ) and ‘staff/service issues’ (SI). The items used for factor analysis were seventeen out of twenty-one and explained 64·3 % of the total variance. In fact, four statements were excluded: (i) two statements were omitted because they were correlated with different factors making their interpretation ambiguous, i.e. ‘I am able to choose a healthy meal in the hospital’ (which had a correlation of 0·48 with FQ and 0·42 with MSQ) and ‘I like to be able to choose different sized meals’ (which had a correlation of 0·37 with FQ, 0·33 with MSQ and 0·42 with HQ; Table 2); and (ii) two statements were treated independently because they could have been included in a fifth factor, ‘physical environment’ (PE), which was not considered due to the insufficient number of items correlated with it, i.e. ‘I am disturbed by the noise of finished meal trays being removed’ (which had a correlation of 0·84 with PE) and ‘The hospital smells stop me from enjoying my meals’ (which had a correlation of 0·85 with PE). The results of the univariate and multiple ordinal regression analyses are shown in Table 3.
Table 3 Crude and adjusted analysis of patient characteristics, hospital admission and food catering factors in relation to overall perceived satisfaction (outcome): hospital patients aged 18+ years, Florence, Italy, November–December 2009

FQ, food quality; MSQ, meal service quality; HQ, hunger and quantity; SI, staff/service issues.
*Odds ratios calculated with single variables (exposure) and overall perceived satisfaction (outcome).
†Odds ratios calculated with single variables (exposure), adjusted for all the others, and overall perceived satisfaction (outcome).
At univariate analysis all of the factors seemed to influence overall satisfaction (OS) significantly (P < 0·001). In addition, the hospital smell item significantly and negatively influenced OS (OR = 0·88, P = 0·003). Males emerged as being more satisfied with hospital foodservice than females (OR = 1·35, P = 0·018). A lower food intake than normal influenced OS negatively (OR = 0·36, P < 0·001). Length of stay seemed to have an inversely negative effect on OS. The type of diet did not influence OS. The adjusted model showed that all four factors remained significantly (P < 0·001) associated with OS. In particular, for a one-unit change in FQ, the odds of a higher level of OS increased 17·2-fold. Apart from the four factors, the only variable significantly associated with OS was gender, wherein the relationship with OS from the univariate analysis become stronger (OR = 1·53; P = 0·024). Females seemed more critical than males: men had a 53 % higher probability than women of positive judgement of overall quality.
Discussion
Some important aspects emerged from the present study: (i) regarding methodology, the questionnaire developed for English-speaking countries, which we adapted to Italy, proved to be practical; (ii) in line with other studies regarding perceived quality(Reference Hartwell, Edwards and Beavis31–Reference Tranter, Gregoire and Fullam33), the most positively scored aspects of foodservice regarded staff and service, whereas food quality was considered less positive; (iii) the aspects that most influenced general satisfaction of patients were those related to food quality while aspects regarding staff, service, environment, patient characteristics and hospital admission emerged as less important; and (iv) we found some differences with respect to the structure of the published ACHFPSQ in some items which constitute it, in the loss of the PE factor and in the addition of the HQ factor. In particular, in our context, we found four factors underlying the twenty-one items: on the one hand, the extra three questions related to hunger and food quantity (‘I am still hungry after finishing the meal’, ‘I am hungry between consecutive meals’ and ‘I received enough food’) highlighted a new factor (HQ) which was not in the published ACHFPSQ; while on the other hand we did not have the PE factor. In fact, of the three items originally included in the Physical Environment dimension, one (‘The hospital smells stop me from enjoying my meals’) became part of the MSQ factor; the other two (‘I am disturbed by the noise of finished meal trays being removed’ and ‘The crockery and cutlery are chipped and/or stained’, the latter changed slightly in our adapted version to ‘I am satisfied with crockery and cutlery’) were included as independent variables in the multiple ordinal regression model because the factor would have been constituted only by two items and we decided to have factors only when the items were at least three(Reference Norman and Streiner28). In addition, the item ‘I am satisfied with meal distribution time’, which we introduced in the questionnaire, became part of the MSQ factor. Our questionnaire response rate was higher than those of other international studies(Reference Wright, Connelly and Capra17, Reference Capra, Wright and Sardie24, Reference Fallon, Gurr and Hannan-Jones34).
Regarding use of the ACHFPSQ in the Italian context, we think that the questionnaire was well received by patients; this is also confirmed by the moderate/good response rate (72 %) compared with other studies(Reference Wright, Capra and Aliakbari15, Reference Wright, Connelly and Capra17, Reference Capra, Wright and Sardie24, Reference Fallon, Gurr and Hannan-Jones34).
Contradictory results seemed to emerge in three items: 56·6 % of the sample answered that they always received enough food, but 52·7 % answered that they were always hungry after meals and 36·3 % that they were always hungry between meals (Table 2). However, these results may not be contradictory if patients received enough food but were unable to consume it for some reason, or were on a special diet and/or did not like the food and therefore did not eat it. The literature indicates that consumers with a good appetite may still have poor oral food intake owing to the food being placed out of reach, inability to handle cutlery, poor dentition, physical eating difficulties, meals being ordered too far in advance and a shortage of staff to encourage client intake and provide feeding assistance(Reference Wright, Connelly and Capra17).
All four factors obtained good Cronbach's alpha values (FQ, α C = 0·74; MSQ, α C = 0·73; SI, α C = 0·65; HQ, α C = 0·74), showing their good capacity to describe the underlying construct of the items. The first three values are consistent with those reported in the literature(Reference Capra, Wright and Sardie24) while the HQ factor, which is not in the published ACHFPSQ, had items which were well aggregated and had a good Cronbach's alpha. Regarding perception of the various aspects of foodservice, in our survey we can certainly state that patients rated staff/service issues very highly, while the food quality dimension was only rated as sufficient. This was also the result of previous studies using the ACHFPSQ: a one-day survey in 2005 (223 patients) was conducted in an acute-care private hospital, where staff/service issues were the most positively and food quality the least positively rated(Reference Fallon, Gurr and Hannan-Jones34); and a survey in 2006 (117 patients) was repeated twice due to introduction of off-site food preparation, but did not modify patients’ perception of quality(Reference Porter and Cant35). In our survey, satisfaction with food quality was certainly lower than previous findings but we do not know if this could be due to greater sample size or actual dissatisfaction.
Regarding the determinants of overall perceived quality among all factors, recent studies have reported that food quality (taste, presentation, flavour, preparation, variety) is the best predictor of overall satisfaction. Our multiple ordinal regression model to determine patients’ overall satisfaction also identified FQ as the major aspect (OR = 17·2). On the other hand, previous authors have suggested that ‘interpersonal’ or service aspects (clean, friendly, polite, helpful nursing staff) were the most important(Reference Gregoire36, Reference Tomes and Chee Peng Ng37). In our model SI was the least important (OR = 1·75). In line with results in the literature(Reference Hartwell, Edwards and Beavis31, Reference Fallon, Gurr and Hannan-Jones34, Reference DeLuco and Cremer38) our model also showed that associations between patients’ characteristics (age, gender, appetite status, length of hospital stay) and overall satisfaction, which were all significant (P < 0·01) in crude associations (apart from type of diet category), lost their explanatory power when adjusted for other variables (except gender, P = 0·024).
The four factors identified explained 64·3 % of the total variance in overall satisfaction, which is almost consistent with results in the literature(Reference Dube, Trudeau and Belanger9, Reference Capra, Wright and Sardie24, Reference Belanger and Dube39). Allowing patients to write comments on the survey was critical, as qualitative data provided in this manner can be used to support and enhance understanding of quantitative results. The comments also revealed new areas that could not be investigated but reflected patients’ needs and influenced their perception of food quality. Several comments stressed the need for a wider variety of food, suggesting the possibility of ordering in advance and flexible menus, especially for patients with allergies or food intolerances and pregnant women. We noticed that many patients would also like to have individually packaged dressings (e.g. salt, pepper, oil, vinegar) while others understood the importance of a balanced diet low in salt. Although staff/service ranked high, it could still be improved: patients complained about hygiene and especially the absence of gloves. This may indicate a need for public/patient education more than a need to improve staff hygiene. The public in general has many misconceptions about the indications for gloves v. hand washing.
Patients hospitalized in departments far from the central kitchen complained about the temperature of hot food. Other authors have already shown that how food is delivered influences patient satisfaction: hospitals using a bulk trolley method of food distribution provided food with better texture, temperature and flavour(Reference Hartwell, Edwards and Beavis31, Reference Edwards and Hartwell40–Reference Reglier-Poupet, Parain and Beauvais42).
Since to our knowledge the present study is one of the first conducted in an Italian hospital using the ACHFPSQ, we have to consider two aspects in benchmarking our results with similar European studies: (i) none of the statements refer to culinary tradition, which is recognized as an Italian prerogative; and (ii) our sample was bigger than those of other studies(Reference Wright, Connelly and Capra17, Reference Capra, Wright and Sardie24, Reference Fallon, Gurr and Hannan-Jones34, Reference Porter and Cant35) and this may increase the significance of our findings. The first point may raise the satisfaction threshold slightly, because perceived food quality was lower than in other European countries.
However, the research has some limits, the first being that patients’ overall satisfaction with foodservice is difficult to measure and quantify since it is largely subjective and influenced by many variables. The ACHFPSQ focuses on many aspects of foodservice overall satisfaction, but there are still aspects of quality that the questionnaire could miss. For example, we were aware that distribution times of meals could be relevant to determinate overall satisfaction and we added this question(Reference Donini, Castellaneta and Magnano18, Reference Donini, Riti and Castellaneta25). On the other hand, too long a questionnaire could annoy patients, making some answers less reliable. Moreover, other study results(Reference St-Arnaud-McKenzie, Paquet and Kergoat4, Reference Monsbakken, Vandvik and Farup43, Reference Simmons, Cleeton and Porchak44) indicate that variables such as pain, anxiety, irritable bowel syndrome, loss of sense of taste and depression may play an important role in the way patients reply to questions. It is also difficult to establish a cut-off of patient satisfaction, as there are few studies measuring hospital foodservice aspects with this validated instrument. Another aspect is that the sickest patients have low motivation to fill in questionnaires, as do patients with non-Italian speaking backgrounds. As we mentioned in the inclusion criteria, patients were not enrolled in the study if nursing staff considered their condition too poor or if they were not served food (no oral diet) or were too confused to answer or provide consent. Critical, very elderly and disabled patients were therefore presumably left out of the study, affecting the representativeness of the patient population. However, since the response rate was higher than in previous studies and there were no differences in the characteristics of respondents and non-respondents to all ACHFPSQ items, we believe that the effect of a selection bias is limited.
Conclusions
Lack of appetite for medical reasons is probably the main cause of malnutrition in hospitals. Our study also aimed to provide a basis for improving patients’ nutrient intake to accelerate recovery and to reduce the length of hospital stay. In conclusion, our findings suggest that the following improvements are possible: a wider menu, information on ingredients and better timing, distribution and presentation of food. These aspects should of course be added to those found by the questionnaire, such as how vegetables are cooked and why all foods tend to taste the same. To improve food quality, it may be necessary to train operators to choose high-quality primary materials according to Ministry for Health hospital food guidelines, which encourage local sourcing of ingredients and organic production(45).
The items regarding the role of hospital staff on overall quality were found to be the most positively rated but not the most determining. We highlight this aspect because it has a positive influence on patients’ experience of hospital food(Reference Johns, Hartwell and Morgan32).
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The authors declare that they have no conflicts of interest. G.M. collaborated in performing the study, carried out the data analysis and wrote the article; R.F. had the idea for the article, collaborated in the study design, collected the data and reviewed the drafts of the manuscript; F.V. performed the literature research, collaborated in the study design, collaborated in writing the article and reviewed the drafts of the manuscript; F.N. collaborated in the study design, made data available and coordinated the data collection, helped to conceptualize ideas and reviewed the drafts of the manuscripts; C.Q. collaborated in performing the data analysis, collaborated in writing the article, helped to conceptualize ideas and reviewed the drafts of the manuscripts; N.N. collaborated in performing the study, supervised the work, helped to conceptualize ideas and reviewed the drafts of the manuscripts. All the authors contributed to conception of the article, drafting and revision of content. All the authors have seen and approved the contents of the submitted manuscript. The authors thank Dr Olivia Wright for providing the questionnaire for their study.



