


Acute poisoning is a major health problem and accounts for many hospital admissions annually. Most cases involve self-poisoning (96%), Reference Hovda, Bjornaas, Skog, Opdahl, Drottning and Ekeberg1 and self-poisoning is the method used in 92–94% of episodes of self-harm and parasuicide. Reference Hawton, Zahl and Weatherall2–Reference Hall, O'Brien, Stark, Pelosi and Smith4 Previous self-harm is a known risk factor for suicide, and repeated self-harm represents an even greater risk for subsequent suicide than a single episode. Reference Zahl and Hawton5 Studying the repetition pattern of self-poisoning is important in both surveying the extent of the problem and identifying predictors of repetition.
Several studies have analysed the repetition patterns for self-poisoning and other self-harm. A systematic review found a 16% median repetition rate of non-fatal self-harm at 1 year and 23% at 4 years after the index episode. Reference Owens, Horrocks and House6 Similarly, other studies of self-poisoning have shown 1-year repetition rates of 6.3–18%. Reference Goldacre and Hawton7–Reference Rafnsson, Oliver, Elton and Bateman10 All these studies were based on hospitalised patients, but self-poisoning is frequently treated outside hospital without further referral, even though many of these poisonings are severe. Reference Buajordet, Naess, Jacobsen and Brors11 These poisonings are often related to drug or alcohol misuse, but evaluating intent is problematic in the pre-hospital setting. The index and subsequent episodes may be treated on different levels in the healthcare system, and the only way to identify a repetition pattern is to include all poisonings in a specified geographical target area.
To the best of our knowledge, no studies have focused on the repetition of poisoning, systematically including both hospital admissions and patients treated outside hospital. Previous studies have been limited to certain degrees of suicidal or other intent. However, patients presenting with self-harm, poisoning, drug addiction, alcoholism, suicide attempt, suicide, or with causes of sudden death other than suicide, may overlap in complex ways. Almost half of the people who misuse drugs admitted for detoxification have previously attempted suicide, Reference Johnsson and Fridell12 and 28% of suicide attempters misuse substances. Reference Hawton, Simkin and Fagg13 Alcohol or substance misuse is found in up to half of all suicides. Such misuse is second in frequency only to depressive disorders and is a significant contributor to suicide. Reference Murphy, Hawton and Van Heeringen14 The delineation of the different intentions behind poisoning is vague and overlaps substantially in different groups of individuals who present with self-poisoning or intentional/unintentional misuse-related overdose. Hence, the intention may be difficult to evaluate, and has been evaluated differently in different studies. Reference Welch15 Many patients admitted for self-poisoning that is evaluated as a suicide attempt may later be treated for poisoning that is interpreted as unintentional and vice versa. However, the long-term consequences may be severe, irrespective of the intention behind the poisoning, and both unintentional overdose and intentional self-poisoning increase the risk of later suicide and violent death from other causes. Reference Rygnestad16–Reference Bjornaas, Jacobsen, Haldorsen and Ekeberg18
The aims of this study were to quantify the rate of repetition in an unselected population of all the acute poisonings in Oslo in 1 year, irrespective of intention or level of healthcare, and to identify possible risk factors for repetition.
Methods
Study design
This was a 1-year prospective multicentre study. The inclusion criteria were patients ≥16 years of age with a main diagnosis of acute poisoning, either intentional or unintentional. The exclusion criteria were chronic poisoning and patients with another primary diagnosis, such as trauma, even if there was additional acute poisoning. The geographical target area was the city of Oslo. The medical emergency system in Oslo is relatively simple and clear, with only one ambulance service (part of the public healthcare system) and one large out-patient clinic located in the city centre (Oslo Emergency Ward), and all patients requiring admission are transferred to one of four public emergency hospitals. Data in this study were collected from these institutions, which are responsible for the medical treatment of all acute poisonings in Oslo. Rare exceptions may be cases treated by general practitioners without transferral to a higher healthcare level or cases admitted directly to non-internal medicine specialist department such as ear, nose and throat departments.
Study sample
Oslo is an urban setting, with a population in 2004 of 521 886 people, 428 198 of whom were ≥16 years of age. Of these, 48.2% were male, median age was 40 years (men) and 42 years (women), and interquartile range was 30–55 years (both genders). 19 There was a total of 3774 contacts during one year: 947 in hospitals, 958 in the out-patient clinic, and 1869 with the ambulance service (Fig. 1). Because some patients were transferred, more than one contact for each episode was possible, and these contacts resulted from 2997 poisoning episodes (700/100 000/year), involving 2298 individuals. Of the total number of episodes, 771 were registered at two (n=765) or three (n=6) levels of care, and 699 episodes were repetitions (163/100 000/year). Sixty per cent of all patients were men, but this differed between hospitals (44%), the out-patient clinic (68%), and the ambulance service (66%). The median age was 35.8 years, range 16–92 years, with no differences between the levels of healthcare.
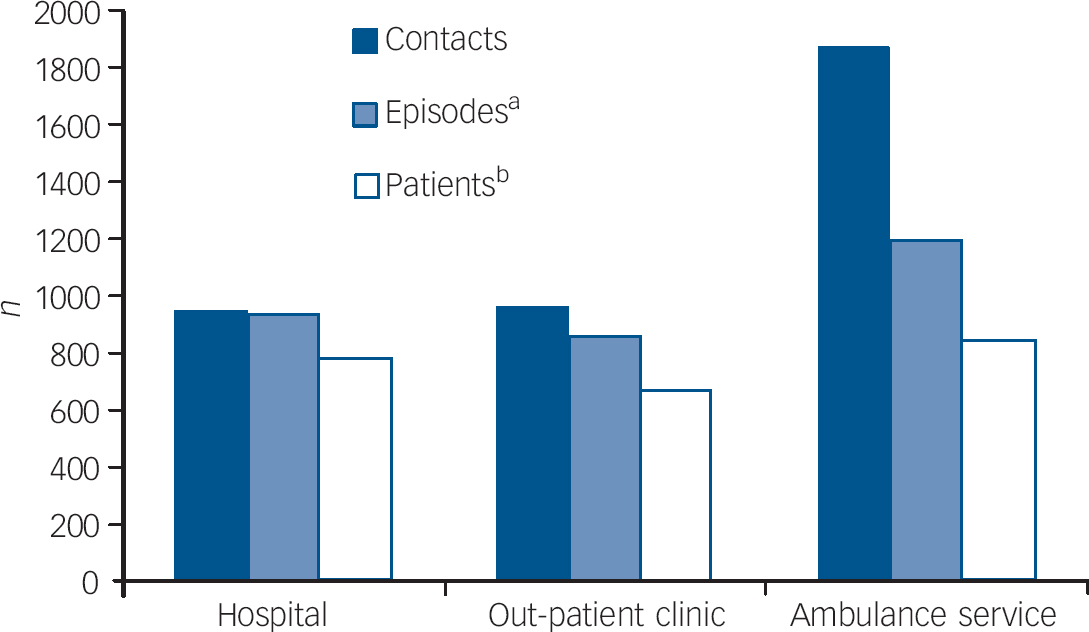
Fig. 1 Acute poisonings in Oslo in 1 year. In total, 3774 contacts for 2997 episodes in 2298 patients were registered (repeated episodes on the same day were considered one episode). a. Each episode was counted once, at the highest healthcare level for that episode. b. Patients were counted once at the highest healthcare level at which they were treated.
Thirty-six patients were transferred from an ambulance or the out-patient clinic to hospitals outside Oslo. Patients fulfilling the inclusion criteria were included even if they refused to be transferred from an ambulance or the out-patient clinic to hospital. Missing or uncertain identities made the tracking of 236 (10.3%) individuals difficult. Compared with patients of known identity, the ‘missing patients’ (uncertain identity) were more frequently men (72% v. 58% respectively; P<0.001); slightly younger (median age 30 v. 36 years respectively; P<0.001); more frequently treated in an ambulance or in the out-patient clinic (96% v. 67% respectively; P<0.001); used an opiate as the toxic agent (45% v. 25% respectively; P<0.001); and were comatose (33% v. 22% respectively; P<0.001). Patients who died during the index (first) episode (n=16) were excluded from the analysis. The repetition analysis was performed on 2745 episodes involving 2046 patients.
In total, 72 of the patients died during the study period: 16 during the index episode and 56 subsequently. Of the latter, 15 were self-poisonings considered as repetitions (11 opiate overdoses, 2 unspecified poisonings in drug addicts, and 2 multiple-tablet poisonings), 8 of which were second episodes counted as repetitions and 7 of which were deaths subsequent to repeated episodes already counted in the analyses; for 41 of the 72 deaths for whom poisoning was not the primary cause of death, 33 were censored by date of death in the repetition analyses, and 8 died after repeated episodes already counted in the analyses (Fig. 2). Of all the non-poisoning deaths, 8 were suicides by violent methods (4 with additional self-poisoning): 5 by hanging, 2 by drowning, and 1 by jumping in front of a train. Five deaths were accidents: 3 falls and 2 fire accidents. Twenty-eight were deaths by natural causes according to ICD–10. 20 The causes of death were obtained from the National Death Register.
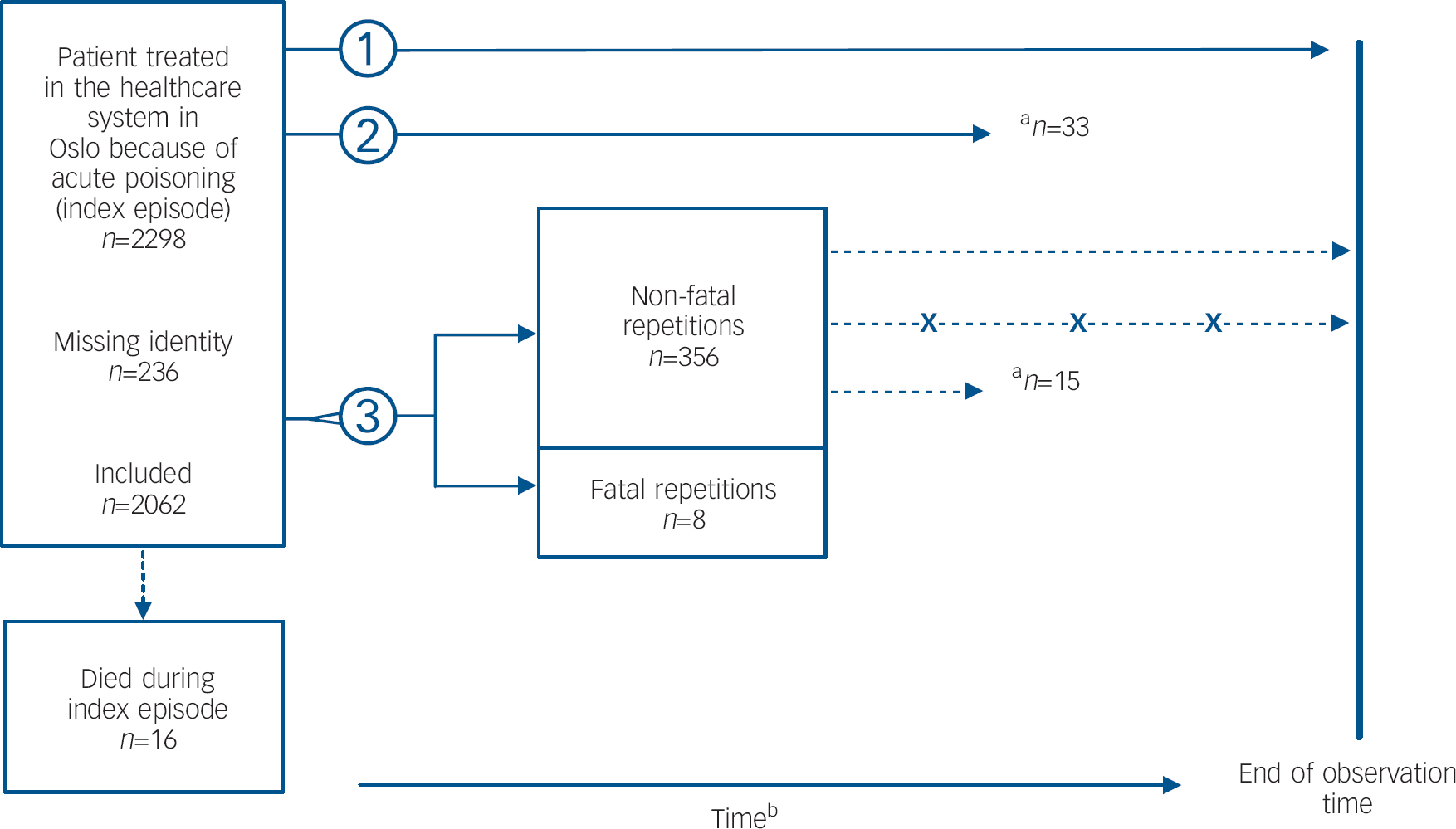
Fig. 2 Flow diagram. Line 1: patients with no repetition – censored by the end of the observation time in the repetition calculations. Line 2: patients with no repetition, who died of non-poisoning causes – censored by the date of death in the repetition calculations. Line 3: patients with non-fatal or fatal repetitions of acute poisoning – those with non-fatal repetitions may have subsequently had more episodes (X) or died. They appear with the first non-fatal repetitions in the repetition calculations. a. Number of deaths subsequent to poisoning episodes. b. Observation time varied depending on the time of inclusion in the study.
Data collection
Data were collected from 1 April 2003 until 31 March 2004. To guarantee complete collection, all participating centres had a study coordinator to ensure that all eligible patients were included, and the centres were followed up on a weekly basis by the researchers. Standardised registration forms were completed by the physicians at the hospitals and the out-patient clinic, and by paramedics in the ambulance service. In the pre-hospital settings, limitations on the time available for filling out forms was an important factor, and the study forms were less comprehensive for the ambulance and out-patient clinic part of the study than for the hospital part. The forms were optically scanned and processed using TeleForm Desktop version 9.1 for Windows. All patients were checked against the National Death Register, and patients who died were censored by the date of death in the Cox regressions and Kaplan–Meier calculations.
Classification
The first registered episode for each patient was called the ‘index episode’, and all subsequent episodes treated by at least one of the participating institutions during the observation period were classified as ‘repeated episodes’. More than one episode on the same day (date) was considered as one episode. Every episode was represented by the last and highest healthcare level in the chain of transferral.
The ‘main toxic agent’ was defined as the substance considered to be most toxic in the amount taken. Other ingested agents were defined as ‘additional agents’. This classification was based on information from the patients or their companions, clinical observations and, if applicable, findings at the scene of the overdose. We report the main toxic agents by major pharmacological classes (Table 1), but paracetamol was considered as a distinct group because of its special position as an intoxicant compared with other non-opioid analgesics.
Table 1 Cox regression analysis of repetition after the first registered episode at all participating centresa

| Crude effect | Adjusted effect | ||||||
|---|---|---|---|---|---|---|---|
| n | HR | 95% CI | P | HR | 95% CI | P | |
| Toxic agent | |||||||
| Alcohol (ethanol)b | 694 | ||||||
| Sedatives | 267 | 1.62 | 1.16-2.26 | 0.01 | 1.56 | 1.11-2.18 | 0.01 |
| Antidepressants | 62 | 1.41 | 0.73-2.71 | 0.30 | 1.40 | 0.73-2.68 | 0.32 |
| Antipsychotics | 50 | 0.82 | 0.33-2.02 | 0.66 | 0.79 | 0.32-1.93 | 0.60 |
| Opiates | 502 | 2.22 | 1.71-2.90 | <0.001 | 2.04c | 1.55-2.69 | <0.001 |
| Other illicit drugs | 144 | 1.02 | 0.63-1.65 | 0.95 | 1.03 | 0.63-1.69 | 0.91 |
| Other agents | 214 | 1.18 | 0.78-1.77 | 0.44 | 1.17 | 0.78-1.76 | 0.44 |
| Paracetamol | 113 | 1.14 | 0.67-1.94 | 0.63 | 1.15 | 0.67-1.96 | 0.61 |
| Age, years | |||||||
| <30b | 689 | ||||||
| 30-49 | 922 | 1.52 | 1.20-1.92 | 0.001 | 1.36 | 1.07-1.74 | 0.01 |
| 50-69 | 336 | 1.04 | 0.75-1.45 | 0.81 | 1.14 | 0.81-1.61 | 0.44 |
| >70 | 99 | 0.55 | 0.27-1.12 | 0.10 | 0.61 | 0.27-1.27 | 0.19 |
Consciousness was classified according to the following scale: awake (n=1309); somnolent, could be kept awake when stimulated (n=1026); coma, responsive to painful stimuli (n=340); and deep coma, no response to painful stimuli (n=322). Coma and deep coma correspond to a Glasgow Coma Score Reference Teasdale and Jennett21 <8.
Additional classifications in the hospitals
The intentions of the poisonings were evaluated by the hospital physicians based on the patients' own reported intentions and information from other sources, such as ambulance personnel and companions. Special attention was paid to letters confirming the patient's suicidal intent where available, the supposed lethal doses of the toxic agent, and other active procedures used to secure a fatal outcome, such as intake of substances in remote places or hiding after intake. Intentional self-poisonings were defined as definite suicidal (n=92), possible suicide (n=240), and appealing/manipulative (n=232). Other self-poisonings were drug- or alcohol-misuse related (n=344), and non-self-poisonings were classified as accidental poisonings (n=39). The following parameters were also recorded: previous suicide attempt (self-reported: during the past 12 months (n=232); before the past 12 months (n=145); yes but cannot remember when (n=33); none (n=361); unknown (n=176)); ongoing or previous psychiatric treatment (yes (n=550); no (n=244); unknown (n=153)); marital status (single (n=346); married or cohabiting (n=292); widow/er (n=42); divorced (n=163); unknown (n=104)); highest level of education (primary school (n=240); high school (n=265); college or university (n=137); other (n=28); unknown (n=277)); ethnicity (Norwegian (n=781); other Nordic countries (n=23); other European countries (n=33); North American (n=1); South American (n=11); African (n=15); Asian (n=73); Australian (n=0); unknown (n=10)); occupational status (working or equivalent (n=338); on sick leave (n=83); unemployed (n=120); living on social welfare (n=284); other (n=15); unknown (n=107)). The group ‘working or equivalent’ included pupils and students at school for school-aged individuals, employed individuals for those of working age, and retired individuals for the elderly. The frequency of drug and alcohol use was registered, and grouped into daily misuse (n=270), no daily misuse (n=477), or unknown (n=200). Patients with missing or unknown variables were excluded from the Cox regression analysis. Thus, the total number in the multivariate analyses was less than that in the total of the study.
Statistical analysis
Statistical tests were performed using SPSS, version 15 for Windows. To compare frequencies, the Pearson χ2-test was used with a 5% significance level. A Kaplan–Meier plot was calculated to estimate repetition after the first registered episode, showing the cumulative percentage of repeaters. Reference Pocock, Clayton and Altman22 Cox regression analysis was used to estimate the hazard ratios (HR) for potential predictors of repetition. For multivariate Cox analysis, the maximum number of categories included was less than 10% of the number of events analysed (reference categories excluded). The variables included in the multivariate analysis were selected primarily for their clinical importance. Subsequent crude analysis of these variables was performed, and only those variables with P<0.2 for any of the categories were included. Non-significant variables in the multivariate model were removed and added back one at a time, to check whether they contributed significantly to the model as confounders. If no such contribution was noted, the variables were omitted from the model. Possible interactions were analysed, focusing on gender and age. Correlations between independent variables were calculated to ensure no correlation of 0.7 or more. The proportionality of the hazards assumption was checked in each model and found to be adequately fulfilled.
Ethics
Treatment was given according to standard hospital protocols and in accordance with the Helsinki Declaration. Permission was obtained from the National Data Inspectorate and the regional ethics committee. All data were stored anonymously, and the links to social security numbers and names were kept by Statistics Norway.
Results
A total of 2062 patients of known identity were treated for 2761 episodes of acute poisoning, giving an episode:patient ratio of 1.34. In total, 364 (17.7%) patients had more than one episode during the study period, and 150 (7.3%) had three or more episodes. The greatest number of episodes for a single individual was 24 (with 33 contacts). Of all episodes for people of known identity, 699 (25.3%) were repetitions and these were distributed equally across the different healthcare levels.
The Kaplan–Meier calculations showed that the cumulative proportion of patients without repetition was 0.704 (95% confidence interval (CI) 0.65–0.76), indicating that 30% of patients treated for acute poisoning repeated the poisoning during the first year (Fig. 3). The curve was steepest during the first month, and 10% of patients repeated their poisoning within 50 days. For the remainder of the year, the curve was linear. When stratified according to index episode treated inside or outside hospital (the out-patient clinic or ambulance), Kaplan–Meier calculations revealed a repetition rate of 27% for hospitalised patients and 31% for patients treated outside of the hospital. Cox regression analysis gave an HR for repetition of 0.82 (95% CI 0.66–1.03; P=0.10) for hospitalised patients v. those treated outside hospital.
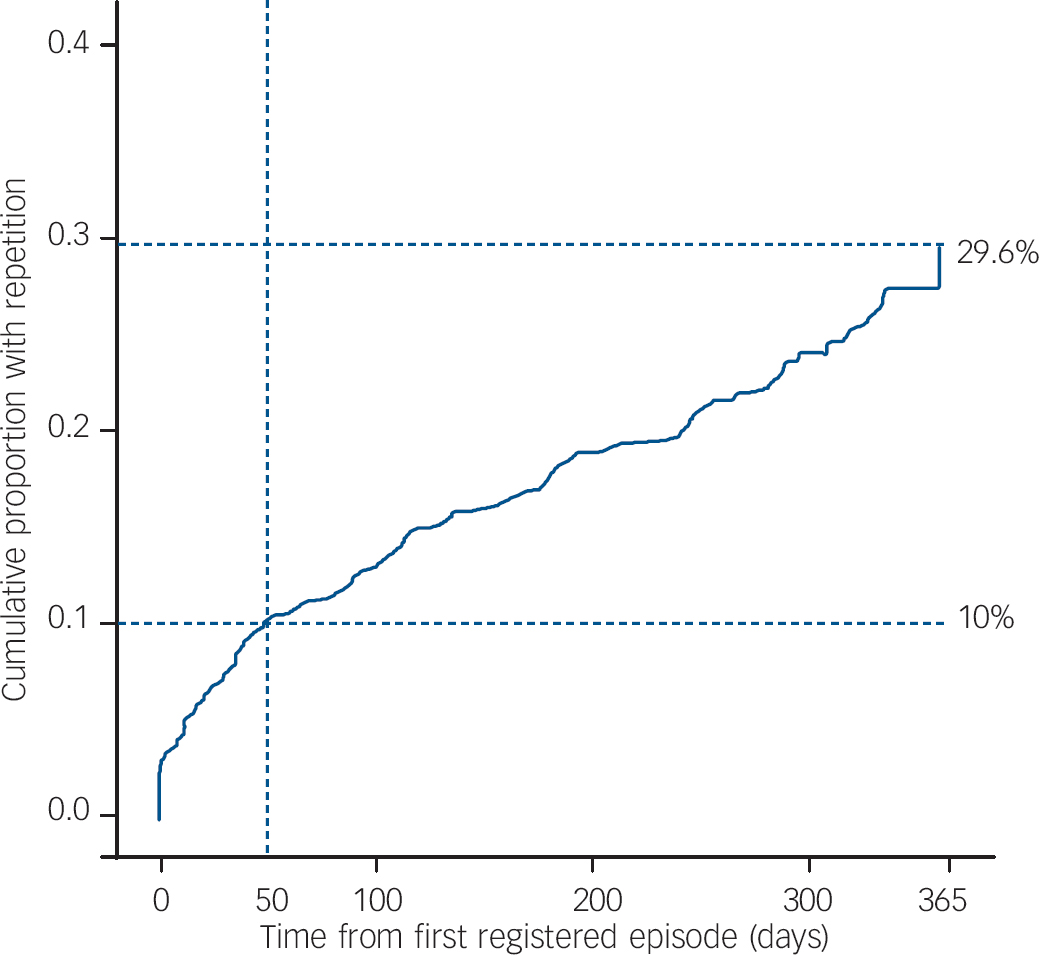
Fig. 3 Repetition of acute poisoning over 1 year estimated with Kaplan–Meier analysis. The last repetition occurred on day 360, when 29 patients were still under observation. Patients under observation: day 1, n=2038; day 180, n=918; day 300, n=319.
Cox regression models were used to identify possible predictors of repetition. Gender, age, consciousness, and toxic agent were analysed for the whole study sample. Crude analyses showed no gender differences in repetition (female: HR=1.01, 95% CI 0.82–1.24; P=0.93), even when included in the multivariate model. Although consciousness alone contributed significantly (overall P=0.01; deep coma: HR=1.7, 95% CI 1.25–2.37; P=0.001), this effect disappeared in the multivariate analysis when corrected for toxic agent and age. Consciousness was not a confounding variable, and it was therefore not included in the multivariate model. Age made a non-linear contribution to repetition (Fig. 4). The contribution was greatest in middle-aged individuals, so this variable was transformed from a continuous to a categorical variable. Age between 30 and 49 years contributed significantly to repetition compared with age <30 years (HR=1.4, 95% CI 1.07–1.74; P=0.01). There were no interactions between age and gender. The main toxic agents, opiates (HR=2.0, 95% CI 1.55–2.69; P<0.001) and sedatives (HR=1.6, 95% CI 1.11–2.18; P=0.01), were significant predictors compared with alcohol, used as the reference (Table 1). However, opiates interacted significantly with age (P<0.001). Poisoning with opiates entailed higher repetition in the age group <30 years (HR=7.7, 95% CI 3.93–15.25; P<0.001) than in the age group 30–49 years (HR=1.2, 95% CI 0.84–1.70; P=0.3). No interactions with gender were identified.
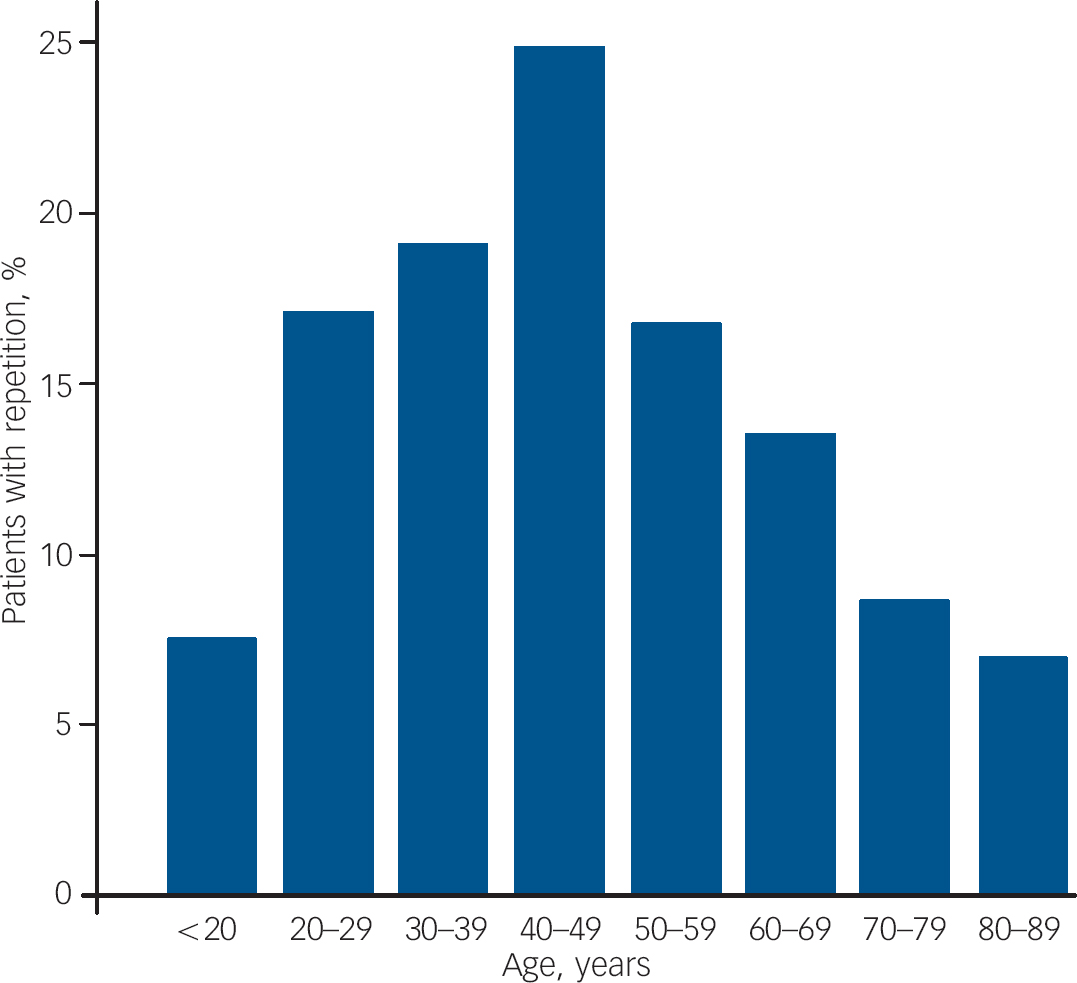
Fig. 4 Repetition according to age group. Each bar represents the percentage repetition within each age group. The percentages are based on observed numbers, and are therefore lower than the estimates based on survival statistics.
More variables were recorded for hospitalised patients. Overall, 701 patients were hospitalised during their first recorded episode, and 691 of these were registered with confirmed identity. Crude Cox regression analyses were calculated on this sub-sample: age, gender, toxic agent, educational level and marital status did not significantly affect repetition. Ethnicity did not contribute significantly, even when the groups were collapsed into nonWestern v. Western backgrounds (HR=0.6, 95% CI 0.30–1.26; P=0.18). The intention behind the poisoning did not influence repetition (overall P=0.32; none of the categories had significant values), even when corrected for gender, age and toxic agent. Daily drug or alcohol misuse alone contributed significantly (HR=1.8, 95% CI 1.22–2.86; P=0.004), but the effect disappeared in the multivariate analysis, and the variable was not included in the multivariate model. The variables predicting repetition in the multivariate model were unemployment (HR=2.9, 95% CI 1.41–6.10; P=0.004), living on social welfare (HR=2.9, 95% CI 1.58–5.40; P=0.001), a history of psychiatric treatment (HR=2.1, 95% CI 1.07–3.97; P=0.03), and a previous suicide attempt (HR=1.8, 95% CI 1.06–3.11; P=0.03) (Table 2). No interactions with gender or age were found. When analysing the time from a previous suicide attempt to the index episode, patients who had made a suicide attempt in the past 12 months repeated significantly more often than patients who had made a suicide attempt before the last 12 months (HR=2.3, 95% CI 1.26–4.04; P=0.006).
Table 2 Cox regression analysis of repetition after the first registered episode, in hospitalised patients onlya
| Crude effect | Adjusted effect | ||||||
|---|---|---|---|---|---|---|---|
| n | HR | 95% CI | P | HR | 95% CI | P | |
| Occupational status | |||||||
| Working or equivalentb | 222 | ||||||
| Sick leave | 51 | 1.15 | 0.38-3.43 | 0.81 | 0.87 | 0.29-2.62 | 0.80 |
| Unemployed | 62 | 3.06 | 1.47-6.36 | 0.003 | 2.93 | 1.41-6.10 | 0.004 |
| On social welfare | 138 | 4.07 | 2.25-7.36 | <0.001 | 2.92 | 1.58-5.40 | 0.001 |
| Other | 6 | 7.84 | 1.79-34.4 | 0.006 | 11.47 | 2.53-52.0 | 0.002 |
| Psychiatric treatmentc | 301 | 2.80 | 1.53-5.12 | 0.001 | 2.06 | 1.07-3.97 | 0.03 |
| Previous suicide attemptd | 198 | 2.66 | 1.63-4.33 | <0.001 | 1.81 | 1.06-3.11 | 0.03 |
Among patients with more than one hospitalisation (n=96), the intention changed from unintentional drug overdose to intentional self-poisoning and vice versa for 23 (24%) patients from one episode to the next, equally in both directions. Among all hospitalised patients, 619 (71%) answered the question about a previous suicide attempt, and 275 (44%) of these confirmed such an attempt. In the group with drug-misuse-related poisonings, a previous suicide attempt was confirmed by 27%.
The repetition rates for patients presenting with the significant risk factors identified in the multivariate models described above were estimated with Kaplan–Meier calculations. In the study as a whole, when the toxic agent was a sedative or opiate and the patient's age was 30–49 years, the repetition rate was 47%, which was 60% higher than the rate in the overall study population. In hospitalised patients who were unemployed or on social welfare, with a history of psychiatric treatment and a previous suicide attempt, the repetition rate was 41%, which was 52% higher than the rate in the overall hospitalised study population.
Discussion
To the best of our knowledge, our study is the first to show the repetition pattern for all acute poisonings treated both inside and outside hospital in a capital city. The estimated 1-year repetition of acute poisonings was 30%, irrespective of the intention or healthcare level. For all patients, the predictors of repetition were intoxication with opiates or sedatives and age between 30 and 49 years. The predictor variables among hospitalised patients were unemployment or living on social welfare, a previous suicide attempt, and a history of psychiatric treatment.
The 1-year repetition rate in our study is higher than the rates of 6.3–18% reported in other studies of acute poisoning Reference Goldacre and Hawton7–Reference Rafnsson, Oliver, Elton and Bateman10 and 10–16% in studies of self-harm. Reference Gunnell, Brooks and Peters3,Reference Hall, O'Brien, Stark, Pelosi and Smith4,Reference Owens, Horrocks and House6 Our 1-year rate of 30% is equal to the long-term rates (5–20 years) of other studies (28–39%), Reference Hall, O'Brien, Stark, Pelosi and Smith4,Reference Zahl and Hawton5,Reference Rafnsson, Oliver, Elton and Bateman10,Reference Gibb, Beautrais and Fergusson23–Reference Beautrais24 whereas even some 4- and 5-year follow-up studies had lower rates (15.5–21%). Reference Rygnestad16,Reference Cooper, Kapur, Webb, Lawlor, Guthrie and Mackway-Jones25,Reference Leslie, Greig, Mackie, Gotz and Morrison26 Our high repetition rate may be related to the inclusion of and follow-up in pre-hospital treatment facilities, which has not been done systematically elsewhere, and to the inclusion of drug and alcohol overdoses that were not solely intentional. Moreover, studies that do not use survival statistics may underestimate repetition rates. The rate of previous suicide attempts in our study was 44% in hospitalised patients, but other studies using the recall of previous self-harm or parasuicide have reported rates of more than 50%. Reference Batt, Eudier, Le Vaou, Breurec, Baert and Curtes27,Reference Ojehagen, Regnell and Traskman-Bendz28 Such studies also record episodes treated outside the catchment area or study institutions, and our findings are consistent with these rates.
Long-term studies indicate that the first year after poisoning or self-harm has the highest probability for repetition, Reference Hall, O'Brien, Stark, Pelosi and Smith4,Reference Owens, Horrocks and House6,Reference Rafnsson, Oliver, Elton and Bateman10,Reference Rygnestad16 and within the first year the probability is highest during the first few months. Reference Carter, Whyte, Ball, Carter, Dawson and Carr9,Reference Leslie, Greig, Mackie, Gotz and Morrison26,Reference McEvedy29 This is consistent with our findings, which show a very steep Kaplan–Meier curve in the first month.
It is a common clinical impression that the ambulance service treats more drug-misuse-related poisonings than do hospitals, and that these poisonings are subject to more repetition than intentional self-poisonings. Although not significant, slightly more repetitions were seen after index episodes treated outside hospital than inside hospital. However, surprisingly, the proportion of admissions that were repetitions was equal inside and outside hospital. We found no significant difference in the repetition rate between deliberate self-poisonings and intentional/unintentional drug-misuse-related poisonings among hospitalised patients. However, these groups are often described to considerably overlap, Reference Johnsson and Fridell12–Reference Murphy, Hawton and Van Heeringen14 and the difficulties encountered in assigning specific intentions to these patients can make such comparisons problematic. The high proportion of patients (24%) who presented in one episode with intentional self-poisoning and in another with unintentional drug-misuse-related poisoning and vice versa) emphasises the importance of broad inclusion criteria in studies of repetition patterns of acute poisoning. The fact that many patients were treated for both intentional/unintentional poisonings illustrates a possible pitfall in studies that focus solely on either intentional self-poisonings or unintentional overdoses.
Surprisingly, gender was never a significant predictor of repetition, even when corrected for other variables in the study. This confirms the results of some studies of poisoning Reference Rafnsson, Oliver, Elton and Bateman10,Reference Rygnestad16,Reference McEvedy29 and parasuicide; Reference Batt, Eudier, Le Vaou, Breurec, Baert and Curtes27,Reference Groholt, Ekeberg and Haldorsen30 however, others have shown that females tend to repeat self-harm more frequently than males. Reference Carter, Whyte, Ball, Carter, Dawson and Carr9,Reference Gibb, Beautrais and Fergusson23 The higher repetition rate for patients aged 30–49 years is consistent with other studies that have shown higher repetition rates in middle age (25–54 years). Reference Owens, Dennis, Read and Davis8,Reference Carter, Whyte, Ball, Carter, Dawson and Carr9,Reference Gibb, Beautrais and Fergusson23
Opiates and sedatives were the drugs with the highest repetition rates, consistent with another study. Reference Rafnsson, Oliver, Elton and Bateman10 However, that study reported rates for antidepressants and antipsychotics in the same range as benzodiazepines, which is inconsistent with our data. Interestingly, young people (<30 years) who overdosed with opiates had a much higher risk of repetition than that of middle-aged individuals (30–49 years) who overdosed with opiates.
Among the predictors identified in hospitalised patients, occupational status had the strongest effect on repetition. The risk was almost three times higher for those who were unemployed or living on social welfare. These categories are good markers of social deprivation. Other studies have also found unemployment Reference Owens, Dennis, Read and Davis8 or low Carstairs index of social deprivation Reference Rafnsson, Oliver, Elton and Bateman10 to be significant risk factors for repetition, and a recent study of young people found the highest rate of self-harm among those outside the labour market. Reference Young, van, Sweeting and West31 Although daily drug misuse was not significant in the multivariate analysis in our study, alcoholism increased the risk of both repetition Reference Batt, Eudier, Le Vaou, Breurec, Baert and Curtes27 and suicide Reference Cooper, Kapur, Webb, Lawlor, Guthrie and Mackway-Jones25 after self-harm in other studies. In our and other studies, Reference Owens, Dennis, Read and Davis8,Reference Beautrais24,Reference Groholt, Ekeberg and Haldorsen30 a previous suicide attempt and a history of psychiatric treatment were predictors of repetition, although we found that occupational status was a stronger predictor.
Strengths and limitations
The completeness of the inclusion of patients in these types of studies can always be questioned. However, we included patients at three levels of healthcare, and transferrals between these levels were common. This helped to make the study more complete because each patient could have been included in up to three treatment facilities during each episode. Although we censored patients who died, we did not correct for patients who may have moved away from the city during the observation period. Such adjustments would probably have increased the repetition rate. The cases not included in the repetition analyses because of missing identity constituted 10.3% of the study population, and this shortfall may weaken the analyses. However, the missing patients had more frequently overdosed with opiates and were younger than the study population as a whole. Therefore, the inclusion of this group could have increased the repetition rate, according to the findings of the Cox regression analyses. A systematic review of the repetition of self-harm Reference Owens, Horrocks and House6 made several recommendations for the design of studies of repetition patterns including: no obvious bias towards mild or severe cases; no deliberate exclusions; all admitted cases included; patients enrolled from accident and emergency departments; catchment area targeted; and statistical methods using survival statistics with censorship and a uniform at-risk period. Our study fulfilled all these criteria, but the at-risk period varied between 1 and 365 days because we did not observe patients after the inclusion period of 1 year. This was a prospective study that included several different healthcare facilities, which involved a large number of healthcare workers. Therefore, it was not practicable for us to extend the observations beyond the study year. Nevertheless, with such a large patient population, and the use of survival analyses and censorship by the end of the observation or by the date of death according to the National Death Register, we believe the methodological quality was adequate. When using Kaplan–Meier calculations to estimate repetitions, one must be cautious about the accuracy of the last part of the curve because of the few remaining patients and the high impact on the results of each new event. Altman Reference Altman and Altman32 recommended ending the calculation when only five patients remain under observation, but others have advocated curtailing the curve when only 10% are still under observation. Reference Pocock, Clayton and Altman22 In our study, the last repetition occurred 5 days before the end of the observation period, when 29 patients remained. The linearity of the curve in the last 10 months of the year strengthens this estimation.
The amount of information was obviously more comprehensive for hospitalised patients. For practical reasons, it was not possible to obtain detailed information on social status and previous psychiatric history from the ambulance service or in a crowded out-patient clinic. Furthermore, because of the breadth of the study and the number of collaborators, the questionnaires were intentionally simple and easy to complete. For example, the evaluation of suicidal v. other intentions was expressed in the usual way by describing the patients as normally done in the clinical setting, instead of using a larger, validated scheme. Toxic agents were not routinely confirmed by laboratory tests because, in most of the patients treated by the ambulance service and at the out-patient clinic, no such tests were available. Identifying toxic agents is difficult, and may be wrong in many cases. However, if such categories are shown to have value as predictive variables for repetition, classification should be made as in the usual clinical setting.
Conclusion
Repetition after acute poisoning treated at all levels of the healthcare system is high, regardless of the intention behind the poisoning. Thirty per cent of patients repeated during the first year, with the highest incidence in the first month. Predictive factors among all patients included poisoning with opiates or sedatives and an age of 30–49 years, whereas unemployment or living on social welfare, a previous suicide attempt, or a history of psychiatric treatment predicted repetition among hospitalised patients.
Acknowledgements
This study was supported by a grant from the Norwegian Directorate for Health and Social Affairs, Department for Emergency Medicine and Preparedness, and by a grant from the Eastern Norway Regional Health Authority. Our thanks go to the Oslo Ambulance Service, the Oslo Emergency Ward, Aker University Hospital, Diakonhjemmet Hospital, Lovisenberg Hospital, and Ullevaal University Hospital for their help with data collection, and to Professor Leiv Sandvik, University of Oslo, for statistical advice.







eLetters
No eLetters have been published for this article.