



Introduction
Since its introduction by Bowlby (Reference Bowlby1969), attachment theory has given insight into how early social experiences, including loss and trauma, may affect human behavior and mental processes. According to Bowlby (Reference Bowlby1973), children form expectations of the world, themselves, and their attachment figures. Attachment figures are preferred persons, such as parents, to whom children turn when anxious or alarmed. Children's expectations of their attachment figures, developing throughout childhood and adolescence, help them to be effective in eliciting support and protection when needed. Loss and other events that disrupt the accessibility of attachment figures as sources of comfort may therefore be cause for alarm. After the loss of an attachment figure, attached persons usually go through a process of mourning. Bowlby (Reference Bowlby1980) proposed several components of mourning. Following the first shock of loss, persons may initially continue to search for and yearn for contact with the deceased. Usually, the complex set of emotions gives way to reorganization of their expectations of the world – one in which they can no longer turn to their loved one in times of distress. For some persons, such reorganization continues to be a challenge, and as a result these persons may enter a chronic state of unresolved mourning. Bowlby's (Reference Bowlby1980) framework can also be applied to understand other unresolved trauma involving attachment figures, such as physical or sexual abuse. For instance, persons who experienced parental abuse in childhood may continue struggling with the idea of a world wherein their parent has not always been protective. In addition, reorganization of abuse experiences may be elicited when they later recognize that other parents can be sensitive and protective. In such cases, unresolved trauma may entail efforts to distance oneself from the abuse or its potential psychological effects.
Drawing on Bowlby's (Reference Bowlby1980) ideas, Main and colleagues developed a linguistic framework for assessing adults’ disorganized state of mind about loss or trauma, as expressed through their narrative about childhood memories (Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990). The Adult Attachment Interview (AAI; George, Kaplan, & Main, Reference George, Kaplan and Main1984, Reference George, Kaplan and Main1985, Reference George, Kaplan and Main1996) was introduced as an interview about early family relationships and includes opportunities for participants to discuss experiences of loss, abuse, and other potential trauma. Interviewees are asked to bring to mind and discuss attachment-related experiences, all the while maintaining a coherent narrative for the interviewer to follow (Hesse, Reference Hesse1996). Main and her colleagues concluded that an unresolved/disorganized/disoriented (U/d) state of mind regarding loss or trauma is expressed through lapses in the monitoring of reasoning or discourse (unresolved discourse) in the interviewee's narrative about these experiences (Main, DeMoss, & Hesse, Reference Main, DeMoss and Hesse1991/1994; Main, Goldwyn, & Hesse, Reference Main, Goldwyn and Hesse2003). These lapses may indicate disrupted or irrational ideas about loss or abuse (e.g., by expressing beliefs that a loved one who died long ago is still alive) or losing track of the interview context (e.g., by changing to a eulogistic style of speech). Unresolved states of mind are overrepresented in clinical populations (Bakermans-Kranenburg & Van IJzendoorn, Reference Bakermans-Kranenburg and Van IJzendoorn2009) and have been associated with frightening, frightened, and dissociated parenting behaviors (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van IJzendoorn, Moran, Pederson and Benoit2006).
Questions remain about the generative mechanisms underlying these phenomena. Main and Hesse (Reference Main, Hesse, Ammaniti and Stern1992) theorized that unresolved loss/trauma reflects memories containing perceptions that were partially processed or dissociated due to their overwhelmingly distressing or frightening nature. When the AAI directs attention to these memories, the speaker may experience frightening intrusions of the loss or trauma, flooded working memory, and reduced ability to produce coherent reasoning or speech. In addition, Hesse (Reference Hesse, Cassidy and Shaver2016) suggested that individual differences in coherent discourse in the AAI may reflect “differences in what are presumed to be deeply internalized strategies for regulating emotion and attention” (p. 557). Based on these explanations, emotional dysregulation is likely to go along with unresolved discourse about loss or trauma. However, this hypothesis requires further specification and empirical testing. Indicators of emotional arousal, such as activity of the autonomic nervous system (ANS; Kreibig, Reference Kreibig2010), may provide insight into the regulatory mechanisms involved in unresolved states of mind. Previous studies suggest that adults’ recall of childhood loss or trauma is associated with dysregulated ANS reactivity (Bernstein, Measelle, Laurent, Musser, & Ablow, Reference Bernstein, Measelle, Laurent, Musser and Ablow2013; Dale et al., Reference Dale, Shaikh, Fasciano, Watorek, Heilman and Porges2018; Koopman et al., Reference Koopman, Carrion, Butler, Sudhakar, Palmer and Steiner2004; Luecken, Reference Luecken, Stroebe, Hansson, Schut and Stroebe2008). Thus far, only one study investigated the relation between unresolved states of mind and ANS reactivity during the AAI, using a sample of adolescents (Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn, & Juffer, Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008). These authors connected ANS reactivity to the questions in the AAI and found a significant relation between responding to the loss question and higher interbeat interval (IBI) reactivity, compared to the baseline, during which the participants completed a questionnaire. However, this relation was not moderated by being classified as U/d. The current study aimed to contribute to understanding of unresolved states of mind by examining relations between unresolved loss/trauma in the AAI and indicators of ANS reactivity.
ANS reactivity, emotional arousal, and social behavior
Emotional arousal can be measured by activity of the ANS (Balzarotti, Biassoni, Colombo, & Ciceri, Reference Balzarotti, Biassoni, Colombo and Ciceri2017; Kreibig, Reference Kreibig2010; Levenson et al., Reference Levenson, Lwi, Brown, Ford, Otero, Verstaen, Berntson, Cacioppo and Tassinary2016). The two branches of the ANS, the parasympathetic and the sympathetic nervous system, regulate vital functions of the body including the cardiovascular system, and contribute to controlling bodily arousal (Berntson et al., Reference Berntson, Cacioppo, Binkley, Uchino, Quigley and Fieldstone1994; Cacioppo, Uchino, & Berntson, Reference Cacioppo, Uchino and Berntson1994). According to polyvagal theory (Porges, Reference Porges2003, Reference Porges2007), the ANS responds to environmental threats through a process called neuroception and supports cognitive and behavioral responses for coping. Porges (Reference Porges2003) proposed that perceptions of safety and threat affect the extent to which individuals can engage in social behavior. The parasympathetic nervous system is responsible for maintaining homeostasis when there is no environmental risk. During states of relaxation, the influence of the parasympathetic tone on the heart is high, which slows down the heart rate, supports restoration of the body's organs, and facilitates social engagement. When neuroception evaluates the environment as threatening, the parasympathetic nervous system withdraws, allowing for an increase of sympathetic nervous system activity, which speeds up the heart rate and helps prepare the body for a fight-or-flight response. This internal state is expected to hinder the fluent expression of social engagement behaviors (Porges, Reference Porges2003). Thus, to understand the mechanisms involved in unresolved states of mind, it may be informative to study indicators of parasympathetic and sympathetic reactivity and their linkages with discourse about loss or trauma.
In psychophysiological research, heart rate is the most commonly used indicator of physiological reactivity in relation to emotion (Levenson et al., Reference Levenson, Lwi, Brown, Ford, Otero, Verstaen, Berntson, Cacioppo and Tassinary2016). Heart rate is regulated by both the parasympathetic and sympathetic nervous system (Berntson et al., Reference Berntson, Cacioppo, Binkley, Uchino, Quigley and Fieldstone1994). Therefore, it provides limited insight into the specific involvement of these systems. In research on mental health and ANS functioning, parasympathetic nervous system response is often indicated by the high-frequency component of heart rate variability (HF-HRV). Another widely used indicator of parasympathetic reactivity is respiratory sinus arrhythmia (RSA), which is a naturally occurring variation in heart rate synchronized with the respiratory cycle (Berntson, Cacioppo, & Quigley, Reference Berntson, Cacioppo and Quigley1993). Sympathetic nervous system response is frequently indicated by electrodermal activity such as skin conductance level (SCL) (Levenson et al., Reference Levenson, Lwi, Brown, Ford, Otero, Verstaen, Berntson, Cacioppo and Tassinary2016), and by preejection period (PEP), an index of contractility of the heart (Sherwood et al., Reference Sherwood, Allen, Fahrenberg, Kelsey, Lovallo and van Doornen1990). The current study included these measures of parasympathetic and sympathetic response. These measures and their associations with states of deactivation (rest) and activation (stress/arousal) are presented in Table 1.
Table 1. Indicators of ANS response and relations with states of deactivation and activation
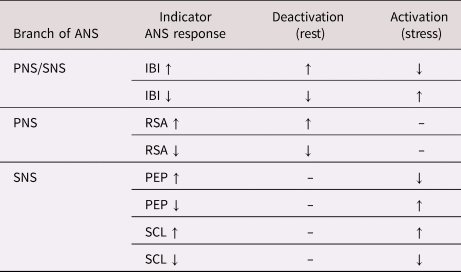
Note. IBI = interbeat interval, an indicator of heart rate; PNS = parasympathetic nervous system; SNS = sympathetic nervous system.. Arrows indicate increased (↑) or decreased (↓) values (indicators of ANS response) or states (deactivation/activation). Based on Berntson et al. (Reference Berntson, Cacioppo, Binkley, Uchino, Quigley and Fieldstone1994), Levenson et al. (Reference Levenson, Lwi, Brown, Ford, Otero, Verstaen, Berntson, Cacioppo and Tassinary2016), and Porges (Reference Porges2007).
Loss, trauma, and ANS reactivity
To date, few researchers have examined ANS reactivity during the AAI (Beijersbergen et al., Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008; Dozier & Kobak, Reference Dozier and Kobak1992; Roisman, Tsai, & Chiang, Reference Roisman, Tsai and Chiang2004). Both Dozier and Kobak (Reference Dozier and Kobak1992) and Roisman et al. (Reference Roisman, Tsai and Chiang2004) used the Adult Attachment Interview Q-Set (Kobak, Reference Kobak1989/1993) to code the interviews, which does not include a scale for assessing unresolved loss or trauma. Beijersbergen et al. (Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008) did not find that responses to the loss and trauma questions in the AAI were associated with the interview being classified as U/d. However, their analysis did not control for differences between the groups in type of unresolved experience discussed (i.e., loss, abuse, or other potential trauma). Furthermore, as Beijersbergen et al. (Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008) mentioned in the discussion, this study only focused on the specific interview questions that probe for loss and trauma. Because speakers can bring up loss and trauma anywhere in the interview, linking ANS reactivity to discussion of these experiences across the entire AAI may provide more insight. Moreover, the direct association between individual instances of unresolved discourse and ANS response on a micro-level was not addressed.
Findings outside the realm of attachment theory suggest that recall of trauma may be linked to aberrant ANS reactivity. Studies in which participants were asked to recall traumatic memories have linked posttraumatic stress disorder (PTSD) and trauma-related dissociation to blunted ANS response (Griffin, Resick, & Mechanic, Reference Griffin, Resick and Mechanic1997; Koopman et al., Reference Koopman, Carrion, Butler, Sudhakar, Palmer and Steiner2004; Sack, Cillien, & Hopper, Reference Sack, Cillien and Hopper2012). In the study by Griffin et al. (Reference Griffin, Resick and Mechanic1997), which involved female victims of rape, participants with high dissociation showed blunted skin conductance responses and decreasing heart rate when discussing their trauma. During a similar task, Sack et al. (Reference Sack, Cillien and Hopper2012) found a relation between dissociation and decreasing heart rate, as well as diminished RSA reactivity. A study involving female undergraduates with a history of trauma showed that participants with high dissociation had larger decreases in RSA and shorter PEP when recalling traumatic memories, indicating withdrawal of the parasympathetic nervous system and increased fight-or-flight responses (Sledjeski & Delahanty, Reference Sledjeski and Delahanty2012).
Similarly, studies among persons with PTSD found decreasing parasympathetic reactivity during trauma recall tasks (Keary, Hughes, & Palmieri, Reference Keary, Hughes and Palmieri2009; Sack, Hopper, & Lamprecht, Reference Sack, Hopper and Lamprecht2004). For example, Sack et al. (Reference Sack, Hopper and Lamprecht2004) found a pattern of decreasing RSA accompanied by increased heart rate, suggesting involvement of both the parasympathetic and sympathetic nervous system. In contrast, Chou, La Marca, Steptoe, and Brewin (Reference Chou, La Marca, Steptoe and Brewin2018) found that persons with PTSD showed increased parasympathetic reactivity (indicated by HF-HRV) when asked to recall their traumatic experience, which is inconsistent with other findings (e.g., Keary et al., Reference Keary, Hughes and Palmieri2009). According to the authors, their choice of a neutral recall baseline as compared to resting baseline in other studies may have partially contributed to this inconsistency, because both speaking and recalling memories may affect measures of cardiovascular activity (Chou et al., Reference Chou, La Marca, Steptoe and Brewin2018). Taken together, PTSD and trauma-related dissociation are linked to dysregulated ANS responses, although not consistently. Following the theoretical propositions about unresolved states of mind (e.g., Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990) this indirect evidence points to the possibility that dysregulated ANS reactivity may be underlying unresolved discourse. However, as available work in attachment theory does not provide clarity about the psychological processes of unresolved discourse and unresolved states of mind, the expected nature of this relation (e.g., heightened or diminished ANS reactivity) is uncertain.
This study
In the current study, we tested ANS responses as indices of emotional arousal involved in U/d states of mind about loss/trauma. First-time pregnant women participated in the AAI while ANS response was recorded, allowing assessment of parasympathetic and sympathetic nervous system response. We examined associations between ANS reactivity and (a) responding to questions about loss, abuse, and other trauma; (b) discussion of experiences of loss/trauma anywhere in the interview; (c) the interview being classified as U/d; and (d) instances of unresolved discourse about loss/trauma. The study design, hypotheses, and data analytical procedures were preregistered on Open Science Framework (http://doi.org/10.17605/OSF.IO/A4J6Q). The following hypotheses were tested:
1. It was hypothesized that responding to questions about loss/trauma would be associated with changes in ANS reactivity, and that this association would be moderated by unresolved status.
2. It was hypothesized that discussion of loss/trauma anywhere in the interview would be associated with changes in ANS reactivity, and that this association would be moderated by unresolved status.
3. It was hypothesized that unresolved discourse in response to questions about loss/trauma would be associated with changes in ANS reactivity.
4. It was hypothesized that unresolved discourse anywhere in the interview would be associated with changes in ANS reactivity.
Method
Participants
Data were used from the ongoing Generations2 longitudinal study on parenthood and the development of the parent-child relationship. First-time pregnant women (N ~2,000) in the larger cohort were recruited through midwifery practices, pregnancy fairs, and the project's website. The current study used data from a focus sample of women who were invited to participate in intensive measurements including the AAI (N = 254). This focus sample consists of first-time pregnant women from normative and high-risk groups. Women in the normative group (n = 135) were invited for participation after their first prenatal questionnaires were received (around 12 weeks of pregnancy). The high-risk group (n = 119) included 56 women who reported visiting a psychologist or psychiatrist or being in youth care before the age of 18, and five women who reported heightened scores on prenatal assessments of depression and anxiety. Fifty-eight women in the high-risk group were recruited from youth care organizations or institutions, or from prenatal parenting programs for at-risk women. Women were excluded for participation in the study if they reported a prenatal diagnosis for a congenital abnormality of the fetus.
Only women who reported any loss or trauma experiences in the AAI were selected for this study (N = 235), of whom 51% were from the normative group and 49% from the high-risk group. For the purposes of the current study and because the same measures were used, women from both groups were combined into one group. When the AAI was administered, during second or third trimester of pregnancy, women's ages ranged from 15 to 41 years (M = 27.88, SD = 6.02). The majority of women had parents who were born in the Netherlands (88%). Most women (54%) were highly educated with a bachelor's or master's degree, 22% had completed further vocational education, 16% had completed secondary school, and 4% had completed up to eight groups of primary education. Regarding marital status, 85% of women had a partner, of whom 50% were cohabiting and 41% were married. Fifteen percent of women were single.
This study used data collected during the second or third trimester of pregnancy, depending on the time of recruitment. The data were collected between 2009 and 2013. Before the start of the study, all women signed informed consent, and if younger than 18 years, also their legal guardians. Women were home-visited by a trained interviewer to conduct the AAI, during which signals of electrocardiography (ECG), impedance cardiography (ICG), and skin conductance were recorded. Women from the normative group received a 60-euro gift card after the first year of measurements was completed, and women from the at-risk group received financial compensation after each measurement, with a total of 100 euro. This study has been approved by the Medical Ethical committee of the Vrije Universiteit Medical center (NL24319.029.08).
Measures
Unresolved loss and trauma
Participants’ unresolved states of mind about loss or trauma were assessed using the Dutch version of the AAI (George, Kaplan, & Main, Reference George, Kaplan and Main1996; van IJzendoorn et al., Reference Willemsen, de Geus, Klaver, Van Doornen and Carroll1991). The AAI is a semi-structured interview consisting of 20 questions with follow-up probes and covers one's early relationship experiences with their caregivers, including reflections on how these experiences have affected their development into adulthood. The interviews were transcribed verbatim. Trained coders of the AAI, who established reliability on the Berkeley reliability set, rated the interview transcripts for unresolved discourse about loss or trauma (i.e., lapses in the monitoring of reasoning or discourse) using the coding system by Main and colleagues (Reference Main and Goldwyn1994, Reference Main, Goldwyn and Hesse2002). Unresolved responses were rated on two separate rating scales, one for unresolved loss and one for unresolved trauma (range 1–9). Interviews were classified into the U/d category if they contained significant unresolved responses to loss or trauma, usually on the basis of a score of 6 or higher on either of the unresolved rating scales. The average kappa score between three AAI coders for the U/d classification was 0.72 (range 0.58–1.00; based on 15 interview transcripts).
Of the 254 participants from which our subsample was drawn, 20% (n = 51) were classified as U/d. This proportion did not differ from the proportion of U/d classifications in nonclinical samples (Bakermans-Kranenburg & Van IJzendoorn, Reference Bakermans-Kranenburg and Van IJzendoorn2009), χ2(1, N = 254) = 0.40, p = .525. Classification into the U/d category was an independent variable in this study and was dichotomously coded (0 = not classified as U/d, 1 = classified as U/d).
This study included behaviorally focused subquestions on trauma. These questions were already included in the AAI protocol that was used, as recommended by Bailey, Moran, and Pederson (Reference Bailey, Moran and Pederson2007) and Madigan, Vaillancourt, McKibbon, and Benoit (Reference Madigan, Vaillancourt, McKibbon and Benoit2012), and were more deliberately probed by the interviewers in this study: (a) “Were you ever hit as a child?”; if confirmed: “Could you tell me more about what happened?”, “Could you describe the circumstances?”, “How old were you at the time?”, “How often did it happen?”. If the circumstances were still unclear: “Could you think of a specific time that it happened?”, “Was there an object used?”, “Where on your body were you hit?”, “Did it ever leave marks?”; (b) “Some people have had negative sexual experiences in their childhood. Did anything like that ever happen to you or someone in your family?”. If confirmed: “Could you tell me more about what happened?”, “How old were you at the time?”, “How often did it happen?”. If the circumstances were still unclear: “What did he/she try to do to you?”, “Did he/she use physical coercion to threaten or hurt you?”; (c) “Some people have memories of threatening experiences, maltreatment, or abuse by people outside their family, during childhood. Did anything like that ever happen to you or someone in your family?”; and (d) “Do you have memories of threatening experiences, maltreatment, or abuse by people outside of your family, after you were 12 years old? Or did anything like that happen to someone in your family?”. After each discussed experience, the speaker was asked about how they felt the experience still affected them as an adult.
To be able to connect discussions of loss/trauma to recordings of ANS reactivity, these experiences were extracted from the AAI scoring sheets and marked interview transcripts and were then linked to the time points in the interview audio recordings. The data were prepared through the following steps: (a) a team of 11 undergraduates listened to the interview audio recordings while reading the marked transcripts and AAI scoring sheets; (b) in a separate Excel file, the undergraduates took notes of the time points at which interviewees discussed loss/trauma; (c) the first author (who received training in coding the AAI by Main and Hesse on 12–23 June 2017, Berkeley) went back to the original marked transcripts and AAI scoring sheets to check the students’ notations of trauma and corrected them where necessary; (d) the first author used the original marked interview transcripts to identify instances of unresolved discourse about loss/trauma. Marked indices of unresolved discourse were identified in responses to the loss/trauma questions as well as in responses to the other interview questions (see also Table S1 in the Supplementary Materials). For the purposes of this study, discussions of abuse (physical and sexual abuse by attachment figures) and other potential trauma (e.g., abuse by non-attachment figures, car accidents) were both marked as “trauma.”
Participants’ response to the interview questions was a within-subject independent variable with 21 categories, representing each of the interview questions. The first interview question (asking for an overview of the speaker's early family situation) was used as the baseline. Interview question 8 was divided into two categories, each representing a separate part of the question: one about experiences of rejection by caregivers, and one about feelings of worry or fright. This decision was made because of the possibility that speakers would bring up loss/abuse when asked about the latter.
Per interview question, it was indicated whether participants discussed any loss/trauma, and whether they showed any indications of unresolved discourse. Discussion of loss/trauma and unresolved discourse about loss/trauma were within-subject independent variables. These were dichotomously coded (0 = no loss/trauma discussed, 1 = loss/trauma discussed; 0 = no unresolved discourse, 1 = unresolved discourse). Figure 1 presents an overview of the within-subject independent variables.

Figure 1. Within-subject independent variables. The first two interview segments are presented here, corresponding to participants’ responses to the first two Adult Attachment Interview (AAI) questions.
Autonomic nervous system reactivity
During administration of the AAI, signals of ECG, ICG, and skin conductance were recorded using the Vrije Universiteit Ambulatory Monitoring System (VU-AMS; De Geus, Willemsen, Klaver, & Van Doornen, Reference De Geus, Willemsen, Klaver and Van Doornen1995; Willemsen, de Geus, Klaver, Van Doornen, & Carroll, Reference Willemsen, de Geus, Klaver, Van Doornen and Carroll1996). A lead wire connector and seven disposable gelled ECG electrodes were used for recording the ECG and ICG. The electrodes were positioned on the participants’ bodies according to standard procedures described for the VU-AMS, while participants were sitting at a table (De Geus et al., Reference De Geus, Willemsen, Klaver and Van Doornen1995; Willemsen et al., Reference Willemsen, de Geus, Klaver, Van Doornen and Carroll1996). The ICG signal (dZ/dt) was derived from the change in thoracic impedance (dZ) due to pulsatile variation. For skin conductance, a separate wire connector was used with an electrode holder filled with gel for the index and middle or ring finger.
The VU-DAMS software (version 4.0; Pelt & Viswanathan, Reference Pelt and Viswanathan2015) was used to divide the physiological data into labelled segments indicating participants’ responses to the interview questions. Each interview segment also indicated whether loss or trauma was discussed and/or if the segment contained indices of unresolved discourse. The physiological data were labelled by the first author and the undergraduate students involved in this project. Data labelled by the undergraduate students were corrected by the first author if necessary. This study included indicators of heart rate (IBI), sympathetic reactivity (PEP and skin conductance) and parasympathetic reactivity (RSA), which were averaged across the interview questions. IBI is defined as the time (ms) between two consecutive R-peaks in the ECG signal and was automatically scored by the software. Ensemble averaged ICG (dZ/dt) waveforms were computed across the interview questions and were automatically scored for the specific locations of the upstroke (B-point), dZ/dtmin (C-point), and incisura (X-point). From these points, PEP was acquired, defined as the time (ms) from the Q-wave onset in the ECG complex to the B-point in the ICG waveform (Riese et al., Reference Riese, Groot, Van den Berg, Kupper, Magnee, Rohaan and de Geus2003). The ICG waveforms were visually inspected, and morphologically inconsistent B-points were manually corrected following the guidelines by Sherwood et al. (Reference Sherwood, Allen, Fahrenberg, Kelsey, Lovallo and van Doornen1990). To ensure reliability, a set of 14 subjects (n = 577 ICG waveforms) were double-coded by the first and second author, which yielded excellent interrater reliability (ICC = .99; single measures, absolute agreement).
The tonic component of skin conductance was used in this study (also referred to as skin conductance level; SCL). The frequency of the skin conductance signal (μS) was 10 samples per second (10 Hz; signal range 0–95 Hz). Clipping levels were automatically detected and removed from further analysis. To estimate RSA, the VU-DAMS software utilizes the peak-to-valley method (De Geus et al., Reference De Geus, Willemsen, Klaver and Van Doornen1995; Grossman, Van Beek, & Wientjes, Reference Grossman, Van Beek and Wientjes1990) which combines heart period (IBI) and respiratory data. The respiration signal was acquired from the filtered (0.1–0.4 Hz) dZ signal. For each respiratory cycle, RSA (ms) was computed by subtracting the shortest IBI during the inhalation interval from the longest IBI during the exhalation interval. Respiratory cycles were scored automatically by the software algorithm. RSA values were positively skewed (skewness = 1.47). Therefore, RSA was transformed to its natural logarithm (skewness = −.36).
Per interview segment, outliers were defined using standardized values (z scores < −3.29 | > 3.29) following Tabachnick and Fidell (Reference Tabachnick and Fidell2013). Outlying values were winsorized: the outliers were replaced by the next-most extreme non-outlying values. One outlying IBI value, 26 RSA values, 6 PEP values, and 2 SCL values were winsorized. In addition, we found 30 zero-values of SCL, which were set to missing. Overall, less than 0.1% of data were missing for IBI, 2% were missing for RSA, 3% were missing for PEP, and 1% were missing for SCL.
Statistical procedure
R version 3.5.2 (R Core Team, 2018) was used for the analyses. First, descriptives of the study variables were calculated, which included distributions of the outcome variables (IBI, RSA, PEP, SCL), and frequencies of the independent variables (participants’ discussion of loss/trauma, and indices of unresolved discourse). Secondly, as age may affect cardiovascular measures of psychophysiology (Berntson, Quigley, Lozano, Cacioppo, & Tassinary, Reference Berntson, Quigley, Lozano, Cacioppo, Tassinary, Berntson, Cacioppo and Tassinary2007), we examined whether age should be included as a covariate in the analyses. Logistic regression was used to test the association between age and the interview being classified as U/d.
Hypothesis testing analyses
The study hypotheses were tested using multilevel modeling (linear mixed models; R package nlme, Pinheiro, Bates, DebRoy, & Sarkar, Reference Pinheiro, Bates, DebRoy and Sarkar2018). Multilevel modeling is commonly used in psychophysiological studies, because it considers the hierarchical structure of the data and handles nonindependent observations by including the possibility to fit random intercepts and random slopes for the independent variables (Page-Gould, Reference Page-Gould, Berntson, Cacioppo and Tassinary2016; Ruwaard, Kooistra, & Thong, Reference Ruwaard, Kooistra and Thong2018). We used a two-level design with repeated measures (level 1) nested within the study participants (level 2).
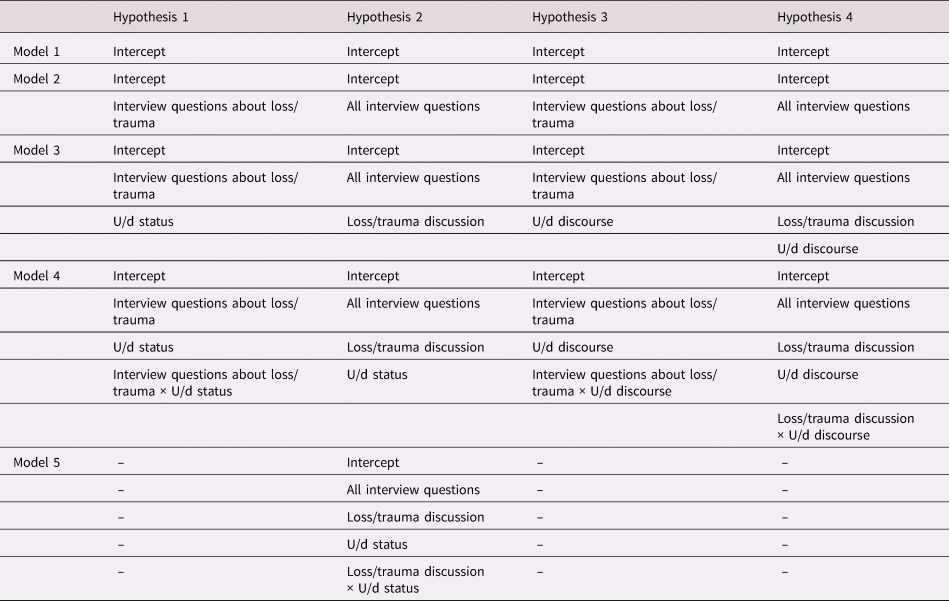
The outcome variables were indicators of ANS response (IBI, RSA, PEP, and SCL), which were averaged across the interview segments. These were within-subject variables (level 1). The following independent variables were entered in the models: (a) within-subject (level 1) categorical variables representing each of the 21 interview questions (dummy-coded), accounting for change in ANS reactivity compared to the baseline (i.e., the first interview question, which was the reference category in the analyses); (b) within-subject (level 1) categorical variables indicating whether an interview segment contained discussion of loss or trauma (dichotomously coded); (c) a within-subject (level 1) categorical variable indicating whether an interview segment contained indices of unresolved discourse (dichotomously coded); and (d) a between-subject (level 2) variable indicating participants’ classification of U/d (dichotomously coded) (see also Figure 1). An autocorrelated covariance structure was used, which is considered appropriate for repeated measures designs in which the order of the observations is important (Page-Gould, Reference Page-Gould, Berntson, Cacioppo and Tassinary2016). Maximum likelihood estimation was used to estimate the model parameters. Likelihood ratio tests were performed to compare the goodness of fit between two subsequent models. Pairwise comparisons (estimated marginal means) were calculated to follow-up on significant findings.
Each hypothesis was tested with different unconditional and conditional growth models, of which the specific variables are presented in Table 2. For all hypotheses, an unconditional means model (Model 1) was first estimated. This model included only a random intercept, which was used to assess the degree of nonindependency in ANS responses across the interview segments (within-subject observations). Intraclass correlation coefficients (ICC) were computed to examine how much of the variance in ANS reactivity (on the within-subject level) would be accounted for by differences between participants. ICCs close to zero would imply statistical independence of the within-subjects observations (Hayes, Reference Hayes2006). In the next step, for all hypotheses, an unconditional growth model with a random intercept would be estimated (Model 2), in which the dummy variables representing the 21 interview questions were added as predictors. These variables accounted for change in the indicators of ANS reactivity across the interview questions, with the baseline (i.e., the first interview question) as the reference category. Next, we would include a random slope for the interview questions, which would allow participants to vary in ANS reactivity during the interview segments. If adding a random slope model did not improve the model fit, we dropped the random slope and continued with an intercept-only model. The same approach was used regarding participants’ discussion of loss/trauma. As seen in Table 2, subsequent models (i.e., Model 3, 4, and 5) were different for each hypothesis. In Model 3, participants’ U/d classification (level 2), discussion of loss/trauma (level 1), and/or unresolved discourse (level 1) were added as predictors, to investigate whether these variables would be associated with change in the outcome variables, over and above the effect of the interview questions. In Model 4 and Model 5, interactions terms were added involving various combinations of the level 1 and level 2 variables. Effect sizes were determined by calculating f 2, which compares the explained variance (R 2) by the model of interest versus the unconditional means model (Lorah, Reference Lorah2018; see also Cohen, Reference Cohen1992; Snijders & Bosker, Reference Snijders and Bosker2012).
Table 2. Growth models and variables per study hypothesis
Results
Descriptive statistics
Table 3 shows the means and standard deviations of the outcome variables during the baseline and the interview questions about loss, abuse, and other trauma. Frequencies of the within-subject independent variables are presented in the Supplementary Materials (Table S1).
Table 3. Descriptives of the outcome variables per interview question

IBI = interbeat interval, an indicator of heart rate; PEP = preejection period; RSA = respiratory sinus arrhythmia; SCL = skin conductance level.
Preliminary analyses
A binary logistic regression was used to examine the association between age and the likelihood of being classified as U/d in the AAI. The logistic regression model with age as a predictor was not significantly different from the null model (χ2 (1) = 0.665, p = .42). Therefore, age was not included as a covariate in subsequent analyses. In a preliminary analysis for Hypothesis 1, we tested both models with separate interview responses (~5,004 within-subject observations) and combined interview questions and responses (~10,190 within-subject observations). The likelihood ratio estimates of these models were not directly comparable due to differing numbers of observations. Reported analyses included only the responses to the interview questions, because participants could only discuss experiences of loss/trauma and show unresolved discourse when responding to a question. Analyses with the less-parsimonious models are reported in the Supplementary Materials (Table S2).
Hypothesis 1: The effect of responding to questions about loss/trauma on ANS reactivity, and moderation by unresolved status
It was hypothesized that responding to questions about loss/trauma would be associated with changes in ANS reactivity, and that this effect would be moderated by unresolved status. The results of these analyses are reported in Table 4. Including a random slope for the interview questions resulted in nonconvergence of the models, even when the maximum number of iterations was increased and when the random intercept/slope covariance parameter was removed. To obtain convergence, the models reported in Table 4 are random intercept models allowing the intercept, but not the slope, to vary across participants.
Table 4. Hypothesis 1: The effects of responding to questions about loss and trauma on ANS reactivity, and moderation by unresolved/disorganized status
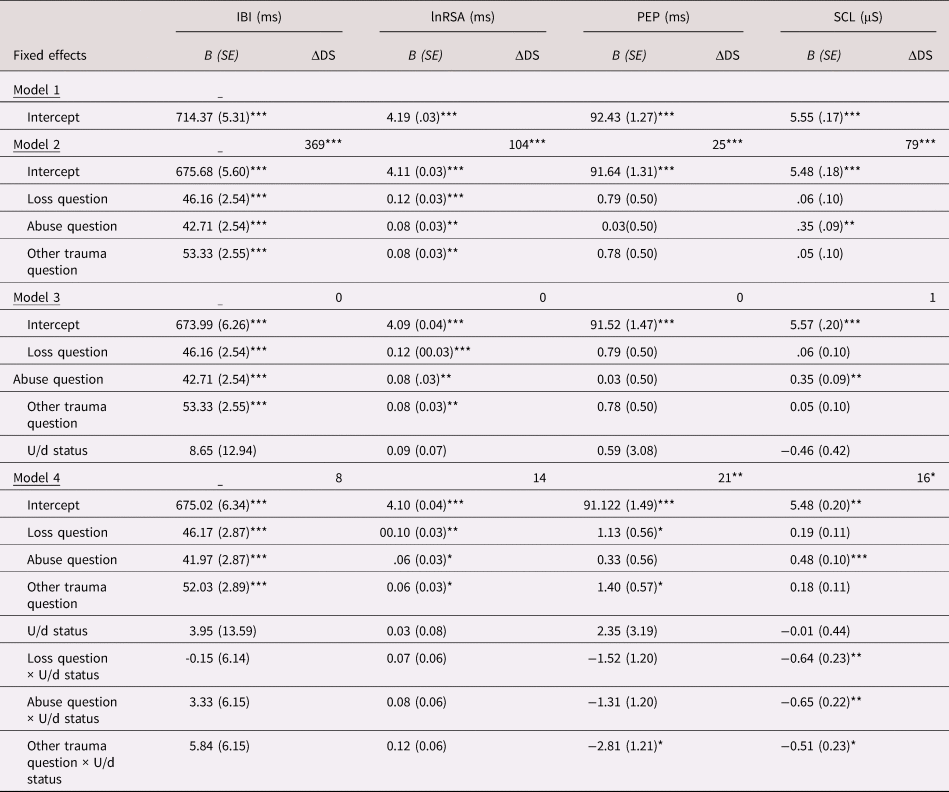
Note. ΔDS = decrease in deviance statistic (Log-likelihood). U/d = being classified as unresolved/disorganized (dichotomous). Responses to the interview questions were coded as dummy variables with the first question as reference. Responses to all 20 interview questions were included in the analyses, but only the questions about loss, abuse, and other trauma are reported in this Table. * p < .05 ** p < .01 *** p < .001
The ICCs from the unconditional means models revealed that a large proportion of the variance in ANS reactivity was accounted for by differences between participants (IBI = 84%, RSA = 70%, PEP = 93%, SCL = 82%), which indicates a high dependency of the within-subject observations, confirming that multilevel modeling is appropriate in this study (Hayes, Reference Hayes2006).
Responding to questions about loss/trauma
Including the interview questions as a predictor to the unconditional means model (Model 2) resulted in an improved model fit for all indicators of ANS reactivity (ps < .001). Larger IBIs and higher RSA were significantly associated with responses to questions about loss (ps < .001), abuse (resp. p < .001 and p = .002), and other trauma (resp. p < .001 and p = .002). For PEP, no significant associations were found (ps > .112). Higher SCL was associated with the abuse question (p < .001), but not with the loss and other trauma questions (ps > .555). The model for IBI explained 4% in variance (f 2 = 0.04), compared to the variance unexplained by the model. Explained model variance was only 1% (f 2 = 0.01) for RSA and 0.05% (f 2 = 0.005) for SCL. Pairwise comparisons showed that IBIs were significantly larger during responses to questions about loss (M = 722.02, SE = 5.60, p < .001), abuse (M = 718.57, SE = 5.60, p < .001), and other trauma (M = 729.19, SE = 5.60, p < .001) compared to baseline (M = 675.86, SE = 5.60).
Moderation by unresolved status
For all indicators of ANS reactivity, the model fit did not improve when unresolved status was included as a predictor (Model 3) (ps > .214). Including the interaction term between questions about loss/trauma and unresolved status (Model 4) did not result in an improved model fit for IBI and RSA (ps > .149). Including the interaction term resulted in an improved model fit for PEP and SCL (resp. p = .002 and p = .035). For PEP, there was a significant interaction effect between unresolved status and responses to the question about other trauma (p = .020), but not for the questions about loss and abuse (ps > .203). For SCL, the interaction effect between unresolved status and responses to questions about loss, abuse, and other trauma was significant (resp. p = .006, p = .003, and p = .032). Explained model variance was a mere 0.2% for PEP (f 2 = 0.002) and 1% for SCL (f 2 = 0.01).
Hypothesis 2: The association between discussion of loss/trauma anywhere in the interview and ANS reactivity, and moderation by unresolved status
It was hypothesized that discussion of actual loss/trauma anywhere in the interview would be associated with changes in ANS reactivity, and that this association would be moderated by unresolved status. The results of these analysesFootnote 1 are reported in Table 5.
Table 5. Hypothesis 2: The association between discussion of actual loss/trauma and ANS reactivity, and moderation by unresolved/disorganized status
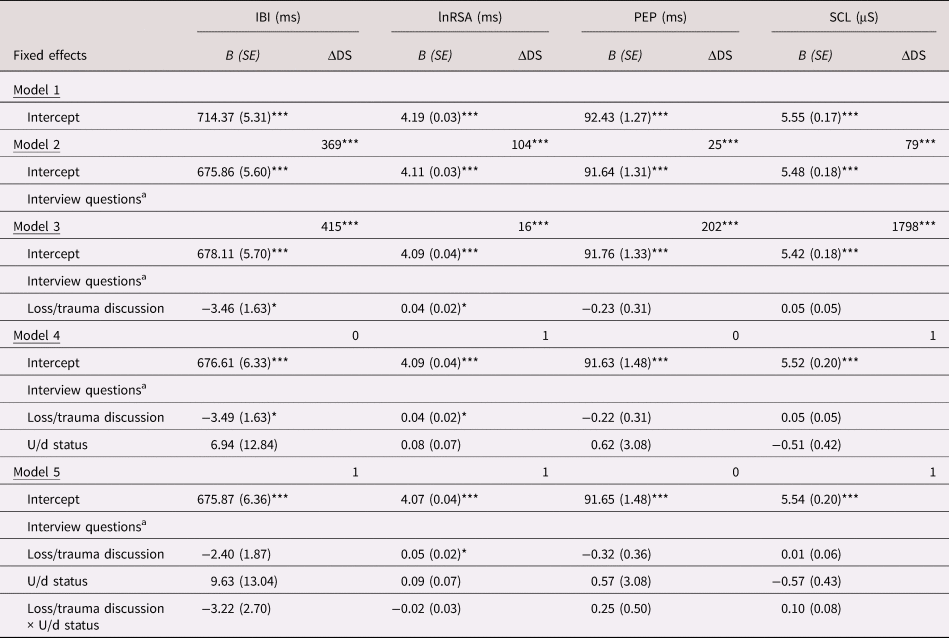
Note. ΔDS = decrease in deviance statistic (Log-likelihood). U/d = being classified as unresolved/disorganized (dichotomous). IBI = interbeat interval, an indicator of heart rate; PEP = preejection period; RSA = respiratory sinus arrhythmia; SCL = skin conductance level.
a Responses to the interview questions were included as predictors, but are not reported in this Table for parsimony. Responses were coded as dummy variables with the first question as reference (baseline). Responses to all 21 interview questions were included in the analyses (5004 within-subject observations).
*p < .05 ** p < .01 *** p < .001
Discussion of loss/trauma anywhere in the interview
Including the interview questions as predictors to the unconditional means model (Model 2) resulted in an improved model fit for all indicators of ANS reactivity (ps < .001). Including discussion of loss/trauma as predictor to the model with the interview questions (Model 3) resulted in an improved model fit for IBI and RSA (resp. p = .033 and p = .035) but not for PEP and SCL (resp. p = .511 and p = .112). For all indicators of ANS reactivity, the model fit improved when random slopes were added (ps < .001), which indicated that participants varied in their ANS reactivity when discussing experiences of loss or trauma. Smaller IBIs (higher heart rate) and higher RSA (more parasympathetic reactivity) were significantly associated with discussion of loss/trauma (resp. p = .034 and p = .018). For PEP and SCL, no significant associations were found (ps > .356). Explained model variance was 13% for IBI (f 2 = 0.13) and 41% for RSA (f 2 = .41). Pairwise comparisons revealed that IBIs were smaller during discussion of loss/trauma (M = 712.68, SE = 5.40, p = .034), compared to when these experiences were not discussed (M = 716.14, SE = 5.38). RSA was higher during discussion of loss/trauma (M = 4.23, SE = 0.03, p = .018), compared to when these experiences were not discussed (M = 4.19, SE = 0.03).
Additional preregistered analyses with separate variables indicating loss or trauma showed that smaller IBIs were significantly associated with discussion of loss but not trauma (resp. p = .005 and p = .691). There was no significant relation between RSA and discussion of loss or trauma (resp. p = .080 and p = .106).
Moderation by unresolved status
For all indicators of ANS reactivity, including unresolved status as a predictor (Model 4) did not improve the model fit (ps > .227). Nor did the model fits improve when the interaction between discussion of loss/trauma and unresolved status was included (Model 5) (ps > .231).
Hypothesis 3: The association between unresolved discourse in response to the loss/trauma questions and ANS reactivity
It was hypothesized that unresolved discourse in response to questions about loss/trauma would be associated with ANS reactivity. The results of these analysesFootnote 2 are reported in Table 6. No unresolved discourse was found in response to questions 16–20, which were therefore excluded from the analysis.
Table 6. Hypothesis 3: The association between unresolved discourse in response to questions about loss/trauma and ANS reactivity

Note. ΔDS = decrease in deviance statistic (Log-likelihood). U/d discourse = unresolved/disorganized responses about loss/trauma (dichotomous). Responses to the interview questions were coded as dummy variables with the first question as reference (baseline). Responses to 15 interview questions were included in the analyses, but only the questions about loss/trauma are reported here (3829 within-subject observations). * p < .05 ** p < .01 *** p < .001
Including the interview questions as predictors to the unconditional means model (Model 2) resulted in an improved model fit for all indicators of ANS reactivity (ps < .001). Including unresolved discourse as a predictor to the model with the interview questions (Model 3) resulted in an improved model fit for IBI (p < .001) but not for RSA, PEP, and SCL (ps > .138). Smaller IBIs (higher heart rate) were associated with unresolved discourse (p = .017). Explained model variance was 3% (f 2 = 0.03). Pairwise comparisons revealed that IBIs were smaller during responses with unresolved discourse (M = 706.45, SE = 5.56, p = .017), compared to responses without unresolved discourse (M = 710.70, SE = 5.31).
Additional preregistered analyses with separate variables indicating loss or trauma showed that smaller IBIs were associated with unresolved discourse about loss but not trauma (resp. p = .018 and p = .313). The model fits did not improve when the interaction term between the interview questions and unresolved discourse was included (Model 4) (ps > .078).
Hypothesis 4: The association between unresolved discourse about loss/traumaanywhere in the interview and ANS reactivity
It was hypothesized that unresolved discourse anywhere in the interview would be associated with ANS reactivity. The results of these analysesFootnote 3 are reported in Table 7. These models included a random slope for discussion of loss/trauma.
Table 7. Hypothesis 4: The association between unresolved discourse about loss/trauma anywhere in the interview and ANS reactivity

Note. ΔDS = decrease in deviance statistic (Log-likelihood). U/d discourse = unresolved/disorganized responses about loss/trauma (dichotomous).
a Responses to the interview questions were included as predictors, but are not reported in this Table for parsimony. Responses were coded as dummy variables with the first question as reference (baseline). Responses to 15 interview questions were included in the analyses (3829 within-subject observations).
*p < .05 ** p < .01 *** p < .001
Including the interview questions as predictors to the unconditional means model (Model 2) resulted in an improved model fit for all indicators of ANS reactivity (ps < .001). For all indicators of ANS reactivity, the model fit improved when discussion of loss/trauma and unresolved discourse were included as predictors to the model with the interview questions (Model 3; ps < .001 for IBI, PEP, and SCL, p = .002 for RSA). There was no significant association between unresolved discourse and IBI (p = .073). However, additional preregistered analyses with separate variables indicating loss or trauma showed that smaller IBI was associated with unresolved discourse about loss (p = .047), over and above the effect of discussion of loss (p = .049). Explained model variance was 13% (f 2 = 0.13).
For RSA, PEP, and SCL, no significant associations were found (ps > .381), also not when examining separate variables indicating loss or trauma. The model fit indices did not improve further when the interaction term between discussion of loss/trauma and unresolved discourse was included (Model 4) (ps > .294).
Exploratory analyses
Exploratory analyses were performed to follow up on some of the hypothesis testing results. These analyses were not preregistered, hence their exploratory nature.
Unresolved discourse during the interview baseline
We discovered that 10 participants showed unresolved responses during the baseline (the first question in the AAI, see also Table S1 in the Supplementary Materials). As this might have affected the neutrality of the baseline, we examined whether participants with unresolved discourse during baseline had different ANS activity, compared to participants without unresolved discourse. t tests demonstrated no significant difference in IBI (t(11.98) = 1.28, p = .23), RSA (t(10.03) = −0.68, p = .51), PEP (t(9.62) = −0.91, p = .39), and SCL (t(9.94) = −1.77, p = .11) during baseline. Further, t tests revealed that baselines were not significantly different for participants with and without a U/d classification; IBI (t(87.01) = −0.26, p = .79), RSA (t(91.72) = −0.51, p = .61), PEP (t(78.26) = −0.63, p = .53), and SCL (t(72.63) = −0.17, p = .77).
Trajectories of ANS reactivity throughout the entire interview
A visual inspection of the moderating effects of unresolved status in Hypothesis 1 suggested that there may be important time-trends in physiological response across the interview as a whole, which the prior analyses focused on comparisons of specific interview segments, had not addressed. Therefore, we estimated the trajectories of ANS response across the entire interview, moderated by unresolved status. First, a continuous “time” variable was created representing the questions and responses in the AAI (~43 observations per subject, 10,190 within-subject observations in total). Unresolved status was dichotomously coded (0 = not classified as U/d, 1 = classified as U/d). We used multilevel modeling. In the first step, an unconditional means model was estimated (Model 1). Secondly, the interaction between time and unresolved status was included as a linear effect (Model 2). In the next steps, we included polynomial transformations of time (quadratic, cubic, quartic) and their interactions with unresolved status as predictors. Likelihood ratio tests were used to compare the goodness of fit between two subsequent models.
Results
Due to space limitations, the full multilevel models are provided in the Supplementary Materials (Table S5). The best-fitting models are presented in Figure 2.

Figure 2. Estimated trajectories of interbeat interval (IBI) (A; cubic), respiratory sinus arrhythmia (RSA) (B; quartic), preejection period (PEP) (C; quadratic), and skin conductance level (SCL) (B; cubic) across the Adult Attachment Interview (AAI). Significant moderation effects of unresolved status were found for PEP and SCL. Error bounds represent standard errors.
IBI
The best fitting model for IBI was the cubic model, which had a better fit than the quadratic model (p < .001). The cubic effect of time on IBI was significant (p < .001), but the interaction between time and unresolved status was not (p = .74). For that reason, another cubic model was estimated including only the main effects of time. The linear, quadratic, and cubic effects of time on IBI were significant (ps < .001). IBI increased over the course of the interview, suggesting decreasing heart rate.
RSA
The best-fitting model for RSA was the quartic model, which had a better fit than the cubic model (p < .001). The quartic effect of time on RSA was significant (p < .001), but the interaction between time and unresolved status was not (p = .59). Therefore, another quartic model including only the main effects of time was estimated. The linear, quadratic, cubic, and quartic effects of time on RSA were significant (ps < .001).
PEP
The best-fitting model for PEP was the quadratic model, which had a better fit than the linear model (p < .001). The quadratic and linear effects of time on PEP were significant, as were the interaction effects between time and unresolved status (ps < .001). PEP decreased for participants classified as U/d, suggesting an increase in sympathetic reactivity; whereas PEP increased for those not classified as U/d. However, as seen in Figure 2, standard errors were large, suggesting that these results should be interpreted with caution.
SCL
The best-fitting model for SCL was the cubic model, which had a better fit than the quadratic model (p < .001). The cubic, quadratic, and linear effects of time on SCL were significant, as were the interaction effects between time and unresolved status (ps < .001). Participants classified as U/d showed diminished SCLs, compared to those not classified as U/d.
Discussion
This study tested ANS responses as indices of emotional arousal involved in U/d states of mind about loss/trauma. Relations were tested between ANS reactivity and (a) responding to questions about loss, abuse, and other trauma; (b) discussion of experiences of loss/trauma anywhere in the interview; (c) the interview being classified as U/d; and (d) instances of unresolved discourse about loss/trauma (i.e., lapses in the monitoring of reasoning or discourse). The first question in the AAI was used as the baseline.
First, we hypothesized that responses to questions about loss/trauma (Hypothesis 1) and discussion of loss/trauma anywhere in the interview (Hypothesis 2) would be associated with changes in ANS reactivity, and that these relations would be moderated by participants’ unresolved status (U/d). Responding to questions about loss and trauma was weakly associated with larger IBI, indicating lower heart rate (Hypothesis 1). Discussing actual loss anywhere in the interview was moderately associated with smaller IBIs (Hypothesis 2). However, against our expectations, these relations were not materially moderated by unresolved status. No main nor interaction effects were found for RSA, PEP, and SCL. Secondly, we hypothesized that unresolved discourse about loss/trauma would be associated with changes in ANS reactivity (Hypotheses 3 and 4), over and above the effect of discussion of loss/trauma. Interview questions with unresolved discourse about loss were associated with smaller IBIs, indicating heightened physiological arousal (Hypothesis 3 and 4). This finding provides preliminary support for the theory that unresolved loss/trauma reflects potentially dissociated attention to distressing experiences. No associations were found between unresolved discourse and RSA, PEP, and SCL.
The exploratory finding of increasing IBI across the interview as a whole may account for why responses to questions about loss and trauma were associated with larger IBIs (Hypothesis 1), because these questions usually appear in the second half of the AAI. Responding to questions about loss, abuse, and other trauma (which would often involve reporting the absence of such experiences) was not associated with indicators of parasympathetic (RSA) and sympathetic reactivity (PEP and SCL) (Hypothesis 1). The absence of moderation by unresolved status is consistent with previous findings by Beijersbergen et al. (Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008), and would appear to run counter to Main and Hesse's (Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990, Reference Main, Hesse, Ammaniti and Stern1992) theorizing. This implies either that (a) the physiological measures do not adequately index emotional dysregulation or the effects of unresolved states of mind regarding attachment; or (b) responding to questions about loss/trauma in the AAI does not or very weakly prompt emotional dysregulation or the effects of unresolved states of mind. One possibility is that the loss and trauma probes in the AAI may not be challenging enough to evoke states of fear or threat strong enough to trigger specific parasympathetic or sympathetic nervous system responses. One reason to consider this is that other researchers have alleged that the AAI interview protocol does not adequately probe for trauma (Bailey et al., Reference Bailey, Moran and Pederson2007; Crowell, Treboux, & Waters, Reference Crowell, Treboux and Waters2002). Bailey et al. (Reference Bailey, Moran and Pederson2007) noted that the way the abuse question is phrased “calls for the respondent to evaluate whether an experience was abusive” (p. 143), which may lead to underreported abuse. However, the interviewers in this study specifically pursued the AAI protocol's follow-up questions about trauma.
Discussion of actual loss anywhere in the interview was associated with smaller IBIs (Hypothesis 2). Increased heart rate has been associated with negative emotions such as sadness, anxiety, or fear (Kreibig, Reference Kreibig2010). This finding therefore indicates that bringing up memories of loss may trigger such emotions, which is in line with our expectations. Again, there was no moderation by unresolved status. To the degree that ANS response is an index of emotional arousal, such findings suggest that unresolved states of mind do not have an additional effect during recall of loss/trauma, over and above the impact of these experiences in themselves. To the degree that unresolved loss/trauma would be expected according to current theory to be reflected in emotional arousal, the current results call for further specification of this theory.
This study made a first attempt to connect ANS reactivity to parts of the interview with occurrences of unresolved discourse about loss or trauma (i.e., lapses in the monitoring of reasoning or discourse). Unresolved discourse about loss was associated with smaller IBIs (increased heart rate), over and above the effect of discussing any loss (Hypothesis 3 and 4). This finding suggests that some emotional arousal may occur when interviewees show lapses in the monitoring of reasoning or discourse about loss. However, it is unclear whether these responses are triggered by frightening intrusions (fear) as theorized by Main and Hesse (Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990, Reference Main, Hesse, Ammaniti and Stern1992) or whether these merely indicate sadness or anxiety about the loss (Kreibig, Reference Kreibig2010). This study failed to show an effect of unresolved discourse on specific parasympathetic and sympathetic responses (RSA, PEP, and SCL). However, this might be due to the way that occurrences of unresolved discourse were operationalized. Per interview question, we indicated whether participants’ responses to the interview questions included lapses in the monitoring of reasoning or discourse. These momentary lapses can appear anywhere during an interview response, which can sometimes be quite long. Future research might timestamp the exact moment identified as an occurrence of unresolved discourse to detect changes in parasympathetic and sympathetic reactivity, for example, by measuring nonspecific skin conductance responses.
In an exploratory analysis, we investigated participants’ trajectories of ANS reactivity throughout the entire interview. IBI and RSA increased during the interview, but these trajectories did not differ according to participants’ classification of U/d. These findings can be explained using Porges’ polyvagal theory (Reference Porges2007). Activity of the parasympathetic nervous system supports individuals’ abilities to engage in social behavior, which is needed to cope with the task of participating in the AAI. The exploratory findings for PEP indicated different trajectories of PEP according to participants’ classification of U/d. Participants classified as U/d showed decreasing PEP across the interview, indicating increasing sympathetic reactivity. This might suggest that these participants experienced an increase in stress over the course of the interview. For participants not classified as U/d, PEP increased across the interview. These participants might have felt nervous at the start of the interview, not knowing what to expect, and became increasingly comfortable over the course the interview. However, the findings on PEP should be interpreted with caution, because the standard errors were large.
Further, exploratory findings showed that participants classified as U/d had blunted SCLs over the course of the interview. A similar finding has been reported by Reijman et al. (Reference Reijman, Alink, Compier-De Block, Werner, Maras, Rijnberk and Bakermans-Kranenburg2017), who showed that women classified as U/d had decreased SCLs when watching a video in which two animated ellipses, “parent” and “child,” appeared to be separated from one another (Johnson, Dweck, & Chen, Reference Johnson, Dweck and Chen2007). The authors cautiously suggested that the decreased SCLs of women classified as U/d might reflect passive emotional coping (sadness without crying; Kreibig, Reference Kreibig2010), and also pointed to the potentially dissociative character of unresolved states of mind, as theorized by Main and Hesse (Reference Main, Hesse, Ammaniti and Stern1992). Blunted SCLs have been found among persons with PTSD and dissociation and have been linked to early exposure to trauma and multiple types of trauma (D'Andrea, Pole, DePierro, Freed, & Wallace, Reference D'Andrea, Pole, DePierro, Freed and Wallace2013). In line with Main and Hesse's (Reference Main, Hesse, Ammaniti and Stern1992) thinking, responding to general questions about attachment relationships in the AAI may trigger attachment-related memories of frightening loss or abuse experiences, which may activate a dissociative state. However, this association has not been empirically tested, and the current study did not include measures of dissociation. There is some empirical evidence of the relation between unresolved states and dissociative symptomatology (Abrams, Rifkin, & Hesse, Reference Abrams, Rifkin and Hesse2006; Riggs et al., Reference Riggs, Paulson, Tunnell, Sahl, Atkinson and Ross2007; Schuengel, Bakermans-Kranenburg, & van IJzendoorn, Reference Schuengel, Bakermans-Kranenburg and van IJzendoorn1999; Thomson & Jaque, Reference Thomson and Jaque2014), but findings are not consistent (Madigan et al., Reference Madigan, Vaillancourt, McKibbon and Benoit2012; Stovall-McClough & Cloitre, Reference Stovall-McClough and Cloitre2006). Further research is required to investigate the potential role of dissociation involved in unresolved states of mind. However, the principle of allostatic load (McEwen, Reference Willemsen, de Geus, Klaver, Van Doornen and Carroll2010) may provide another explanation for the findings. Early experiences and environmental factors can influence the way in which individuals respond to stressful situations, in terms of behavior as well as physiology. After prolonged or intense exposure to stress, allostatic systems – such as the ANS – may be unable to shut down or become exhausted, leading to wear and tear on the brain and body. This may result in either exaggerated or blunted physiological reactivity to stress (Lovallo, Reference Lovallo2011). It could be that discussing loss/trauma in the AAI is a stressful task and having an unresolved state of mind may create an additional challenge, leading to exhausted physical capacities to respond. In addition, there is evidence that cumulative risk factors (e.g., depressive symptoms and childhood poverty) could influence physiological stress reactivity and allostatic load (Evans & Kim, Reference Evans and Kim2012; Sturge-Apple, Skibo, Rogosch, Ignjatovic, & Heinzelman, Reference Sturge-Apple, Skibo, Rogosch, Ignjatovic and Heinzelman2013). Future research should focus on exploring these mechanisms.
The hypothesis-testing results showed no differences in parasympathetic (RSA) and sympathetic reactivity (SCL, PEP) in relation to participants’ unresolved state of mind (U/d) and unresolved discourse. This is in contrast with previous studies outside of the field of attachment, in which participants with PTSD and/or dissociation showed aberrant sympathetic and parasympathetic nervous system responses when recalling traumatic memories (e.g., Chou et al., Reference Chou, La Marca, Steptoe and Brewin2018; Sledjeski & Delahanty, Reference Sledjeski and Delahanty2012). This might be explained by differences in the study design. In trauma recall experiments, participants are often asked to close their eyes, bring to mind their most distressing traumatic experience, and describe the event vividly and in detail. In the AAI, interviewees are probed to discuss experiences of loss, and are briefly asked about potential abuse, but are not required to provide a rich description of events and may even choose to refrain from answering the questions. As mentioned previously, the loss/trauma questions in the AAI may therefore not have evoked specific parasympathetic or sympathetic responses or too weakly relative to the statistical power of the study. Van IJzendoorn and Bakermans-Kranenburg (Reference Willemsen, de Geus, Klaver, Van Doornen and Carroll2014) wondered whether the unresolved classification on the AAI “shows sufficient incremental validity beyond established measures for posttraumatic stress symptomatology” (p. 165). This important question remains unanswered. In our study, expected correlates for PTSD (dysregulated parasympathetic and sympathetic nervous system reactivity) were not found in relation to unresolved states of mind in the AAI, offering some evidence that these are different constructs. One the other hand, it may still be possible that unresolved states and PTSD have similar characteristics, such as intrusions and behavioral avoidance (Harari et al., Reference Harari, Bakermans-Kranenburg, de Kloet, Geuze, Vermetten, Westenberg and Van IJzendoorn2009; Nye et al., Reference Nye, Katzman, Bell, Kilpatrick, Brainard and Haaland2008; Stovall-McClough & Cloitre, Reference Stovall-McClough and Cloitre2006; see also Fearon & Mansell, Reference Fearon and Mansell2001). Further research is required to establish the common and distinct phenomena of unresolved states and PTSD.
Limitations
This study used a comprehensive approach and a sample of considerable size to investigate the relation between unresolved loss and trauma and ANS reactivity. Although we employed robust statistical methods and preregistered the analysis plan, we encountered some statistical constraints that did not allow us to model random slopes for the interview questions. This might explain why we were unable to demonstrate an interaction effect of responses to questions about loss/trauma and unresolved states of mind on indicators of parasympathetic and sympathetic reactivity. The small effect sizes found for Hypothesis 1 and 3 should also be interpreted in the context of leaving out random slopes – including these would likely have explained more variance in ANS reactivity. Furthermore, the study baseline (asking for an orientation to the speaker's early family situation) was not ideal. This question might have already triggered some emotional response for participants with a history of adversity, and participants might have felt nervous during the first interview questions. Future studies should use a more neutral talking baseline.
Implications
Overall, our findings suggest the need for further specification and clarification of theory. In line with Beijersbergen et al. (Reference Beijersbergen, Bakermans-Kranenburg, Van IJzendoorn and Juffer2008) findings, this study found no effect of either unresolved states of mind and unresolved discourse on parasympathetic and sympathetic reactivity during recall of loss or trauma in the AAI. This might partially be explained by methodological limitations, but otherwise has significant implications for theory. Main and Hesse's explanations of unresolved loss and trauma (e.g., Main & Hesse, Reference Main, Hesse, Ammaniti and Stern1992) remain speculative, and at times there is a lack of specificity in the theory. This hinders us in knowing how to interpret the results of our study. If not attributed to methodological limitations, the results could represent a partial falsification of the theory. Or they could signal that the processes Main and colleagues are discussing are not relevant to specific parasympathetic and sympathetic nervous system responses.
Taken together, this study raised several questions regarding the current state of theory of unresolved states of mind. For example, Main and Hesse (Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990) have explained unresolved states of mind as resulting from fear. However, our findings indicate that, during the AAI, persons with an unresolved state of mind may not experience fear as conceptualized by polyvagal theory (threat or danger; Porges, Reference Porges2007). On the other hand, these persons might experience a kind of fear not being picked up by the physiological measures in our study. To further investigate the role of fear – both in unresolved states of mind and the caregiver–child attachment relationship – a next step could be to link caregivers’ ANS responses to frightening/frightened parenting behaviors during interactions with their child (e.g., Lyons-Ruth, Bronfman, & Parsons, Reference Lyons-Ruth, Bronfman and Parsons1999; Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990). Another question raised by this study more broadly regards the psychological characteristics of unresolved states of mind. Some of the lapses in the monitoring of reasoning or discourse, as described by Main et al. (Reference Main, DeMoss and Hesse1991/1994; Reference Main, Goldwyn and Hesse2003), may not represent any fear or fright. Rather, these lapses might reflect the speaker's efforts to make sense of painful experiences during the interview, for example by manipulating their mind and diverting their attention away from difficult memories. Furthermore, there has been a lack of attention in the literature regarding the nature and psychological consequences of loss versus trauma in relation to U/d. To investigate assumptions about the “architecture” of unresolved states of mind, future studies would need sufficient statistical power and/or detailed qualitative data. Another area of ambiguity is that over the years, Main and colleagues have given different interpretations of the term “dissociation” in relation to unresolved states of mind, sometimes referring to dissociated or segregated memory systems and in other instances referring to altered states of consciousness (Main & Hesse, Reference Main, Hesse, Ammaniti and Stern1992; Main & Morgan, Reference Main, Morgan, Michelson and Ray1996). Yet there is currently a lack of direct evidence to support these interesting ideas. In addition, given the current state of knowledge it might even be possible that, for some persons, unresolved states of mind reflect other aspects of psychological functioning or childhood care (Lyons-Ruth, Yellin, Melnick, & Atwood, Reference Lyons-Ruth, Yellin, Melnick and Atwood2003).
In conclusion, this study was the first to link ANS responses directly to manifestations of unresolved loss and trauma in the AAI. Current findings indicate that persons with an unresolved state of mind may experience some physiological dysregulation throughout the entire interview, but questions remain about the psychological processes involved. Taken together, we argue that the theory of unresolved states of mind is still evolving, and more direct empirical evidence is needed to further articulate the psychological characteristics of unresolved states of mind.
Supplementary Material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579420001492
Acknowledgments
The authors would like to thank the mothers for participation in the Generations2 study. They also thank the researchers and research assistants who contributed to data collection.
Funding Statement
This research was supported by a grant from the Wellcome Trust to Lianne Bakkum [208155/Z/17/Z] and a grant from the Wellcome Trust to Robbie Duschinsky [WT103343MA].
Conflicts of Interest
None.












 Open access
Open access