


Currently, there is extensive evidence that lifestyle factors, such as unhealthy diet, excessive alcohol consumption, smoking and sedentary lifestyle, contribute to an increase in morbidity and mortality due to the development of chronic diseases such as CVD, type 2 diabetes and cancer, among others(Reference Mokdad, Marks and Stroup1, Reference Thiele, Mensink and Beitz2).
Despite the fact that most studies have focused on the independent effect of each lifestyle factor on disease risk, recent publications have studied the synergistic effect of several combined lifestyle factors on health risk(Reference Ford, Bergmann and Kroger3–Reference Mozaffarian, Kamineni and Carnethon7). This is particularly important given that lifestyle factors tend to cluster in individuals(Reference Chou8–Reference Tobias, Jackson and Yeh11). Hence, the study of the clustering of risk factors has important implications on both disease risk and the development of preventive interventions targeting the combination of risk factors rather than individual risk factors.
As recent studies suggest, physical activity and diet are key factors for health maintenance, sharing – even synergistically – physiological mechanisms affecting the global metabolism(Reference Danaei, Ding and Mozaffarian12, Reference Sangster, Furber and Allman-Farinelli13).
It is well known that the prevalence of smoking, alcohol consumption and physical inactivity is increasing in Spanish adolescents and young adults, but information on the clustering of these behaviours is scarce(14). Moreover, because behaviours tend to cluster in adolescence and are maintained through adulthood, and socio-economic status is a determinant of lifestyle factors, it is important to assess lifestyle characteristics in this segment of the population. Thus, the aim of the present study was to ascertain the prevalence of and association between main lifestyle factors (diet, physical activity, alcohol consumption and smoking) in students from the Balearic Islands University.
Methods
Study design and sample selection
The present cross-sectional, descriptive study was carried out in a sample of university students. From May to November 2010, a sample of 987 students (age range 17–48 years), from a total of about 13 000 students from the University of Balearic Islands, was recruited. Students were randomly selected from the different faculties in the university. Twenty-five lecture rooms proportionally distributed among the different degrees were randomly selected, and all students present in the room were invited to complete the questionnaire. A total of 1100 questionnaires were distributed within the same semester and 113 students declined to participate in the study. Written informed consent was obtained from all participants. The gender, age and degree distribution of participants in our sample was similar to that of the overall university; hence this sample can be considered representative of the students of the university. The sample size allows a difference in proportions of 5 % (α = 0·05) to be detected with 99 % statistical power.
The questionnaire
The questionnaire was a short version of the Spanish National Health Survey 2006, completed with information about motivation for physical activity practice based on a previous questionnaire specifically developed for Spanish university students(Reference Pavon Lores, Moreno Murica and Gutierrez15). It was self-completed by the students with the supervision of trained interviewers.
The questionnaire included questions on the following.
1. Demographic and anthropometric characteristics of participants: age, gender, type of study, self-reported weight and self-reported height. BMI (kg/m2) was calculated. Individuals were classified as underweight (BMI < 18·5 kg/m2), normal weight (BMI = 18·5–24·9 kg/m2), overweight (BMI = 25·0–29·9 kg/m2) or obese (BMI ≥ 30·0 kg/m2).
2. Lifestyle: smoking habit (yes or no, age at start and number of cigarettes per day; smokers were also asked about trying to quit smoking), alcohol consumption (yes/no, age at start, frequency of consumption and frequency of drunkenness, type of alcohol consumed) and cannabis consumption (frequency).
3. Physical activity practice: students’ PA practice was ascertained with the question ‘Do you practise any type of sport or leisure physical activity during your free time?’ (possible answers: yes or no). The physically active students were also asked about the type of physical activity performed and weekly time spent on physical activity practice.
4. Dietary habits: a semi-quantitative FFQ, with additional questions on total number of meals per day and food preferences(Reference Schroder, Covas and Marrugat16).
Diet quality scores
Three different scoring systems covering different diet quality aspects were applied to this sample.
1. A Diet Diversity Score (DDS) evaluating the daily consumption of foods from different food groups: (i) protein-rich foods (meat, fish, eggs); (ii) Ca-rich foods (dairy products and legumes); (iii) complex carbohydrate-rich foods (cereals and tubers); (iv) fruits; and (v) vegetables. Two points were given to each individual consuming at least one serving size of each food group (i to v); 0 points were given when the consumption was below one serving size. The DDS range was 0–10 points(Reference Fransen and Ocke17).
2. A modified version of the Mediterranean Diet Score (MDS) evaluating the consumption of eight typical and two atypical Mediterranean diet food groups. When the individual's consumption of cereal products, whole grains, legumes, fruits, nuts, vegetables, fish and olive oil was above the sex-specific median, 1 point was given; 0 points were given otherwise (consumption below sex-specific medians). On the other hand, when the intake of dairy products and meat products was above the sex-specific median, the participant received 0 points and 1 point otherwise. The score range was 0–10 points. This score is a variation of the original MDS adapted to the dietary patterns and nutritional needs of this population group(Reference Trichopoulou, Costacou and Bamia18–Reference Trichopoulou, Orfanos and Norat21).
3. A Dietary Guidelines Score (DGS) assessing the degree of concordance with the Spanish dietary guidelines was created(Reference Aranceta and Serra-Majem22, Reference Serra-Majem and Aranceta23). Individuals with consumption (in serving sizes) of the food groups included in the Spanish food pyramid (cereals, fruits/vegetables, olive oil, dairy products, lean meat, legumes/nuts, fish, eggs, red/processed meat, fats and oils different from olive oil, and snacks/soft drinks/sweets) similar to recommendations obtained 1 point. When the intake was lower or higher (depending on the food group) participants received 0 points. The DGS score range was 0–10 points.
Moreover, an average Global Diet Quality Score (GDQS) was created by averaging the points obtained on each of the three scores (DDS, MDS and DGS). These three scoring systems were selected given their associations with chronic disease risk. Hence, the GDQS score range was also 0–10 points.
Statistical analysis
Descriptive statistics were based on the calculation of percentages for categorical variables, and means, medians and standard deviations for continuous variables. The level of significance of differences between percentages was assessed using the χ 2 test; the level of significance of the differences among means was assessed using one-way ANOVA.
Multivariate analyses were used to study the associations among main lifestyle factors and to study the sociodemographic and lifestyle determinants of being physically active (yes or no) and having a high (GDQS ≥ 5) or low (GDQS < 5) diet quality. First, univariate logistic regression was used to study the individual effect of all plausible determinants of diet quality and physical activity (sex, age, BMI, number of meals consumed daily, consumption of alcohol, tobacco and drugs, physical activity, diet quality). Variables that were significantly associated in the univariate analyses were included in the multivariate model. Hence, multivariate logistic regression, with the calculation of corresponding odds ratios, was used to assess which determinant factors were associated with diet quality and physical activity practice.
The existence of significant bivariate correlations among determinants and diet quality scores was ascertained by means of determining Pearson correlation coefficients.
The data analysis procedures were carried out using the SPSS statistical software package version 19·0 (SPSS Inc., Chicago, IL, USA).
Ethical approval
The study was performed in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of the University of the Balearic Islands. All participants were assigned fictitious names to prevent data from being traceable to any individual.
Results
Of participants in the study, 45·5 % were men and the mean age was 21·5 (sd 3·3) years. Mean BMI was 23·2 (sd 2·9) kg/m2 and 20·1 (sd 2·3) kg/m2 in men and women, respectively. Some 54 % of the students (43 % of women and 67 % of men) reported physical activity practice. The difference between genders was statistically significant (P < 0·01). Fitness, football and swimming were the most prevalent types of physical activity. Men were more likely to play football and women to swim or go to the gym (fitness). Among those who practised physical activity, 85·7 % did so for ⩾3 h/week. Eighty per cent of participants in the study reported to consume alcohol, either sporadically or regularly. On average, students reported to consume alcohol 5·5 (sd 5·0) times/month, of which alcohol consumption led to drunkenness 1·6 (sd 2·3) times/month. Consumption of alcohol and times of drunkenness per month were higher in men than in women (P < 0·05). The mean age at which students started to consume alcohol was 15·2 (sd 2·0) years. The most consumed alcoholic beverages were wine, spirits and beer. Regarding smoking habits, 35·9 % of participants were smokers (with 8·8 % of students reported to smoke sporadically and 27·1 % smoking on a regular basis). No statistically significant difference in the proportion of smokers between genders was found. Some 57·5 % of smokers reported to have tried quitting smoking without success, with no difference among genders. The mean age at which students reported to start smoking was 16·4 (sd 2·3) years, with no differences between genders. Regarding the use of cannabis, 44·1 % of participants in the study consumed cannabis, with no differences between genders in the age they started the consumption but with a higher consumption in men (Table 1).
Table 1 Lifestyle characteristics of the sample population: students (n 987) from the Balearic Islands University, Spain, 2010

DDS, Diet Diversity Score; MDS, Mediterranean Diet Score; DGS, Dietary Guidelines Score; GDQS, Global Diet Quality Score.
Data are presented as mean and standard deviation, unless otherwise specified.
Level of significance of the observed differences between means or percentages as assessed by one-way ANOVA or the χ 2 test, respectively: *P < 0·05, **P < 0·01, ***P < 0·001.
The mean score for the MDS was 5·1 (sd 1·8), for the DDS 7·6 (sd 1·9) and for the DGS 2·1 (sd 1·3). Women showed significantly higher DDS scores (mean 7·8, sd 1·9) than men (mean 7·4, sd 1·8). However, both sexes showed similar scores in the MDS and DGS. The mean score for the GDQS was 5·0 (sd 1·3), being significantly higher in women (5·0, sd 1·3) than in men (4·9, sd 1·3; Table 1).
Table 2 shows the consumption of food groups in men and women in relation to the Spanish dietary recommendations. The students’ dietary pattern was characterized by a low consumption of cereals and tubers, fruits, vegetables, olive oil, legumes and nuts, and a high consumption of processed meat, sweets, snacks, soft drinks and pastries. Women consumed significantly more fruits, vegetables and nuts than men. However, men were more likely to consume foods rich in fat and protein.
Table 2 Average intake of food groups in relation to the Spanish Food Guidelines in the sample population: students (n 987) from the Balearic Islands University, Spain, 2010
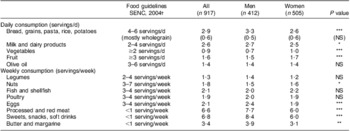
Level of significance of the observed differences between means as assessed by one-way ANOVA: *P < 0·05, **P < 0·01, ***P < 0·001.
†Food Guidelines for the Spanish population of the Spanish Society of Community Nutrition (SENC)(Reference Gerber62).
Table 3 shows the determinants of physical activity practice. Univariate analyses showed that men, older individuals, those with higher BMI, participants with a higher diet quality (GDQS) and non-smokers were more likely to be physically active. When all of these variables were included in the multivariate model we observed that only male gender, non-smoking and diet quality remained significantly associated with physical activity practice.
Table 3 Determinants of physical activity practice in the sample population: students (n 987) from the Balearic Islands University, Spain, 2010

GDQS, Global Diet Quality Score; Ref., referent category.
Level of significance of the crude odds ratio or adjusted odds ratio as assessed by univariate logistic regression or multivariate logistic regression, respectively: *P < 0·05, **P < 0·01, ***P < 0·001.
A similar analysis was performed to assess the sociodemographic and lifestyle determinants of diet quality. For that, the GDQS was divided into two categories (<5 and ≥5 points). Determinants of diet quality, both in the univariate and multivariate analyses, were physical activity practice, sex, age and number of meals consumed daily (Table 4).
Table 4 Determinants of diet quality in the sample population: students (n 987) from the Balearic Islands University, Spain, 2010
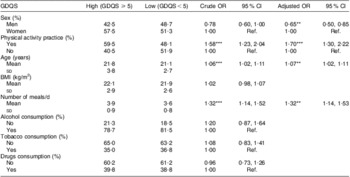
GDQS, Global Diet Quality Score; Ref. referent category.
Level of significance of the crude odds ratio or the adjusted odds ratio as assessed by univariate logistic regression or multivariate logistic regression, respectively: **P < 0·01, ***P < 0·001.
Table 5 shows the relationships between several determinants and the scores of the diet quality indices. Positive and statistically significant correlations were found between number of meals consumed daily and all of the diet quality scores determined. Higher number of meals consumed daily was correlated with higher scores for DDS, MDS, DGS and GDQS. However, no significant associations were found between the diet quality scores and determinants such as BMI, weekly hours of physical activity, tobacco consumption and frequency of alcohol consumption.
Table 5 Association between determinants and diet scores in the sample population: students (n 987) from the Balearic Islands University, Spain, 2010
DDS, Diet Diversity Score; MDS, Mediterranean Diet Score; DGS, Dietary Guidelines Score; GDQS, Global Diet Quality Score.
Daily meals (number of meals/d), Physical activity (h/week), Alcohol (alcohol consumption, times/month) and Tobacco (cigarettes/d) were used as determinants.
*Significance of the correlation (Pearson bivariate correlation): P < 0·01.
Discussion
In the present study we analysed food patterns, diet quality and physical activity practice and determinants among university students from the Balearic Islands. We were able to observe the clustering of lifestyle factors in the present sample, mainly physical activity and diet. Taking all these results together, we can determine which health promotion strategies could be more effective among university students.
Despite the great variation between different populations in the onset age of alcohol consumption, our study shows a similar age(Reference Pericas, Gonzalez and Bennasar24) or slightly higher age than reported in other studies(Reference Almazan, Sousa and Fernández25), which found a range between 12 and 15 years. Results from the present study show that alcohol consumption was not related to diet quality and physical activity levels. This may be because this alcohol consumption is so ingrained in our society to the point of being independent of other factors(Reference Breslow, Guenther and Juan26).
The smoking prevalence among participants in the present study is higher than the Spanish average and also higher than the prevalence in other neighbouring countries such as France and Italy(Reference Bogdanovica, Godfrey and MacNeill27). Furthermore, and in accordance with most studies that have focused on participants aged 18–24 years, this smoking prevalence tends to be higher in women than in men(Reference Bogdanovica, Godfrey and MacNeill27, Reference Howat, Hallet and Kypri28). It seems that this upward trend is supported by data from the school population (2008) because it was reported that 48·3 % of 18-year-old students smoked at least once in the 30 d preceding the date of the interview(29). The onset age of smoking found in the present study, about 16·4 years, is likely to have remained stable during past years. The high proportion of smokers who wanted to quit smoking and could not (57·5 %) is similar to that reported in other studies in similar environments and even in the same university in previous years, confirming the addictive power of tobacco(Reference Pericas, Gonzalez and Bennasar24, Reference Hyland, Rezaishiraz and Bauer30).
Results from the present study show an association between physical activity practice and lower smoking prevalence. This is in agreement with data reported by the Ministry of Health in 2005 and other authors who, in addition, have also associated physical activity practice with lower consumption of alcohol and other drugs(29). In this sense, more recent and complete studies have reported that belonging to groups of high risk (unhealthy) or low risk (healthy) is correlated with smoking prevalence, practice of exercise, alcohol intake and diet quality, with a tendency for specific health lifestyle factors to aggregate in clusters(Reference Dodd, Al-Nakeeb and Nevill31).
No relationship between quality of diet and smoking prevalence has been found in the current study. Literature reflects a great controversy regarding this issue(Reference Arabshahi, Lahmann and Williams32). Other studies found similar results to ours with not only a similar physical activity practice among smokers and non-smokers, as in the present study, but also a similar energy intake(Reference French, Popovici and Maclean33–Reference Guo, Warden and Paeratakul35). On the other hand, some researchers have shown a relationship between smoking and a less healthy diet (and also increased alcohol consumption)(Reference Dyer, Elliott and Stamler36–Reference Pisinger, Toft and Jorgensen38).
The percentage of students reporting being physically active in the present study is similar to that observed in a previous meta-analysis (about 50 %)(Reference Keating, Guan and Pinero39). As reported previously, men were more likely to be physically active than women(Reference Eisenmann, Bartee and Smith40–Reference Molina-Garcia, Castillo and Pablos44). Also, engagement in other healthy habits, such as a healthy diet and being a non-smoker, was associated with the practice of physical activity. Similar associations between healthy habits and physical activity have been observed in previous studies(Reference Faeh, Viswanathan and Chiolero45–Reference Seo, Torabi and Jiang48). However, no associations were found between the weekly hours of physical activity and quality diet scores, indicating that among the students who were physically active, the diet quality was not higher in those performing more hours of physical activity.
The dietary pattern of these university students is quite similar to that of Western societies. It is outstanding in the high consumption of food items from the top of the nutritional food pyramid which should be avoided, such as red and processed meat, snacks, soft drinks, sweets and pastries, butter and margarine. On the other hand, the consumption of fruits, vegetables, legumes, nuts and whole grains is much lower than recommended. Hence the high consumption of foods with high contents of saturated fat and simple sugars, and the low consumption of vegetables, reflect a change in dietary patterns as a consequence of the nutrition transition, and therefore the diet of young generations from the Balearic Islands has become quite different from the healthy Mediterranean diet(Reference Moreno, Sarria and Popkin49–Reference Serra-Majem, Ribas and Perez-Rodrigo53). This has also been observed in previous studies conducted within the same population(Reference Tur, Puig and Benito54–Reference Tur, Romaguera and Pons56). The change of dietary patterns towards a less healthy diet may lead to an increased risk of developing chronic diseases, such as CVD and cancer, in the future(57, 58).
In order to study diet quality in the present sample, several diet quality scores were applied. The evaluation of the overall diet from a global perspective is widely used in nutritional epidemiology studies as a way of taking into account simultaneously several nutritional aspects associated with diet quality and better health status(Reference Bach, Serra-Majem and Carrasco59–Reference Kant64). In the present study, diet diversity, concordance with dietary guidelines and adherence to the Mediterranean diet were considered important aspects of diet quality for the present population. In this population, despite showing overall high scores for diet diversity, the concordance with the Spanish Food Recommendations was very low. High diet diversity has been reported in developed populations where access to plenty of food items is common. Mean DDS was higher in women than in men, which led to an overall higher global diet quality in women compared with men. Better nutritional profiles in young women than men has been reported previously(Reference Serra-Majem, Garcia-Closas and Ribas50, Reference Serra-Majem, Ribas and Pérez52). Another independent determinant of diet quality is the number of meals consumed each day. Probably more frequent food consumption led to higher diet diversity and, hence, to higher diet quality.
A limitation of the present study and the methods used to assess diet quality is the fact that we could not adjust dietary intakes for total energy. This was due to the method of dietary assessment that did not allow us to derive energy intake properly, as has been indicated previously(Reference Schroder, Covas and Marrugat16). Adjusting for energy intake would have permitted us to reduce part of the measurement error associated with dietary assessment tools and probably may have deattenuated part of the observed associations. Nevertheless, previous authors have questioned whether using energy-adjusted food intakes for the derivation of dietary patterns is necessary or appropriate(Reference Northstone, Ness and Emmett65), even with the use of dietary scores such as the MDS, given that energy intake may be in the causal pathway linking a Mediterranean diet with several health outcomes(Reference Trichopoulou, Naska and Orfanos66).
It is difficult to estimate whether physical activity leads to higher diet quality or vice versa in the present cross-sectional study. However, both factors tend to cluster in this population. Although subtle gender differences may exist, promoting physical activity practice may lead to a better diet quality and the other way round. According to these results, perhaps among women more emphasis should be made on the promotion of physical activity and among men on improving diet quality. Nevertheless, in both genders the association between the two factors was linear and significant (data not shown).
In addition to the lack of adjustment for total energy intake indicated above, our study presents some more limitations. The first one is that, as indicated in the Methods section, some information has been obtained based on self-reports and therefore is subject to measurement errors. Furthermore, it is possible that categorization of variables may have affected our findings, and probably more categories should have been introduced in order to improve results regarding the associations tested. On the other hand, the fact that the study supposes an update of a topic with only a few previous studies focused on the Spanish university population could be considered the most important strength. The relatively high number of participants in the study as well as the number of variables collected from the participants could be also taken into account when considering the strength of results from the study.
Conclusions
Results of the present study demonstrate a tendency for clustering of risk factors (smoking, diet and physical inactivity) among Spanish university students. Overall diet quality was low, due to important differences from dietary recommendations and loss of the traditional Mediterranean dietary pattern. Nutritional education campaigns that include promotion of physical activity practice are needed to improve the overall health status of this population.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. There are no conflicts of interest. C.M.-G. and A.A.-P. were responsible for the study conception and design; S.M.-A., P.T.-R. and M.B.-V. performed the data collection and data analysis; D.R.-B. provided statistical expertise and contributed to the final review; A.A.-P., P.T.-R. and M.B.-V. wrote the manuscript; J.P.-B. and C.M.-G. provided support and contributed to revisions of the project and the manuscript. The authors would like to especially thank all the participants, since without them it would not have been possible to carry out this study.





