



The number of employees in shift work is increasing. Shift work is defined as, ‘any method of organizing shift work, whereby workers succeed each other on the same workstations according to a given pattern’(1). Globally, approximately 20 % of the overall workforce is engaged in a shift work pattern(2,Reference Straif, Baan and Grosse3) .
Shift work affects circadian rhythm and metabolic functions, including melatonin and cortisol levels(Reference Desantis, Diez-Roux and Hajat4–Reference Manenschijn, Van Krg and Jong7), and as expected, studies have identified a higher prevalence of obesity, metabolic syndrome and other chronic diseases among populations of shift workers(Reference Brum, Filho and Schnorr8–Reference Canuto, Pattussi and Macagnan11). In addition, certain work-related risk behaviours such as irregular food consumption, low level of physical activity, lack of sleep routines, smoking and excessive consumption of alcoholic beverages may further aggravate the health damage caused by this life routine(Reference Roenneberg, Justice and Merrow12,Reference Souza, Sarmento and De Almeida13) .
Women appear to be more affected by shift work with increased abdominal obesity (AO) compared with men. In female shift workers, a dose–response relationship was observed in one study that estimated that for every 10 years in shift work, there is a 10 % increase in elevated waist circumference (WC) (OR 1·10; 95 % CI 1·01, 1·20)(Reference Guo, Rong and Huang9). A meta-analysis showed that among shift workers, women were more likely to be obese than men (OR 1·25; 95 % CI 1·17, 1·34)(Reference Sun, Feng and Wang14).
The extent of the problems experienced by Brazilian female shift workers has been poorly studied, and shift work may be a susceptible factor to unfavourable behaviour. Hence, the aim of this study was to explore the association between behavioural characteristics with the prevalence of AO among female shift workers in Southern Brazil.
Methods
A cross-sectional study was conducted among female shift workers of a large plastic utensils manufacturing facility located in Southern Brazil. Female employees working in the factory’s production line, in the same occupation, were eligible to be studied if they were over 18 years old, were permanent employees and had been working fixed shifts for more than 3 months on the production line. Pregnant women were excluded from the study.
Data on socio-economic, demographic, work schedule and behavioural characteristics were collected using standardised, pre-coded, pre-tested questionnaires used by trained interviewers. All interviews were conducted on the factory during work hours between June and August 2017.
The socio-demographic characteristics included age (18–30, 31–40 or 41–61 years), self-reported skin colour in these categories (white, black, yellow, brown, indigenous or other), after categorised (white or no white), marital status (having a partner or not) and educational level (≤8, 9–11 or ≥12 full years of formal schooling).
The work schedule was provided by the company and confirmed by the workers during the interview. Shift workers were classified as hybrid shift workers (shifts between morning/afternoon 07.00 and 14.00 hours or afternoon/evening 14.00 to 22.00 hours) or night shift workers (22.00 to 07.00 hours). The period of time (in months) that the employee worked in the current shift was categorised ≤3, 4–6 or >6 years.
Behavioural factors included self-reported smoking status (current smoker, former smoker or non-smoker). Women were asked about which meals (breakfast, snack, lunch, snack, dinner, supper, snack during the sleep or another) they had during a normal day; the order of the meals since waking up, the usual number of meals per day (categorised ≤3 or >3); use of sleep medication (yes or no); self-reported usual hours of sleep (categorised ≤5 or >5 h) and physical activity (when commuting and/or leisure time; yes or no); we used a questionnaire that was validated by Craig and collaborators(Reference Craig, Marshall and Sjostrom15).
Anthropometric measures were obtained by trained study coordinators and supervisors. AO was estimated using WC, measured in cm at the midpoint between the iliac crest and lowest rib using a non-stretching measuring tape, with readings performed on exhalation(16). The average of two consecutive measures was obtained in duplicate by the same researcher, and the average was calculated between both measures. WC was used to classify women as having AO (WC ≥ 88 cm) or no AO (WC < 88 cm).
Data quality (questionnaire) was assessed via phone interviews using a simplified version of the original questionnaire, including items that could not have changed in the time elapsed since the original interviews, in a random sub-sample corresponding to 10 % of the study participants.
Data were double entered (EPI-DATA version 3.1). Bivariate and multivariate analyses were performed using STATA version 12.0 (StataCorp). χ 2 tests were used to assess the statistical significance of the associations between the outcome and exposures of interest. Prevalence ratios and their respective 95 % CI were estimated using Poisson regression with robust error variance.
The multivariate analysis included only those variables which were associated with AO on bivariate analysis with P-value ≤ 0·20. A conceptual multivariable analysis model(16) was used for variables adjusted among themselves at each level: distal at the first level (demographic and socio-economic variables), intermediate at the second level (work variables) and proximal at the third level (behavioural variables). Associations were considered significant when the probability level was ≤5 % (P < 0·05).
Results
The company employed 480 female workers, but thirty of them were considered as losses because they were not in the company on the day of data collection three times or refused to participate in the survey. The final sample consisted of 450 female shift workers with average age 36 ± 9 years, 18–61 years.
Characteristics of the participants are shown in Table 1. Most women in the sample were older than 30 years, did not engage in physical activity for leisure, slept more than 5 h/d, were non-smoker, had more than three meals per day (60·9 %) and worked in hybrid shift work. The prevalence of sleep privation (hours of sleep ≤5) was higher among night shift workers (54·0 %). A larger number of women (42·0 %) working night shifts had three or less meals a day.
Table 1 Sample characteristics and the prevalence of abdominal obesity according to sociodemographic, behavioural characteristics among women workers in Southern Brazil (n 450)

* Column percentage.
† P value from linear by linear association.
‡ P value from t test.
§ P value from χ 2 test.
The prevalence of the AO in the women shift workers was 44·5 % (95 % CI 40·0–49·2 %), 56·1 % comparing to 40·9 %, respectively, in night shift workers and hybrid shift workers (P = 0·006). AO prevalence was higher with the increase of age, having a partner, lower schooling, former smoking, less active, fewer (three or less) meals per day, working night shift, longer employment time and sleeping <5 h/d (Table 1).
Table 2 shows the crude and adjusted prevalence ratios of AO. After adjustments for covariates, the prevalence of AO was greater among women with more than 30 years comparing with those aged 30 years or less. Women who were current smoker had a 46 % less prevalence of AO (95 % CI 0·32, 0·90) compared with those who never smoked. Physical activity was associated with a 29 % less prevalence of AO (95 % CI 0·54, 0·95) compared with sedentary. Women who had three or fewer meals per day had a 46 % more prevalence of AO (95 % CI 1·17, 1·82) compared with those eating more frequent meals. In the adjusted model, education level, working time and hours of sleep have lost their association with AO. Night shift work was associated with increase in AO prevalence compared with hybrid shift (PR 1·33; 95 % CI 1·08, 1·64).
Table 2 Crude and adjusted prevalence ratios (PR) of abdominal obesity according to socio-demographic and behavioural variables in a sample of women shift workers in Southern Brazil (n 450)
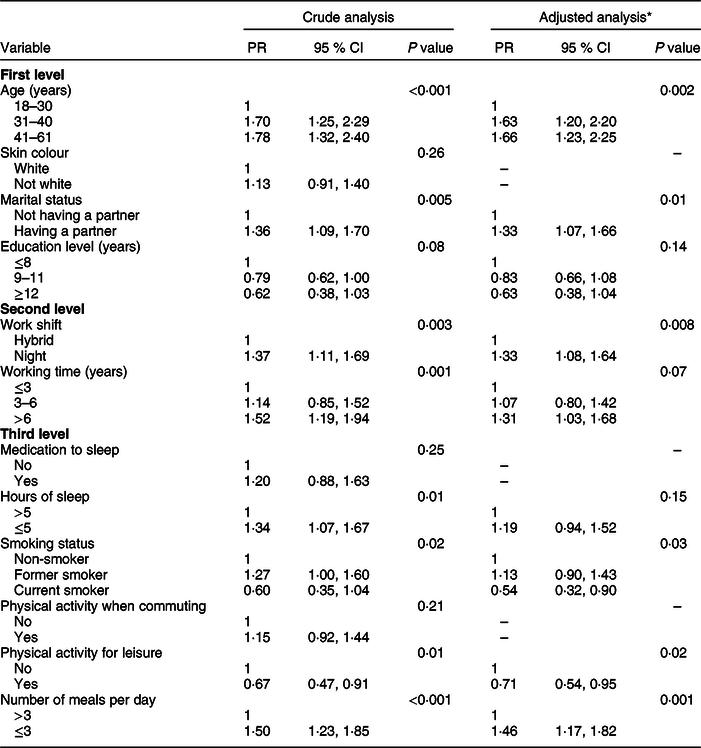
* First level: demographic variables; second level: first level + shift work and working time; third level: second + behavioural variables.
Figure 1 shows the adjusted association between hours of sleep and number of meals, and AO, stratified by shift work. The prevalence of AO was 45 % higher among night workers who had five or fewer hours of sleep per day than those had five or more hours of sleep. AO was higher among night shift workers who had fewer meals per day (three or less) compared with those eating more frequently, with statistical significance.

Fig. 1 Prevalence ratios (PR) of abdominal obesity stratified by shift work according to hours of sleep and number of meals in a sample of women workers in Southern Brazil (n 450). Model adjusted between hours of sleep and number of meals per day plus demographic, socio-economic and behavioural variables. ![]() , Night workers;
, Night workers; ![]() , day workers
, day workers
Discussion
Our findings showed high prevalence of AO in Brazilian shift working women. In the adjusted analysis, the prevalence was associated with increased age, having a partner, being less active, having fewer (three or less) meals per day and working night shift. The prevalence of AO was lower among smokers compared with non-smokers. When we stratified the analysis for shift work, behavioural characteristics (number of meals and hours of sleep) were more associated with AO in night workers.
The prevalence of AO found in our study was lower than that found in an earlier study in Southern Brazil 59·9 % (95 % CI 56·4–63·3)(Reference Canuto, Pattussi and Macagnan11) and in a study in Canada with female hospital employees, 70·3 % of the night workers and 64·3 % of the hybrid workers had AO(Reference Lajoie, Aronson and Day18). However, the prevalence of AO in the present study was higher than that observed in Poland, 31 % of nurses in a rotating shift with AO and 32 % in daytime workers had AO(Reference Peplonska, Bukowska and Sobala19). In addition, there are still few studies that evaluate AO in working women in shift. Our findings suggest that night shift work can modify women’s lifestyles, making it a worse standard for health, with less physical activity, number of meals and hours of sleep. In a previous meta-analysis of twenty-eight studies, an association of night shift work with obesity/overweight and particularly AO was estimated (OR 1·23, 95 % CI 1·17–1·29), demonstrating similarities to the present study(Reference Sun, Feng and Wang14).
Light is considered to be the most potent circadian synchroniser for humans. Exposure to artificial light at night may lead to a deregulation of the circadian system, through reductions in the melatonin secretion. Exposure to artificial light between midnight and 04.00 hours results in complete inhibition of melatonin secretion during what is known to be the peak of production in humans; this fact contributed to the development of obesity(Reference Guerrero-Vargas, Espitia-Bautista and Baujis20). In addition, the exposure of the workers to artificial light at night decreases the time spent sleeping, and it disrupts the circadian structure, the sleep cycle, social life and meal times. These facts result in a perturbation of the functioning of the biological clock that is often called ‘social jet lag’ because of the misalignment between the biological clock and social time. As a result of this metabolic change, there is a tendency to increase weight and fat in the abdominal region(Reference Touitou, Reinberg and Touitou21).
Changes in the timing of meals are also an important regulator of circadian rhythm and metabolic functions. Changes in the time of food intake are especially problematic when meal time does not coincide with the light–dark cycle(Reference Guerrero-Vargas, Espitia-Bautista and Baujis20). This study showed a higher prevalence of AO was associated with having three or fewer meals per day. After the adjustment for potential confounding factors, AO prevalence was 33 % higher (95 % CI 1·02, 1·73) in day workers and 130 % (95 % CI 1·30, 4·12) in night workers who had three or fewer meals per day, with the lower bound of the CI suggesting at least 30 % increase in prevalence. The mechanism by which few meals, shift work and AO interact is likely linked to alterations in the secretion of hormones regulating appetite such as leptin and ghrelin, two peripheral signals that contribute to the central regulation of food intake. Leptin is usually below normal levels among night shift workers. The circulating leptin concentrations are responsive to acute changes in energy balance resulting from increased or decreased energetic intake. In contrast to the anorexigenic effects of leptin, ghrelin is a hormone that is associated with increases in food intake via appetite regulation, promoting body weight gain, both can be altered by circadian rhythm changes(Reference Crispim, Waterhouse and Dâmaso22).
Eating more frequent meals is associated with increased appetite control, eating smaller portions and better quality of food(Reference Leidy and Campbell23). About the quality of food consumed, a systematic review with thirty-three studies showed an association between night shift worker and higher consumption of saturated fats and soft drinks when compared with hybrid shift workers. Likewise, night shift workers skip more meals. Regarding energy intake and micronutrient consumption, results are inconsistent and most studies found no associations(Reference Souza, Sarmento and De Almeida13). In the present study, we did not assess the quality of the diet, but it is suggested that longitudinal studies assess these characteristics of food consumption to verify the relationship with AO.
Leisure physical activity was associated with lower prevalence of AO among female shift workers, but physical activity is known to be associated with diet quality and energetic intake which in turn are associated with body composition as well. Physical activity also helps regulate circadian rhythms, and a review of experimental studies indicates that voluntary physical activity is associated with lower weight gain independently of changes to the circadian rhythm caused by light exposure at night(Reference Nelson and Chbeir24).
In our study, current smokers presented lower prevalence of AO than non-smoker women; however, this phenomenon can be called ‘fake benefit’, and it was conflicting in the literature. In the ‘fake benefit’, it is believed that smoking can control weight. This mechanism is explained by the influence of nicotine on the increase in the RMR and decreased appetite. Smoking twenty-four cigarettes per day increases energy expenditure by 10 %(Reference Szurkowska and Szybiński25,Reference Wierzejewska and Jarosz26) . On the other hand, the increase of the AO showed in some studies can be explained by the influence of nicotine on insulin resistance, predisposing to obesity and endocrine dysfunction among smokers. Moreover, visceral adipose tissue is sensitive to cortisol, which is elevated in the serum of smokers because of an increased sympathetic nervous system activity. Furthermore, women who smoke have lower levels of bioavailable oestrogen(Reference Wierzejewska and Jarosz26). The substances found in tobacco smoke also damage the granulosa cells of ovaries, causing a decrease in oestrogen and an increase in testosterone, resulting in AO(Reference Owczarczyk-Saczonek and Nowicki27,Reference Reich, Straszak and Śliwinska28) .
In our study, when we stratified by shift work, the association of 5 h or fewer of sleep on night shift workers with AO was perceptible (RP 1·45; 95 % CI 1·05, 2·02). Our findings go in the same direction as other studies, which show an association between fewer hours of sleep and increase in AO(Reference Guo, Rong and Huang9,Reference Canuto, Pattussi and Macagnan29–Reference Hairston, Bryer-Ash and Norris32) . Studies have suggested possible hypotheses for this association: short sleep duration may be associated with irregular eating habits, such as having a greater predominance of snacks rather than full meals, increased fat and sweets intake, and increased energy intake; on the other hand, decreased dietary intake of fruits and vegetables, and lower level of physical activity(Reference Souza, Sarmento and De Almeida13,Reference Canuto, Pattussi and Macagnan29,Reference Ohida, Kamal and Uchiyama33,Reference Parvaneh and Poh34) . Our findings went in the same direction: behavioural characteristics such as few meals per day and lower physical activities were associated with higher AO prevalence.
A limitation of a cross-sectional study is that exposures and outcomes or illnesses are measured at the same time which can lead to a bias, which we call reserve causation; therefore, we cannot distinguish whether the exposure preceded the development of the disease or whether the presence of the disease affected the individual’s levels of exposure. In addition, we suggest future studies to evaluate the population of workers on fixed shifts because our findings can be extrapolated to a population with the similar characteristics, fixed shift workers from the same manufacturing facility.
Our findings indicate that behavioural characteristics are associated with a higher prevalence of AO in female shift workers, thus, suggesting that behavioural modifications among women working shifts, such as increase meal frequency and increase physical activity, may reduce AO.
Acknowledgements
Acknowledgements: None. Financial support: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. M.T.A.O. received research funding from PQ/CNPQ (307257/2013-4; 307175/2017-0). Conflict of interest: None. Authorship: H.T. developed the project, data collection, statistical analysis and article writing. D.G.B. performed the statistical analysis and final revision of the article. J.C.d.S. conducted the literature review and data collection. K.G.M. developed the project. G.H.C. assisted in project development and data collection. J.C.S. assisted in project development and data collection. M.T.A.O. developed the project, statistical analysis and final revision of the article. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Research Ethics Committee of the University of Vale do Rio dos Sinos, RS, Brazil, under number 2.057.810/2017. Written informed consent was obtained from all subjects.



