



Introduction
Mathematical modeling has been widely used across all aspects of public health response efforts during the coronavirus disease 2019 (COVID-19) pandemic to facilitate policy decisions; understand epidemiological burden, trends, and transmission dynamics; and, to a lesser extent, evaluate infection prevention and control (IPC) measures. Reference Biggerstaff, Slayton, Johansson and Butler1–Reference Borchering, Healy and Cadwell3 Although mathematical modeling was used to inform IPC implementation prior to the COVID-19 pandemic, the use of modeling during the pandemic underscored its value as a tool for improving IPC in health care. In September 2023, 40 experts from the fields of IPC, healthcare epidemiology, and mathematical modeling convened in Geneva, Switzerland, for the 2023 IPC Think Tank, funded by the US Centers for Disease Control and Prevention. The Think Tank meeting sought to evaluate the use of mathematical modeling as a tool for healthcare epidemiology in light of the COVID-19 pandemic and highlight where mathematical modeling may augment current epidemiological approaches to IPC more broadly. In this article, we summarize the key messages and conclusions of the 2023 IPC Think Tank.
Complementary roles of conventional epidemiology and modeling
The goals of healthcare epidemiology and IPC programs in healthcare settings include protecting patients and care providers from infectious diseases, including HAI, and limiting the spread of antimicrobial resistance. These goals are achieved through efforts such as epidemiological studies to identify risk factors for infection, surveillance for infections in the healthcare setting, and implementation and evaluation of interventions to prevent transmission of pathogens. Conventional epidemiology uses observational data to assess predictive factors and outcomes; however, these methods, at times, fall short in addressing many important questions in the fields of healthcare epidemiology and IPC. This may be, in part, because HAI and antimicrobial resistance emerge from very complex systems that are difficult, if not impossible, to directly observe or quantify and for which observational time frames are necessarily longer than ideal when rapid interventions are needed. Mathematical modeling provides a simplified representation of a complex system formalized by mathematical equations. It is an extension of conventional epidemiological analyses by which mechanistic causal processes, often not directly observed, are explicitly included. Mathematical modeling is, therefore, particularly helpful in addressing the complexity of HAI and antimicrobial resistance. Some of the similarities and differences between conventional epidemiological and mathematical modeling approaches are summarized in Table 1. Importantly, these 2 approaches are complementary rather than competing and can be used to enhance healthcare epidemiology and IPC, as described in the following examples.
-
1) Transmission pathways in healthcare settings
Table 1. Similarities and differences between conventional epidemiological approaches and mathematical modeling approaches

Note. EQUATOR, Enhancing the QUAlity and Transparency Of health Research.
Understanding transmission pathways by reconstructing outbreaks (ie, who infected whom) in healthcare settings can help inform and refine infection control policies. Successful epidemiological approaches for identifying and halting nosocomial transmission rely heavily on early identification and isolation of cases and their contacts. However, conventional epidemiological approaches may not be able to provide a complete or correct picture of transmission pathways in an epidemic. This is because of the variability in the incubation period of infections due to different pathogens and variation in the extent to which transmission occurs from asymptomatic or presymptomatic persons with viral infections or from people colonized with antimicrobial-resistant bacteria. Reference Lindsey, Villabona-Arenas and Campbell4 Further, key events in the mechanistic chain often cannot be directly observed in epidemiological studies; mathematical modeling approaches offer insights into unobserved events.
During the COVID-19 pandemic, the integration of viral genomic, epidemiological, and location data using a modeling framework was used to identify more accurate estimates of within-hospital transmission and transmission mechanisms and to identify individuals or groups who contribute disproportionately to transmission. In this approach, transmission is supported if the time of symptom onset and the serial interval distribution (ie, time from illness onset in a primary case to illness onset in a secondary case) of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) are compatible, if location data indicate that the individuals were in the same hospital location at the time of a suspected transmission event, and if there is a high degree of relatedness between viral genomes. Reference Lindsey, Villabona-Arenas and Campbell4 This approach has been used to understand SARS-CoV-2 transmission among patients and health workers in a large UK National Health Service Trust, Reference Lindsey, Villabona-Arenas and Campbell4 as well as between older patients and healthcare workers in acute geriatric settings. Reference Abbas, Cori and Cordey5
The integration of genomic and epidemiological data to enhance understanding of nosocomial transmission was not a novel development during the COVID-19 pandemic; this method has been used to enhance understanding of methicillin-resistant Staphylococcus aureus (MRSA) transmission in a high transmission hospital setting Reference Hall, Holden and Srisomang6 and of healthcare-associated Clostridioides difficile. Reference Eyre, Laager, Walker, Cooper and Wilson7 The increased availability and decreasing costs of high-throughput genomic sequencing and the development of specific software packages Reference Campbell, Didelot, Fitzjohn, Ferguson, Cori and Jombart8 facilitate the integration of genomic sequencing and epidemiological data for reconstructing nosocomial transmission dynamics. This approach can be applied to the transmission of other respiratory viruses, beyond SARS-CoV-2, and potentially to multidrug-resistant organisms (MDRO) in healthcare settings.
-
2) Forecasting transmission and healthcare impact
The ability to anticipate epidemic dynamics through mathematical modeling has proven critical during the COVID-19 pandemic. The use of these models has allowed for optimizing the public health response (eg, facility closures and reopening) and allocation of healthcare demand, supplies (eg, personal protective equipment, therapeutics, and vaccines), personnel, and resources. Reference Smith, Chervet and Pinettes2,Reference Paireau, Andronico and Hozé9–Reference Kahn, Holmdahl, Reddy, Jernigan, Mina and Slayton14 Forecasting models have been used to provide quantitative, evaluable, and probabilistic predictions about the trajectory of SARS-CoV-2 transmission and COVID-19 impact across the near-term future. Reference Cramer, Ray and Lopez15 Although there may be high variation inaccuracy in forecasting COVID-19 deaths between and within individual models, there is greater accuracy using multimodel ensemble forecasts for which individual forecasts from all eligible models are combined and for which the performance exceeds most, if not all, of the models that contributed to it. Reference Paireau, Andronico and Hozé9,Reference Cramer, Ray and Lopez15 Importantly, the accuracy of both standalone and multimodel ensemble forecasts is dependent on the quality of surveillance data. This highlights both the complementarity of conventional epidemiological and mathematical modeling approaches and the need for collaboration and active coordination between public health surveillance and mathematical modeling groups.
MDRO surveillance in Europe, for example, relies on the submission of antimicrobial susceptibility data from invasive clinical isolates. Some of the modeling approaches developed during the COVID-19 pandemic to forecast COVID-19 impact across the near-term future could be used to forecast the emergence and impact of MDRO within populations and healthcare facilities, although this is not without substantial challenges compared to forecasting acute viral infections. The major challenges to forecasting MDRO include, but are not limited to, the extent of asymptomatic carriage, susceptible and resistant strain competition and the effect of antimicrobial drug use, and longer time scales than acute viral infections. Reference Pei, Blumberg and Vega16 Despite these challenges, the addition of more data on colonization derived from community-based specimens and asymptomatic carriage in patients in healthcare settings could be used in a modeling framework to more accurately estimate MDRO burden (ie, deaths, hospitalizations, days of work lost, direct and indirect economic costs, and evolution of resistance).
-
3) Improving the validity of interpretation of surveillance data
Surveillance of the asymptomatic carriage of antimicrobial-resistant organisms provides data that are used to target IPC activities and to provide a deeper epidemiological understanding than is feasible with data from surveillance that includes only microbiology testing performed for clinical care. However, analyzing colonization data using conventional analytical methods has limitations, which can be resolved, at least in part, by model-based approaches. A simple example is the use of admission screening to estimate the admission prevalence of asymptomatic carriage. A more complex example is construing that a positive follow-up test in a patient with a negative admission test represents an acquisition event. In both instances, the likelihood that the observed test results are being correctly interpreted depends on the characteristics of the microbiological test (ie, false negativity and false positivity), as well as several other assumptions about the underlying dynamics. Modeling methods that explicitly represent transmission while also accounting for imperfect tests can reduce the bias associated with estimating admission prevalence and acquisition rates. Reference Khader, Thomas and Huskins17 Similarly, modeling approaches can provide a more accurate assessment of the probability that colonization with a resistant organism has resolved, given 2 or more consecutive negative tests. Reference Khader, Thomas and Huskins17 Yet another example where transmission dynamic models improve the interpretation of epidemiological data is in the analysis of the effect of colonization pressure on acquisition rates. Reference Khader, Thomas and Huskins17,Reference Khader, Thomas and Stevens18 All of these examples highlight the importance of using analytic methods that explicitly distinguish between observed and unobserved events.
-
4) Evaluating the impact of infection prevention and control interventions
Another area of healthcare epidemiology that mathematical modeling can support is in estimating or anticipating the impact of IPC interventions, particularly when several preventive measures are bundled together. More specifically, dynamic transmission models can be used to better understand clinical trial study design and statistical power, both to re-evaluate the true impact of a completed intervention (post hoc) and to improve the design of future clinical trials (ex ante). The use of these models can address some of the most challenging issues with IPC intervention trials, including insufficient follow-up times, outcome measurement biases, and disentangling the effects of multiple intervention components.
Two examples of post hoc analyses that illustrate how dynamic models can be used to more precisely estimate the impact of different IPC interventions studied in large clinical trials are the 2 published re-analyses of the Strategies to Reduce Transmission of Antimicrobial Resistant Bacteria in Intensive Care Units (STAR*ICU) trial Reference Khader, Thomas and Huskins17 and the Benefits of Universal Glove and Gown (BUGG) study. Reference Harris, Morgan, Pineles, Perencevich and Barnes19,Reference O’Hagan, Reddy and Yi20 In the former, a Bayesian transmission modeling framework was created using data collected from the STAR*ICU trial to estimate the observed transmission and clearance rates separately for MRSA and vancomycin-resistant enterococci (VRE) while accounting for the imperfect coverage of surveillance tests. Consistent with the original trial, this work suggested no reduction of transmission for either MRSA or VRE due to the intervention, though it also revealed subtle but important differences between the pathogens regarding transmission, importation, and clearance rates. In the latter, an agent-based model calibrated and validated using data from the BUGG study was used to quantify the relative benefits of the 3 different components of the intervention, ultimately concluding that the decrease in MRSA acquisition seen in the clinical trial was likely due primarily to the barrier effects of glove and gown use. These 2 post hoc analyses show how dynamic transmission models can be used to gain deeper insights into clinical trial results and potentially direct subsequent investigations, including further evaluations of components of IPC bundles.
Mathematical models can also be very useful for improving the design of intervention trials, particularly in evaluating whether trials employ valid designs to estimate the effect of the interventions being studied accurately. Because of the nature of most hospital- or facility-based IPC intervention trials, it is difficult, complex, and costly to account for several challenging issues related to disease transmission. For instance, short hospital stays may result in unobserved acquisitions or infections that manifest postdischarge, short intervention and follow-up times may result in missing intervention effects that can build for many years before plateauing, and studies done at single centers may underestimate an intervention’s effect by not accounting for effects that may occur at other network facilities as a consequence of patient transfer. Many types of mathematical transmission models can be employed to explore the impact of accounting for these design issues on the validity of a proposed study and the extent to which it can fully estimate the effect of the intervention and its individual components.
-
5) Guiding IPC and antimicrobial treatment and stewardship decision-making
During the COVID-19 pandemic, mathematical modeling studies explored various IPC decision-making questions, including the impact of community-based non-pharmaceutical interventions, Reference Sonabend, Whittles and Imai12,Reference Howerton, Contamin and Mullany21 implementation factors for vaccination programs, Reference Paltiel, Schwartz, Zheng and Walensky22 and evaluation of changes to screening, vaccination, and IPC policies in nursing homes across the pandemic waves. Reference See, Paul and Slayton13,Reference Kahn, Holmdahl, Reddy, Jernigan, Mina and Slayton14,Reference Holmdahl, Kahn, Slifka, Dooling and Slayton23–Reference Singh, Walker and Paul25 Scenario modeling has been used to create and analyze different hypothetical situations and assess how they affect nosocomial transmission dynamics of SARS-CoV-2, therefore guiding implementation and, crucially, de-implementation of various IPC measures in hospitals. Reference Singh, Walker and Paul25,Reference Smith, Duval and Grant26
Beyond COVID-19, models have been used to assess the trade-offs of different regional containment strategies for resistant infections, helping decision-makers evaluate the trade-offs of selection of facilities and frequency of conducting point prevalence surveys Reference Slayton, Toth and Lee27–Reference Bartsch, Wong and Mueller30 and the cost-effectiveness of such approaches. Reference Lin, Tseng and Gatalo31 Additionally, models have evaluated the trade-offs among prevention strategies and aided in the selection of priority facilities for recruitment into a large public health demonstration project, “Shared Healthcare Intervention to Eliminate Life-threatening Dissemination of MDROs.” Reference Cincotta, Walters and Ham32,Reference McKinnell, Singh and Miller33 As novel vaccines or agents designed to reduce MDRO colonization or infection make their way through the development pipeline, modeling can be used to evaluate the potential impact of these agents by accounting for not only the direct benefit to the treated individual but also the indirect population benefit resulting from prevention of transmission. Reference Toth, Keegan and Samore34,Reference Toth, Samore and Nelson35
Expanding the use of modeling in healthcare epidemiology
The examples described above demonstrate the added value of mathematical modeling as a tool for improving understanding of HAIs and IPC efforts and facilitating public health decision-making. Table 2 highlights current priority areas for expanding the use of modeling in healthcare epidemiology and IPC. Nonetheless, there is a need to exercise some caution in this endeavor. Importantly, mathematical modeling does not replace the need for observational studies and interventional trials. Although modeling can be used when empirical data are not available, modeling cannot substitute for the absolute absence of empirical data. As such, it is increasingly important that modelers are active in the design of high-quality epidemiological studies to ensure that data needed for models are collected. Further, the expectations of modeling, as well as how modeling output should and should not be used, need to be clear. Finally, efforts to harmonize the reporting standards for modeling studies are needed to increase transparency of inputs, assumptions, uncertainties, and results. For example, the MInD-Healthcare Framework provides a standardized approach for describing and reporting agent-based models of MDRO and HAIs. Reference Slayton, O’Hagan and Barnes36
Table 2. Priority areas for expanding the use of modeling in healthcare epidemiology and infection prevention and control
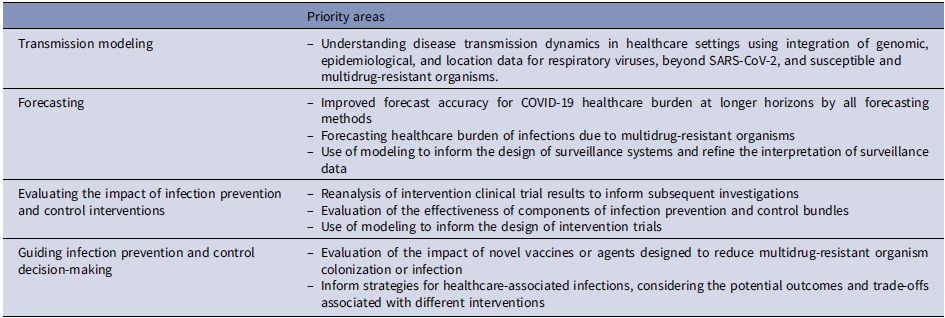
Note. SARS-CoV-2, severe acute respiratory coronavirus virus 2; COVID 19, coronavirus disease 2019.
It must also be underscored that traditional epidemiological studies offer invaluable insights that can enhance the accuracy and relevance of mathematical modeling in healthcare epidemiology. By providing detailed observations of the disease’s natural history, incidence rates, and risk factors, these studies offer critical data points for model calibration. For example, the detailed contact tracing efforts during the Ebola outbreak in West Africa provided data on transmission rates and incubation periods, which were crucial for developing predictive models to forecast the spread and guide intervention strategies. Reference Agua-Agum and Ariyarajah37–Reference Pandey, Atkins and Medlock41 Similarly, traditional epidemiological investigations into influenza outbreaks contribute to refining mathematical models that can be used to predict the timing, peak, and intensity of influenza seasons, thereby aiding in vaccine distribution and public health preparedness. Reference Thompson, Stockwin and van Gaalen38 These examples underline how empirical data from traditional epidemiological studies are instrumental in informing and validating mathematical models, making them more robust and tailored to real-world scenarios in healthcare epidemiology.
Conclusion
During the COVID-19 pandemic, there has been a rapid expansion in the use of mathematical modeling, underscoring the utility of modeling for public health and patient care. Opportunities remain to expand the use of mathematical modeling in healthcare epidemiology and IPC. Importantly, this should be seen as complementary to conventional healthcare epidemiological approaches and requires collaboration and active coordination between IPC, healthcare epidemiology, and mathematical modeling groups.
Acknowledgments
The authors would like to thank all participants for their contributions to the 2023 IPC Think Tank: Mohamed Abbas (Switzerland), Benedetta Allegranzi (Switzerland), Rafael Araos (Chile), Chedly Azzouz (Tunisia), Michael Bell (United States), Philip Bemah (Liberia), Gabriel Birgand (France), Martin Bootsma (Netherlands), Tcheun-How Borzykowski (Switzerland), Icaro Boszczowski (Brazil), Niccolò Buetti (Switzerland), Yehuda Carmeli (Israel), John Conly (Canada), Ben Cooper (United Kingdom), Anne Cori (United Kingdom), Francesco Di Ruscio (Norway), David Eyre (United Kingdom), Michael Gasser (Switzerland), Petra Gastmeier (Germany), Yonatan Grad (United States), Rebecca Grant (Switzerland), Nicholas Graves (Singapore), Stephan Harbarth (Switzerland), Anthony Harris (United States), Susan Huang (United States), Karima Hunter (United States), Alejandro Jara (Chile), John A. Jernigan (United States), Gwen Knight (United Kingdom), Alison Laufer Halpin (United States), Fernanda Lessa (United States), Marc Lipsitch (United States), Mark Loeb (Canada), Eric Lofgren (United States), Kalisvar Marimuthu (Singapore), L. Clifford McDonald (United States), Bonnie Okeke (United Kingdom), Ben Park (United States), Didier Pittet (Switzerland), Glen Lelyn Quan (Japan), Sujan Reddy (United States), Michael Rubin (United States), Hiroki Saito (Japan), Matthew Samore (United States), Marin Schweizer (United States), Erica S. Shenoy (United States), Rachel B. Slayton (United States), Arjun Srinivasan (United States), Andrew J. Stewardson (Australia), Jean-François Timsit (France), Maroya Walters (United States), David J. Weber (United States), Martin Wolkewitz (Germany), and Marie-Céline Zanella (Switzerland).
Financial support
The 2023 IPC Think Tank was co-funded by the US Centers for Disease Prevention and Control through a cooperative agreement with Training Programs in Epidemiology and Public Health Interventions Network (TEPHINET).
Competing interests
All authors report no conflicts of interest relevant to this article.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the views and official policies of their affiliated institutions, including the US Centers for Disease Control and Prevention and the US government.



 Open access
Open access