



Introduction
Loneliness is a distressing and pervasive experience, defined as the feeling that one's desired quantity or quality of the social connection is unfulfilled (Peplau & Perlman, Reference Peplau and Perlman1982). Among older people, it is associated with a diverse range of health outcomes, including cardiovascular disease and stroke (Valtorta et al. Reference Valtorta2016), increases in blood pressure (Hawkley et al. Reference Hawkley2010), changes in gene expression (Cole et al. Reference Cole2007), elevated cortisol (Adam et al. Reference Adam2006), cognitive impairments (Shankar et al. Reference Shankar2013) and physical decline (Perissinotto et al. Reference Perissinotto, Cenzer and Covinsky2012). A large body of epidemiological evidence has established loneliness as a strong predictor of premature death, with effect sizes similar to or greater than other well-established risk factors such as smoking and obesity (Elovainio et al. Reference Elovainio2017; Holt-Lunstad et al. Reference Holt-Lunstad, Smith and Layton2010; Luo et al. Reference Luo2012). According to a cross-national study by the Office for National Statistics (2014), the percentage of the UK population with access to supportive social relationships is the third-lowest of all the 28 EU nations. This makes loneliness a public health concern of particular relevance to the UK.
Although widely studied from a gerontological perspective, loneliness is not confined to old age and is particularly prevalent among young adults (Victor & Yang, Reference Victor and Yang2012; Qualter et al. Reference Qualter2015). A survey by the Mental Health Foundation (2010) has indicated that the proportion of people in the UK who often feel lonely, worry about feeling lonely, and seek help for loneliness is highest among younger people (aged 18–34 years) compared with older age groups. More than half of young adults surveyed reported having felt depressed at some time because they felt alone, compared with one-third of older respondents. Given this high prevalence, young adults today could be particularly at risk for loneliness-related health problems in later life. This high occurrence of loneliness among the young also underscores the need for greater understanding of how loneliness impacts young people's lives and the early factors that contribute to its emergence.
Feelings of loneliness have been shown to predict increases in depressive symptoms in both older and younger people (Cacioppo et al. Reference Cacioppo, Hawkley and Thisted2010; Vanhalst et al. Reference Vanhalst2012). As well as being a risk factor for psychopathology, loneliness may co-occur with a broad variety of other health and lifestyle-related impairments, making it a risk marker of high clinical relevance. This could be particularly true for young adults, given the high prevalence of loneliness in this group and the life changes that take place at this age, such as entering the labour market and leaving the family home. The burden of loneliness may undermine young people's confidence in their employment prospects or lead them to adopt maladaptive coping strategies and behaviours detrimental to later health. Wide-ranging descriptive research on loneliness is required to study its pervasiveness across different domains of health and functioning.
As well as examining the profile of loneliness in terms of its correlates in adulthood, it is important to consider individuals’ childhood history and experiences that may shape individuals’ vulnerability to loneliness. On the one hand, loneliness is likely to be an adversity that can befall people from a diverse range of socioeconomic and family backgrounds. On the other hand, emotional problems or difficulties with peer relationships in the childhood years may foreshadow greater feelings of loneliness in young adulthood. The investigation of these potential risk factors can help to identify groups of children who are particularly vulnerable to becoming lonely in adulthood and to identify targets for preventative interventions.
The aim of the present study was to examine the profile of loneliness in a prospective, contemporary, nationally representative cohort of 18 year-olds living in the UK. Cross-sectional data were used to investigate the functioning of lonely young adults in four domains: mental health, physical health and health risks, coping and functioning, and career prospects. Longitudinal data were used to examine the childhood history of lonely individuals, in terms of the family environment, child characteristics, mental health, as well as victimisation and social relationships.
Methods
Participants
Participants were members of the Environmental Risk (E-Risk) Longitudinal Twin Study, which tracks the development of a birth cohort of 2232 British children. The sample was drawn from a larger birth register of twins born in England and Wales in 1994–1995 (Trouton et al. Reference Trouton, Spinath and Plomin2002). Full details about the sample are reported elsewhere (Moffitt & E-Risk Study Team, Reference Moffitt2002). Briefly, the E-Risk sample was constructed in 1999–2000, when 1116 families (93% of those eligible) with same-sex 5-year-old twins participated in home-visit assessments. This sample comprised 56% monozygotic (MZ) and 44% dizygotic (DZ) twin pairs; sex was evenly distributed within zygosity (49% male).
Families were recruited to represent the UK population with newborns in the 1990s, to ensure adequate numbers of children in disadvantaged homes and to avoid an excess of twins born to well-educated women using assisted reproduction. The study sample represents the full range of socioeconomic conditions in Great Britain, as reflected in the families’ distribution on a neighbourhood-level socioeconomic index [ACORN (A Classification of Residential Neighbourhoods), developed by CACI Inc. for commercial use] (Odgers et al. Reference Odgers2012a, Reference Odgersb). Specifically, E-Risk families’ ACORN distribution matches that of households nation-wide: 25.6% of E-Risk families live in ‘wealthy achiever’ neighbourhoods compared with 25.3% nationwide; 5.3% v. 11.6% live in ‘urban prosperity’ neighbourhoods; 29.6% v. 26.9% live in ‘comfortably off’ neighbourhoods; 13.4% v. 13.9% live in ‘moderate means’ neighbourhoods; and 26.1% v. 20.7% live in ‘hard-pressed’ neighbourhoods. E-Risk underrepresents ‘urban prosperity’ neighbourhoods because such houses are likely to be childless.
Follow-up home visits were conducted when the children were aged 7 (98% participation), 10 (96%), 12 (96%) and at 18 years (93%). There were 2066 children who participated in the E-Risk assessments at age 18, and the proportions of MZ (55%) and male same-sex (47%) twins were almost identical to those found in the original sample at age 5. The average age of the twins at the time of the assessment was 18.4 years (s.d. = 0.36); all interviews were conducted after their 18th birthday. There were no differences between those who did and did not take part at age 18 in terms of socioeconomic status (SES) assessed when the cohort was initially defined (χ2 = 0.86, p = 0.65), age-5 IQ scores (t = 0.98, p = 0.33), or age-5 emotional or behavioural problems (t = 0.40, p = 0.69 and t = 0.41, p = 0.68, respectively). Home visits at ages 5, 7, 10 and 12 years included assessments with participants as well as their mother (or primary caretaker). The home visits at age 18 included interviews only with the participants. The Joint South London and Maudsley and the Institute of Psychiatry Research Ethics Committee approved each phase of the study. Parents gave informed consent and twins gave assent between 5 and 12 years and then informed consent at age 18.
Measures
Loneliness
Loneliness was assessed when participants were 18 using four items from the UCLA Loneliness Scale, Version 3 (Russell, Reference Russell1996): ‘How often do you feel that you lack companionship?’, ‘How often do you feel left out?’, ‘How often do you feel isolated from others?’ and ‘How often do you feel alone?’ A very similar short form of the UCLA scale has previously been developed for use in large-scale surveys and correlates strongly with the full 20-item version (Hughes et al. Reference Hughes2004). The scale was administered as part of a computer-based self-complete questionnaire. Interviewers were blind to participants’ responses. The items were rated ‘hardly ever’ (0), ‘some of the time’ (1) or ‘often’ (2). Items were summed to produce a total loneliness score (Cronbach α = 0.83). The heritability of loneliness has been reported in a previous study of the E-Risk cohort (Matthews et al. Reference Matthews2016), in which 38% of the variance in loneliness was estimated to be explained by genetic influences.
Correlates of loneliness in young adulthood
Functioning in adulthood was measured in terms of mental health, physical health and health risks, coping and functioning, and employment prospects. Mental health measures comprised past year diagnoses of depression, anxiety, attention-deficit hyperactivity disorder (ADHD), conduct disorder, alcohol dependence and cannabis dependence, as well as any instances of self-harm or suicide attempts between ages 12 and 18. Participants also reported whether they had seen a GP, psychiatrist, counsellor or psychotherapist for mental health problems in the past year. The physical health and health risk domain comprised measures of body mass index (BMI), C-reactive protein (CRP, a marker of inflammation), day-to-day physical activity and daily smoking. The coping and functioning domain included life satisfaction, coping with stress and problematic technology use. Participants were asked about their highest qualification level, and whether they were currently in employment or studying. Participants also completed questionnaires about their job search behaviour, their optimism about opportunities to succeed in their career, and their perceived job preparedness. Full details of measures are shown in Table 1.
Table 1. Summary of measures
ADHD, Attention-deficit hyperactivity disorder; BMI, body mass index; CRP, C-reactive protein; SES, socioeconomic status; IQ, intelligence quotient.
Childhood predictors of loneliness in young adulthood
Childhood measures were collected between the ages 5 and 12. Predictors were grouped in four domains: family environment, child characteristics, child mental health, and experiences of victimisation and social relationships. Family environment variables included maternal warmth, maternal depression, parental antisocial behaviour and exposure to domestic violence. Child characteristics captured IQ, theory of mind, and personality traits such as openness to experience, conscientiousness, extraversion, agreeableness and neuroticism. Child mental health variables were symptom counts of depression, anxiety, ADHD, conduct disorder and substance use (alcohol, tobacco and other drugs). Victimisation comprised measures of physical maltreatment by an adult and bullying by peers, while social relationships were indexed by social isolation. Full details of measures are shown in Table 1.
Data analysis
Concurrent associations between loneliness and mental health diagnoses, self-harm, suicide attempts and service use in young adulthood were tested using logistic regressions. Associations between loneliness and measures of physical health and health risks, coping and functioning and employment prospects were tested using linear and logistic regressions. Loneliness was entered as the independent variable in each analysis.
Longitudinal analyses were conducted using linear regression with age-18 loneliness as the outcome variable. Childhood predictors were entered individually. As a further step, to test the independence of the associations, the variables that were significantly associated with loneliness were entered together in blocks by domain (family environment, child characteristics, child mental health, victimisation and social relationships). Significant predictors from each domain were then entered into a final model.
The proportion of participants with missing data from the interview assessments was ⩽10% for all variables except CRP (13%). Cases with incomplete data were excluded listwise in all regression analyses. Participants in this study were pairs of same-sex twins, and therefore each family contained data for two individuals, resulting in non-independent observations. To correct for this, all regression analyses were based on the Huber–White or sandwich variance (Williams, Reference Williams2000), which adjusts the estimated standard errors to account for the dependence in the data. Regression analyses were conducted in Stata, version 14 (StataCorp, 2015).
Results
Prevalence of loneliness
In response to the four items about feelings of loneliness, 23–31% of participants reported experiencing any of these feelings ‘some of the time’, and 5–7% reported feeling them ‘often’ (Fig. 1). These rates indicate that feelings of loneliness in the general population of young adults are not uncommon but their frequency is high only in a small group. All subsequent analyses were conducted using the summed scale of these items (M = 1.57, s.d. = 1.94). Mean levels of loneliness did not differ across genders (males M = 1.51, females M = 1.62; p = 0.22), nor across SES groups (low M = 1.69, middle M = 1.52, high M = 1.49; p = 0.09).
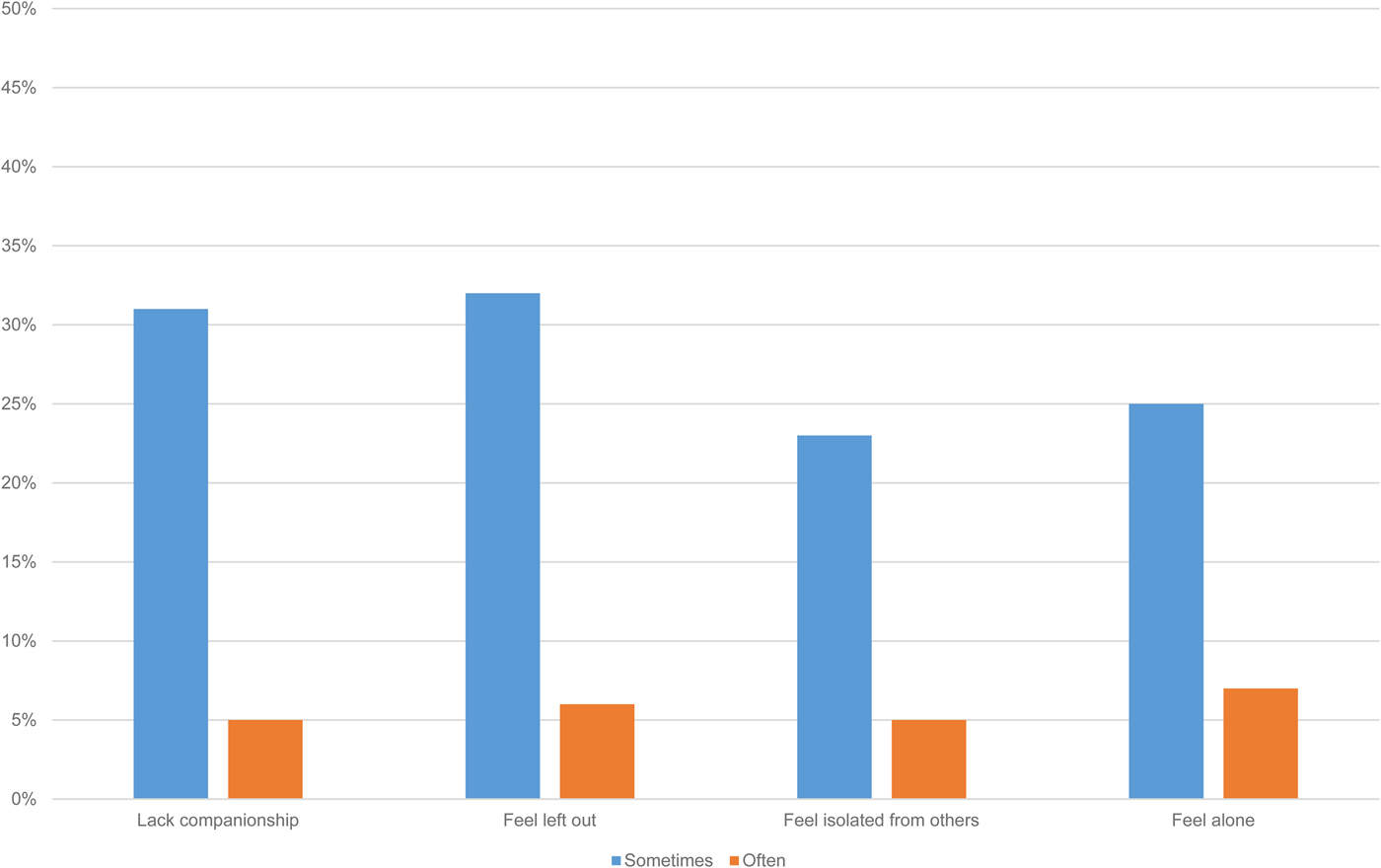
Fig. 1. Prevalence of reported feelings of loneliness among young adults.
Correlates of loneliness in young adulthood
Lonelier 18 year-olds were more likely to meet diagnostic criteria for depression, anxiety, ADHD, conduct disorder, alcohol and cannabis dependence, to have self-harmed, and to have attempted suicide (Table 2). Loneliness was most strongly associated with depression and anxiety, the odds of which more than doubled with a one standard deviation increase in loneliness. The overlap between loneliness and these two disorders is illustrated in Fig. 2. Lonelier individuals were also more likely to have sought help for mental health problems from a GP, psychiatrist, counsellor or psychotherapist in the past year.
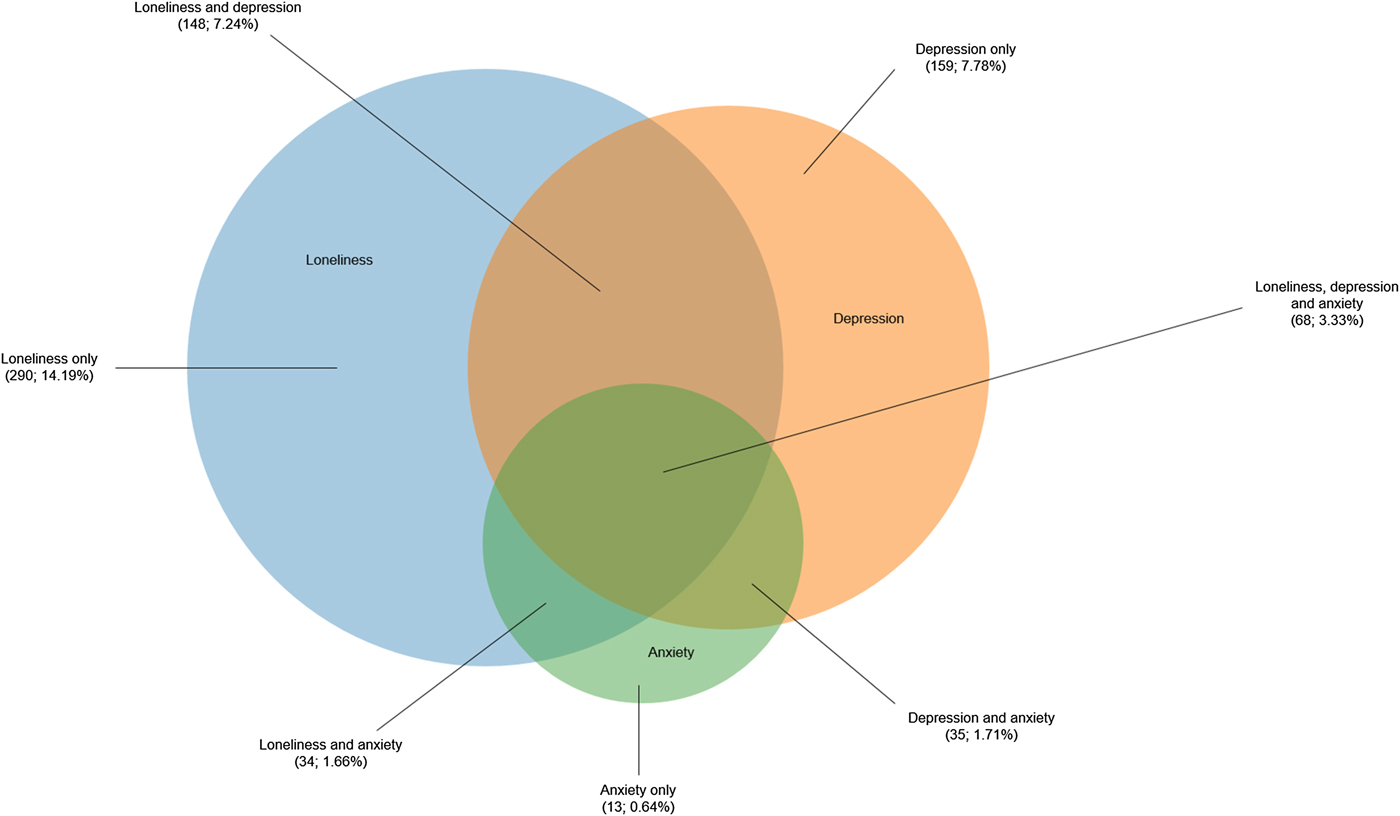
Fig. 2. Overlap in the prevalence of loneliness, depression and anxiety. For illustrative purposes, the loneliness scale was dichotomised by taking the top quartile.
Table 2. Characteristics of lonely young adults
M, Mean; N, number; s.d., standard deviation; β, standardised regression coefficient (interpretable as equivalent to a correlation); OR, odds ratio; CI, confidence interval; ADHD, attention-deficit hyperactivity disorder; BMI, body mass index; CRP, C-reactive protein.
All associations adjusted for gender and socioeconomic status. In logistic regression analyses, loneliness scores were standardised to obtain ORs based on a 1 s.d. increase in loneliness. Note: for sleep quality and coping with stress, higher scores reflect worse sleep and more positive coping strategies, respectively.
Loneliness was not associated cross-sectionally with indicators of poor physical health, such as BMI or CRP (Table 2). However, it was associated with risk behaviours that predict future ill health: lonelier individuals engaged in less day-to-day physical activity and were more likely to be daily smokers. Lonelier young adults had lower overall life satisfaction, reported more problematic technology use, and used more negative strategies to cope with stress, such as withdrawing and obsessing about problems rather than seeking help or taking pragmatic steps to rectify the situation. Loneliness was unrelated to individuals’ efforts to seek employment. Nonetheless, lonelier 18 year-olds were more likely to be out of work and education, and to have low educational qualifications. Regard to job market preparedness, lonelier individuals rated themselves lower in terms of their personal attributes (e.g. team working), but not their practical skills (e.g. computer programming). They also reported lower optimism about their ability to succeed in life.
Tests of robustness and independence
The associations between loneliness and each mental health disorder were tested further by controlling for prior symptoms of the disorder in childhood. All associations remained significant (Table 3). As a further step, to test the independence of each association, all comorbid mental health problems in young adulthood were additionally controlled for. Loneliness remained independently associated with depression, anxiety, ADHD, conduct disorder, self-harm and suicide attempts, but not with alcohol or cannabis dependence.
Table 3. Associations between loneliness and mental health problems in young adulthood
N, Number; M, mean; s.d., standard deviation; OR, odds ratio; CI, confidence interval; ADHD, attention-deficit hyperactivity disorder.
Loneliness scores were standardised to obtain ORs based on a 1 s.d. increase in loneliness. All associations adjusted for gender and socioeconomic status.
The independence of the associations between loneliness and life satisfaction, coping, problematic technology use, job market preparedness (personal attributes) and optimism were tested by controlling for mental health problems. All associations remained robust to these controls (life satisfaction β = −0.29, 95% CI −0.34 to −0.25; coping β = −0.27, 95% CI −0.32 to −0.22; problematic technology use β = 0.17, 95% CI 0.12 to 0.23; job market preparedness β = −0.20, 95% CI −0.26 to −0.14; optimism β = −0.20, 95% CI −0.25 to −0.15). Furthermore, the associations between loneliness and lower job market preparedness and optimism remained significant when controlling additionally for being not in employment, education or training, and for having low qualifications (job market preparedness β = 0.19, 95% CI −0.26 to −0.14; optimism β = −0.19, 95% CI −0.24 to −0.14).
Childhood predictors of loneliness in young adulthood
Loneliness was not associated with aspects of the early family environment, including maternal warmth, maternal depression, parental antisocial behaviour and domestic violence in the home (Table 4). However, children who had higher levels of neuroticism, depression or anxiety, or who experienced bullying or social isolation in childhood were lonelier at age 18. When these predictors were considered together, they all remained independently associated with loneliness, although the effect sizes were small. IQ and theory of mind were associated with loneliness in the univariate analyses but became non-significant when controlling for other variables. Childhood ADHD, conduct disorder and substance use did not predict loneliness when controlling for depression and anxiety. Physical maltreatment was not associated with loneliness after social isolation and bullying were accounted for.
Table 4. Childhood predictors of loneliness in young adulthood
β, Standardised regression coefficient (interpretable as equivalent to a correlation); CI, confidence interval; IQ, intelligence quotient; ADHD, attention-deficit hyperactivity disorder.
All analyses adjusted for gender and socioeconomic status.
Discussion
Loneliness is an important determinant of long-term health and functioning. Although often presumed to be an affliction of older age, this study demonstrates that loneliness is also a common experience in young people, occurring indiscriminately across genders and socioeconomic strata. The findings also show that loneliness is a marker of poor functioning across many different domains of well-being and health. To reduce the public health burden of loneliness in later life, the experience of feeling lonely in this age group merits particular consideration.
This study builds upon previous research showing that loneliness is robustly associated with depression (Cacioppo et al. Reference Cacioppo, Hawkley and Thisted2010; Vanhalst et al. Reference Vanhalst2012) and extends these findings to a range of other mental health problems. Despite high comorbidity between the disorders under investigation, loneliness was independently associated with each one. The only exceptions to this were alcohol and cannabis dependence, possibly because substance abuse is a social activity among young adults (Borsari & Carey, Reference Borsari and Carey2001). This pervasiveness of loneliness across different mental health disorders could imply either that loneliness’ effect on psychopathology is pleiotropic in nature or, conversely, that individuals with any mental health disorder are more likely to feel lonely and marginalised.
With regard to physical health, long-term outcomes of loneliness may not present until later adulthood, and this could explain why no differences were found in BMI in this young cohort, whereas such an association has been found in other samples of adults (Lauder et al. Reference Lauder2006). The null association with CRP, however, is consistent with other findings which suggest that objective social isolation, rather than feeling lonely, may be more strongly associated with inflammation (Shankar et al. Reference Shankar2011). Nonetheless, the finding that lonelier individuals were more likely to engage in physical health risk behaviours could signal cause for concern with regard to health outcomes later in adulthood. Furthermore, a previous study using the same cohort (Matthews et al. Reference Matthews2017) found that lonelier individuals had poorer sleep quality in young adulthood, which may further compromise health over time.
Feelings of loneliness co-occur with difficulties in other domains of functioning, beyond mental and physical health. For instance, lonelier individuals reported poorer global satisfaction with their lives and adopted more negative ways of coping with stress. Regarding technology use, although social media and messaging apps could provide lonely individuals with opportunities to form and strengthen social connections with others (Nowland et al. Reference Nowland, Necka and Cacioppo2018), lonelier young adults in this study reported using technology compulsively, at the expense of other activities and obligations. Excessive use of electronic devices may, in turn, constitute an additional risk for impaired sleep quality (Carter et al. Reference Carter2016).
School leavers in the UK today enter an economy still recovering from the fallout of the 2008 financial crisis. Low wage growth, decreased job security and rising house prices mean that young people face considerable challenges and uncertainty in their pursuit of financial stability (Belfield et al. Reference Belfield2014). Even though they were from similar socioeconomic backgrounds, lonelier young adults had lower educational attainment by age 18 than their non-lonely peers and were more likely to be out of work and education. This suggests either that loneliness could be a force for downward social mobility, or alternatively that being unemployed could itself diminish individuals’ sense of belonging. Although they were no less committed to job-seeking, lonelier young adults were less optimistic about their career prospects. Lonely individuals are characterised by shyness and lower self-esteem (Cacioppo et al. Reference Cacioppo2006), and these traits may undermine their confidence in their ability to compete in the labour market. Low income and unemployment may, in turn, contribute to feelings of loneliness (Luhmann & Hawkley, Reference Luhmann and Hawkley2016).
The longitudinal findings indicate that young adults’ propensity to feel lonely can be shaped by experiences earlier in life. Adversities in the family environment, though important for other emotional and behavioural outcomes (Caspi et al. Reference Caspi2004; Jaffee et al. Reference Jaffee2007), do not appear to be associated specifically with loneliness. Instead, early risk factors for loneliness lie with children's own emotional health and experiences with their peers. It should be noted, however, that the effect sizes of these factors were small. Furthermore, while parental psychopathology and domestic violence did not predict loneliness, this does not rule out a potential role of other factors in the home, such as neglect or sibling relationship quality.
This study has some limitations. First, as loneliness was measured only at one time point, the directionality of the associations could not be tested. Further longitudinal research is needed to advance causal hypotheses about the observed associations. Second, it was not possible to investigate the stability of loneliness from childhood to adulthood. Different trajectories of loneliness during childhood and adolescence may predict different outcomes (Qualter et al. Reference Qualter2013). Third, because the sample consisted of twins, all participants had at least one sibling, which could mean that the correlates of loneliness are underestimated. Nonetheless, the prevalence of loneliness in this sample is similar to that found in other studies of young people (Mental Health Foundation, 2010; Victor & Yang, Reference Victor and Yang2012). Fourth, this study focused on residents of one particular country, and the generalisability of these data to other regions of the world is not clear. Similar research in different populations is required to establish whether loneliness and its correlates differ across national and cultural demarcations.
Conclusion
The implications of chronic loneliness for longevity (Holt-Lunstad et al. Reference Holt-Lunstad, Smith and Layton2010; Luo et al. Reference Luo2012; Elovainio et al. Reference Elovainio2017) attest to the importance of intervening early to prevent loneliness persisting across time. However, simply increasing individuals' amount of social contact with others is unlikely to be sufficient, as loneliness can be experienced even in the company of others. A meta-analysis of interventions to reduce loneliness indicates that the most successful strategies involve addressing destructive patterns of social cognition in a counselling or psychotherapeutic setting (Masi et al. Reference Masi2011). Furthermore, the findings of this study indicate that strategies to prevent the emergence of loneliness in young people should devote particular attention to children who experience problems of an internalising nature, or who are bullied or isolated by their peers.
Acknowledgements
The authors are grateful to the Study members and their families for their participation. The E-Risk Study is funded by the Medical Research Council (UKMRC grant G1002190). Additional support was provided by the National Institute of Child Health and Human Development (grant HD077482), the Economic and Social Research Council (grant ES/P010113/1), and by the Jacobs Foundation. Candice L. Odgers is a Jacobs Foundation and Canadian Institute for Advanced Research Fellow. Louise Arseneault is the ESRC Mental Health Leadership Fellow. Our thanks to the Nuffield Foundation, the Avielle Foundation, CACI, Inc., and to the members of the E-Risk team for their dedication, hard work and insights.
Declaration of Interest
None.






