


Electroconvulsive therapy (ECT) is the most effective acute treatment for severe depression, 1 with reported remission rates above 50%. Reference Dierckx, Heijnen, van den Broek and Birkenhäger2,Reference Kellner, Knapp, Husain, Rasmussen, Sampson and Cullum3 Although some reports demonstrate even higher remission rates (such as 75% in patients with psychotic depression Reference Petrides, Fink, Husain, Knapp, Rush and Mueller4 ), these could be below 50% for treatment-resistant depression or in community settings. Reference Heijnen, Birkenhäger, Wierdsma and van den Broek5,Reference Prudic, Olfson, Marcus, Fuller and Sackeim6 ECT is often portrayed in mainstream media as a barbaric treatment Reference Byrne7 and its cognitive side-effects as profound and debilitating, leading to public, patient and carer concerns. ECT does cause retrograde amnesia and acute disorientation immediately following a treatment, Reference Semkovska and McLoughlin8 however, research has suggested that this is only a short-lived side-effect. A meta-analysis by Semkovska & McLoughlin Reference Semkovska and McLoughlin9 analysed the cognitive tests of 2981 patients from 84 studies, performed before and after single courses of ECT, and found that a decline in cognitive performance was limited to the first 3 days following a treatment. Patients showed no cognitive deterioration when tested 2 or more weeks after their last ECT session. This does not apply to retrograde amnesia, which was not part of this analysis, and it cannot be extended to cognitive functions that were not tested. Much less is known about the side-effects of long-term ECT, including maintenance ECT. A major concern of patients and some health professionals is that it could lead to progressive cognitive deficits, especially if given for prolonged periods of time. Small studies and case reports have addressed this question and have found no evidence to support this concern (see Discussion). Over the past 10 years we performed prospective cognitive tests on 199 patients, of whom 96 had >12 ECTsessions during their lifetime (the usual maximum duration of a single ECT course). We wanted to find out whether there was evidence that their cognitive performance deteriorated with the increasing number of ECT sessions.
Method
We introduced cognitive testing for ECT patients at our department in 2004, first as part of a study comparing ECT and magnetic seizure therapy. Reference Kirov, Ebmeier, Scott, Atkins, Khalid and Carrick10 Influenced by the general perceptions at that time, we expected that ECT would cause a deterioration in cognitive tests. We found the tests very useful when making decisions about repeated ECT courses or maintenance ECT and when addressing patients' concerns. Therefore, we introduced these tests as part of the standard assessments of patients. More recently routine cognitive testing was recommended by the ECT Accreditation Service (ECTAS) of the Royal College of Psychiatrists. The list of nine tests that we use is presented in the Appendix. Reference Semkovska and McLoughlin9,Reference Lezak, Howieson and Loring11,Reference Loring, Meador, Knight and Kaplan12 Tests were administered by the authors of this paper, staff at the ECT department, students or psychiatrists at Cardiff University, as part of their projects over the years. All raters were trained and supervised in administering the tests by the first author. Therefore this is a non-masked study, with all the potential biases arising from such studies. However, the tests have been administered by many people, who might have had different expectations and could not know how the results could be analysed, therefore we cannot identify any systematic bias that has operated on the scoring. All patients who were referred for ECT were offered cognitive testing. Not everybody wanted to be tested and the more impaired patients were not able to perform some or all of the tests. Tests were performed before the start of a course, within 1 week after its end and at 3-month follow-up. Over the 10 years, many patients came for repeated courses and were offered repeated testing. Some patients required maintenance ECT (for example 11 patients had >50 ECT sessions) and we were initially concerned that they would experience a progressive cognitive deterioration. We wanted to monitor this and introduced yearly testing of patients having maintenance ECT.
Patients had between 0 and 186 previous ECT sessions at the time of their tests. A total of 199 patients were assessed on between one and seven occasions. The number of assessments on any single test varied between 332 and 493, as some tests were introduced later and not everybody completed all tests at each assessment point as a result of refusal, time constraints or technical problems. We excluded patients with schizophrenia, because of their known cognitive deficits. Reference Heinrichs and Zakzanis13 Patients who were not fluent in English were not included in this analysis.
The mean age of patients at the time of their last assessment was 56.3 years (s.d. = 15.8, range 21–88) and 71.9% of them were female (n = 143). The majority had unipolar depression (n = 166, 83.4%), the remaining 33 had bipolar affective disorder, but everybody included in this analysis was treated for depressive episodes. The average number of ECT sessions that patients had prior to their tests was 15.3 (s.d. = 23.2, range 0–186). Figure 1 shows the distribution of the numbers of ECT sessions that patients had prior to their tests.
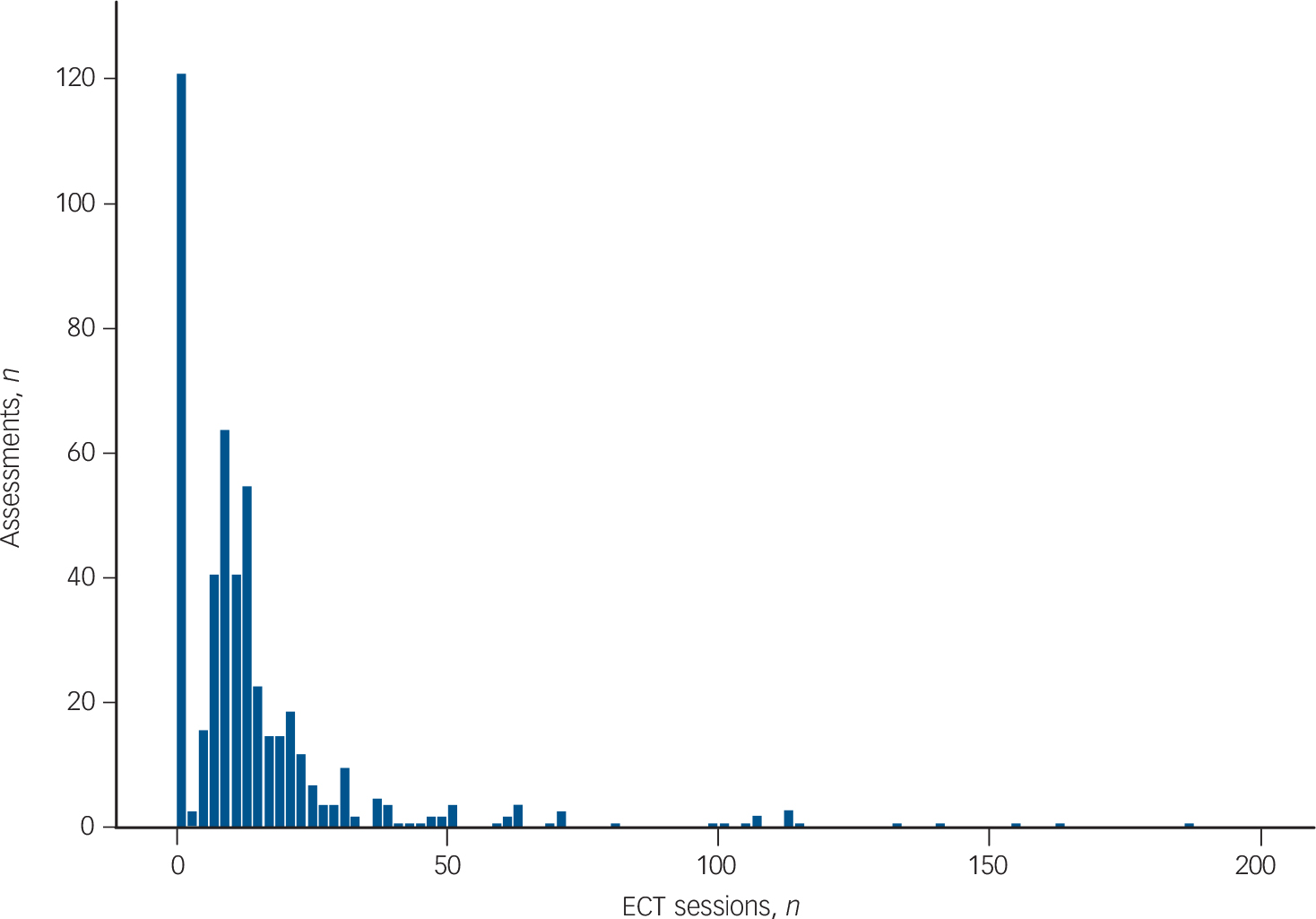
Fig. 1 Number of electroconvulsive therapy (ECT) sessions received by patients prior to the assessments.
The highest number of tests done were prior to their first-ever electroconvulsive therapy session (n = 122).
Statistical analysis
Our aim was to evaluate whether the cumulative number of ECT sessions received during the lifetime of patients prior to testing was inversely correlated with their performance on the cognitive tests. We obtained histories of previous courses and recorded the total number of ECT sessions they had received prior to each test. As other factors can influence cognitive performance, we included the following four covariates: age, number of days since last ECT session, severity of depression and the number of times the patient had undertaken the test previously. Age is an obvious confounder, as cognitive performance declines with age. It has been shown that cognitive performance is worse in the first 3 days after an ECT session and tends to improve with time. Reference Semkovska and McLoughlin9 We recorded the number of days since the last ECT session (for those who had no previous ECT sessions, we entered an arbitrary, but very large number of 10 000 days (about 30 years), in order to keep these assessments in the analysis). As these data were extremely skewed, we log-transformed the number of days since the last ECT. As our cognitive testing always includes an objective measure of the severity of depression (the 24-item Hamilton Rating Scale for Depression, HRSD-24), Reference Blacker, Sadock, Sadock and Ruiz14 we included these scores as a covariate, expecting that patients who were more severely depressed might perform worse. The number of times a test had been undertaken previously by a patient was also included as a covariate in order to control for the possibility that patients improve their performance with practice. As some patients had undertaken tests on more occasions than others (between one and seven occasions), we also wanted to control for the potentially disproportionate effect of inter-individual differences. We therefore used a linear mixed-effect regression model with random effects attributed to individual patients and fixed effects to the four covariates listed above. We used the R statistical package with the library lme4 (function lmer). As a secondary analysis we compared the first and last cognitive tests of those patients who had 13 or more ECT sessions between these tests (more than a standard ECT course of 12 sessions). We used a paired samples t-test to compare these pre- and post-ECT results.
Results
Results are presented in Table 1. We show the effect size and statistical significance of the effect from the number of ECT sessions and the four covariates on cognitive performance. Effect size denotes the change on the cognitive score with each unit of the covariate (such as each year of age or each ECT session). Deterioration is always indicated with a negative sign of the effect size, whether it refers to reduction in score (for example verbal fluency), or increase in the time needed to perform a test (Trail Making and Reaction Time), or increase in the Cognitive Failures Questionnaire (CFQ) score. Reference Semkovska and McLoughlin9,Reference Lezak, Howieson and Loring11 The number of ECT sessions prior to testing had no significant effect on any of the tests. The other covariates had statistically significant effects on the results, in the predicted directions.
Table 1 Statistical significance and effect size of the number of electroconvulsive therapy (ECT) sessions and the four covariates on the cognitive tests a
| Digit Span |
Recognition (memory) |
Verbal fluency |
MMSE | Complex figure |
CFQ | Reaction time |
Trail
making A |
Trail
making B |
|
|---|---|---|---|---|---|---|---|---|---|
| Assessment, n | 460 | 455 | 479 | 493 | 384 | 360 | 418 | 340 | 332 |
| ECT sessions, n | |||||||||
| Effect size | 0.005 | − 0.008 | −0.004 | 0.005 | − 0.004 | −0.02 | −1.0 | 0.02 | − 0.5 |
| P | ns | ns | ns | ns | ns | ns | ns | ns | ns |
| HRSD | |||||||||
| Effect size | − 0.01 | − 0.05 | − 0.02 | − 0.03 | − 0.03 | − 0.5 | − 2.9 | −0.4 | −1.8 |
| P | 0.03 | 0.0006 | ns | 0.002 | ns | 9 × 10 −10 | 0.0007 | 0.002 | 0.003 |
| Age | |||||||||
| Effect size | − 0.01 | − 0.08 | − 0.05 | − 0.07 | − 0.3 | 0.3 | − 4.9 | − 1.2 | − 4.7 |
| P | 0.005 | 6 × 10 −10 | 0.005 | 10 −12 | 8 × 10 −14 | 8 × 10−6 | 4 × 10−11 | 4 × 10 −17 | 3 × 10 −15 |
| Days since ECT | |||||||||
| Effect size | − 0.002 | 0.5 | 0.3 | 0.1 | 0.4 | − 0.6 | 6.8 | 3.1 | 6.7 |
| P | ns | 0.0003 | ns | ns | ns | ns | ns | 0.006 | ns |
| Practice (repetition of test) |
|||||||||
| Effect size | 0.05 | 0.1 | 0.1 | − 0.02 | 0.7 | 0.2 | 20.2 | 4.6 | 13.1 |
| P | ns | ns | ns | ns | ns | ns | 0.04 | 0.006 | ns |
MMSE, Mini-Mental State Examination, CFQ, Cognitive Failures Questionnaire; HRSD, Hamilton Rating Scale for Depression.
a. Results with P>0.05 are shown as non-significant (ns). No correction for multiple testing is applied. Effect size indicates the degree of change on the cognitive test score by each unit of the variable. For example for the variable age, each year reduces the performance on the MMSE by 0.07 points, i.e. a patient who is 50 years older than another one, scores on average 3.5 points lower. All effect sizes have been converted so that a minus (−) sign always denotes a deterioration.
The variable with the strongest effect on the tests was age, with performance significantly declining with increasing age on all tests except the CFQ. The CFQ is a self-assessment of cognitive/memory problems and the results suggested that older patients complained less of cognitive problems. The next factor influencing the results was the severity of depression at the time of testing, which adversely (and significantly) affected seven of the nine tests. Patients showed significant improvements in performance with increasing time-gaps since the last ECT session on two of the tests (memory and Trail Making A). Practice (repetition of the tests) significantly improved the performance on two tests (Reaction Time and Trail Making A).
As a secondary analysis we compared the pre- and post-ECT results on 55 patients who had 13 or more ECT sessions between their first and last cognitive assessment (i.e. more than the standard duration of a single ECT course of up to 12 sessions). The median number of ECT sessions these patients had between the tests was 20 (range 13–156). We used paired samples t-tests and present the results in Table 2. All results improved, two of them improved significantly. The improvements are most likely because of improvements in depression at the end of a course or at follow-up (HRSD-24 scores were on average 29.1 at the first and 14.7 at the time of the last tests).
Table 2 Comparison between the first and last cognitive tests in patients who had 13 or more electroconvulsive therapy sessions between the tests a
| Test | Patients, n | Start (s.d.) | End (s.d.) | Change (95% CI) | P |
|---|---|---|---|---|---|
| Digit span backwards | 50 | 4.4 (1.3) | 4.7 (1.3) | 0.3 (− 0.02 to 0.7) | 0.06 |
| Recognition of words, shapes and faces (memory, maximum 28) | 48 | 23.4 (3.7) | 23.7 (3.2) | 0.3 (− 0.5 to 1.1) | 0.5 |
| Verbal fluency | 52 | 10.7 (4.3) | 11.0 (4.6) | 0.3 (− 1.1 to 1.6) | 0.7 |
| Mini-Mental State Examination (maximum 30) | 55 | 27.7 (3.0) | 27.7 (2.9) | 0.0 (− 0.6 to 0.7) | 1 |
| Complex Figure immediate recall (maximum 36) | 40 | 20.7 (11.3) | 21.7 (8.2) | 1.0 (− 1.9 to 4.0) | 0.5 |
| Cognitive Failures Questionnaire (CFQ) | 31 | 50.1 (19.0) | 42.1 (17.0) | − 8.0 (− 13.4 to −2.5) | 0.006 |
| Reaction time, s (maximum 1.1 s) | 43 | 0.66 (0.23) | 0.54 (0.16) | − 0.12 (− 0.18 to −0.05) | 0.001 |
| Trail making A, s (maximum 300s) | 32 | 56.8 (47.9) | 51.0 (50.7) | − 5.8 (− 13.0 to 1.4) | 0.1 |
| Trail making B, s (maximum 600s) | 32 | 119.4 (117.4) | 111.2 (121.0) | − 8.2 (− 30.8 to 14.3) | 0.5 |
a. Paired samples t-tests. All results indicate improvements (the minus signs for the last four tests also suggest improvements, as the tests were completed faster, or in the case of the CFQ, the patients rated themselves less impaired).
Discussion
Findings from other studies
Memory problems and fears of cognitive decline are probably the biggest deterrents for patients' willingness to undergo ECT. 15 The internet abounds with reports of people complaining that ECT has destroyed their memory and mainstream media tends to portray it as a barbaric treatment. Reference Byrne7 Complaints of memory loss regarding events occurring around, or a few months prior to ECT courses (retrograde amnesia) are very frequent and were also reported by many of our patients (the tests in the Appendix do not measure retrograde amnesia). However, a meta-analysis Reference Semkovska and McLoughlin9 showed that the reduced performance on various cognitive tests is limited to only the first few days after a ECT session, and tends to improve when such tests are performed more than 2 weeks after the last session. However, the improvement of depression after ECT could have improved performance and masked a small underlying cognitive deterioration (we were able to control for depression severity in the current study). There is less evidence as to whether repeated courses of ECT, or maintenance ECT given over several years, will result in cumulative cognitive deficits. It is conceivable that some small damage is caused by each ECT, which could be overlooked if testing is limited to 3–12 sessions, the typical duration of the majority of ECT courses included in the meta-analysis. Reference Semkovska and McLoughlin9 It is impractical to conduct such studies as part of masked, control trials, as they require years of observations and testing patients who might lose capacity to provide informed consent at some periods of their treatments. Most of the evidence on long ECT courses is from case reports and small case series and they show lack of cumulative deterioration. Case reports by Wijkstra & Nolen Reference Wijkstra and Nolen16 on a patient who received 244 ECT sessions over 7 years, Barnes et al Reference Barnes, Hussein and Anderson17 on a patient who had 420 ECT sessions and Zisselman et al Reference Zisselman, Rosenquist and Curlik18 on a patient who had 12 months of weekly maintenance ECT found no evidence of progressive deterioration on the Mini-Mental Sate Examination (MMSE). Russell et al Reference Russell, Rasmussen, O'Connor, Copeman, Ryan and Rummans19 conducted a retrospective chart review of MMSE scores of 43 patients who had received at least 1 year of maintenance ECT and found a small, not significant improvement in the mean scores. Abraham et al Reference Abraham, Milev, Delva and Zaheer20 tested memory changes in 18 patients who had received at least 3 months of maintenance ECT. ‘Mild memory impairment’ affected just three patients, whereas severe memory changes were only found in one patient. Vothknecht et al Reference Vothknecht, Kho, van Schaick, Zwinderman, Middelkoop and Blansjaar21 reported on 11 patients who underwent maintenance ECT and who received sessions on average 2.2 weeks apart and who were tested with a battery of neuropsychological tests at baseline and after 6 months. The results actually improved after 6 months of maintenance ECT. It has been suggested that the risk of cognitive impairment during longer courses of maintenance ECT may even decrease, because of the longer time intervals between sessions. Reference Trevino, McClintock and Husain22
Main findings
To our knowledge, the current study is the first of its kind, reporting on 10 years of cognitive data collection on consecutive ECT patients, where each patient's lifetime number of ECT sessions has been recorded and included in the analysis. Our results show a lack of cumulative cognitive deterioration with an increasing number of ECT sessions. In contrast, other covariates, such as age and severity of depression, produced clear trends in the expected directions, suggesting that we have not missed trends where they exist, because of noise in the data or bias that can occur in an open study. An example of this is presented in Fig. 2 that shows a clear deterioration of the scores on the Complex Figure test Reference Loring, Meador, Knight and Kaplan12 with increasing age of the patients, but there is no such trend with increasing number of ECT sessions. The results are supported by our observations on patients who accumulated the highest numbers of ECT sessions over the 10-year period of monitoring and showed no deterioration in their performance (Table 2).
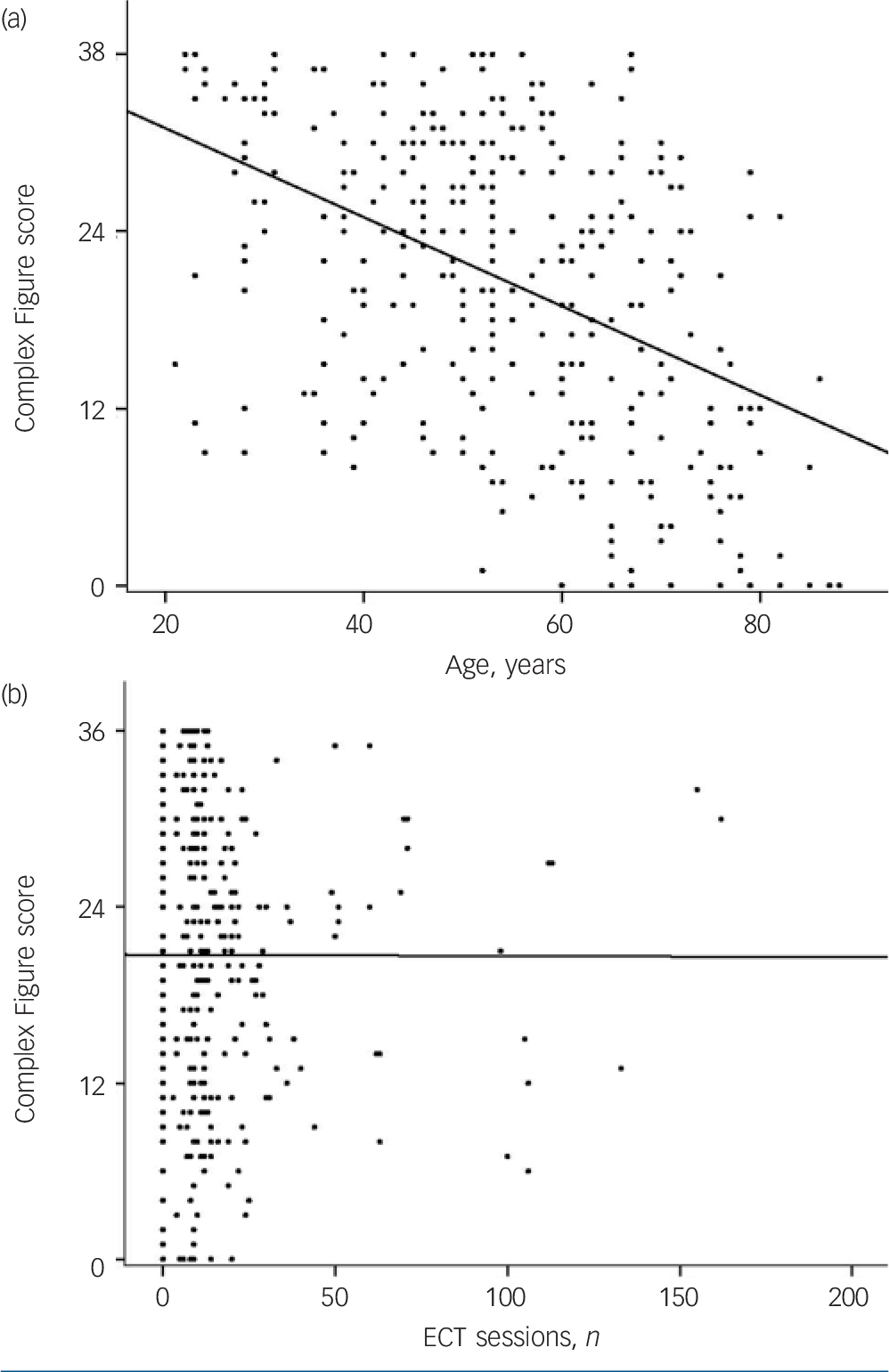
Fig. 2 Scores on the Complex Figure immediate recall test.
The score on the Complex Figure immediate recall test reduces with the increasing age of patients (a) but not with the increasing number of previous electroconvulsive therapy (ECT) sessions (b). The maximum score for a perfectly memorised and reproduced figure is 36 points. Reference Loring, Meador, Knight and Kaplan12
Limitations
As an open, uncontrolled study, our work has limitations that we acknowledge. For example, some patients might have had early stages of dementia or underlying cerebrovascular disease, which could lead to a reduced cognitive reserve. To reduce this potential problem, we re-analysed the results while excluding people over the age of 65. The lack of effect from the number of ECT sessions remained for all cognitive tests (data not presented). The effect size caused by age was reduced, as expected, but remained in the same direction. It is also possible that the patients who persist with more ECT sessions may be those who had fewer cognitive side-effects, so that those who have more ECT sessions will tend to have fewer adverse effects. This potential bias is difficult to address in a naturalistic study, and we can only report that many of our patients on maintenance ECT or repeated courses complained of subjective memory problems and stopped their treatments on many occasions, i.e. they did not appear to be more tolerant of side-effects. We were unable to measure any cumulative retrograde amnesia because of the longitudinal nature of the testing (patients are more likely to forget the original events, if tested 1 or more years later, when they come for new ECT courses).
Implications
We find that discussing the cognitive results with patients is highly reassuring for them, as they can see for themselves that their cognitive performance remains stable. This has helped their decisions when accepting further ECT courses or maintenance treatment, something that might have been unacceptable to them or to their treatment teams only a few years ago. Our results suggest that patients can have repeated courses or maintenance ECT without this resulting in long-term cumulative cognitive deterioration. We hope that this study will help to counter the negative public view of ECT, which may be having an effect on prescribers and thus aid in the appropriate prescribing of this effective treatment.
Appendix
List of cognitive tests and the functions they measure a
| Test | Description of the test | Cognitive domain tested |
|---|---|---|
| Digit Span backwards | Number of digits repeated backwards (four versions) | Concentration, attention and working memory |
| Recognition of words, shapes and faces | Recognising 12 words, 8 shapes and 8
faces presented 20–30 min earlier |
Verbal and visual episodic (anterograde) memory |
| Verbal fluency | Naming words beginning with a given
letter in 1 min (four versions: F, S, T, A) |
Executive functioning and linguistic ability |
| Mini Mental State Examination (MMSE) | Four versions adapted from the standard MMSE | Global cognitive functioning and orientation |
| Complex Figure immediate recall | Complex figure to be drawn from memory (four versions) | Visual episodic memory and executive functioning |
| Cognitive Failures Questionnaire (CFQ) | Self-rating on a series of 25
statements about everyday cognitive/memory problems |
Subjective assessment of memory and
cognitive performance |
| Reaction time | Speed of reactions assessed with a
computer test (maximum time limited to 1.1 s) |
Processing speed |
| Trail making A | The time needed to connect 24
scattered numbers in ascending order (maximum time limited to 5 min) |
Processing speed, visual scanning, mental flexibility |
| Trail making B | The time needed to connect 12
scattered numbers and 12 letters in order (maximum time limited to 10 min) |
Executive functioning, visual
scanning, mental flexibility |
a. After Lezak et al Reference Lezak, Howieson and Loring11 and Semkovska & McLoughlin. Reference Semkovska and McLoughlin9 For some tests we prepared four different versions in order to reduce the possible practise effect. For Complex Figures we used the four versions of the Medical College of Georgia (MCG) Complex Figures. Reference Loring, Meador, Knight and Kaplan12






eLetters
No eLetters have been published for this article.