



Introduction
Survivors of the atomic bombings of Hiroshima and Nagasaki, Japan, experienced extreme physical and emotional distress (Oughterson and Warren, Reference Oughterson and Warren1956; Lifton, Reference Lifton2012). Research among survivors has primarily focused on physical health effects and has established significant associations of radiation dose from the atomic bombings with increased risk of leukaemia, solid cancer and non-cancer diseases (Yamada et al., Reference Yamada, Wong, Fujiwara, Akahoshi and Suzuki2004; Ozasa et al., Reference Ozasa, Shimizu, Suyama, Kasagi, Soda, Grant, Sakata, Sugiyama and Kodama2012; Hsu et al., Reference Hsu, Preston, Soda, Sugiyama, Funamoto, Kodama, Kimura, Kamada, Dohy, Tomonaga, Iwanaga, Miyazaki, Cullings, Suyama, Ozasa, Shore and Mabuchi2013; Grant et al., Reference Grant, Brenner, Sugiyama, Sakata, Sadakane, Utada, Cahoon, Milder, Soda, Cullings, Preston, Mabuchi and Ozasa2017). The psychological sequelae of the atomic bombings have been characterised to a lesser extent (Zwigenburg, Reference Zwigenburg2019).
Early small surveys of atomic bomb survivors reported neurosis, somatisation and other symptoms consistent with post-traumatic stress reactions (Tsuiki et al., Reference Tsuiki, Ueno, Segawa and Kaburagi1951; Konuma et al., Reference Konuma, Furutani and Kubo1953; Nishikawa and Tsuiki, Reference Nishikawa and Tsuiki1961). Higher symptom frequencies were observed among survivors who experienced acute radiation sickness and those in closer proximity to each blast's hypocentre (Konuma, Reference Konuma1956, Reference Konuma1967). More recently, several retrospective studies, including larger surveys, have emphasised the persistent nature of these psychological repercussions. One study found that 73.5% of surveyed survivors were at high risk for mood or anxiety disorders 45 years after the bombings (Kim et al., Reference Kim, Tsutsumi, Izutsu, Kawamura, Miyazaki and Kikkawa2011). Others observed excess risk for mental disorders driven by acute symptom presence, loss of family members due to the bombings and painful experiences from social stigma (Ohta et al., Reference Ohta, Mine, Wakasugi, Yoshimine, Himuro, Yoneda, Yamaguchi, Mikita and Morikawa2001; Honda et al., Reference Honda, Shibata, Mine, Imamura, Tagawa, Nakane and Tomonaga2002; Yamada and Izumi, Reference Yamada and Izumi2002; Asukai et al., Reference Asukai, Sugiyama, Kato, Nakajima and Saeki2012). Importantly, epidemiological studies conducted in other populations exposed to psychologically traumatic events, but not radiation, have linked elevated rates of post-traumatic stress disorder and depression with increased suicide risk (Ferrada-Noli et al., Reference Ferrada-Noli, Asberg, Ormstad, Lundin and Sundbom1998; Bernal et al., Reference Bernal, Haro, Bernert, Brugha, de Graaf, Bruffaerts, Lépine, de Girolamo, Vilagut, Gasquet, Torres, Kovess, Heider, Neeleman, Kessler and Alonso2007; Rytwinski et al., Reference Rytwinski, Scur, Feeny and Youngstrom2013).
The Life Span Study is a large, well-defined longitudinal cohort study of atomic bomb survivors that was established in 1950 to determine the long-term risks of cancer and other diseases due to radiation exposure from the atomic bombings (Ozasa et al., Reference Ozasa, Cullings, Ohishi, Hida and Grant2019). Previously, suicide mortality was examined in relation to radiation dose, which is not known to survivors, and risk was not assessed by age, sex or other factors (Shimizu et al., Reference Shimizu, Pierce, Preston and Mabuchi1999). In this study, we evaluated suicide mortality among atomic bomb survivors in relation to measures of exposure severity experienced by survivors at the time of or shortly after the bombings. We hypothesised that closer proximity to the hypocentre, lack of shielding to the blast and the occurrence of acute injuries would be associated with greater psychological impact and, thus, with higher risk of suicide death.
Methods
Study cohort
The Life Span Study includes 93 741 atomic bomb survivors who were located within 10 km of the hypocentre in either Hiroshima or Nagasaki at the time of the bombings (6 August and 9 August 1945, respectively) and 26 579 residents of Hiroshima and Nagasaki who were not in either city (or, not-in-city) at the time of the bombings (Ozasa et al., Reference Ozasa, Cullings, Ohishi, Hida and Grant2019). Survivors were recruited through a supplementary survey to the 1950 National Census of Japan; their follow-up began on 1 October 1950. Not-in-city residents were recruited through surveys conducted by the Atomic Bomb Casualty Commission in 1950 and 1951, and resident surveys by Nagasaki and Hiroshima cities in 1950 and 1953, respectively, and matched to proximal survivors (within 2 km) on city, sex and age. For not-in-city residents, follow-up began on 1 October 1950, 1 October 1951 or 1 June 1953. Follow-up continued until the date of death obtained from the Japanese National Family Registry system, which is virtually complete. Censoring events were emigration from Japan, aged 110 years or the end of the study period on 31 December 2009. After excluding 86 participants with unknown permanent residence and three participants whose death date was at or before the beginning of follow-up, the analysis cohort included 120 231 participants.
Cause of death
For deceased participants, cause of death was obtained from death certificates and classified according to the International Classification of Diseases (ICD), Revision 7 to Revision 10. ICD codes E970–E979 (Revision 7); E950–E959 (Revision 8); E950–E959 (Revision 9) and X60–X84, Y84.0 (Revision 10) were classified as suicide death. ICD codes E800–E965, E980–E999 (Revision 7); E800–E949, E960–E999 (Revision 8); E800–E949, E960–E999 (Revision 9) and V01–X59, X85–Y36, Y87.1, Y87.2, Y40–Y86, Y88, Y89 (Revision 10) were classified as death due to external causes other than suicide.
Measures of exposure severity
We used several measures of exposure severity as indirect measures of psychological trauma arising from exposure to the atomic bombings: proximity to the hypocentre, type of shielding between the survivor and the blast and self-reported occurrence of acute radiation and thermal injuries among survivors; and time of entry into the cities after the bombings among not-in-city residents.
Proximity to the hypocentre and type of shielding were determined from questionnaires (1949–1963) to survivors or their surrogates regarding survivors' location at the time of the bombings (Cullings et al., Reference Cullings, Fujita, Funamoto, Grant, Kerr and Preston2006). Location data were recently improved through review of the original questionnaires, modernisation of mapping techniques and correction for other errors (Cullings et al., Reference Cullings, Grant, Egbert, Watanabe, Oda, Nakamura, Yamashita, Fuchi, Funamoto, Marumo, Sakata, Kodama, Ozasa and Kodama2017). Proximity was categorised based on maps produced by the U.S. Strategic Bombing Survey that indicated the extent of fire and blast damage (0 to <1.8, 1.8 to <3.4, 3.4 to <5, 5 to 10 km); proximity was also modelled as a continuous variable such that contrasts were per km closer to the hypocentre. Shielding was categorised as inside any structure (e.g. wooden house or concrete building), outside or unknown. Occurrence of acute radiation injuries (skin epilation that occurred within 2 months, oropharyngeal lesions that occurred within 2 months and flash burns produced by thermal radiation from the blast) was obtained from baseline surveys (1953–1961), as in previous studies (Ozasa et al., Reference Ozasa, Sakata, Cullings and Grant2016). Among not-in-city residents, time of entry into the cities was recorded from baseline surveys (1955–1961) and categorised as early v. late entry (⩽30, >30 days).
We did not use estimated radiation dose as an indirect measure of psychological trauma because radiation doses, unlike proximity to and shielding from the blast, are not generally known to survivors; radiation doses are unknown for ~15% of proximal survivors due to complex shielding situations that are not accommodated by the dosimetry system used to estimate radiation doses; there is no heterogeneity in estimated radiation doses among survivors located beyond 3 km from the hypocentre (Cullings et al., Reference Cullings, Grant, Egbert, Watanabe, Oda, Nakamura, Yamashita, Fuchi, Funamoto, Marumo, Sakata, Kodama, Ozasa and Kodama2017); and we are not aware of any biological basis for an association between radiation dose and suicide risk.
Covariates
Demographic characteristics included city (Hiroshima or Nagasaki), sex and age at the time of the bombings, which is equivalent to birth year because all survivors were exposed in 1945. We evaluated education level (less than high school, high school, more than high school, unknown) and marital status (single, married, separated or divorced, widowed, unknown) because these are known risk factors for suicide death that could vary between survivors exposed in different locations and not-in-city residents. Data on education level and marital status were obtained from in-clinic questionnaires (1963, 1965, 1968) and mailed surveys (1965, 1969, 1978, 1991); 60.0% of participants responded at least once. To avoid bias from over-counting time at risk in known categories, participants were classified as having unknown status until the date at which they first provided information on education level or marital status.
Statistical methods
Unadjusted mortality rates were calculated across exposure and covariate strata. Cox regression models, with age as the time scale, estimated adjusted associations with the hazard (risk) of suicide death (Cox, Reference Cox1972; Cologne et al., Reference Cologne, Hsu, Abbott, Ohishi, Grant, Fujiwara and Cullings2012). All models included city, sex, age at bombing, education level and marital status. In analyses focused on exposures among atomic bomb survivors, not-in-city residents were included in a separate stratum to inform covariate adjustment, and vice versa (Cologne and Preston, Reference Cologne and Preston2001; French et al., Reference French, Cologne, Sakata, Utada and Preston2017). Adjustment for age at bombing was determined from exploratory data analysis and by comparing the Akaike information criterion between models with parsimonious specifications (i.e. linear, linear-quadratic) and natural cubic splines. Separate models were fit for proximity to the hypocentre (categorical and continuous) and shielding, each acute injury and entry time. Models for acute injuries were adjusted for proximity to the hypocentre and shielding.
Given that the effect of exposure to trauma can differ between women and men (Bale and Epperson, Reference Bale and Epperson2015), all analyses were stratified by sex. Based on prior studies that reported associations of trauma exposure during childhood and adolescence with mental health disorders and suicide attempts in adulthood (Kessler et al., Reference Kessler, McLaughlin, Green, Gruber, Sampson, Zaslavsky, Aguilar-Gaxiola, Alhamzawi, Alonso, Angermeyer, Benjet, Bromet, Chatterji, de Girolamo, Demyttenaere, Fayyad, Florescu, Gal, Gureje, Haro, Hu, Karam, Kawakami, Lee, Lépine, Ormel, Posada-Villa, Sagar, Tsang, Ustün, Vassilev, Viana and Williams2010; Angelakis et al., Reference Angelakis, Gillespie and Panagioti2019), we also explored effect modification by age at bombing, with a focus on young survivors. Categorisation of age at bombing was based on a combination of focusing on survivors who might be at highest risk (<25 years), while having a sufficient sample size (and corresponding number of events and degrees of freedom) to allow detailed multivariable modelling. Thus, some analyses were based on finer age categories (e.g. <15 and 15 to <25 years when analysing suicide risk by proximity) compared to the other analyses (e.g. <25 years when analysing suicide risk by shielding and occurrence of flash burns).
Deaths due to external causes other than suicide were not suspected to be associated with measures of exposure severity and were therefore analysed as a negative control outcome. Weighted residuals were used to evaluate the proportional hazards assumption (Grambsch and Therneau, Reference Grambsch and Therneau1994); no violations were noted. Statistical hypotheses regarding regression parameters were evaluated using likelihood ratio statistics. All analyses were completed using R 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The analysis cohort consisted of 120 231 participants (70 092 women and 50 139 men), including 93 665 atomic bomb survivors and 26 566 not-in-city residents, observed for a total of 4 876 970 person-years. During the 60-year follow-up period, 1150 suicide deaths – 510 among women and 640 among men – were recorded. The unadjusted suicide rate per 100 000 person-years was 23.6 overall, 17.2 among women and 33.6 among men (Table 1). The median age at suicide was 59.1 (inter-quartile range: 40.2, 72.4) years among women and 54.6 (inter-quartile range: 39.3, 65.7) years among men. Among men, suicide rates peaked at 42.8 and 44.3 per 100 000 person-years in 1955–1959 and 1980–1984, respectively (online Supplementary Figs S1, S2). In contrast, suicide rates among women generally declined over calendar time.
Table 1. Unadjusted rates and adjusted HRs for suicide death, by demographic characteristics, Life Span Study, 1950–2009
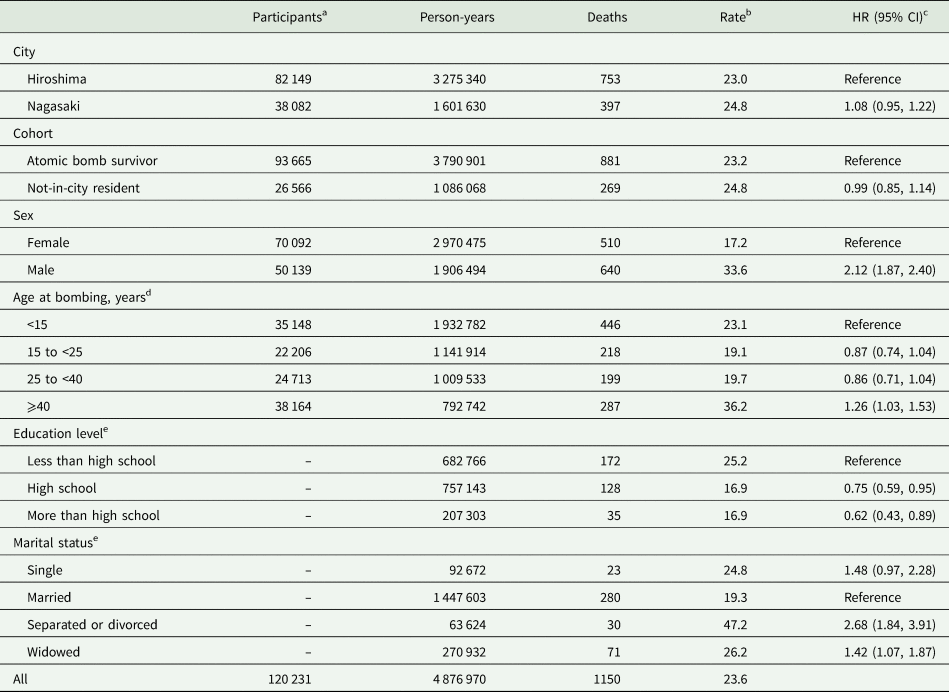
CI, confidence interval; HR, hazard ratio.
a Number of participants is not provided for time-dependent variables.
b Per 100 000 person-years.
c Adjusted for all other variables listed.
d Age at bombing is equivalent to birth year because all survivors were exposed in 1945.
e Numbers do not sum to total because results for unknown categories are not included.
A mutually adjusted model indicated significantly higher suicide risk among men compared to women, participants who were separated or divorced or widowed compared to married, and participants ⩾40 years of age at the time of the bombings (i.e. born ⩽1905) (Table 1). Higher levels of education were associated with significantly lower suicide risk. There was no difference in suicide risk between atomic bomb survivors and not-in-city residents.
A majority of survivors (73 864, or 78.9%) were located within 3.4 km of the hypocentre (online Supplementary Table S1). Survivors at proximal locations were more likely to be shielded indoors compared to survivors at distal locations because shielding was required for survival from the blast (Jablon et al., Reference Jablon, Ishida and Yamasaki1965). Survivors at proximal locations were also more likely to report acute radiation injuries compared to survivors at distal locations because proximal survivors were exposed to higher radiation doses. Survivors who reported epilation were also likely to report oropharyngeal lesions and flash burns, but there was not a strong association between oropharyngeal lesions and flash burns.
Measures of exposure severity and risk of suicide
There was no association between proximity to the hypocentre – as either a categorical or continuous variable – and risk of suicide death (Table 2). Compared to survivors shielded inside any structure at the time of the bombings, a non-significant increase in suicide risk was observed among those outside, with evidence of heterogeneity by age at bombing (p = 0.054). Increased suicide risk was observed for survivors outside v. shielded inside among those <25 years of age (hazard ratio (HR): 1.24; 95% confidence interval (CI): 1.03, 1.48), but not among those ⩾25 years of age (HR: 0.94; 95% CI: 0.75, 1.18).
Table 2. Unadjusted rates and adjusted HRs for suicide death, by measures of exposure severity, Life Span Study, 1950–2009
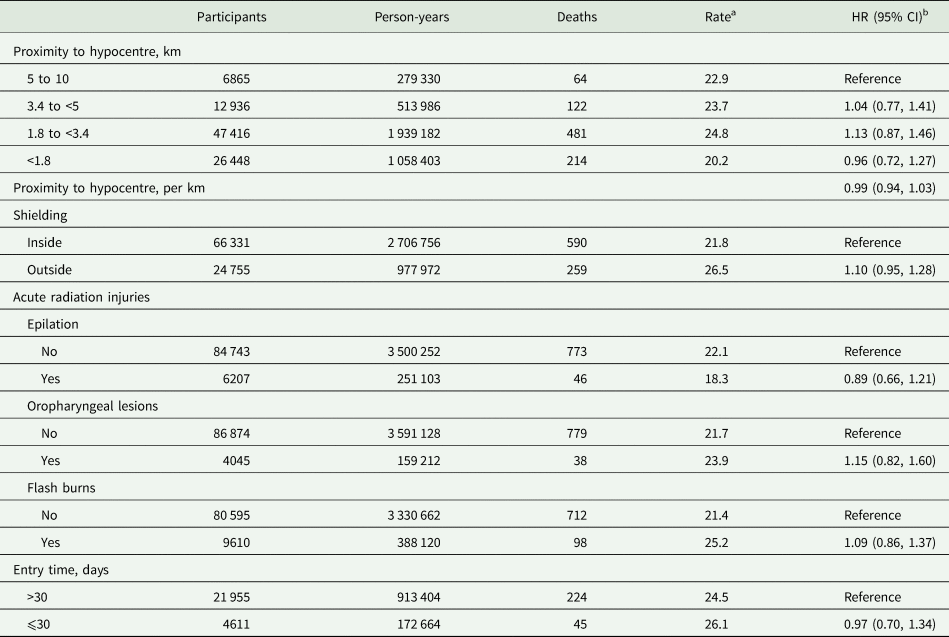
CI, confidence interval; HR, hazard ratio.
a Per 100 000 person-years.
b Adjusted for city, cohort, sex, age at bombing (linear-quadratic), education level and marital status. Models for acute radiation injuries are also adjusted for proximity to hypocentre and shielding.
Self-reported occurrence of epilation, oropharyngeal lesions and flash burns was not associated with suicide risk (Table 2). Small numbers of suicide deaths among survivors who reported epilation and oropharyngeal lesions precluded more detailed modelling. However, there was significant heterogeneity by age at bombing in the association of flash burns with suicide risk (p = 0.025). Flash burns were associated with increased suicide risk among survivors <25 years of age (HR: 1.32; 95% CI: 1.00, 1.73), but not among those ⩾25 years of age (HR: 0.80; 95% CI: 0.56, 1.16).
Among not-in-city residents, there were no differences in suicide risk by entry time (Table 2).
Sex-stratified analyses of suicide risk
Sex-specific unadjusted rates of suicide death by proximity to the hypocentre among atomic bomb survivors and by entry time among not-in-city residents are shown in Fig. 1. Closer proximity to the hypocentre was associated with a non-significant increase in suicide risk among women (Table 3). There was evidence of heterogeneity by age at bombing (p = 0.067), with a positive association between proximity and suicide risk among women <15 years of age (HR: 1.09 per km; 95% CI: 1.00, 1.18). A finer categorisation for age at bombing revealed a significant association among women 10 to <15 years of age (HR: 1.10 per km; 95% CI: 1.02, 1.20), but not <10 years of age (HR: 1.06 per km; 95% CI: 0.97, 1.16). Among men, closer proximity was associated with decreased suicide risk, with no evidence of heterogeneity by age at bombing (p = 0.50).

Fig. 1. Unadjusted rates of suicide death, by proximity to the hypocentre (among atomic bomb survivors) and entry time (among not-in-city residents) and stratified by sex, Life Span Study, 1950–2009.
Table 3. Adjusted HRs for suicide death, by measures of exposure severity and stratified by sex, Life Span Study, 1950–2009
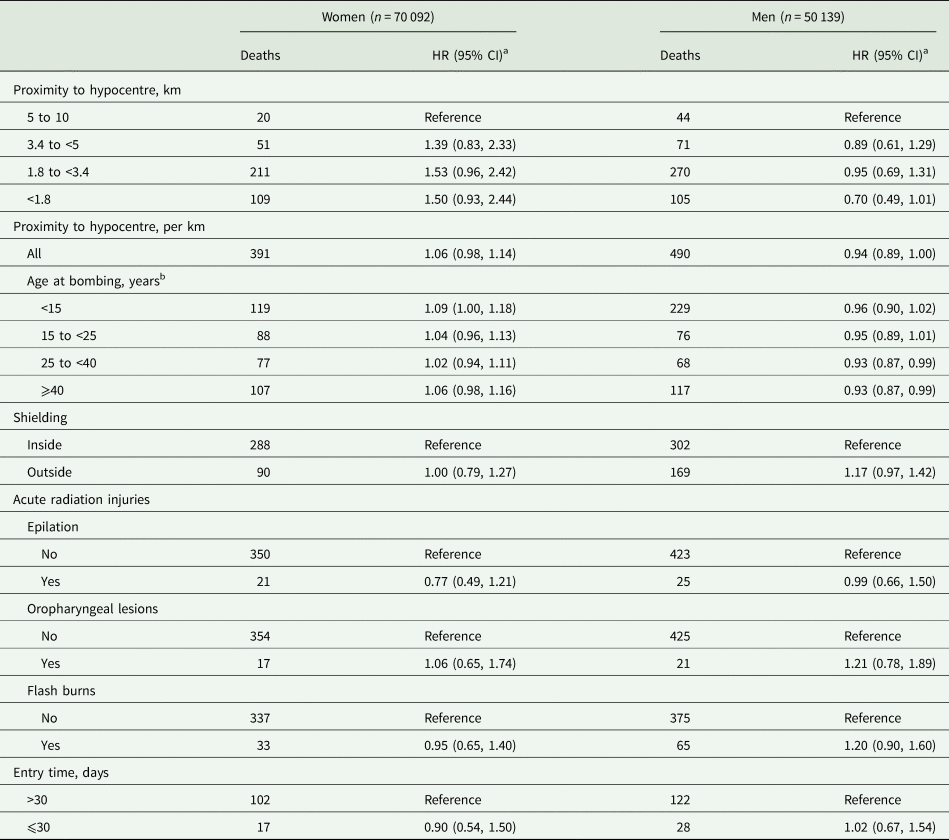
CI, confidence interval; HR, hazard ratio.
a Adjusted for city, cohort, age at bombing (linear-quadratic), education level and marital status. Models for acute radiation injuries are also adjusted for proximity to hypocentre and shielding.
b Likelihood ratio p value for evaluating the null hypothesis of equality in HRs across age groups (3 degrees of freedom): women, p = 0.067; men, p = 0.50.
Among men, a non-significant increase in suicide risk was observed among those who were outside compared to those shielded inside (Table 3), with significant heterogeneity by age at bombing (p = 0.047). Increased suicide risk was observed for men outside compared to men shielded inside among those <25 years of age (HR: 1.34; 95% CI: 1.07, 1.68), but not among those ⩾25 years of age (HR: 0.93; 95% CI: 0.68, 1.26). There was no association of shielding with suicide risk among women, and there was no evidence of heterogeneity by age at bombing (p = 0.64).
There was a non-significant increase in suicide risk among men who reported flash burns, but not among women (Table 3). Of note, an association of flash burns with increased suicide risk among survivors <25 years of age was observed among men (HR: 1.41; 95% CI: 1.00, 1.98), but not among women (HR: 1.22; 95% CI: 0.77, 1.94).
Risk of death due to other external causes
During the follow-up period, there were 2549 deaths due to other external causes (unadjusted rate of 52.3 per 100 000 person-years). Descriptive results for deaths due to other external causes are provided in online Supplementary Table S2 and Figs S3, S4. There was no evidence of a positive association between proximity and risk of death due to other external causes overall, among women or men and no evidence of heterogeneity by age at bombing among either sex (online Supplementary Tables S3, S4). There was also no evidence of association between shielding, acute radiation injuries including flash burns or entry time with risk of death due to other external causes.
Discussion
In this large cohort study of atomic bomb survivors, our analysis suggested no statistically significant associations between measures of exposure severity, as indirect measures of psychological trauma, and suicide mortality. Overall, closer proximity to the hypocentre, lack of shielding to the blast and the occurrence of acute injuries were not associated with increased suicide risk. Despite previous studies that associated these factors with harmful psychological consequences among atomic bomb survivors (Konuma, Reference Konuma1956, Reference Konuma1967; Ohta et al., Reference Ohta, Mine, Wakasugi, Yoshimine, Himuro, Yoneda, Yamaguchi, Mikita and Morikawa2001; Honda et al., Reference Honda, Shibata, Mine, Imamura, Tagawa, Nakane and Tomonaga2002; Yamada and Izumi, Reference Yamada and Izumi2002; Kim et al., Reference Kim, Tsutsumi, Izutsu, Kawamura, Miyazaki and Kikkawa2011; Asukai et al., Reference Asukai, Sugiyama, Kato, Nakajima and Saeki2012), these consequences were not reflected in increased risk for suicide completion in our study. One possible explanation for the lack of association is that, while survivors located in distal regions (i.e. beyond 2–3 km from the hypocentre) and not-in-city residents were enrolled in the Life Span Study as internal and external comparison groups for radiation exposure, pervasive deprivation and reduced living standards throughout Japan during and after the war could have increased suicide rates among these comparison groups, as well (Yamashita, Reference Yamashita2015).
In sex- and age-stratified analyses, suicide risk was elevated among young men (<25 years of age) who were outside at the time of the bombings or reported flash burns and among young women (<15 years of age) who were closer to the hypocentre. The lack of positive association between measures of exposure severity and risk of death due to other external causes supports the validity of these findings. A previous examination of suicide mortality in the Life Span Study (1950–1990) identified, counter-intuitively, an inverse association between suicide likelihood and radiation dose (Shimizu et al., Reference Shimizu, Pierce, Preston and Mabuchi1999). Our results, based on extended follow-up and additional data from young survivors, indicate that youth may be particularly sensitive to psychological trauma that manifests in elevated suicide risk. These results are consistent with prior studies that reported higher sensitivity to trauma among children and adolescents, particularly in the period prior to and during puberty (De Bellis and Zisk, Reference De Bellis and Zisk2014; Marshall, Reference Marshall2016; Kuhlman et al., Reference Kuhlman, Chiang, Horn and Bower2017). Coupled with other studies, our results suggest the importance of long-term monitoring of mental health among young populations exposed to catastrophic events or mass trauma such as war, terrorism or natural disasters (North et al., Reference North, Oliver and Pandya2012; Kõlves et al., Reference Kõlves, Kõlves and De Leo2013; Orengo-Aguayo et al., Reference Orengo-Aguayo, Stewart, de Arellano, Suárez-Kindy and Young2019).
It is unclear why measures of exposure severity are differentially associated with suicide risk between young women and men (i.e. proximity to the hypocentre among women, outside exposure or the occurrence of flash burns among men). These differences might suggest a greater sensitivity to visually traumatic or painful experiences among men compared to women, differential recall, gender differences in emotion regulation or an alternative explanation (Canli et al., Reference Canli, Desmond, Zhao and Gabrieli2002; McRae et al., Reference McRae, Ochsner, Mauss, Gabrieli and Gross2008; Nolen-Hoeksema, Reference Nolen-Hoeksema2012; Bale and Epperson, Reference Bale and Epperson2015). Studies in other populations exposed to war-related trauma found high prevalence of post-traumatic stress disorder among boys and girls with lasting negative impact, but did not evaluate suicidal behaviour or suicide mortality (Attanayake et al., Reference Attanayake, McKay, Joffres, Singh, Burkle and Mills2009; Kletter et al., Reference Kletter, Rialon, Laor, Brom, Pat-Horenczyk, Shaheen, Hamiel, Chemtob, Weems, Feinstein, Lieberman, Reicherter, Song and Carrion2013). The best available evidence on suicide risk following early-life trauma comes from studies of physical, mental or sexual abuse (Angelakis et al., Reference Angelakis, Gillespie and Panagioti2019); it is unclear, however, if these findings can be generalised to atomic bomb survivors.
Historically, rates of suicide in Japan have been high, but have declined in recent years (World Health Organization, 2017). Our results are consistent with these trends. Similar to studies conducted among general Japanese populations, our findings confirmed several demographic risk factors for suicide death (Nock et al., Reference Nock, Borges, Bromet, Cha, Kessler and Lee2008; Inoue et al., Reference Inoue, Tanii, Mori, Nishimura, Hara, Nishida, Nata and Ono2011; Yamauchi et al., Reference Yamauchi, Fujita, Tachimori, Takeshima, Inagaki and Sudo2013; Kimura et al., Reference Kimura, Iso, Honjo, Ikehara, Sawada, Iwasaki and Tsugane2016). Specifically, an education level of high school or more was associated with lower suicide risk, whereas male sex and separated, divorced or widowed marital status were associated with elevated risk.
Strengths of our study include the long and nearly complete follow-up of the unique and well-defined Life Span Study cohort, which allowed us to characterise suicide risk throughout the lifetime of atomic bomb survivors. We examined several measures of exposure severity, including those based on overt observation (i.e. acute injuries) and those based on perception (i.e. proximity, shielding). Large numbers of women and men across a wide range of birth years facilitated detailed estimation of risk differences by sex and age.
We acknowledge the following limitations. First, no data are available on deaths that occurred from August 1945 to October 1950. Previous studies on the aftermath of disasters suggest a delayed increase in suicidality that peaks within 1 year; however, a return to pre-disaster levels has typically been observed shortly thereafter (North et al., Reference North, Oliver and Pandya2012; Matsubayashi et al., Reference Matsubayashi, Sawada and Ueda2013; Ohto et al., Reference Ohto, Maeda, Yabe, Yasumura and Bromet2015; SAMHSA Disaster Technical Assistance Center, 2015). Therefore, survival bias could not be excluded (Pierce et al., Reference Pierce, Vaeth and Shimizu2007). Second, we used information from baseline questionnaires regarding radiation exposure to define measures of exposure severity as indirect measures of psychological trauma, rather than direct measures such as the CAPS-5 and IES-R (Weiss, Reference Weiss, Wilson and Tang2007; Weathers et al., Reference Weathers, Bovin, Lee, Sloan, Schnurr, Kaloupek, Keane and Marx2018). It is possible that the selected measures do not capture the full spectrum of psychological trauma experienced by survivors. Third, reporting errors due to recall bias or other factors could not be excluded because participants self-reported information retrospectively. In particular, misreporting of location (specifically, proximity to the hypocentre) could depend on sex; for example, women, especially those at or before child-bearing age, might be more concerned about discrimination due to radiation exposure. Therefore, estimated associations could be biased towards the null. In addition, there could also be error in survivors' self-reporting of acute radiation and thermal injuries. However, our goal was not to quantify acute radiation syndrome, but rather survivors' perception of their exposure severity and their psychological reaction to it. Finally, although this study adds unique data to the literature regarding trauma-associated psychological sequelae among non-Western populations, the results might not directly generalise to other populations.
Conclusion
Proximity to the hypocentre, shielding and history of acute injuries do not generally appear to influence risk for suicide death among atomic bomb survivors. However, heterogeneity may exist by age and sex, with younger survivors potentially more sensitive to trauma. The results of our analysis should not be used to discount the pain and suffering experienced by many survivors.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S204579602100024X.
Data
Data may be made available to qualified researchers upon request by submitting an inquiry at http://www.rerf.or.jp/en/contact/rinfo-en/.
Acknowledgements
None.
Financial support
The Radiation Effects Research Foundation, Hiroshima and Nagasaki, Japan, is a public interest incorporated foundation funded by the Japanese Ministry of Health, Labour and Welfare and the US Department of Energy. The research was also funded in part through Department of Energy award DE-HS0000031 to the National Academy of Sciences and through the Japan–United States Educational Commission. The views of the authors do not necessarily reflect those of the two governments.
Conflict of interest
None.
Ethical standards
This publication was supported by Radiation Effects Research Foundation research protocol 1–75, which was approved by the Human Investigation Committee of the Radiation Effects Research Foundation. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000.






 Open access
Open access