


The weight of the brain is approximately 1.4% of that of the body, and it varies with age and gender (Reference LudwigLudwig, 1979). The mean weight of ‘wet’ autopsy brain of an adult male is 1300-1450 g (female, around 100 g less), with an average increase of 8% after fixation (Reference KnightKnight, 1996). The mean brain weight of men aged 60-70 is 1323 g (range 1018-1600) and for ages 70-85, 1279 g (1039-1485); for women aged 60-70, mean brain weight is 1178 g (920-1372) and for ages 70-85, 1121 g (852-1370) (Reference KnightKnight, 1996). Brain weight has been explored in normal ageing as well as in a number of psychiatric conditions. Mueller et al (Reference Mueller, Moore and Kerr1998) reported that insignificant brain volume loss is observed over time in healthy people aged over 65. This suggests that large changes seen in crosssectional studies reflect the presence of preclinical dementia in older groups (Reference Mueller, Moore and KerrMueller et al, 1998). Courchesne et al (Reference Courchesne, Müller and Saitoh1999) reported that post-mortem brain weights of people with autism were similar to those of the normal population. Johnstone et al (Reference Johnstone, Bruton and Crow1994) found that decreased brain weight in schizophrenia was significantly related to poor premorbid global function and to more severe negative symptoms. Lower brain weights were also reported by Pearlson & Warren (Reference Pearlson and Warren1989) in Down's syndrome and by Nochlin et al (Reference Nochlin, van Belle and Bird1993) in Alzheimer's disease. Brown et al (Reference Brown, Colter and Corsellis1986) reported that the decrease in brain weight in schizophrenia was less than in Alzheimer's disease and Huntington's chorea. Hakim and Mathieson (Reference Hakim and Mathieson1979) reported a significantly reduced weight in brains from Parkinson's disease cases, compared to a matched control group. Harper and Blumberg (Reference Harper and Blumberg1982) reported that the brain weight of alcohol-dependent males was significantly less than that in a normal population, both for brains with alcohol-related nutritional damage (Wernicke's encephalopathy) and brains which appeared ‘normal’ macroscopically and microscopically.
We found only one published article about the effect of various methods of fatal self-harm (FSH) on brain weight. Schroder and Saternus (Reference Schröder and Saternus1983), investigating changes in the brain caused by suicidal hanging, found that the brain weight - both for typical and atypical hanging - was greater in all age groups than the average found in clinical autopsy. Investigating the effect of hypothalamic-pituitary-adrenal dysfunction in major depression and suicidal behaviour, Szigethy et al (Reference Szigethy, Conwell and Forbes1994) found that the mean left adrenal weight was significantly higher in suicide victims, but these authors did not comment on brain weight.
In this study we attempt to explore whether brain weight measured postmortem varies with different methods of FSH and whether it differs from that of persons who died of natural causes.
METHOD
We carried out a retrospective review of records of coroners' inquests on older people. In an attempt to reduce any ascertainment bias of suicide, we use the term ‘fatal self-harm’ (FSH) to include all cases where the coroner's verdict was suicide, cases who killed themselves but in which the coroner returned an open verdict because of insufficient evidence, and those who had committed some deliberate act which resulted in death, but the apparent intent to die was absent (‘misadventure’).
Fatal self-harm data
Data were extracted from coroners' records of all deaths of persons aged 60 years or over from 1994 to 1998 occurring within the North Cheshire and Birmingham districts, for those classified as having committed suicide (ICD-9 E950-959), and for those for whom an open verdict or a verdict of misadventure was returned (ICD-9 E980-989; World Health Organization, 1978), from two Coroner's Offices, in Warrington (35% of the sample) and Birmingham (65%). Information extracted included demographic data, method of death and coroner's verdict, and brain weight as recorded by the pathologist. The brain weights of people aged ≥ 60 whose deaths were unexpected, sudden or unexplained (thus requiring a post-mortem), but attributed to natural causes, were also collected for comparison. Unfortunately, data relating to body weight and height were not available. The deceased were matched by obtaining equal means and variances of the two groups for age by gender. For all subjects, whether death was due to natural causes or FSH, post-mortem examination was reported to have been carried out within 6-12 hours of death. All brain weights included in the study were reported as ‘wet’ autopsy weights where no formalin fixation was used.
RESULTS
Data were available on the weight of 292 post-mortem brains: 87 male (64%), 105 female (36%). Of these, 150 (51%) were deaths due to natural causes: 107 male (71%), 43 female (29%); and 142 (49%) due to FSH: with a suicide verdict in 93 cases (55 male (59%), 38 female (41%)) and an open verdict in 49 cases: 25 male (51%), 24 female (49%). The mean age of the sample was 72 years (s.d.=8): male 71.7 (s.d.=8) and female 12.9 (s.d.=8). Men who died of FSH (n=80) or natural causes (n=107) had a matched mean age of 71.5 years (s.d.=7) and for women, the matched mean age was 72.9 (s.d.=8) for both FSH (n=62) or natural causes (n=43).
Of the methods of fatal self harm, 39% were overdose, 24% hanging, 9% drowning, 16% asphyxia or inhalation of carbon monoxide and 12% were other means (mostly violent). The natural causes of deaths were cardiac or cardiovascular (80%), respiratory (15%) and cerebral haemorrhage (5%). The mean brain weight for the entire sample was 1291 g (s.d.=124) (median 1280) (males, 1310 g (s.d.=122); females, 1258 g (s.d.=119)). Table 1 gives the basic statistics.
Table 1 Brain weight (g)
| Method of death | No. | Median | Mean | s.d. | Range | Male | Female | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | s.d. | n | Mean | s.d. | ||||||
| Natural causes | 150 | 1240 | 1238 | 37 | 1050-1420 | 107 | 1260 | 79 | 43 | 1184 | 82 |
| Fatal self-harm | 142 | ||||||||||
| Overdose | 55 | 1344 | 1322 | 119 | 960-1558 | 20 | 1352 | 79 | 35 | 1305 | 127 |
| Hanging | 34 | 1383 | 1394 | 159 | 1050-1780 | 29 | 1409 | 167 | 5 | 1309 | 54 |
| Drowning | 13 | 1392 | 1321 | 145 | 985-1473 | 7 | 1339 | 34 | 6 | 1299 | 126 |
| Run over by train | 3 | 1355 | 1341 | 27 | 1310-1359 | 2 | 1334 | 34 | 1 | 1335 | |
| Asphyxia | 16 | 1349 | 1341 | 111 | 1164-1497 | 4 | 1445 | 30 | 12 | 1307 | 107 |
| Jumping from height | 5 | 1315 | 1310 | 81 | 1207-1398 | 4 | 1319 | 93 | 1 | 1315 | |
| Electrocution | 3 | 1347 | 1286 | 109 | 1160-1357 | 3 | 1286 | 109 | 0 | 0 | 0 |
| Car exhaust | 7 | 1379 | 1409 | 159 | 1215-1698 | 7 | 1409 | 59 | 0 | 0 | 0 |
| Knife | 4 | 1400 | 1391 | 100 | 1260-1505 | 2 | 1400 | 70 | 2 | 1382 | 173 |
| Set fire to self | 2 | 1342 | 1342 | 74 | 1290-1395 | 2 | 1342 | 74 | 0 | 0 | 0 |
Figure 1 is a box plot graph of the highest and lowest brain weights; the median is a thick line inside each box, which contains 50% of cases within the interquartile range. The central position of the median indicates a normal distribution of weights, with positively skewed distribution in some FSH methods involving small numbers.
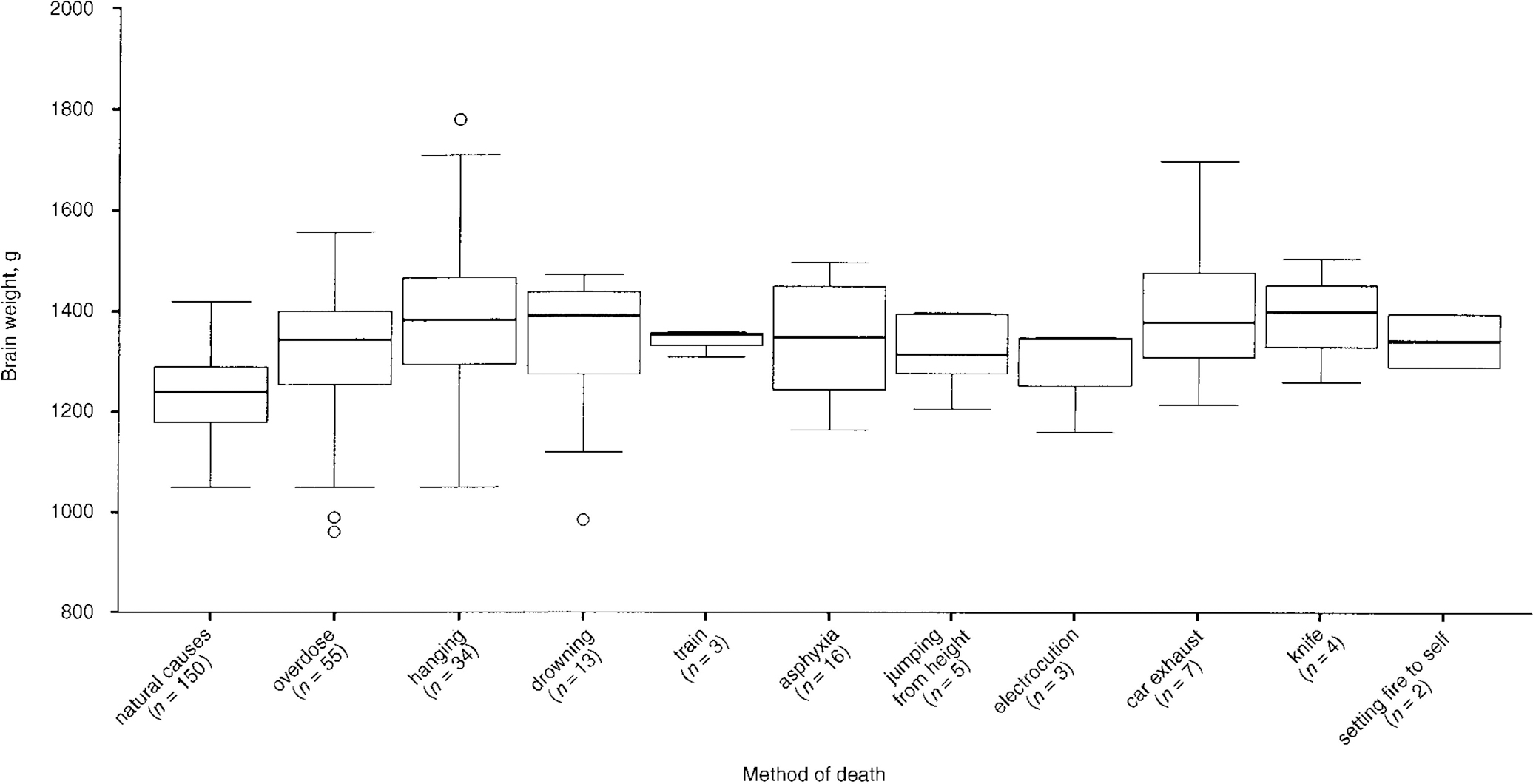
Fig. 1 Brain weight in cases of fatal self-harm.
Table 2 summarises the distribution of brain weight in FSH cases in relation to the method of death. A suicide verdict appears to have been returned more frequently in cases of FSH by hanging and asphyxia using a plastic bag; but a suicide verdict was also returned in all incidents of FSH by wounding, electrocution and carbon monoxide poisoning using car exhaust. An open verdict was returned more frequently in cases of death by drowning, being killed by a train, jumping from a height and setting fire to oneself. Electrocution, car exhaust and setting fire to oneself were methods used only by men.
Table 2 Mean brain weight (g) in fatal self-harm (FSH)
| Method of FSH | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Suicide | Open verdict | Suicide | Open verdict | |||||
| n (%) | Mean | n (%) | Mean | n (%) | Mean | n (%) | Mean | |
| Overdose | 14 (70) | 1330 | 6 (30) | 1345 | 19 (54) | 1311 | 16 (46) | 1299 |
| Hanging | 24 (83) | 1403 | 5 (17) | 1435 | 5 (100) | 1309 | ||
| Drowning | 7 (100) | 1339 | 3 (50) | 1283 | 3 (50) | |||
| Run over by train | 1 (50) | 1359 | 1 (50) | 1310 | 1 (100) | 1316 | ||
| Asphyxia | 3 (75) | 1444 | 1 (25) | 1450 | 9 (75) | 1291 | 3 (25) | 1355 |
| Jumped from height | 1 (25) | 1207 | 3 (75) | 1359 | 1 (100) | 1315 | ||
| Electrocution | 3 (100) | 1286 | ||||||
| Car exhaust | 7 (100) | 1409 | ||||||
| Knife | 2 (100) | 1400 | 2 (100) | 1382 | ||||
| Set fire to self | 2 (100) | 1342 | ||||||
Means of brain weight were compared using the t-test for the following groups:
-
(a) suicide (n=93) v. natural death (n=150): mean brain weights 1352 v. 1238 g, respectively (t=-8, P<0.001, 95% CI for mean difference ‒141.8 to ‒86.6; females only t=-6.1, P<0.001; males only t=-7.45, P<0.001);
-
(b) open verdict (n=49) v. natural death (n=150): mean brain weights 1338 v. 1238 g, respectively (t=-6, P<0.001, 95% CI for mean difference ‒133.4 to ‒67.8; females only t=-5.5, P<0.001; males only t=-4.9, P<0.001);
-
(c) suicide (n=93) v. open verdict (n=49): mean brain weights 1352 v. 1338 g, respectively (t=0.6, P=0.5, 95% CI for mean difference ‒32.6 to 59.9; females only t=-0.12, P=0.9; males only t=0.5, P=0.5); and
-
(d) all FSH verdicts (n=142) v. natural death (n=150): mean brain weights 1347 v. 1238 g, respectively (t=-8.4, P<0.001, 95% CI for mean difference ‒135.2 to ‒83.8; females only t=-6.1, P<0.001; males only t=-7.45, P<0.001).
Comparison of the means seems to suggest that the brain weight of deceased elderly cases of suicide or an open verdict after FSH was significantly higher than that of those who died naturally. There was no significant difference in brain weight between the two groups, indicating that open verdict and suicide cases belong to the same population within the FSH group.
Nor was there any significant difference between mean brain weights for all methods of death in the FSH group (ANOVA P>0.05), nor any significant variations in brain weight with cause of death within the comparison group (cardiac, cardiovascular or respiratory causes). The brain weights of all those who had died naturally or fatally harmed themselves were nevertheless within the expected normal range for this age group.
DISCUSSION
Limitations of the study
A number of factors may have influenced the study findings and should be considered when interpreting the results.
-
(a) Bias may have resulted from the method the pathologists used in removing the brains for examination. The method described in Knight's (Reference Knight1996) forensic textbook seems to be an internationally accepted standard used by pathologists. However, any such bias is likely to have been random, thus equally affecting the groups of FSH and those who died naturally.
-
(b) Information bias might have arisen from the many different pathologists' reports used for data collection, as well as from the records of two different coroners, with some variation in the quality and style of reporting. However, all the coroners' records reviewed were quite detailed, accurate and highly organised. Also, the FSH and control groups were equally distributed between the two coroners (35% v. 65%, for both cases and controls).
-
(c) The time between death and postmortem examination might have varied. However, in all subjects, whether death was due to natural causes or FSH, post-mortem examination was reported in the records to have been carried out within 6-12 hours of death.
-
(d) Bias may have resulted from variations in method, cause and, in particular, mode of death. In almost all FSH cases, death was sudden or rapid. Deaths due to natural causes were selected from cases of unexpected or unexplained death, mostly either rapid or sudden, referred for hospital autopsies or coroner's post-mortem. It was difficult, if not impossible, to match the two groups accurately by mode of death, other than in general terms (rapid as opposed to slow or prolonged). In the majority of natural deaths, the direct cause was reported as cardiovascular, which would have been rapid.
-
(e) Although cases were matched for age, the possibility of preclinical dementia in the group of hospital autopsies cannot be excluded. This might have led to somewhat lower brain weights in this group.
-
(f) The unavailability of pre-study data to determine sample size and study power may limit the study's inferential value. The difference in mean values may have been the result of bias (a), above, rejecting a true null hypothesis of no difference. However, an adequate level of significance was used to guard against such error.
Interpretation of the findings
Brain weights vary with age, gender, cause and mode of death and what happened to the brains after death (Reference KnightKnight, 1996). The brain is usually examined immediately (‘wet cutting’) or is suspended in formalin until fixed, a process which takes several weeks. In the majority of autopsies there is no real need for fixation if no cerebral lesions are suspected, expected or apparent on external examination (Reference KnightKnight, 1996). In this study all brain weights were reported as ‘wet’ autopsy weights where no formalin fixation was used, so increased weight cannot be attributed to the fixation process.
The increase in brain weight in association with histological signs of oedema in hanging was put down to a definite terminal post-mortem brain swelling, as it is known in all forms of peracute death caused by unrestricted arterial flow but reduced venous return from intracranial sinuses (Reference Schröder and SaternusSchröder & Saternus, 1983). Cerebral oedema can be caused by hypoxia, intracranially due to direct or indirect trauma, or from any part of the body, and, whether traumatic or hypoxic, the cerebral oedema is self-potentiating and develops surprisingly quickly (Reference KnightKnight, 1996). The neuropathological findings in irreversible coma give similar findings of brain swelling and softening.
Walker et al (Reference Walker, Diamond and Moseley1975), in their study on cerebral survival, reported that brain weight fluctuated, increasing during the first 24 hours after resuscitative measures were started, falling on the second day and then rising again. Patients in whom resuscitation was stopped on the basis of presumed brain death had on the average heavier brains (70 g, P<0.01).
Respirator brain syndrome is described by Walker et al (Reference Walker, Diamond and Moseley1975) as a dynamic process that may progress until pulmonary or cardiac disturbances terminate the patient's life or until resuscitation is stopped. The changes seen in respirator brain result from impaired cerebral blood flow causing brain swelling, complicated by concurrent post-mortem changes (Reference Moseley, Molinari and WalkerMoseley et al, 1976). This process requires approximately 24 hours for maturation (Reference Walker, Diamond and MoseleyWalker et al, 1975). Factors contributing to respirator brain are acute ischaemia, acidosis, hypoxia, low systolic blood pressure, subnormal temperature, history of respiratory dependency and extensive tissue necrosis (Reference Moseley, Molinari and WalkerMoseley et al, 1976), and probably present before death in some cases. Although a mechanism similar to that in respirator brain syndrome may provide partial explanation for our findings, it cannot fully explain the relative increase in brain weight in those who died of fatal self-harm, regardless of the method of death, compared to those who died naturally.
The element of bias in the study, although systematic, probably occurred randomly in both groups, so it is unlikely to be solely responsible for the study findings. Moreover, the sample included only persons over the age of 60, so the results cannot be generalised to younger age groups. However, it may prove difficult to obtain enough young subjects who have died naturally to match for age with those who die of FSH. Prospective studies with carefully selected and matched cases and controls may overcome the limitations encountered in this retrospective exploratory study. Data could be obtained from routine neuropathological examination, macroscopically and microscopically assessing the extent of cerebral oedema, brain chemistry and the state of its receptors at death; such investigations should be carried out as a matter of course for all victims of fatal self-harm. As we are dealing with small number of cases (9.7 per 100000) the cost would not be expected to be prohibitive, and the process is certainly feasible.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Brain weight in all methods of fatal self-harm (FSH) was found to be significantly greater than in death from natural causes. There was no significant difference in brain weight for different methods of FSH. Brain weights for all those who died naturally or fatally harmed themselves were nevertheless within the expected normal range for this age group.
-
▪ This unexpected finding requires critical examination, particularly in view of the reported bias, which may have significantly influenced the results.
-
▪ We propose a confidential neuropathological database for all FSH incidents, containing classified neurohistochemical findings.
LIMITATIONS
-
▪ Bias may have resulted from the method which the pathologists used in brain removal for examination, the fact that many different pathologists' reports were used for data collection, variations in method, cause and mode of death, and the possibility of the presence of preclinical dementia in some cases.
-
▪ Mode of death as a confounder is probably a crucial factor that we were unable to control due to the nature of data collection.
-
▪ The undetermined study power may limit its inferential value.
ACKNOWLEDGEMENTS
The authors are grateful to the Coroners' Offices of Birmingham and Warrington for their support, and to Sheila Cawley, Michael Salib, Jeanie Hedley and Kate Spencer for their help in data collection and preparing the manuscript.




eLetters
No eLetters have been published for this article.