


Developing countries have experienced increasing rates of overweight( Reference Popkin, Adair and Ng 1 , Reference Finucane, Stevens and Cowan 2 ). In Brazil, increasing prevalence rates of overweight have been observed in the population at all life stages. Overweight was observed in 7·3 % of children under 5 years old( Reference Ministério da Saúde 3 ) and in 33·5 % of children aged 5–9 years( 4 ). Among women, over the course of a 35-year period, overweight increased from 28·7 % in 1974 to 48 % in 2008. In addition, the obesity rate among women increased more than twofold during the same period, from 8 % to 16·9 %( 4 ).
Genetic( Reference Franks and Ling 5 ), psychosocial( Reference Perez, Garcia and Herrera 6 ) and metabolic( Reference Godfrey, Gluckman and Hanson 7 ) factors may be associated with obesity. However, the factors that best explain the growing number of overweight people involve changes in lifestyle( Reference Lee, Houser and Must 8 ), the high prevalence of physical inactivity and the increased consumption of processed foods with high energy density, particularly those rich in saturated fat and simple carbohydrates( Reference Kourlaba, Panagiotakos and Mihas 9 ).
Unlike overweight, the prevalence of child undernutrition has declined globally over the past decades. However, this reduction in undernutrition is occurring unevenly; in fact, the problem has increased in some countries( 10 ). It is estimated that 186 million children under 5 years of age are affected by protein–energy malnutrition worldwide( 10 ). In Brazil, between 2008 and 2009, 6 % of children under 5 years old were malnourished. Social and economic inequities are the main predictive factors of undernutrition( 4 , Reference Monteiro, Gomes and Cannon 11 ).
In this context, the current scenario of the nutrition transition in poor and developing countries is characterized by the double burden of malnutrition, which refers to under- and overnutrition occurring simultaneously, even within members of the same family( Reference Doak, Adair and Bentley 12 ). High prevalence of the double burden of malnutrition has been increasing in middle- and low-income countries( Reference Doak, Adair and Monteiro 13 ). In Guatemala, Argentina and Africa it has been shown that underweight or short stature of the child can coexist with maternal overweight( Reference Lee, Houser and Must 14 – Reference Bassete, Romaguera and Gimenez 16 ).
The determinants of these two nutritional phenomena in the same household are well described in the literature( Reference Monteiro, Szarfarc and Mondini 17 , 18 ); however, there are few studies assessing the factors associated with the coexistence of this double burden morbidity( Reference Aitsi-Selmi 19 , Reference Garrett and Ruel 20 ). Studies describe that it is associated with low levels of maternal education( Reference Bassete, Romaguera and Gimenez 16 ), lower household incomes( Reference Doak, Adair and Monteiro 13 ) and environmental factors, which include changes in dietary patterns with intakes of high-energy and nutrient-poor foods( Reference Ochola and Masibo 21 ). Epidemiological evidence also suggests that maternal nutrition during pregnancy may influence the risk of child undernutrition and subsequent obesity in adulthood( Reference Black, Allen and Bhutta 22 ).
The present study was designed because there are few studies investigating factors associated with the coexistence of undernutrition and overweight, two outcomes of an apparently antagonistic nature, among different members of the same family that share the same physical space, and because of the importance of elucidating possible relationships between poorly investigated variables and the variables already known to be involved in the causality network of these nutritional outcomes. Thus, the present study aimed to estimate factors associated with double burden of nutritional outcomes in the mother–child dyad at the household level (child stunting and/or maternal overweight) using data from the Brazilian Demographic and Health Survey.
Methods
The current cross-sectional study analysed data from the latest National Demographic and Health Survey of Children and Women conducted between 2006 and 2007 in Brazil (Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher; PNDS). The survey is part of the worldwide Demographic and Health Survey (DHS) programme. This nationwide survey was performed using complex probability sampling and its main objective was to provide information on population, family planning and health( Reference Ministério da Saúde 3 ). The sampling plan of the PNDS was designed to provide estimates representative of the Brazilian population living in private households in common or non-special census tracts (including slums), who were selected in ten sampling strata that comprise a combination of all five major geographical Brazilian regions and of both urban and rural areas. The sampling units were selected in two stages: the primary units were composed by census tracts and the secondary units by households( Reference Ministério da Saúde 3 ). Detailed sampling plans, data collection information and data quality assurance are available in the PNDS/DHS 2006 survey final reports (available at http://bvsms.saude.gov.br/bvs/pnds/index.php).
Details about how the databases were related and edited to allow analysis of the mother–child dyad – the outcome of the present study (child with short stature and maternal overweight) – have been described previously( Reference Felisbino-Mendes, Matozinhos and Miranda 23 ). Anthropometric measurements of mothers and children were performed according to internationally standardized procedures( 24 ) where two measures were obtained for each anthropometric indicator (weight and height) and the mean value was used. Mothers whose children were, at date of the interview, alive and living with them were included in the current analysis. It is important to highlight that when the mother had more than one child in the house (about 22 %), the eldest child was chosen for the mother–child dyad. This choice was due to the fact that the older child would have longer duration of exposure to deprivation and other factors affecting growth( Reference Blackwell, Hayward and Crimmins 25 ). Thus, the final number of mother–child dyad observations was 3676. It should be emphasized that there were no statistically significant differences in socio-economic and demographic characteristics between the excluded and studied children (data not shown). It is noteworthy that some individuals did not present complete data for all variables used in the analyses.
The stature of the children was classified by the height-for-age Z-score (HAZ), with HAZ <−2 considered as short stature( 26 ). Maternal BMI was calculated using the mother’s weight in kilograms and height in metres according to the formula weight/height2 and BMI≥25·00 kg/m2 was considered as overweight( 24 ).
Exposure variables were evaluated in the following levels and blocks according to Fig. 1.
-
1. Level 1, block A, socio-economic factors: included the variables maternal employment (0=mother did not work outside the household, 1=mother worked outside the household), maternal educational level (0=more than 8 years of schooling, 1=less than or equal to 8 years of schooling), mother’s skin colour (0=white, 1=non-white), maternal marital status (0=married, 1=single/widowed/divorced), area of residence (0=urban, 1=rural), region of residence (0=South, 1=Southeast, 2=North, 3=Northeast, 4=Midwest) and economic status assessed by ownership of household goods (based on the Brazilian Economic Classification Criteria of the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa)( 27 ), stratified into tertiles, with the third tertile used as the reference). The variable family income was not included in the analysis due to the high number of missing responses.
-
2. Level 2, block B, environmental factors: included the variables type of residence (0=masonry, 1=others), water supply (0=public, 1=others) and sewage system (0=pipe network, 1=others). Level 2, block C, social vulnerability: included the Brazilian Food Insecurity Scale (Escala Brasileira de Insegurança Alimentar; EBIA)( Reference Pérez-Escamilla, Segall-Corrêa and Kurdian Maranha 28 ), represented by scores (0=food security, 1=mild food insecurity, 2=moderate food insecurity, 3=severe food insecurity), and being a beneficiary of the family allowance programme (0=beneficiary, 1=not a beneficiary).
-
3. Level 3, block D, maternal factors: included maternal height (divided into tertiles, with the third tertile used as the reference), the number of children (0=1 child, 1=more than one child) and breast-feeding (0=yes, 1=no). Level 3, block E, child’s food intake: assessed by the intakes of fruits, vegetables, rice, beans, fish and meat (0=more than 4 d/week, 1=less than or equal to 4 d/week) and candy, soft drinks and fried foods (0=less than 4 d/week, 1=more than or equal to 4 d/week) in the week before the interview. The frequency of consumption was related to the seven days prior to the interview and answer choices for each food item were: not consumed, consumed on one day, two to three days, four to six days, or every day, and do not know( Reference Ministério da Saúde 3 ). We assumed this first group (fruits, vegetables, rice, beans, fish and meat) as a marker of eating healthy foods and the other group, as an unhealthy diet marker. This classification was based on nutritional recommendations for the prevention of chronic diseases and also because there is evidence to suggest the association of these variables with excess weight and other risk factors for chronic diseases, such as dyslipidaemias( 29 – Reference Lopes-Garcia, Schulze and Fung 31 ). The consumption of these foods was denoted by an indicator that expresses the proportion of children who consumed each of the selected foods more frequently (regularly: at least five of the seven days preceding the study) and less frequently (between zero and four days of the seven days preceding the study); this indicator is already used in the risk factors surveillance system( Reference Castro, Cardoso and Egstrom 32 ). The variable birth weight of the child was not included due to the high number of missing responses.

Fig. 1 Conceptual theoretical framework of the possible factors associated with nutritional outcomes in the mother–child dyad
The outcome of interest, the mother–child dyad, was ranked into the following four categories.
-
1. Category 0 (reference): mother with normal weight and child with normal height (NM/NC).
-
2. Category 1: overweight mother and child with normal height (OM/NC).
-
3. Category 2: mother with normal weight and short-stature child (NM/SSC).
-
4. Category 3: overweight mother and short-stature child (OM/SSC), defined as a double burden of malnutrition.
The descriptive statistics included the estimation of absolute frequencies (sample size), relative frequencies, and means and standard errors. Significant differences were evaluated using the χ 2 test based on the sampling design (P<0·05). The hierarchical approach for multinomial logistic regression modelling was used to study the factors associated with OM/NC, NM/SSC and OM/SSC. So, the analysis was conducted in accordance with a predefined conceptual model (Fig. 1). The model defined three hierarchical levels: the first (distal) included one block with all socio-economic variables; the second level included two blocks, social vulnerability and environmental variables; and the third (proximal) level included two blocks, one for maternal characteristics and other for children’s food intake. We assumed that socio-economic conditions were more distal determinants that may affect an individual’s nutritional status directly or partly through determinants in the second level and third level. Then, in accordance with Fig. 1, social vulnerability and environmental variables can influence maternal characteristics such as mother’s stature and also children’s food intake. Finally, all hierarchically higher variables can contribute to explain the double burden of malnutrition taking into account all interrelationships between them. All models included mother’s age and children’s gender and age. The covariates from the first level presenting a P value ≤0·20 were admitted to the next step of intra-block backward selection and only the covariates with P values ≤0·05 at this second step were included as input in the hierarchical modelling for the third level. This reflects the proposed causal mechanism( Reference Victora, Huttly and Fuchs 33 – Reference Strina, Rodrigues and Cairncross 35 ): model A, including the variables of block A, aims to obtain the overall effect of socio-economic factors; model B, adding to model A the significant variables of blocks B and C, estimates the overall effect of the second level, adjusted for confounding in block A; and model C, which adds to model B the third-level variables, aims to estimate the overall effect of maternal factors and food intake, adjusted for confounding of blocks A–C. Models A, B and C were defined by fitting a sequence of multivariate regression models that kept, at the level last added, only the variables selected, again by backward elimination (P value ≤0·05), through a likelihood ratio test.
Data were processed and analysed using the program Statistical Software for Professionals, version 12.1, using the Survey module of the statistical package that considers various aspects of the complex sampling design in the analysis.
Regarding the ethical aspects, the PNDS 2006 was approved by the Research Ethics Committees of the STD/AIDS Reference and Training Center of the São Paulo State Health Department, São Paulo, Brazil. All individuals who agreed to participate in the study signed an informed consent form.
Results
Among the total of 3676 mothers who participated in the study, 85·2 % were married or in a stable relationship; 57·6 % reported that they did not work outside the household; 55·2 % had less than or equal to 8 years of schooling; 34·1 % had a better economic status; 41·8 % were living in the Southeast region of the country; and 81·4 % were living in urban areas. Moreover, most of them had only one child (78·5 %) and breast-fed their children (96·8 %).
The mean age of the mothers was 27 (se 0·21) years and the mean maternal BMI was 25 (se 0·15) kg/m2 (Table 1). The environmental characteristics and social vulnerability of the studied dyads were also considered. Approximately 64·0 % of households had piped water, while only 47·6 % of households were connected to the sewage network; 87·2 % lived in masonry houses, 75·8 % were not beneficiaries of the family allowance programme and 6·4 % had severe food insecurity (see online supplementary material, Supplemental Table 1).
Table 1 Characteristics of the mothers and children in the mother–child dyads (n 3676), National Demographic and Health Survey of Children and Women, Brazil (PDNS), 2006–2007

HAZ, height-for-age Z-score.
The mean age of the children was 2 (se 0·03) years and their mean HAZ was 0·28 (se 0·04; Table 1). There was a slightly higher proportion of males (52 %). In addition, 54·4 %, 72·2 % and 67·2 % of the studied children consumed fruits, rice and beans, respectively, on more than 4 d/week. However, 66·8 % and 83·0 % of them consumed legumes and vegetables, respectively, on less than or equal to 4 d/week. Other characteristics of the children are shown in the online supplementary material, Supplemental Table 1.
The prevalence of the double burden of malnutrition was 2·2 (95 % CI 0·01, 0·03) %, of child stunting was 6·4 (95 % CI 0·05, 0·08) % and of mothers with overweight was 44·2 (95 % CI 0·38, 0·47) %. In addition, 50·9 (95 % CI 0·47, 0·53)%, 43·0 (95 % CI 0·39, 0·46)% and 3·9 (95 % CI 0·02, 0·05)% were classified as NM/NC, OM/NC and NM/SSC, respectively (Fig. 2).
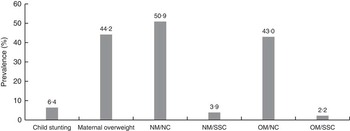
Fig. 2 Prevalence of nutritional outcomes (child stunting and/or maternal overweight) in mother–child dyads (n 3676) at the household level, National Demographic and Health Survey of Children and Women, Brazil (PDNS), 2006–2007 (NM/NC, mother with normal weight and child with normal height; NM/SSC, mother with normal weight and short-stature child; OM/NC, overweight mother and child with normal height; OM/SSC, overweight mother and short-stature child – double burden of malnutrition)
The results of the analysis of each factor individually associated with the outcome, adjusted for maternal age, age and gender of the child, are shown in the online supplementary material, Supplemental Table 1. The odds of the double burden of malnutrition were significantly higher among mothers with lower educational level (OR=4·54; 95 % CI 1·84, 11·22), living in inadequate households (non-masonry house; OR=3·63; 95 % CI 1·91, 6·90), living in the Northern region of Brazil (OR=3·09; 95 % CI 1·30, 7·35), with severe food insecurity (OR=3·32; 95 % CI 1·42, 7·72), who did not breast-feed (OR=3·07; 95 % CI 1·10, 8·58) and among children who consumed fried food on more than or equal to 4 d/week (OR=3·03; 95 % CI 1·08, 8·47). The odds of child short stature were significantly higher among whose those mothers had a lower educational level (OR=2·46; 95 % CI 1·31, 4·61), were living in inadequate households (non-masonry house; OR=3·18; 95 % CI 1·90, 5·31), were living in the Northern region of Brazil (OR=2·62; 95 % CI 1·14, 6·02), who were in the first tertile of household goods (OR=2·97; 95 % CI 1·52, 5·79), had short stature (OR=4·25; 95 % CI 2·22, 8·15) and among children who consumed vegetables on less than or equal to 4 d/week (OR=2·80; 95 % CI 1·31, 6·01). The odds of maternal overweight were significantly higher among mothers who did not breast-feed their children (OR=1·98; 95 % CI 1·06, 3·70; Supplemental Table 1).
The results of the intra-block analysis of the variables selected in the previous stage are shown in the online supplementary material, Supplemental Table 2. Lower maternal educational level (OR=4·76; 95 % CI 1·99, 11·41), living in the Northern region of Brazil (OR=2·80; 95 % CI 1·17, 6·66) and in inadequate households (non-masonry house; OR=3·63; 95 % CI 1·91, 6·90), having severe food insecurity (OR=2·93; 95 % CI 1·09, 7·80), having a higher number of children (OR=2·19; 95 % CI 1·03, 4·66) and not breast-feeding (OR=3·08; 95 % CI 1·08, 8·72) were associated with the double burden of malnutrition. The first (OR=2·82; 95 % CI 1·20, 6·61) and second tertile (OR=2·21; 95 % CI 1·04, 4·68) of household goods, living in inadequate households (non-masonry house; OR=3·18; 95 % CI 1·90, 5·31), mothers with low stature (OR=4·21; 95 % CI 2·19, 8·09) and children who consumed vegetables on less than or equal to 4 d/week (OR=2·49; 95 % CI 1·10, 5·61) were associated with the category NM/SSC. Not breast-feeding the child was associated with the category OM/NC (OR=1·99; 95 % CI 1·06, 3·72).
Table 2 Final model of the multinomial regression, with odds ratios and 95 % confidence intervals of the factors associated with the nutritional outcomes in the mother–child dyads (n 3676), National Demographic and Health Survey of Children and Women, Brazil (PDNS), 2006–2007
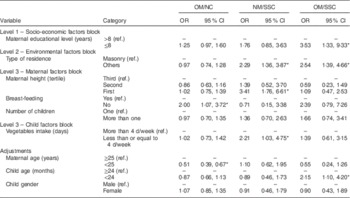
OM/NC, overweight mother and child with normal height; NM/SSC, mother with normal weight and short-stature child; OM/SSC, overweight mother and short-stature child – double burden of malnutrition; ref., reference category.
*P<0·05.
Table 2 shows the final results of multinomial logistic regression analysis using the NM/NC category as the reference. Among the socio-economic factors, lower maternal educational level (OR=3·53; 95 % CI 1·33, 9·33) increased to three times the odds of the double burden of malnutrition. Regarding the environmental characteristics, children living in inadequate households (non-masonry house) were more likely to have short stature (OR=2·29; 95 % CI 1·36, 3·87) and the double burden of malnutrition (OR=2·54; 95 % CI 1·39, 4·66). Regarding maternal characteristics, mother’s short stature (OR=3·41; 95 % CI 1·76, 6·61) increased the odds of the child having short stature by threefold and mothers who did not breast-feed their children were more likely to be overweight (OR=2·00; 95 % CI 1·07, 3·72). Among the variables associated with child nutrition, vegetable intake on less than or equal to 4 d/week (OR=2·21; 95 % CI 1·03, 4·75) increased the odds of short stature among children more than twofold.
Discussion
The current study aimed to estimate factors associated with double burden of nutritional outcomes in the mother–child dyad at the household level (child stunting and/or maternal overweight). In the dyads studied, 2·2 % presented the double burden, which is below the rate of 3·3 % reported in a study conducted in fifty-four countries between 1991 and 2009 with children aged 2–5 years old( Reference Dieffenbach and Stein 36 ). Higher prevalence was shown in Argentina (12 %)( Reference Bassete, Romaguera and Gimenez 16 ) and a study in Algeria reported a rate of 7 % in families that did not have access to a variety of healthy foods and had a diet based on high-sugar foods and poor in fruit and vegetables( Reference Grijalva-Eternod, Wells and Cortina-Borja 15 ).
As shown in previous population research, our study revealed that low maternal educational level (0–8 years of schooling) was associated with the double burden of malnutrition( Reference Bassete, Romaguera and Gimenez 16 ). However, another cross-sectional study conducted with 223 mother–child dyads in the rural area of Malaysia found no association between the double burden and maternal educational level( Reference Ihab, Rohana and Manan 37 ). There is a consensus that women with lower educational levels have lower participation in the labour market and have lower and unstable incomes. In addition, lower educational levels are associated with both greater inefficiency in allocating financial resources and lack of knowledge on buying healthy foods( Reference de Souza Bittencourt, Chaves dos Santos and de Jesus Pinto 38 ). In this scenario, families often adopt compensatory feeding practices, such as increased consumption of fast food, soft drinks, canned goods and candies instead of consumption of foods with better nutritional quality due to the higher cost of the latter( Reference Feinberg, Kavanagh and Young 39 ); this fact can explain the overweight, especially among adults( Reference Birbilis, Moschonis and Mougios 40 ), and height deficit among the children more vulnerable to nutritional deficiencies( Reference Sawaya 41 ) observed in studies evaluating these nutritional outcomes together. Lower maternal educational level is well known to be associated with children’s impaired linear growth( Reference Lakshman, Zhang and Zhang 42 , Reference Hasan, Soares Magalhaes and Williams 43 ), although our findings failed to show association with NM/SSC outcome. It is possible that other variables considered in the modelling process could have eliminated/diminished the negative impact of this variable on child growth.
In the present study, living in an inadequate household (non-masonry house) was associated with the double burden of malnutrition (OM/SSC) and growth deficit in children (NM/SSC). There is no doubt that poor housing conditions promote higher risks of diseases and impaired nutritional status. The literature shows that undernutrition and obesity can coexist in homes with poor conditions( Reference Sawaya, Solymos and Florêncio 44 ). The living condition is widely discussed and is strongly associated with household income which, as mentioned in many studies, defines the previous and current overall health status and the allocation of resources to purchase quality basic foods in quantities necessary for the healthy development and growth of individuals( Reference Drewnowski 45 ). The current study also confirms the association between inadequate household (non-masonry house) and growth deficit (NM/SSC), corroborating the findings of other Brazilian studies conducted mainly in areas of high social vulnerability( Reference Jesus, Castelão and Vieira 46 , Reference Silveira, Alves and Ferreira 47 ). In children under 5 years old, the influence of environmental factors is much more relevant for the expression of growth potential than genetic factors( Reference Martorell, Mendoza and Castillo 48 ). Children living in households with poor floor and ceiling conditions and with no piped water and sewage systems have a higher incidence of recurrent infectious diseases that contribute to child undernutrition( Reference Monteiro, Benicio and Konno 49 ).
Mothers with short stature were three times more likely to have a child with short stature, corroborating a study that also used the PNDS data set( Reference Felisbino-Mendes, Matozinhos and Miranda 23 ) and other studies( Reference Addo, Stein and Fall 50 , Reference Ozaltin, Hill and Subramanian 51 ). Mothers with short stature most likely provide a nutritionally restricted uterine environment; therefore, the fetus will have an inadequate supply of nutrients and restricted growth, which will result in low birth weight and short stature( Reference Martorell, Mendoza and Castillo 48 ). The final adult height is likely influenced by genetic, environmental and social conditions experienced in childhood and poor maternal health, not only in developing countries but also in modern Western societies( Reference Ozaltin, Hill and Subramanian 51 , Reference Silventoinen 52 ).
In the present study, low vegetable intake was associated with the NM/SSC dyad, which is in agreement with the results obtained in a study conducted in the Republic of the Maldives with children under 5 years old( Reference Golder, Erhardt and Scherbaum 53 ) and with other studies showing that inadequate intakes of vegetables, legumes and fruits, which are sources of micronutrients, in particular vitamins and minerals, can cause growth retardation, weight loss and increased susceptibility to infectious diseases in children( Reference Kismul, Van den Broeck and Lunde 54 ). The latest Brazilian Household Budget Survey (2008–2009) showed a high consumption of sandwiches and high-calorie drinks instead of fruit and vegetables among children, which makes this age group vulnerable to nutritional deficiencies and their multiple complications or co-morbidities, including growth deficit( 4 ).
Another important result obtained in the present study was the fact that mothers who did not breast-feed were more likely to be overweight (OM/NC). A cohort study conducted in Pelotas, southern Brazil, with a 5-year follow-up showed that exclusive breast-feeding for 4 months was associated with a lower waist circumference and lower body fat percentage( Reference Gigante, Victora and Barros 55 ). The results of another cohort study consisting of 315 women who were living in two cities of the Brazilian state of Bahia showed that breast-feeding for a period longer than 6 months was associated with weight loss( Reference da Silva, Oliveira Assis and Pinheiro 56 ). A 9-month follow-up study performed in Brazil showed an association between longer duration of breast-feeding and lower postpartum weight retention( Reference Kac, Benício and Velásquez-Meléndez 57 ). Therefore, there are several studies demonstrating controversial results for the association between breast-feeding and postpartum weight loss. This fact can occur due to several reasons, such as the study design, the definition of the variable breast-feeding and its duration and intensity, the postpartum follow-up care of the women and the pre-pregnancy nutritional status, or the control of confounding variables involved in the analysis. One of the mechanisms that explains maternal weight loss during lactation is long duration and intensity of breast-feeding, which has a major influence on the maternal nutritional and energy demand for milk production and can contribute to up to 20 % of total daily energy expenditure( Reference Prentice and Prentice 58 ). However, it must be considered that in the first months after delivery, high levels of prolactin cause an increased appetite to meet the energy demands of breast-feeding. If, on the one hand, weight loss is expected due to the high energy demands of lactation, on the other hand, one can expect an increase in weight due to increased appetite( Reference Sichieri, Field and Rich-Edwards 59 ).
The limitations of the present study include the fact that a cross-sectional design only allows for inferences to be made about a possible association between exposure factors and nutritional outcomes, and does not allow a causality relationship to be established. In addition, food intake variables can have a recall bias. The children’s birth weight is an important predictor for morbidity and mortality in the age group of the studied children but could not be used due to the high number of missing responses. Despite this, we believe that those limitations could not be considered an alternative explanation for our results because the DHS includes a large sample of both rural and urban populations, is representative of the Brazilian population and includes potential determinants of dyad child–mother nutritional outcomes. In general, the findings are in agreement with similar studies, were analysed using appropriate statistical methods and controlled for significant confounding factors according to the conceptual model previously defined.
In summary, lower maternal education level and living in inadequate households were associated with the double burden of malnutrition. It is important to mention that the double burden outcome represents a grouping of opposite manifestations of malnutrition among individuals who share the same environment and household. Thus, it is believed that knowledge of potential determinants of the health of the mother–child dyad can contribute to establishing strategies promoting health and healthy diets by considering the two scenarios concomitantly (growth deficit and overweight). This situation was outlined in the nutritional transition process, with changes in demographics and morbidity/mortality profiles, which have been intensified in recent decades in developing countries.
It is essential that multidisciplinary teams in health promote educational activities about healthy eating and nutrition for the family, through health education; this is considered one of the most important strategies for the prevention of overweight and growth deficit, aiming to raise awareness on the importance of a diet rich in nutrients and low in saturated fats.
Acknowledgements
Financial support: T.G.-H. received a PhD scholarship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil and would also like to thank the Brazilian National Council of Research and Technology (CNPq) for a scholarship that supported a fellowship at the Federal University of Bahia, Brazil. Conflict of interest: None. Authorship: T.G.-H., R.C.R.-S. and R.L.F. planned the study, analysed the data, interpreted of results, wrote and reviewed the manuscript. M.L.B. and G.V.-M. planned the study, interpreted of results and revised the manuscript. All authors read and approved the final manuscript. Ethics of human subject participation: The PNDS 2006 was approved by the Research Ethics Committees of the STD/AIDS Reference and Training Center of the São Paulo State Health Department, São Paulo, Brazil. All individuals who agreed to participate in the study signed an informed consent form.
Supplementary Material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S136898001600080X






