



Introduction
Globally, 45 per cent of mortality among children under the age of 5 years is associated with nutrition-related factors (WHO, 2020). As an undernutrition indicator, stunting in the first 5 years of childhood has irreversible long-term consequences in adult life as well (WHO, 2019): people who experienced stunting in their childhood tend to suffer more frequently from a number of health conditions in their adult life such as diabetes, cardiovascular diseases, and mental disorders. Stunting also impedes cognitive development, therefore, the ability to learn in school and earn a living as an adult (Lumey et al., Reference Lumey, Stein and Susser2011; Roseboom et al., Reference Roseboom, van der Meulen, Osmond, Barker, Ravelli, Schroeder-Tanka, Van Montfrans, Michels and Bleker2000; Brown et al., Reference Brown, van Os, Driessens, Hoek and Susser2000). However, stunting can be prevented by proper measures that enable access to nutrition and well-being (WHO, 2018).
Studies show that large-scale forced migration put children in an even more vulnerable position in terms of nutrition (Hossain et al., Reference Hossain, Leidman, Kingori, Al Harun and Bilukha2019; Khaled, Reference Khaled2016). The conflict in Syria that started in March 2011 forced 6.6 million of its population to seek refuge outside of Syria, of which 47 per cent of them are children (UNHCR, 2023). In addition to the crisis in Syria that aversively affected the well-being of its people, forced migration was another shock for those who left Syria which turned into a humanitarian crisis. Stunting was already common among Syrian children before the forced migration; one-third of preschool children suffered from stunting in Syria during the pre-conflict period (FAO, 2005).
As a neighbouring country to Syria, Türkiye is the largest refugeeFootnote 1 hosting country with over 3.6 million Syrians (48% of them are children) as of 2023 (UNHCR, 2023; Çavlin, Reference Çavlin2021). Both the government of Türkiye and humanitarian organisations have been supporting the basic needs of Syrians in their emergency response operations. This study aims to explore whether the financial assistance provided to the refugees had an influence on reducing stunting among children under the age of 5 years. We particularly analysed to what extent and along which pathways the financial assistance provided to Syrian refugees in Türkiye reduced stunting among children under the age of 5 years through an empirical analysis of the 2018 Turkey Demographic and Health Survey Syrian Migrant Sample (TDHS-SR) data by applying the logistic regression method.
Since their arrival, refugees in Türkiye were assisted by large- to small-scale organisations and various institutions (Turk, Reference Turk2016). Starting from 2016, the ECHOFootnote 2 -funded Emergency Social Safety Net (ESSN) programme was introduced as the largest cash assistance programme in the world, reaching over 1.5 million refugees in Türkiye in 2018 – when the research data was collected (Cuevas et al., Reference Cuevas, Inan, Twose and Celik2019). Aygun et al. (Reference Aygun, Kirdar, Koyuncu and Stoeffler2021) documented higher likelihood for sending children to school among beneficiary households from the ESSN, underlying the opportunity cost and direct cost of schooling. While the ESSN remains one of the main income sources, the financial assistance variable used in this study covers all kinds of financial assistance provided to only Syrian refugees in Türkiye.
Literature and background
Forced migration and nutritional well-being
Shocks like wars, conflicts, or disasters have a detrimental effect on the nutritional well-being of the affected people, as they interrupt stability as in the case of the Dutch Hunger Winter or the Great Famine in China (Lumey et al., Reference Lumey, Stein and Susser2011; Huang et al., Reference Huang, Li, Wang and Martorell2010; Angell-Andersen et al., Reference Angell-Andersen, Tretli, Bjerknes, Forsén, Sørensen, Eriksson, Räsänen and Grotmol2004). Forced migration is another form of shock for people; their displacement is involuntary and driven by push factors (Lee, Reference Lee1966) such as crises and conflicts in country of origin as in the case of the Rohingyas, Afghans, and South Sudanese (UNHCR, 2021b) or environmental conditions like in Somalia, Ethiopia, India, and Pakistan (Migration Data Portal, 2021). Along with food insecurity, forced migrants experience multiple challenges all at once, including poor living conditions, shattered livelihoods, and lost social capital, which worsen their nutritional status. For instance, the size of Venezuelan refugees and migrants in Colombia, Peru, and Ecuador who consume only one meal a day increased from 15 per cent in 2019 when they first arrived increased to 25 per cent in 2020, leaving them in an unhealthier condition with insufficient food intake (WFP, 2020a).
As forcibly displaced people often arrive in a new location without any resources, they primarily rely on assistance provided by humanitarian actors to meet their basic needs and prevent further deterioration (Jacobsen, Reference Jacobsen, Fiddian-Qasmiyeh, Loescher, Long and Sigona2014; Young et al., Reference Young, Aklilu, Were, Catley, Leyland, Borrel, Roberts, Webb, Holland and Johnecheck2002). Fenn et al. (Reference Fenn, Myatt, Mates, Wilkinson and Khara2021) found that general food distribution significantly decreases stunting among all children in refugee camps in Chad and any interruption of the operation interferes with that positive outcome. In contexts where the modality of intervention is cash assistance, a significant impact is observed on growth and reduction in stunting among children in Mexico (Fernald et al., Reference Fernald, Gertler and Neufeld2008), in Pakistan (Fenn et al., Reference Fenn, Colbourn, Dolan, Pietzch, Sangrasi and Shoham2017), in Yemen (Kurdi et al., Reference Kurdi, Breisinger, Ibrahim, Ghorpade and Al-Ahmedi2019), and in Ecuador (Paxson & Schady, Reference Paxson and Schady2010). Furthermore, a cross-sectional data from 70 refugee sites in 17 countries shows that humanitarian assistance decreases the mortality rate of children under the age of 5 years in refugee settings (Tan et al., Reference Tan, Spiegel, Haskew and Greenough2016).
Among other factors, the stability in institutions and sufficient infrastructure in the destination is known to be a determinant for the nutritional well-being of displaced populations. Aside of the food intake, access to clean water and sanitary systems, adequate healthcare, and proper housing with good lighting and ventilation are equality important for nutritional well-being (UNICEF, 2021). Studies show that despite the initial shock of the forced (and even for voluntary) migration, refugees and migrants living in better developed countries have positive nutritional outcomes for children, particularly decrease in stunting figures among them (Pak, Reference Pak2010; Merndoza & Dixon, Reference Mendoza, Dixon, Medicine and Hernandez1999; Yip et al., Reference Yip, Scanlon and Trowbridge1992; Schumacher et al., Reference Schumacher, Pawson and Kretchmer1987). In the settings where infrastructure is inadequate, the nutritional status of the refugee and displaced children worsens; Tresalti et al. (Reference Tresalti, Abdulle, Ismail, Manni and Magalini1985) found that diarrhoea was the most common reason for child mortality among infants in the Somalian refugee camps as parents had to feed them powdered milk prepared with contaminated water. Similarly, the already poor sanitation and crowdedness in Rohingya refugee camps worsened with COVID-19 and resulted in increase in stunting among the children to 30 per cent (Jean, Reference Jean2020). In unstable settings such as militant control in Mogadishu that interrupted humanitarian assistance and led to higher child mortality among the internally displaced population (UN, 2011). Given that Türkiye is a destination with stability and adequate infrastructure for Syrian refugees, it is expected in this study to observe an improvement in overall nutritional status.
The length of stay in the destination is another factor that improves nutritional well-being among the refugees. Food insecurity and child hunger are found to be higher among the newcomers compared to the refugees who are more settled (Hadley et al., Reference Hadley, Zodhiates and Sellen2007; Sellen et al., Reference Sellen, Tedstone and Frize2002). The longer the refugees live in a country, they learn more about how the healthcare system functions and how to access it, start looking for formal or informal livelihood opportunities to generate income, and learn where to find affordable food and such – all of which contribute to their nutritional well-being. However, this is more applicable for the refugees in non-camp settings, as residents of refugee camps often lack opportunities to access the labour market or other institutions (Ferris, Reference Ferris2019). Isolation from the host community delays their adaptation to the new location, which also influences the overall nutritional well-being of refugee households. Aside from the stunting-related variables used in this study, these factors in refugee-specific context will be taken into account.
Syrian refugees in Türkiye and their nutritional well-being
Following the conflict in Syria that created the largest refugee crisis in the world (UNHCR, 2021a), the number of Syrians fleeing to Türkiye was recorded as 3.6 million in 2018 and composed 4.5 per cent of the entire population (DGMM, 2023). Even though the first arrivals were placed in Temporary Accommodation Centers,Footnote 3 the overwhelming majority settled among the host community. In 2023, less than 2 per cent of the refugee population is living in camps (DGMM, 2023).
Syrians in Türkiye has a young population structure; 48 per cent of them are children and almost one-third of the children are under the age of 5 years (DGMM, 2023). It is estimated that 450,000 babies have been born in Türkiye between 2011 and 2019 (Multeciler Dernegi, 2021). Furthermore, given that 77 per cent of the adult women among Syrian refugees are at reproductive age (15–49), the number of children is expected to increase. Because young children are at higher risk of malnutrition, the refugee population in Türkiye is already fragile with high number of child dependents in the households.
The Syrian refugees had inadequate nutritional well-being in the early years of their arrival. According to a survey conducted in the Southeast of Türkiye in 2013, 78 per cent of the non-camp refugee households stated not having enough money to purchase enough food (AFAD, 2014), and in 2015, one-third of the households did not have acceptable food consumption, 66 per cent were prone to food insecurity (WFP, 2016). The same reports show that 19 per cent of households were below the poverty line, of which 93 per cent were below complete poverty line.Footnote 4
Stunting among Syrian children was already prevalent in pre-conflict period and remained as a problem upon their arrival. Though, it declined over time. According to the 2014 collaborative report of AFAD et al. (2016) on malnutrition among refugee children, the prevalence of stunting was 24 per cent among 6- to 60-month-old children, while about 9 per cent of those children were classified as severely stunted. Stunting is common among Syrian refugee children in Lebanon (12%) and Jordan (8%) as well, yet the prevalence is higher among refugees in Türkiye as they are mostly from the rural northern regions of Syria where stunting was already above the Syrian national average (UNHCR, 2014; UNICEF & WFP, 2013; JDHS, 2012; PAPFAM, 2002). In 2016, a study on Syrian refugee children in Türkiye concluded that malnutrition is the second largest problem among Syrian refugee children in Türkiye, following access to education (CHKP, 2016).
The influx of refugees necessitated certain policy-related and humanitarian actions. Exceeding its refugee hosting capacity, the government of Türkiye granted Temporary Protection status to the Syrians, integrated them into its social security system, and provided them free access to services like healthcare and education (DGMM, 2021), and managed to absorb the refugees thanks to its established systems and structures. National and local humanitarian organisations worked to assist the refugees various ways within their capacities under the coordination of AFAD. Shelter and nutrition are among the main activities of NGOs for refugees in Türkiye (Turk, Reference Turk2016). Starting from the hot meals delivered by the Turkish Red Crescent since the refugee arrival in the camps, food parcel deliveries, market gift cards, and food voucher programmes were provided by local to large-scale organisations to vulnerable refugee households, both in camps and off-camp settings (ASRA, 2020; WFP, 2019; TRC, 2014; IOM, 2014; IHH, 2012).
In late 2016, the ESSN, the largest cash assistance programme in the world, was introduced for the refugees in Türkiye. Implemented by WFP and Turkish Red Crescent in collaboration with the government of Türkiye, the ESSN reached over 1.5 million Syrian refugees in 2018, among whom 60 per cent were children (WFP, 2018). Each eligible beneficiary received TRY 132 (equivalent to approximately USD 27 at the time) on average. Even though the programme allowed refugees to decide how to spend the assistance, 40 per cent of the assistance was spent on food items (WFP, 2018).
Although it does not specifically focus on children, WFP’s Comprehensive Vulnerability Monitoring Exercises (CVME) indicate that the nutritional well-being of the Syrian refugees in Türkiye improved over time, particularly among the ESSN beneficiaries. Acceptable food consumption –which is calculated through diversity and frequency of the food consumed in a household –increased from 81 per cent in 2017 to 83 per cent in 2018, and to 98 per cent in 2020 among the ESSN beneficiary households where the figures for the non-beneficiary households are 72 per cent, 90 per cent, and 99 per cent, respectively (WFP, 2020b; WFP, 2019; WFP, 2018).
Despite the overall improvement, nutritional well-being of refugee children remains as a concern. According to 2018 TDHS, only 33 per cent of Syrian refugee children in the age group 6–23 months consumed iron-rich foods the day before the study (HUIPS, 2019b). Furthermore, only 8 per cent of Syrian refugee children under the age of 2 years are fed with a minimum dietary diversity (Koç et al., Reference Koç, Saraç and Çavlin2020). The CVME reports also indicate that the decreasing trend of resorting to coping strategies to meet food needs reversed with the 2018 economic crisis both for beneficiary and non-beneficiary households. Such findings indicate deterioration in nutritional intake. Conversely, access to clean and sufficient water by 93 per cent of refugees in 2018 reflects the well-established infrastructural aspect of nutritional well-being (HUIPS, 2019b; WFP, 2019). Lastly, through time, refugees indicate some degree of adaptation by becoming aware of how to access resources and the labour market – though mostly informally – to generate income for their households (Abbasoğlu Özgören & Arslan, Reference Abbasoğlu Özgören, Arslan and Çavlin2021; Ceritoglu et al., Reference Ceritoglu, Yunculer, Torun and Tumen2017), which make them more self-reliant and likely to improve their nutritional well-being.
Methods
Data
The data source of this study is from the 2018 TDHS-SR (HUIPS, 2019b). Hacettepe University Institute of Population Studies (HUIPS), under the supervision of international DHS programme, conducts nationwide Demographic and Health Survey in Türkiye once in every 5 years since 1993. In addition to national sample (HUIPS, 2019a), the 6th edition for the first time includes a separate sample of Syrian migrants in Türkiye which gives a unique opportunity to study the nutritional well-being of Syrian children and to compare it with the outcomes of host community children. Even though the 2018 TDHS-SR has a different frame than the national sample, the complex sample design-adjusted approach, which refers to weighted, multi-staged, and stratified cluster sampling, was adopted for both samples. The survey provides information about Syrian households and Syrian women who are aged between 15 and 49 years. An adult household member who could give information about that household and other household members, and women at ages 15–49 years who usually live or stayed in visited household a night before the interview regardless of their marital status, were eligible to participate in the survey. The information about children under the age of 5 years was obtained from their mothers. The target sample size was 2,000 Syrian households located in 100 clusters in Türkiye, and a total of 2,391 Syrian women were interviewed with quite high response rates at both household and women (94.5% and 92.7%, respectively). Computer-Assisted Personal Interviewing (CAPI) was used for the data collection (HUIPS, 2019b).
The 2018 TDHS-SR provides detailed information about fertility and fertility preferences, family planning, marriage, reproductive health, infant and child mortality, maternal and child health, as well as nutritional well-being measurements of women and children. The weight and height of the interviewed women and their children under the age of 5 years were measured in a standardised way during the interviews. Thus, indicators like body mass index (BMI) for women aged 15–49 years, underweighting, stunting, and wasting for children under the age of 5 years, children born with low birth weight, feeding with minimum dietary diversity micronutrient intake for children aged 6–23 months, and consumption of foods and liquids in a day could be ranked among the substantial health indicators for Syrian migrant population in Türkiye (Koç et al., Reference Koç, Saraç and Çavlin2020; HUIPS, 2019b).
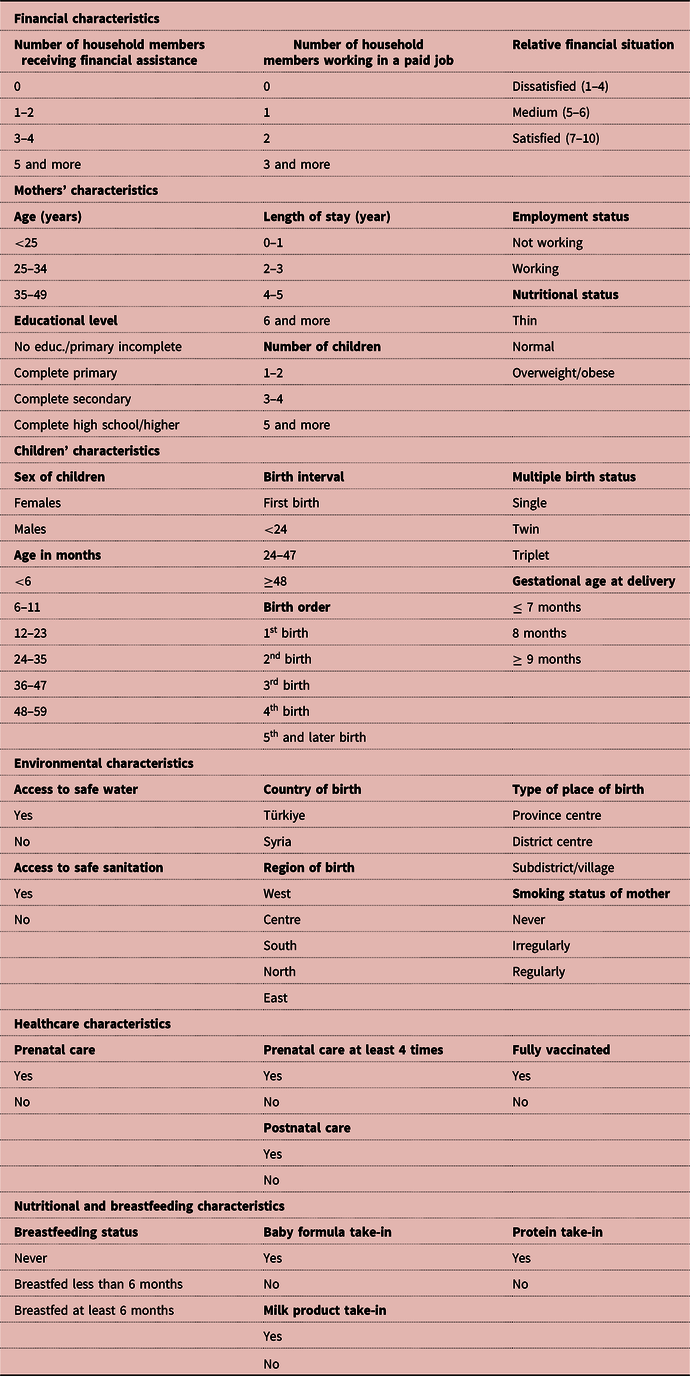
As the household dataset provides information about whether household members receive financial assistance and/or work for a paid job, these variables are integrated into the women’s dataset in order to answer the study questions. The financial assistance question covered any assistance to foreigners with protected status from any institution and was asked for all household members who are at the age of 12 years and over. The immigrant payment information is distinguished from all other payments such as retirement, widow, orphan, and care pension. Moreover, the number of household members who are working in a paid job was included in this analysis given that it potentially impacts the financial situation of Syrian households. Information on the amount of income, contract type (full-time or part-time), length of contract (to measure the sustainability), etc., is not available. Thus, a proxy indicator – relative financial situation – was created to predict the missing information. The relative financial situation of the household refers to the household respondent’s perception about financial situation of that household, where ‘1’ on the scale represents not at all satisfied and ‘10’ refers to completely satisfied. The mother’s nutritional status was constructed according to WHO’s classification that assigns women whose BMI is lower than 18.5 as ‘thin’ and women whose BMI is higher than 25 as ‘overweight/obese’. The remaining women were labelled as ‘normal’. Mother’s age, educational level, length of stay (year) in Türkiye since the migration, number of children, and employment status were the other characteristics of mothers included in the analyses.
Sex and age (in months) of children, birth interval, birth order, multiple birth status, and gestational age at delivery were the variables assessed within the children’s characteristics due to the potential relationships with the incidence of stunting. Birth interval refers to the time (in months) passed between birth of the child and the previous birth, including ‘first birth’, ‘less than 24 months’, ‘between 24 and 47 months’, and ‘48 months and higher’ categories.
Environmental characteristics including access to safe water and sanitation, country, region, and type of place of birth, and smoking status of mother were utilised in the analyses with the thought that they may be influential on stunting. The information about place of birth for children could be obtained from the household list, covering detailed information for each household member.
Moreover, a set of predictors related to healthcare that includes whether receiving prenatal care and postnatal care, receiving prenatal care at least four times, and status of being fully vaccinated were controlled in the analyses. Prenatal care refers to receiving any prenatal care services (e.g., taking blood pressure, taking urine and blood samples, and having an ultrasound scan) from a skilled provider (doctor, nurse, and midwife) at a health facility. A dummy variable that shows at least four visits during pregnancy are constructed since it is suggested by the health system in Türkiye. The postnatal care represents the status of receiving a postnatal check for the newborn by a skilled provider.
Lastly, nutritional and breastfeeding characteristics were considered for the analyses. Breastfeeding status with the duration of 6 months, and whether baby formula, milk product, and protein were taken in were accounted in the statistical analyses. Milk product includes milk rather than baby formula, cheese, and yogurt, while protein covers the meat, fish, poultry, and egg consumed by the children with the last 24hours preceding the survey.
The variables used in the descriptive and multivariate analyses were presented in Table 1.
Table 1. Variables Used in Descriptive and Multivariate Analyses
Statistical techniques
The dependent variable in this study, stunting, is the outcome of a failure to receive adequate balanced nutrition over a long period of time and is also affected by external factors like recurrent and chronic illness (DHS, 2020). The height-for-age index provides an indicator of linear growth retardation among children and is used to measure stunting. Children who are less than 2 standard deviations below the median of the reference population in terms of height-for-age are considered stunted (short for their age) (HAZ<-2 SD). Children who are below -3 standard deviations from the median of the reference population are considered severely stunted (HAZ<-3 SD). Syrian children aged below 5 in Türkiye are the target group for the study.
The binary logistic regression analysis technique was used to investigate the impact of households’ financial assistance status on the stunting experience of Syrian children in Türkiye. The incidence probabilities of stunting for children, namely odds ratios, were calculated through the maximum likelihood estimation process. Furthermore, the variables were evaluated at the 0.05 and 0.01 significance levels and, the explanatory power of covariates was given for each logistic model.
The binary dependent variable for the probability of stunting experience among children under age 5 is as follows:
 $$f = \left\{ {\matrix{ {1,\;if\;children\;with\;stunting} \cr {0,\;if\;otherwise} \cr } } \right.$$
$$f = \left\{ {\matrix{ {1,\;if\;children\;with\;stunting} \cr {0,\;if\;otherwise} \cr } } \right.$$
Four different logistic regression models were employed to understand the impact of the financial assistance status of Syrian households on the incidence of stunting among children under the age of 5 years by holding other covariates constant.
Characteristics like birth interval and birth order, urban–rural differences, household income, income sources, changes in income, agricultural activities, and mothers’ characteristics like education indicated association with stunting (Kirk et al., Reference Kirk, Kilic and Carletto2018; Rahman, Reference Rahman2016; Westcott & Stott, Reference Westcott and Stott1977). Thus, the variables available in the dataset, namely mothers’ age, education level, employment status, nutritional status, as well as the number of children, birth interval, sex, age, gestational age at delivery, and birth order and multiple birth status of the children, were included in the analysis. A recent comparative study targeting Syrian refugee children and natives in Türkiye presents the effect of being born in origin country on stunting (Demirci et al., Reference Demirci, Foster and Kirdar2022). Accordingly, place of birth of refugee children was considered in this study by employing country, region, and type of place of birth for children in the models in addition to other environmental features such as access to safe water and sanitation, and smoking status of mother. The healthcare characteristics and nutritional and breastfeeding characteristics were the other predictors in the models due to the potential effects on stunting.
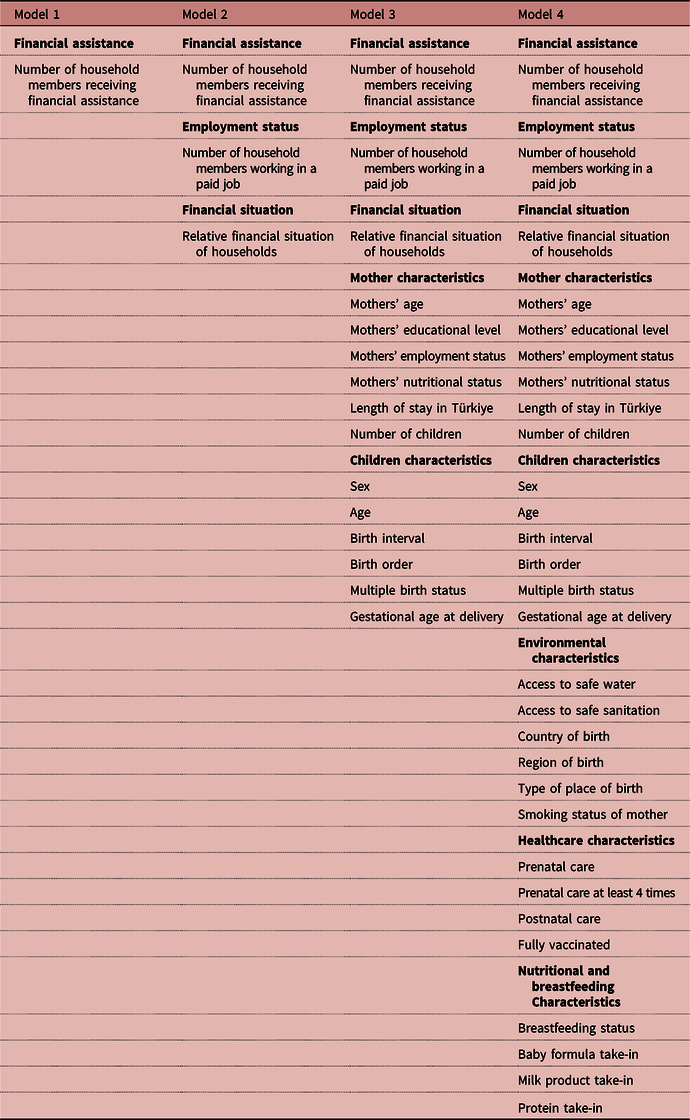
The stepwise approach was adopted in the model estimation process to identify the net impact of financial assistance status of households under the control of covariates. As such, Model 1 includes only the number of household members receiving financial assistance. The number of household members working in a paid job and relative financial situation were included in Model 2 to control income sources other than assistance. The mother and children characteristics were added into the Model 3 to observe their impact on the outcome. The last model includes environmental, healthcare, and nutritional and breastfeeding characteristics in addition to previous covariates included in Model 3 (Table 2).
Table 2. Logistic Regression Models and Covariates in the Models
Although analysis on stunting was conducted over children under the age of 5 years particularly, units of analysis were the children aged 13–36 months and children under the age of 3 years for the analyses of vaccination status, and nutritional and breastfeeding characteristics, respectively.
Limitations
The survey data has a limited number of variables regarding the assistance and income and lacks information on the amount of the assistance and generated income, which could have been used to explain the impact on stunting. The source of assistance, frequency and duration are not included in the survey questionnaire. It is also not possible to distinguish individual assistance from programmes targeting the entire household to control for during the analysis. Another limitation is that the question about assistance is only asked to household members who are at the age of 12 years and above. This, therefore, prevents the researchers from determining the number (and ratio) of people receiving assistance in a given household and impedes the adjustment for a precise analysis. It also makes it impossible to exclude the impact of a particular financial assistance programme on refugees’ nutritional well-being such as the ESSN.
Results
Descriptive results
Profiles of Syrian refugee households and household members
The data show that 48.3 per cent of refugee household members at the age of 12 years and over receive some kind of financial assistance in the form of assistance to foreigners with protected status, old age pension, widowhood or orphanhood payment, care pension, scholarship or any other payment. ‘Assistance to foreigners with protected status’, that refers to immigrant payment, is the most frequent type, received by 46.6 per cent of the refugee household members (Table 3), corresponding to 96 per cent of the assisted refugee households (Table 3). It is evident in many or most cases that this is likely the ESSN, which is by far the largest refugee assistance scheme (WFP, 2018).
Table 3. Percentage of Household Members at Age 12 and Over By Type of Financial Assistance, Number of Household Members Receiving Financial Assistance, and Number of Household Members Working in a Paid Job, 2018 TDHS-SR
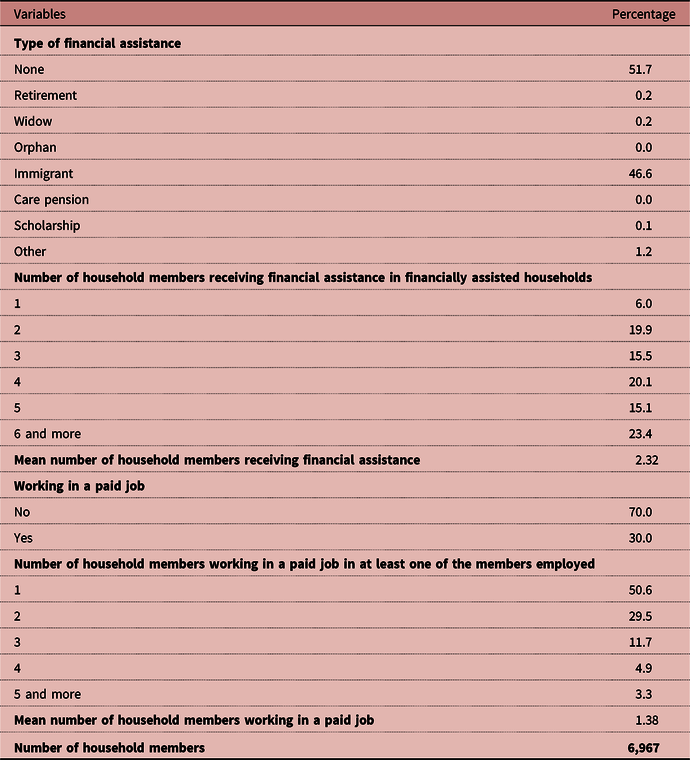
Among refugee households receiving financial assistance, only 6 per cent reported that only one person in the household receive assistance whereas in 38.5 per cent of the households, at least five members receive assistance. Consistently, the mean number of household members receiving financial assistance is 2.32 persons per household. In 39 per cent of refugee households, all members at the age of 12 years and over receive financial assistance in the form of ‘assistance to foreigners with protected status’ (Table 3). This finding seems to be in line with the implementation of the ESSN programme in Türkiye (WFP, 2018). Regarding paid jobs, in 30 per cent of the refugee households, there is at least one working member. In half of these households, only one member is working. On average 1.38 persons in a household are working in a paid job (Table 3).
Although around 82 per cent of refugee household members migrated to Türkiye between 2012 and 2018, the majority of the Syrians in Türkiye (64 per cent) came between 2012 and 2015. The mean length of stay is calculated as 4 years for Syrian refugees, excluding children born in Türkiye.
The data reflect the characteristics of the Syrian refugee population: Children under the age of 15 years account for 45 per cent of the population, of whom 15 per cent were born in Türkiye. Almost 18 per cent are under the age of 5 years, more than two-thirds of the households (66 per cent) have at least one member under the age of 5 years. Perhaps due to the high number of casualties during the conflict, proportion of the households with orphans or foster children under the age of 18 years is over 12 per cent. This figure is much higher than in host community households (only 2%). Similarly, widowhood is widespread among Syrian refugee women (3%), which again reflects the traces of conflict in Syria and loss of male household members.
To sum up, a broad-based population pyramid, prevalence of orphanhood, widowhood, and large family structure as extended families are associated with the vulnerable conditions of Syrian refugees. Also, there are more members receiving assistance than working members in an average Syrian household. This creates serious concerns around dependency on assistance and lack of self-sufficiency in the long run.
Stunting among Syrian refugee children
The percentage of stunting (HAZ<-2SD) is 17.4 per cent among refugee children under the age of 5 years, among whom, around 6 per cent are severely stunted (HAZ<-3 SD) (Table 4). When compared to other national health surveys conducted in pre-conflict Syria (i.e., 2009 Syria Family Health Survey (2009 SFHS), 2006 Syria Multiple Indicator Cluster Survey (2006 SMICS), stunting among Syrian children in Türkiye decreased: the prevalence of stunting was 25.7 per cent in 2001 (2001 SFHS), 22.4 per cent in 2006 (2006 SMICS), and 23.0 per cent in 2009 (2009 SFHS) (PAPFAM, 2009; UNICEF, 2008; PAPFAM 2002). According to OCHA, stunting has become a more significant concern within Syria since the conflict started (OCHA, 2019).
Table 4. Percentage of Children Under Age 5 Classified as Malnourished According to Height-For-Age (Stunting) by Number of Household Members Receiving Financial Assistance, Number of Household Members Working in a Paid Job, Relative Financial Situation of Households, and Length of Stay, 2018 TDHS-SR
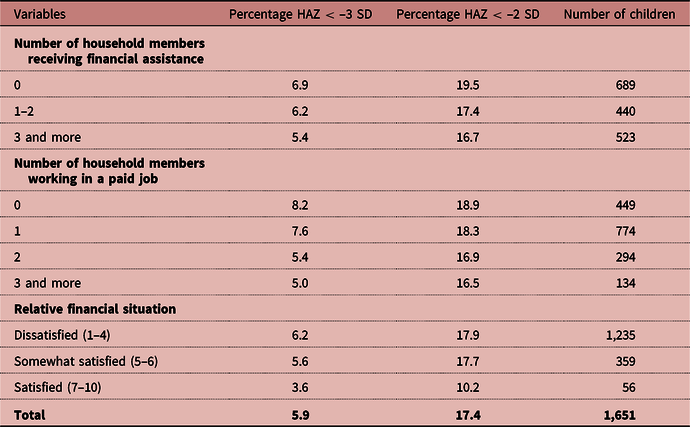
The prevalence of stunting is correlated with all three economic variables. The level of stunting is inversely related with the number of household members receiving financial assistance. The percentage of stunting is 20 per cent (of which 7% are severely stunted) among children in refugee households without financial assistance, while it decreases to 17 per cent in households with three or more members receiving financial assistance (of which 5% are severely stunted) (Table 4).
Stunting prevalence for refugee children also appears to be negatively related with the number of household members working in a job. Nineteen per cent of the refugee children in households without working members are stunted, whereas it is 17 per cent in households with three or more working members. Children in households without working members suffer from severe stunting the most (8%).
The effect of the perceived financial situation on stunting prevalence among refugee children is also apparent. Stunting among children decreases as satisfaction with the households’ financial status improves: stunting prevalence ranged from 10 per cent in satisfied households to 18 per cent in less satisfied households. Prevalence of severe stunting also decreases from 6 per cent to 4 per cent when satisfaction with the financial situation increases.
Length of stay in Türkiye is another variable inversely related with stunting among refugee children. As Table 5 shows, stunting prevalence is considerably higher among children whose mothers have been living in Türkiye for up to 1 year (22%) compared to those living in Türkiye for 6 or more years (12%) (Table 5).
Table 5. Percentage of Children Under Age 5 Classified as Malnourished According to Height-For-Age (stunting) by Mother and Children Characteristics, 2018 TDHS-SR
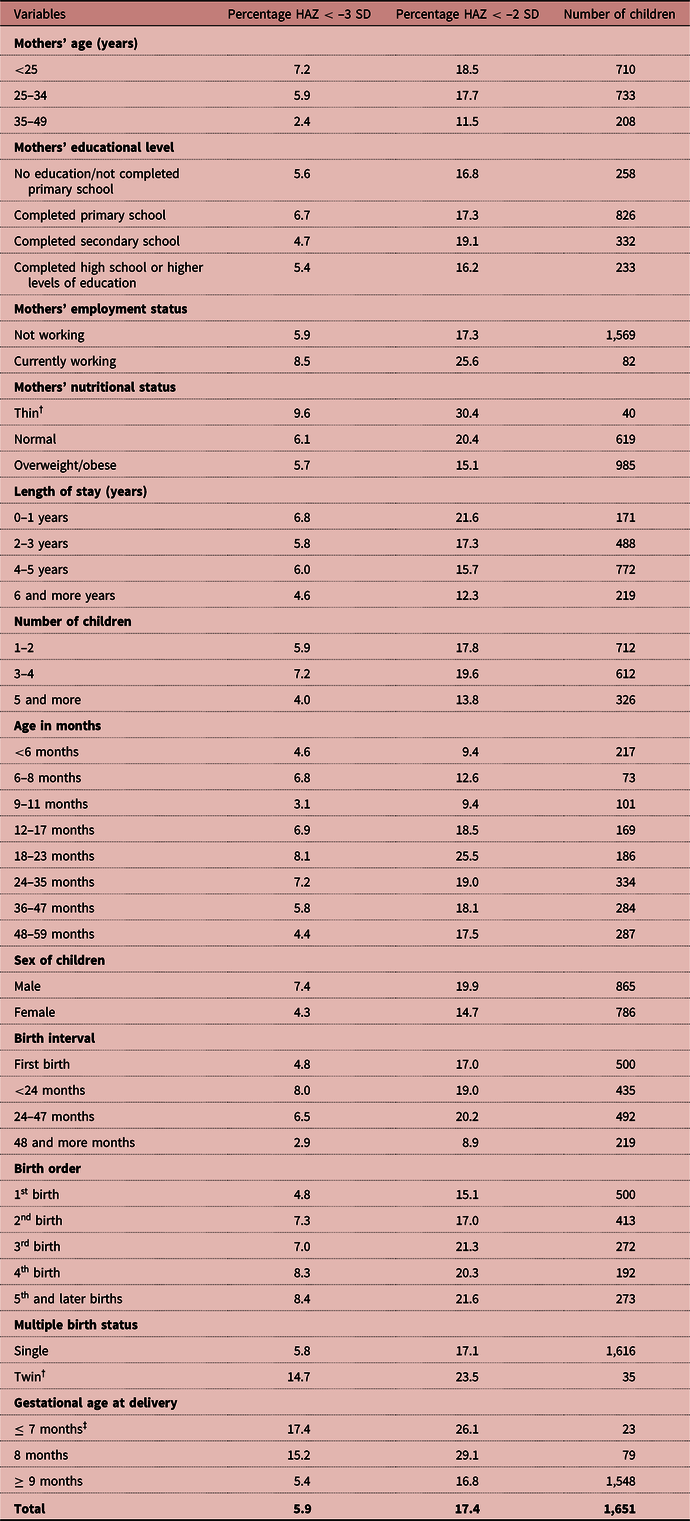
† Figures are based on 25–49 unweighted cases.
‡ Figures are based on less than 25 unweighted cases.
Stunting prevalence also varies by the socio-demographic, socio-economic, and nutritional characteristics of mothers. The prevalence of stunting among children whose mothers are under 25 years (19%) is higher than children whose mothers aged between 35 and 49 years (12%). Severe stunting is also the highest for children whose mother is under 25 years (7%), while it declines to 2% among children whose mothers aged 35–49 years. Stunting among children of normal-weighted mothers is 20 per cent – of which 6 per cent are severely stunted – and it is 15 per cent among children of overweight or obese mothers (Table 5). Mother’s education plays a role in stunting as well. While the level of stunting is highest among children whose mothers completed secondary education (19%), severe stunting is most common among children of primary school graduates (7%). Even though it is a tiny group, when the mother’s employment status is considered, stunting among children with working mothers (26%) is notably higher than children whose mothers are not working (17%). Severe stunting is also high among children whose mothers work (9%). There is no clear pattern on stunting prevalence among refugee children by the number of siblings, while it is the most common among children who have two or three siblings (20%) (Table 5).
While it is at the lowest among less than 12-month-old babies, 26 per cent of children aged 18–23 months are stunted; of which 8 per cent are severely stunted. Both stunting and severe stunting are more common among boys (20% and 7%, respectively) compared to girls (15% and 4%, respectively). Although stunting prevalence is 17 per cent for first-borns, it increases to 20 per cent for children whose birth interval is 24–47 months. Severe stunting, however, increases from 5 per cent among firstborns to 8 per cent if the birth interval is less than 2 years. Birth order appears to be negatively correlated with stunting until the third birth. Stunting prevalence reaches as high as 21 per cent among children who were third births, while it declined to 15 per cent for firstborns. Severe stunting is also higher for third and later births (7–8%) compared to first births (5%). Both stunting and severe stunting are more frequent among twins even though it is a tiny group, compared to single births. Stunting is considerably higher among children who were born in eighth months (26%) than children who were born in ninth months and thereafter (17%). Severe stunting is 5 per cent among children who were born within at least 9 months, while it reaches to 17 per cent among children who were born in seventh month and earlier (Table 5).
The percentage of stunting changes depending on the environmental, healthcare, and nutritional and breastfeeding covariates of refugee children as well. The percentage of stunting is higher among children who were born in Syria (22%) compared to those who were born in Türkiye (17%). Severe stunting is also higher among children born in Syria (9%) compared to children born in Türkiye (5%). Stunting is the highest among children who were born in subdistricts or villages (21%), regardless of the country. Moreover, a regional variation is observed among children born in Türkiye. Eighty per cent of children who born in the East and South regions are stunted, of which 7 per cent and 5 per cent are severely stunted.
Stunting prevalence is also higher among children whose mothers smoke regularly (19%) compared to those whose mothers never smoke (16%), implying a positive relationship. Additionally, access to safe water seems to have a negative association with stunting (Table 6).
Table 6. Percentage of Children Under Age 5 Classified as Malnourished According to Height-For-Age (Stunting) by Environmental, Healthcare and Nutritional and Breastfeeding Characteristics, 2018 TDHS-SR
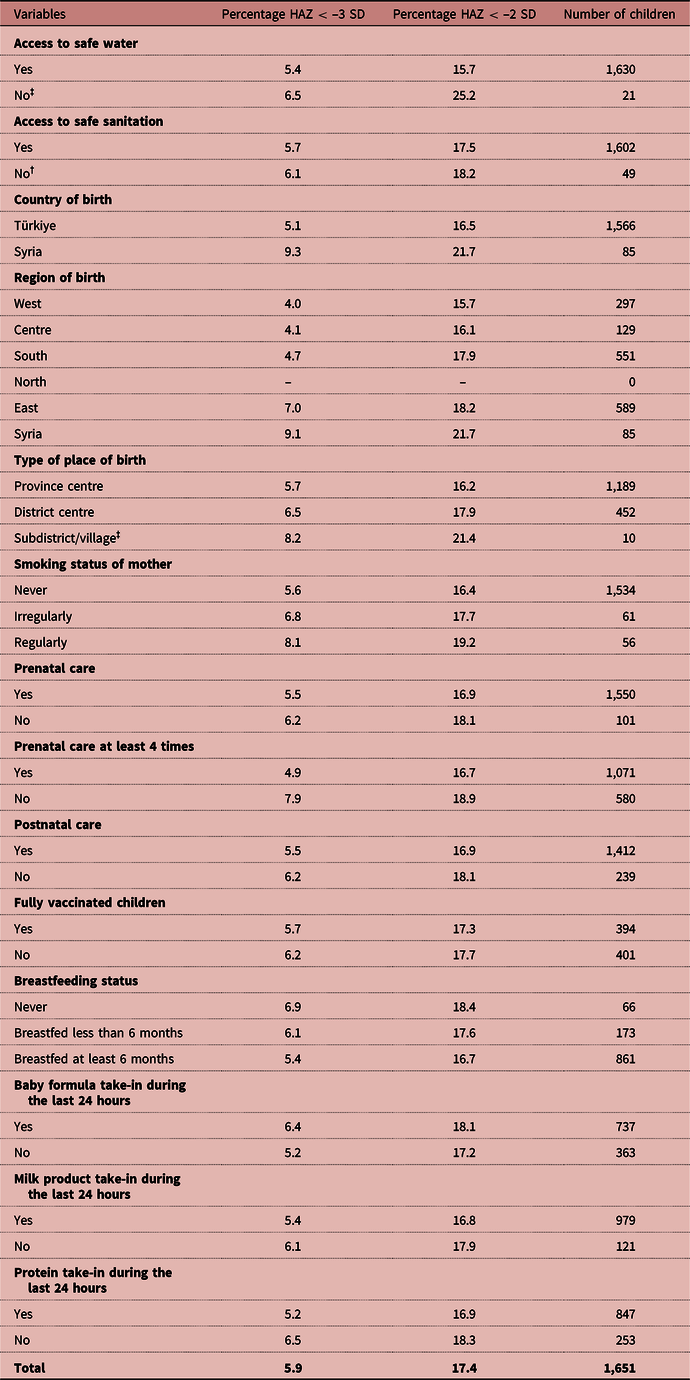
‡ Figures are based on less than 25 unweighted cases.
† Figures are based on 25–49 unweighted cases.
The stunting prevalence is almost the same and slightly less among children whose mothers received prenatal care, prenatal care at least four times, and postnatal care (17%) compared to those whose mothers did not receive prenatal care, prenatal care at least four times, and postnatal care (18–19%). Severe stunting is more common among children whose mothers did not receive prenatal care at least four times (8%) compared to children whose mothers received prenatal care at least four times (5%). The status of vaccination seems to have no influence on both stunting (17–18%) and severe stunting (6%). Similarly, breastfeeding status seems to have no substantial effect on stunting (17–18%), although severe stunting is slightly higher among non-breastfed children (7%) than children who breastfed at least 6 months (5%). Severe stunting is slightly less common among children who took in milk products and protein during the last 24 hours preceding the survey (5%) compared to ones who did not take in (6–7%) (Table 6).
To sum up, the prevalence of stunting among Syrian children under the age of 5 years has decreased after they fled to Türkiye, yet 17.4 per cent and 6 per cent of Syrian children were still stunted and severely stunted, respectively, as of 2018. Analysis also shows that stunting is negatively correlated with financial assistance, income generation, satisfaction with the household’s financial status, length of stay in Türkiye, gestational age at delivery, mother’s age and weight, access to safe water, being born in host country, being born in a province centre, receiving prenatal and postnatal cares, breastfeeding, and taking-in protein and milk product while it is positively correlated with mother’s employment status which may indicate that working women spend less time with their children to monitor their food intake.
Multivariate analysis
The first model that includes only the variable on financial assistance reveals that Syrian refugee children living in households with no members or one to two members receiving financial assistance are 20 per cent (p < 0.05) and 11 per cent (p < 0.05) more likely to suffer from stunting compared to those living in households with five or more financially assisted members. There is no difference in the risk of stunting between the children in households with three to four members receiving financial assistance and the ones in households with five or more members receiving financial assistance (Table 7).
Table 7. Logistic Regression Models for the Risk of Stunting Among Children Under Age 5
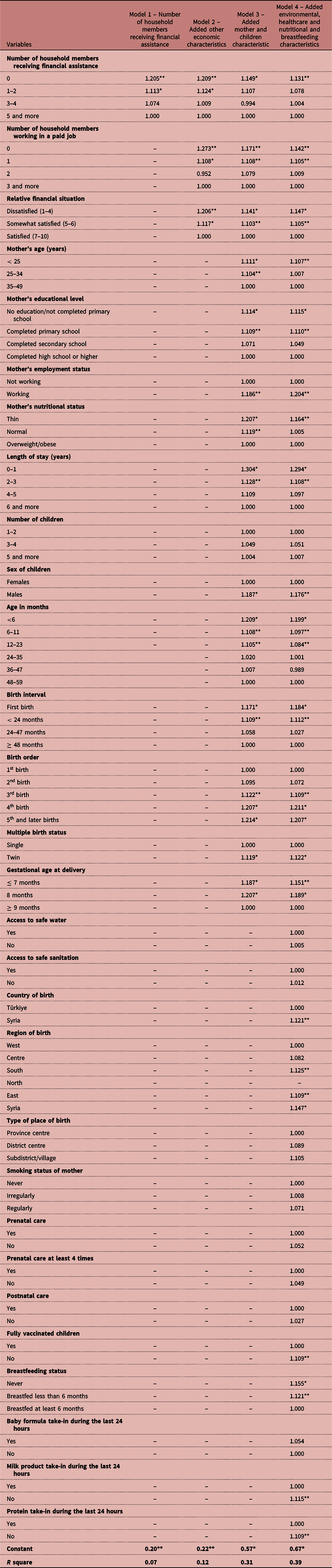
* p < 0.05; ** p < 0.01.
In Model 2, the impact of financial assistance on the risk of stunting among Syrian refugee children is still significant even after including the variables on the number of household members working in a paid job and the perceived financial situation of the household. The risk of stunting for children in households without any working member is 1.27 times (p < 0.01) higher than those living in households with three or more working members. The risk of stunting among children increases by approximately 11 per cent (p < 0.05) in refugee households with one working member compared to the households with three or more working members. Similarly, children in households dissatisfied or somewhat satisfied with their relative financial situation are 21 per cent and 12 per cent more likely to be under the risk of stunting than those in households satisfied with their relative financial situation (Table 7).
After adding the variables on mother and children characteristics into the equation, we observed that refugee children living in households without any members receiving financial assistance are still at a higher risk of stunting with 15 per cent (p < 0.05) than those living in households with at least three members receiving financial assistance. The risk of stunting among children in households with even one member receiving financial assistance seems to be similar with children living in households with at least three members receiving financial assistance (Model 3). In this model, the effect of the variables regarding the employment status of the household members and relative financial situation of household continues to persist in terms of the risk of stunting (Table 7).
Furthermore, Model 3 indicates that the risk of stunting among children whose mothers are working, have an educational level lower than high school, are younger than 35 years of age, and have less weight suffer from malnutrition and migrated to Türkiye in the last 3 years preceding the survey are significantly higher compared to reference categories. Additionally, boys, children under 24 months of age, non-breastfed children, first-born children and children whose birth interval is less than 24 months, twins, and children born before the ninth month have significantly higher risk of stunting compared to reference categories (Table 7).
The higher risk of stunting among children living in households without any members receiving financial assistance is still valid (p < 0.01) even after adding environmental, healthcare, and nutritional and breastfeeding characteristics in Model 4. The final model suggests that children who were born in Syria, and South and East regions of Türkiye, never breastfed or breastfed less than 6 months, not fully vaccinated, and did not consume milk products and protein within the 24 hours preceding the survey have significantly higher risk of stunting. Number of siblings, access to safe water and sanitation, type of place of birth, smoking status of mothers, receiving prenatal and postnatal cares, and taking-in baby formula are not significantly associated with stunting (Table 7).
When the logistic regression analysis for all the odds ratios for stunting in the study is considered, the Nagelkerke’s R2 increases from 7 per cent to 39 per cent. This shows that each model has an additive effect in the explanation of the stunting among Syrian refugee children. Additionally, all the constants in all models seem to be statistically significant at p < 0.01 or p < 0.05 levels. The overall assessment of the models suggests that the last model for all risks is the most explanatory model, and at the same time it fit the data better compared to the other models (Table 7).
Discussion
This paper carries out an analysis of the prevalence of stunting and its underlying factors among Syrian refugee children under the age of 5 years in Türkiye, with a special emphasis on the role of financial assistance. This study focuses on stunting in a refugee context from an empirical approach. Given Türkiye has been hosting the largest refugee population in the world for a decade, one can observe not only the change in stunting prevalence over time but also conduct causal research using the data which represent Syrian refugees in Türkiye through a separate sample in the 2018 TDHS (HUIPS, 2019b).
When compared with the previous findings from 2009 SFHS conducted in pre-conflict Syria, the 2018 TDHS results suggest that the refugee children in Türkiye have better nutritional status compared to pre-conflict period despite having experienced forced migration. According to the literature mentioned earlier, migration towards locations with stable institutions, good services, and infrastructure contribute to the nutritional well-being of migrants and refugees. The experiences of Syrian refugees in Türkiye also seem to fit into this category. The structural and socio-economic conditions in Türkiye play a facilitating role for refugees to overcome the double shock of conflict and forced migration. Along with access to food supplies, clean water, and sanitation infrastructure, the policies of the government of Türkiye that granted Syrian refugees Temporary Protection status, enabling them free access to healthcare and education services, as well as the right to settle in the province of their preference and receive work permits in the recent years, also contributed to these positive outcomes (Erdogan, Reference Erdogan2020). Socio-economic and administrative stability in Türkiye and funds from European Union allowed the country to absorb around 4 million refugees under temporary or international protection, while also possibly providing the underlying conditions for improved nutritional well-being compared to pre-conflict period in Syria. Furthermore, the non-camp context for refugees in Türkiye may have promoted interaction with the host community, facilitating the adaptation process of the refugees by enabling them to access the labour market, albeit mainly informally.
As the descriptive findings show, the length of stay in Türkiye significantly decreases stunting among refugee children. Unless later arrivals came with higher levels of stunting, this would reflect not only the adaptation process refugees naturally undergo in terms of their overall well-being but also their access to services like adequate water infrastructure and health services – which are determinants for nutritional well-being. One of the previous studies confirm that length of stay has positive effect on relative and financial well-being of refugees (Arslan & Çavlin, Reference Arslan, Çavlin and Çavlin2021; Abbasoğlu Özgören & Arslan, Reference Abbasoğlu Özgören, Arslan and Çavlin2021). As for a further comparative study on the impact of the conditions in countries receiving refugees, Jordan and Lebanon might provide comprehensive information to illustrate the impact of the structural and socio-economic conditions of the host country on the nutritional well-being of refugees.
This study examined the impact of financial assistance on stunting among refugee children in Türkiye. The causal analysis confirms the positive effect of the financial intervention on refugee lives. Given that forced migration is a shock that puts refugees in a vulnerable position, financial assistance prevents refugees from being trapped in the vicious cycle of vulnerability. They possibly alleviate the burden on refugees to meet their nutritional needs and therefore decrease stunting among children. Furthermore, since nutritional well-being goes beyond adequate food consumption, financial assistance allows refugees to spend their entitlement for their prioritised needs, which might be paying the water bill on one occasion and buying food in another. Comparative studies on the impact of financial assistance and in-kind assistance particularly on stunting among children under the age of 5 years would enrich the literature and provide insights for policymakers to determine the type of assistance to provide.
Another significant finding is that having someone working in the household is a much stronger predictor than financial assistance for the nutritional well-being of refugee children. The reason for this could be that income from employment is more amount, sustainable and promotes self-reliance for refugee households to live a dignified life. Indeed, employment has various latent contributions to migrants’ lives beyond generating income to meet household needs. It creates a network, increases interaction with the host community, and expands the refugees’ knowledge and understanding about the systems and structures in the host country. Furthermore, employment is considered to be a core indicator for migrant and refugee integration in a host country (Mayblin, Reference Mayblin2014; Phillmore, Reference Phillmore and Goodson2006). Whether they stay in the host country or move back to their home country or to a third country, employment allows refugees to blend into the society and the vulnerability of being a refugee to fade away. The impact of the income from employment on stunting is worth further investigation as it may also be correlated with other factors that positively influence nutritional well-being. For example, households earning an income may show better psychosocial characteristics (higher self-confidence or optimism), better care practices, or less instability.
From policymaking and humanitarian aspects, the findings indicate that providing financial assistance is effective on the nutritional well-being of Syrian refugee children under the age of 5 years as it serves as a safety net when refugees lack financial and social capital in the earlier years upon arrival. Yet, assistance tends to be of a temporary nature and, unlike self-reliance, may not always lead to all of the positive structural outcomes. Therefore, while income from both assistance and employment have positive effects on nutritional well-being, ultimately income from employment seems to have a greater impact. Both types of income are reversible – assistance can be terminated, and the working household member may become unemployed. Nevertheless, from a sustainability perspective, over time the assistance should be replaced with income from employment so as to achieve the best outcomes in terms of nutritional well-being.
Conclusion
In this paper, we examined the impact of financial assistance on stunting among Syrian refugee children in Türkiye by using the 2018 TDHS data, which contains a representative sample for the Syrian population in Türkiye. The trends show that stunting has decreased among Syrian refugees in Türkiye compared to the pre-conflict period in Syria, yet it is still more prevalent than amongst host community children. The regression analysis concluded that financial assistance positively contributes to the nutritional well-being of refugee children. However, the presence of a working member is another strong predictor to reduce stunting. The study also shows that regardless of whether the household is receiving assistance or not, prolonged stay in Türkiye decreases the prevalence of stunting among the Syrian refugee children as part of the adaptation process, although the improvement is more significant among households who received assistance. Other factors that have an impact on stunting include satisfaction with the household’s financial status, the child’s sex, age, birth interval and order, multiple birth status, gestational age at delivery, country and region of birth, vaccination, and breastfeeding status and milk products and protein consumption, and the mother’s age, weight, educational level, and employment status. The effect of country of birth could be attributable to factors associated with prenatal and postnatal care services provided in Türkiye. Moreover, children born in Syria have a forced migration history in early period of their life. Demirci et al. (Reference Demirci, Foster and Kirdar2022) reported the association between country of birth and anthropometric outcomes for Syrian refugee children, supporting our finding.
Further research is needed to examine the conditions where assistance and income prove to be most effective through more comprehensive data that includes the amount and frequency of the assistance, detailed information on in-kind assistance, amount of income generated by employment, and type of work engaged in by each household member to determine undignified ways of generating income such as child labour or begging.
Data availability statement
2018 TDHS-SR dataset can be requested from the link: http://www.tnsaveri_tdhsdata.hacettepe.edu.tr/request.php
Acknowledgements
We thank Başak Berçin Doğan from WFP Turkey Office and Jessica Bourdaire from WFP HQ for their useful comments and discussions that carried out during the writing the paper. We also thank WFP Turkey Office for supporting the project titled ‘An Analytical Study on the Contribution of Financial Assistance to the Nutritional Well-being of Syrian Refugee Women and Children in Turkey’ that was conducted in collaboration with Hacettepe University Institute of Population Studies (HUIPS). Lastly, our thanks to the HUIPS for allowing us to use 2018 TDHS-SR dataset.
Competing interests
The authors have no conflicts of interest to declare.
Ethical approval
The Ethics Committe of Hacettepe University approved the TDHS questionnaires before the data collection period. Moreover, each respondent was asked to give an informed consent to participate survey.








 Open access
Open access