



Introduction
Aggression and violence are behaviors that cause significant harm and distress to individuals and the community. The relationship between child and adolescent aggressive behavior with adult violent and non-violent crime is strong, and it is important to intervene early to interrupt the trajectory (Friedman, Taraban, Sitnick, & Shaw, Reference Friedman, Taraban, Sitnick and Shaw2021; Huesmann, Eron, & Dubow, Reference Huesmann, Eron and Dubow2002). Longitudinal studies show that aggressive behaviors are relatively common among young people, with 17–28% of adolescents in high-income countries self-reporting perpetration of aggressive acts (Henriksen et al., Reference Henriksen, Skrove, Hoftun, Sund, Lydersen, Tseng and Sukhodolsky2021; Patalay & Gage, Reference Patalay and Gage2019). While aggression is frequently demonstrated by children, most young people show reductions in the use of aggressive behaviors throughout adolescence (Nagin & Tremblay, Reference Nagin and Tremblay1999). However, persistent or maladaptive aggression during this formative time can have long-lasting detrimental impacts including school exclusion, mental health problems and service engagement, alcohol and drug abuse, and incarceration (Bobadilla, Wampler, & Taylor, Reference Bobadilla, Wampler and Taylor2012; Fite, Raine, Stouthamer-Loeber, Loeber, & Pardini, Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010; Marcus, Reference Marcus and Marcus2007; Moffitt, Caspi, Harrington, & Milne, Reference Moffitt, Caspi, Harrington and Milne2002; Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004).
Aggression has been differentiated by reactive (i.e. ‘hot’ or defensive) and proactive (i.e. ‘cold’ or calculated) behaviors (Raine et al., Reference Raine, Dodge, Loeber, Gatzke-Kopp, Lynam, Reynolds and Liu2006). While reactive aggression is hostile and emotional, proactive aggression is goal-oriented and employed in anticipation of self-serving outcomes (Bobadilla et al., Reference Bobadilla, Wampler and Taylor2012; Raine et al., Reference Raine, Dodge, Loeber, Gatzke-Kopp, Lynam, Reynolds and Liu2006). Heightened reactive and proactive aggressive behaviors are characteristic of disruptive behavioral disorders in young people, and antisocial personality disorder and psychopathy in adults (Card & Little, Reference Card and Little2006; Connor, Chartier, Preen, & Kaplan, Reference Connor, Chartier, Preen and Kaplan2010; Fite et al., Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010). It is important to assess novel methods for interrupting aggressive trajectories during adolescence, as persistent aggressive behavior can indicate more serious psychopathology and accounts for a significant proportion of referrals for psychological services (Fite et al., Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010; Hubbard, McAuliffe, Morrow, & Romano, Reference Hubbard, McAuliffe, Morrow and Romano2010). Identifying whether existing approaches that effectively reduce harm from shared risk factors (substance use, mental health) can prevent aggressive behavior is critical as few evidence-based interventions exist, especially for proactive aggression which is associated with predatory behavior, violence, and psychopathy in adulthood (Cox et al., Reference Cox, Leung, Baksheev, Day, Toumbourou, Miller and Walker2016; Fite et al., Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010; Matjasko et al., Reference Matjasko, Vivolo-Kantor, Massetti, Holland, Holt and Cruz2012).
Externalizing traits such as impulsivity and sensation seeking can be motivators for both reactive and proactive aggression during adolescence (Pérez Fuentes, Molero Jurado, Carrión Martínez, Mercader Rubio, & Gázquez, Reference Pérez Fuentes, Molero Jurado, Carrión Martínez, Mercader Rubio and Gázquez2016), and there is some support for the influence of internalizing traits on aggression (Marcus, Reference Marcus and Marcus2007). Further, substance use and mental disorders can share underlying psychopathology for other problem behaviors such as aggression, therefore targeting these shared risk factors is a promising way to prevent development and escalation of aggressive behavior (Castellanos-Ryan & Conrod, Reference Castellanos-Ryan and Conrod2011; Mewton et al., Reference Mewton, Lees, Squeglia, Forbes, Sunderland, Krueger and Teesson2020). School settings provide optimal contexts to deliver effective interventions to young people on a wide scale and prevent contact with the criminal justice system. Despite this, there is a lack of research examining the effectiveness of selective school-based interventions in reducing aggression over time, particularly those that target shared risk factors such as a substance and mental health, and personality. Research tends to show small-to-moderate effects for school-based prevention of aggression and violent behavior; however, long-term outcomes for programs are rarely assessed (Castillo-Eito et al., Reference Castillo-Eito, Armitage, Norman, Day, Dogru and Rowe2020; Kovalenko, Abraham, Graham-Rowe, Levine, & O'Dwyer, Reference Kovalenko, Abraham, Graham-Rowe, Levine and O'Dwyer2022). Existing research evaluating selective prevention is limited by quasi-experimental designs, measurement of violence through broad constructs of risk-taking, small sample sizes, short follow-up periods (average 3.65 months), and a focus on youth in clinical or indicated settings (Castillo-Eito et al., Reference Castillo-Eito, Armitage, Norman, Day, Dogru and Rowe2020; Kovalenko et al., Reference Kovalenko, Abraham, Graham-Rowe, Levine and O'Dwyer2022).
Effective prevention approaches typically incorporate cognitive behavioral therapy (CBT), motivational interviewing (MI), and the development of coping, social, and problem-solving skills to target known risk factors (Cox et al., Reference Cox, Leung, Baksheev, Day, Toumbourou, Miller and Walker2016; Kovalenko et al., Reference Kovalenko, Abraham, Graham-Rowe, Levine and O'Dwyer2022; Teesson, Newton, & Barrett, Reference Teesson, Newton and Barrett2012). The Preventure program is a selective prevention intervention that targets adolescents that relate highly to one of the four personality risk factors for substance use: sensation seeking, hopelessness, impulsivity, and anxiety sensitivity (Conrod, Stewart, Comeau, & Maclean, Reference Conrod, Stewart, Comeau and Maclean2006; Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016). Preventure provides personality-specific coping skills via a two-session brief intervention incorporating best practice principles for substance misuse (i.e. CBT, MI). Evaluations of the Preventure program have demonstrated its efficacy in reducing internalizing symptomology and externalizing problems associated with aggression among young people, such as depressive symptoms, alcohol-related harms, and conduct problems (Castellanos-Ryan & Conrod, Reference Castellanos-Ryan and Conrod2006; Conrod et al., Reference Conrod, Stewart, Comeau and Maclean2006; Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016, Reference Newton, Stapinski, Slade, Sunderland, Barrett, Champion and Debenham2022). For example, an Australian study found that compared to control, the personality-targeted Preventure program reduced conduct problems among young people who self-reported victimization of their peers (Kelly et al., Reference Kelly, Newton, Stapinski, Conrod, Barrett, Champion and Teesson2020). This formative work suggests that Preventure may hold promise for reducing aggressive behavior; however, its effectiveness has yet to be established.
To fill this research gap, this study aims to examine the impact of the school-based Preventure program on reactive and proactive aggressive behaviors over the long term from adolescence through to early adulthood.
Method
Study design
The current study examined data collected as part of a larger four-arm cluster randomized controlled trial (RCT) in 27 schools (N = 2607 young people) of school-based interventions to prevent substance use (the Climate and Preventure [CAP] study) (Newton, Teesson, Barrett, Slade, & Conrod, Reference Newton, Teesson, Barrett, Slade and Conrod2012; Newton et al., Reference Newton, Stapinski, Slade, Champion, Barrett, Chapman and Castellanos-Ryan2018). In line with study aims, the current analysis was restricted to data from independent schools (n = 9; young people from public schools were ineligible as ethics requirements precluded assessment of aggression) that were randomized to Preventure (n = 4 schools) or control (n = 5 schools).
Young people who provided informed consent and whose parents also provided passive consent were eligible to participate. A self-report questionnaire was administered across seven occasions from baseline to 6 months, 1, 2, 3, 5.5, and 7 years. Detailed information about the study design, sample size calculations, recruitment, randomization, and consent procedures has been described previously (Kelly et al., Reference Kelly, Grummitt, Birrell, Stapinski, Barrett, Boyle and Newton2021; Newton et al., Reference Newton, Teesson, Barrett, Slade and Conrod2012, Reference Newton, Stapinski, Slade, Champion, Barrett, Chapman and Castellanos-Ryan2018).
Participants
The Consolidated Standards of Reporting Trials (CONSORT) diagram summarizes participant flow and retention rates through the study for each condition (see Fig. 1). The current study examines data obtained from 339 young people in one of the four key personality traits attending nine schools that were randomized to receive Preventure (n = 145) or education as usual (n = 194) (i.e. school-level randomization). Only young people who scored at least one standard deviation above the mean for any of the four traits (as measured by the SURPS) were included in the analysis to allow for comparison of young people who were most at risk of negative aggression outcomes.
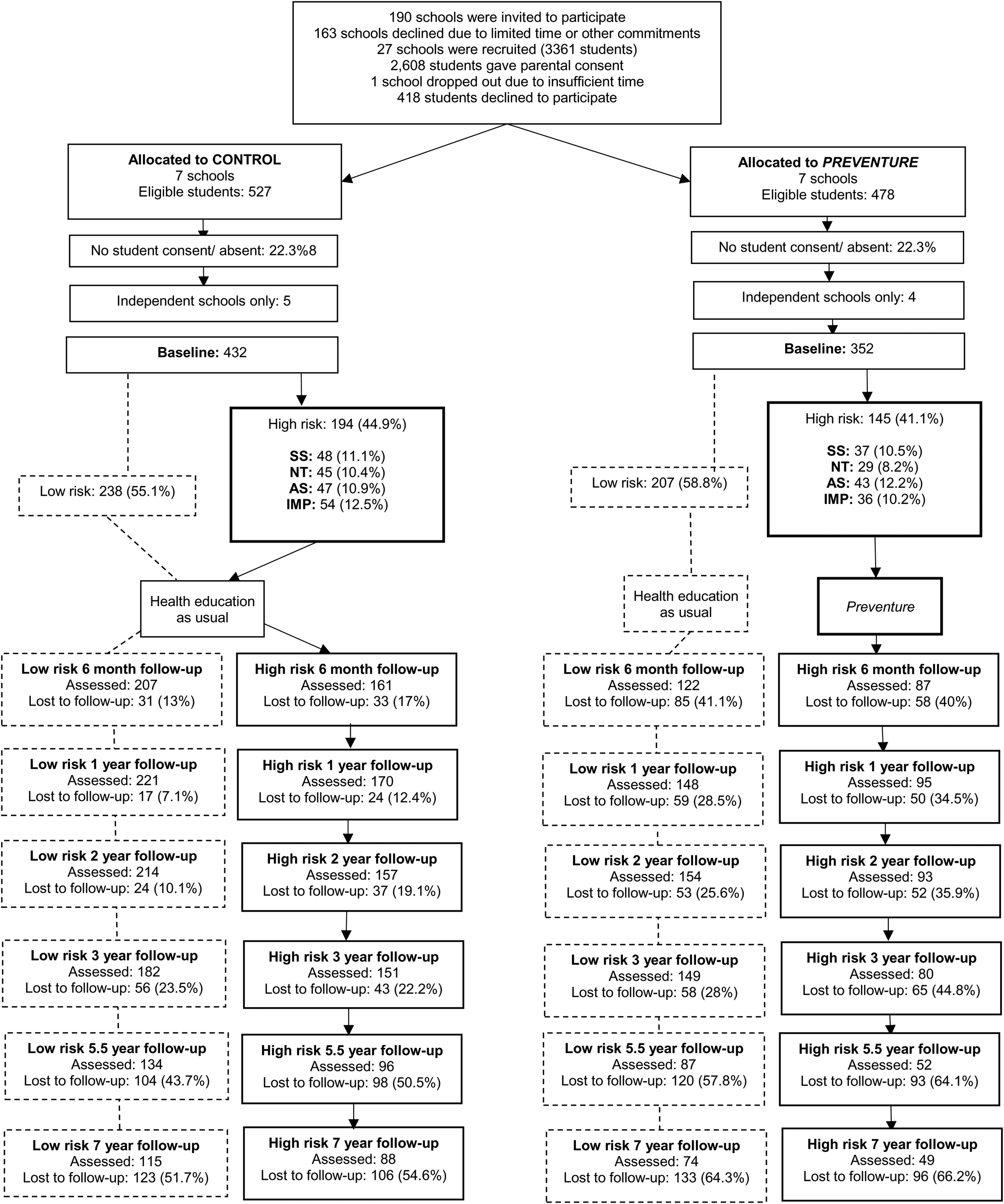
Figure 1. CONSORT flow diagram for participants in the Preventure and control groups at baseline and follow-up. SS, sensation seeking; NT, negative thinking; AS, anxiety sensitivity; IMP, impulsivity.
Intervention
Young people rating highly on one of the four personality traits in Preventure schools were invited to take part in the Preventure program, while those rating highly in these personality traits in control schools received the usual health curriculum. Participants in the Preventure intervention received a workbook specific to the personality trait that they scored highly in and were allocated to the relevant personality group where they participated in two 90-min group sessions delivered 1 week apart in school by trained facilitators (i.e. clinical psychologist and co-facilitator with a minimum training of Bachelor of Psychology with Honours). Core Preventure intervention components were CBT and MI techniques to assist participants in understanding and modulating maladaptive thoughts, feelings, and behavioral responses specific to the personality trait, practice goal setting and discuss healthy ways of coping. Young people were provided with guidance in challenging personality-specific cognitive distortions (e.g. in the impulsivity group this includes over-attribution of hostile intent) that can lead to risky behaviors (e.g. aggression). Further information about the Preventure intervention and primary outcomes are reported elsewhere (Conrod et al., Reference Conrod, O'Leary-Barrett, Newton, Topper, Castellanos-Ryan, Mackie and Girard2013; Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016, Reference Newton, Stapinski, Slade, Sunderland, Barrett, Champion and Debenham2022; Teesson et al., Reference Teesson, Newton, Slade, Carragher, Barrett, Champion and Conrod2017).
Measures
Demographic information
Young people were asked to report demographic information including age, gender, and country of birth. Socio-economic status (SES) was measured through the Index of Community Socio-Educational Advantage (ICSEA) (ACARA, 2020) which is a measure of socio-economic advantage that has been calculated for most schools in Australia. ICSEA scores are mean centered such that scores above zero indicate the young person attends a school with an above average ICSEA score, and scores below zero indicate the school has a below average ICSEA score.
Personality
The SURPS (Woicik, Stewart, Pihl, & Conrod, Reference Woicik, Stewart, Pihl and Conrod2009) is a 23-item scale that examines personality-related risk factors for mental health and substance use problems. The tool measures four dimensions of personality: impulsivity (e.g. I often don't think things through before I speak); sensation seeking (e.g. I enjoy new and exciting experiences even if they are unconventional); hopelessness (e.g. I feel that I am a failure), and anxiety sensitivity (e.g. I get scared when I experience unusual bodily sensations). Young people who scored at least one standard deviation above the school mean (~45% of the population) on one of the subscales of the SURPS were allocated to one of the four corresponding personality groups (Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016; Woicik et al., Reference Woicik, Stewart, Pihl and Conrod2009). Young people who were classified as high on more than one personality trait were allocated to the group where they deviated most from the mean to receive the intervention most relevant to them. The SURPS is scored on a four-point Likert scale (strongly agree–strongly disagree). The relationship between the SURPS subscales and emotional and behavioral problems has also been validated among Australian adolescents (Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016).
Aggression
Aggression was measured using the Reactive–Proactive Aggression Questionnaire (RPQ) (Raine et al., Reference Raine, Dodge, Loeber, Gatzke-Kopp, Lynam, Reynolds and Liu2006). The scale has 23 items pertaining to aggression (11 reactive, 12 proactive) to which there are three possible responses (never, sometimes, often) with scores ranging from 0 to 46. The scale has good cross-cultural validity and reliability (Fung, Raine, & Gao, Reference Fung, Raine and Gao2009) with higher scores indicating higher levels of total, proactive, and reactive aggression. Proactive items include ‘hurt others to win a game’ whereas reactive items included ‘have gotten angry when frustrated’. Composite scores on total, proactive, and reactive aggression were used to measure the outcomes of the intervention on aggression in this analysis. Internal reliability for the total, reactive, and proactive aggression scales at baseline was high (Cronbach's alpha = 0.92, 0.89, and 0.87, respectively).
Statistical analyses
Analyses were conducted in Stata IC 16 (StataCorp, 2019). Multilevel mixed-effects analysis for repeated measures was used to examine the effects of Preventure on aggression. As the data are clustered, multilevel mixed-effects models were estimated across three levels with change over time nested within individuals and individuals nested within schools. This approach uses baseline scores as the reference point, where estimates are based on participant-specific starting points and change over time (Gueorguieva & Krystal, Reference Gueorguieva and Krystal2004). The most appropriate model for change in the outcome over time (e.g. categorical, linear, quadratic) was determined using the likelihood ratio tests which were compared to the unconditional models. The covariance structure was selected using the fit statistics Akaike and Bayesian information criteria with the lower estimate indicating the more parsimonious and suitable model (Singer & Willett, Reference Singer, Willett, Singer and Willett2003). For all three outcomes (reactive, proactive, and total aggression) the linear model and the auto-regressive residual covariance structure were selected as the best fitting structures for the data. Intervention type was dummy coded (control = 0; Preventure = 1). Time is analyzed as a continuous variable representing 6 month time blocks across the seven follow-up time points (0 ‘Baseline’, 1 ‘6 months’, 2 ‘12 months’, 4 ‘24 months’, 6 ‘36 months’, 11 ‘66 months’, 14 ‘84 months’). A group by time interaction was included to examine the difference between the two randomly allocated groups in aggression over time. All models included an individual-level and school-level random intercept and gender as a covariate to control for baseline differences between schools and individuals. There was evidence to include a random slope at the individual level in addition to the random intercept for the reactive and total aggression models but not the proactive aggression model. Models were based on the intention to treat principle, with all young people rating highly on one of the four personality traits allocated to the Preventure or control group included in the analysis (N = 339). Mixed models were estimated with the stata command xtmixed, marginal means were calculated with the margins command. Effect sizes for significant interaction effects were calculated using Cohen's d (Feingold, Reference Feingold2013).
Power calculations based on the original trial (Newton et al., Reference Newton, Teesson, Barrett, Slade and Conrod2012) were conducted to detect a small effect size of 0.3 with 80% power assuming four time points. Based on the original sample size power calculations, this study (with seven time points) is powered to detect a small effect size (0.3). Further, a conservative estimate of 30% attrition across follow-up occasions results in a minimum of 260 young people (n = 130 per group) required to detect a moderate effect size which can be expected based on the existing international literature (Matjasko et al., Reference Matjasko, Vivolo-Kantor, Massetti, Holland, Holt and Cruz2012).
Missing data
Missing data were handled through maximum-likelihood estimation based on the baseline intention to treat principle which includes all young people in the study (n = 339). This is a valid approach to managing missing data in longitudinal analyses using all available information rather than omitting cases and assuming missing data are missing at random (MAR) (Gueorguieva & Krystal, Reference Gueorguieva and Krystal2004). The MAR assumption (i.e. missingness is assumed to be independent of unobserved variables) is considered reasonable as the analysis included several prior measurement occasions for key study variables and covariates (i.e. gender, baseline aggression) predictive of missingness. In addition, under the MAR assumption, multiple imputations were conducted to assess the robustness of findings against the impact of missing data (see the online Supplementary material for details).
Sensitivity analyses
A series of sensitivity analyses were conducted to confirm the accuracy of the findings. To examine the potential impact of non-normal data distribution, the analysis was repeated using square root transformed data. An exploratory Poisson analysis was also run which is suitable for left-skewed data and data that are zero inflated. Given the higher aggression scores at baseline with the Preventure group, change in aggression (e.g. change from baseline to 7 years) was plotted for each decile of baseline aggression scores to examine whether between-group differences were driven by participants with high baseline aggression scores. Lastly, a follow-up sensitivity analysis using the Mee–Chua test (Ostermann, Willich, & Lüdtke, Reference Ostermann, Willich and Lüdtke2008) for regression to the mean was applied. Further details about the sensitivity analyses can be found in the online Supplementary materials.
Results
Sample characteristics
The mean age of participants (N = 339) was 13.03 years (s.d. = 0.47, range 12–15) at baseline and 55.5% were male. Participants in the study came from above average socio-educational backgrounds according to the ICSEA scores (M = 7.26, range −85 to 50, s.d. = 36.53). Most young people in the sample were born in Australia (88.2%) with a small proportion of young people born in other English speaking (8.0%) and non-English speaking (3.5%) countries.
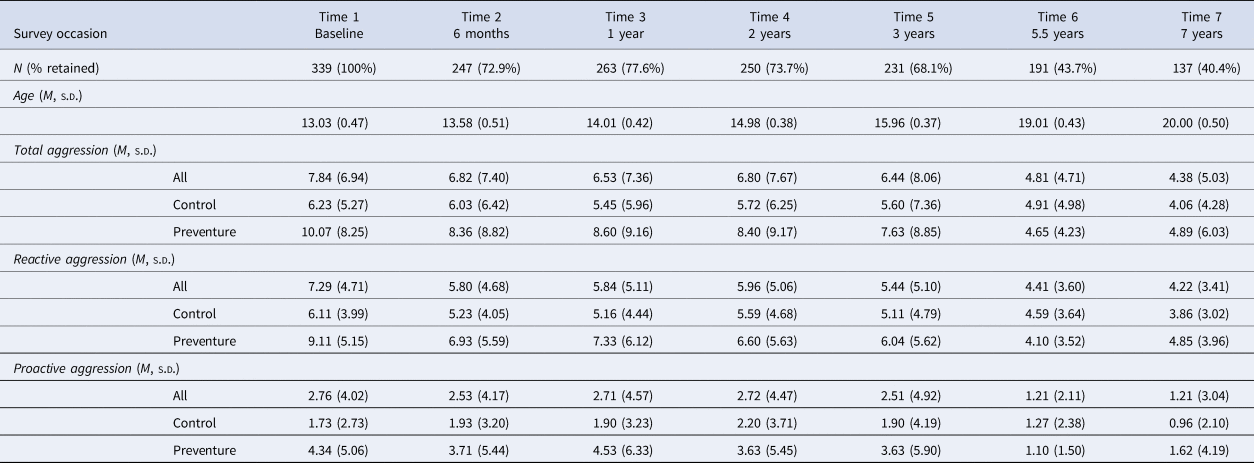
Young people were allocated to one of the four personality groups based on their SURPS scores: impulsivity (26.0%), sensation seeking (25.1%), hopelessness (22.4%), and anxiety sensitivity (26.6%). More male young people were allocated to the Preventure condition (85.5%) compared to control (33.0%). Both single sex and co-educational schools enrolled in the original cluster RCT and, by chance, random allocation resulted in a higher proportion of male students in schools in the intervention group compared to the control group. Aggression scores at each time point are reported in Table 1.
Table 1. Aggression scores (Reactive–Proactive Aggression Questionnaire) at each time point
Attrition analysis
Table 1 provides the details on the participant retention rates across all time points (range 40.4–77.6%). Most young people in this analysis (83.8%) completed surveys on two or more follow-up occasions. Attrition analyses were run to determine whether there were significant differences between young people with missing data for two or more follow-up occasions, compared to those with no missing data. Young people with partial data were more likely to attend a school with a lower ICSEA (SES) ranking (t (305) 2.134, p = 0.034). There were no differences between individuals with less and more complete data on baseline aggression (t (46.29) −1.407, p = 0.166), gender (t (337) 1.333, p = 0.183), impulsivity (t (73.87) −1.983, p = 0.062), hopelessness (t (78.53) −0.529, p = 0.599), anxiety sensitivity (t (70.96) −0.140, p = 0.889), or sensation seeking (t (77.61) 0.695, p = 0.489).
Multilevel modeling outcomes
Results from the final multilevel models are reported in Table 2. Findings show that Preventure had a significant effect on aggression over the 7-year period. Young people randomized to Preventure demonstrated a greater rate of decline in total aggression compared the control condition (−0.60 units every 6 months v. −0.18 units every 6 months, respectively) from baseline to 7-year follow-up (b = −0.42, confidence interval [CI] −0.638 to −0.196; p < 0.000). This is approaching a large effect size for the impact of the intervention across the 7-year period (d = −0.73). Separate analyses of the two forms of aggression revealed that Preventure had a significant impact on both proactive and reactive aggression. Young people in the Preventure group had a greater rate of decline in reactive aggression compared to the control condition (−0.35 units v.−0.13 units every 6 months, respectively) from baseline to 7-year follow-up (b = −0.22, CI −0.349 to −0.098; p = 0.000), with a moderate effect size (d = −0.66). In addition, the rate of change in proactive aggression was accelerated by receiving Preventure compared to control (−0.20 units v. −0.06 units every 6 months, respectively) from baseline to 7-year follow-up (b = −0.14, CI −0.229 to −0.051; p = 0.002). This equates to a moderate effect size for Preventure on proactive aggression (d = −0.49). All outcomes were consistent in direction with multiple imputation analysis, albeit with marginally smaller effect sizes (see the online Supplementary materials for more details).
Table 2. Preventure v. control outcomes for aggression: coefficients, effect sizes, and CIs from multilevel modeling linear change in aggressive behavior from baseline to 7-year follow-up
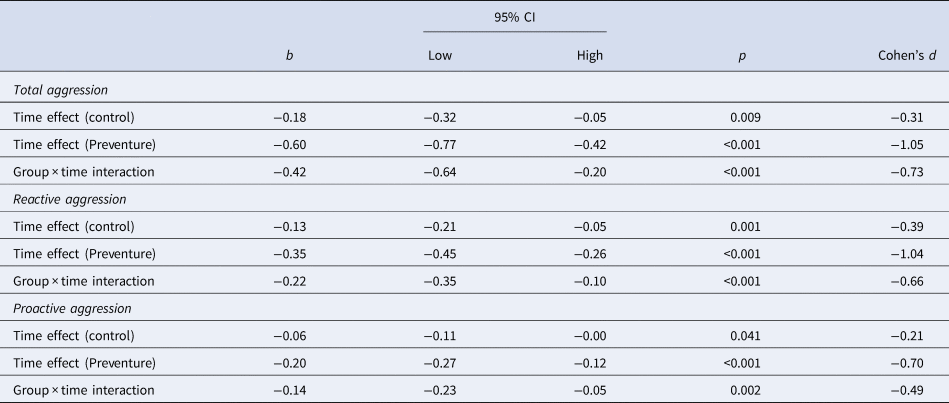
Notes: Cohen's d is the estimated effect size or standardized mean difference which was calculated based on the interaction between receiving Preventure v. control and time (baseline to 7 years). Schools = 9, young people with elevated risk (N = 339).
The pattern of data in the original analysis was robust in analyses with square root transformed data and a Poisson regression analysis. To explore whether the between group differences might be accounted for by higher baseline RPQ scores in the Preventure group, we calculated mean change from baseline follow-up within each decile of baseline RPQ scores. This indicated that the pattern of reducing RPQ scores over time was not driven by participants with extreme RPQ scores at baseline, and rather we saw a consistent pattern of reducing RPQ aggression scores over time in most of the decile groups. We applied the Mee–Chua test (Ostermann et al., Reference Ostermann, Willich and Lüdtke2008) which indicated that the reduction in aggressions scores observed in the Preventure group is likely to reflect true change and not attributable to regression to the mean.
Discussion
This research suggests that a school-based personality-targeted prevention program may be effective in reducing aggression over the long term. The analysis found that students who received the Preventure program demonstrated larger reductions in aggression over the 7-year follow-up period, from adolescence to young adulthood. Overall, all young people in the study showed reductions in aggressive behaviors over time; however, young people who received the Preventure intervention demonstrated accelerated declines in aggressive behaviors compared to those who did not receive the intervention. However, interpretation of these findings is limited by an imbalance in sex ratios across the two groups. Due to school-level randomization (i.e. whole schools were randomized to either the Preventure or control group) and varying gender balance between the trial schools, there was a significantly higher proportion of male young people in the Preventure group relative to control (86% v. 33%). As adolescent males tend to report higher rates of aggression compared to females (Smart et al., Reference Smart, Vassallo, Sanson, Richardson, Dussuyer, McKendry and Oberklaid2003), this imbalance may explain higher average baseline aggression scores at baseline and the greater declines in aggression for Preventure relative to control. Replication of this study in different samples of young people with balanced sex ratios will support external validity of the findings.
To our knowledge, this is the first study to have demonstrated lasting impacts of a school-based program on aggression from age 13 into young adulthood. This study contributes to the literature showing support for school-based programs in the prevention of aggression, carrying implications for future interventions and research (Cox et al., Reference Cox, Leung, Baksheev, Day, Toumbourou, Miller and Walker2016; Hahn et al., Reference Hahn, Fuqua-Whitley, Wethington, Lowy, Crosby, Fullilove and Price2007; Kovalenko et al., Reference Kovalenko, Abraham, Graham-Rowe, Levine and O'Dwyer2022). These results are robust against the impact of missing data and build on previous research findings that show Preventure has a positive impact on conduct problems at 3-year follow-up among Australian adolescents (Newton et al., Reference Newton, Stapinski, Teesson, Slade, Champion, Barrett and Conrod2020) and among adolescents involved in bullying (Kelly et al., Reference Kelly, Newton, Stapinski, Conrod, Barrett, Champion and Teesson2020).
The relatively large effect of Preventure on overall aggression (d = −0.73) is significant, as existing evidence for selective violence-prevention interventions is weak and there is limited evidence for school-based interventions in this area (Averdijk, Eisner, Luciano, Valdebenito, & Obsuth, Reference Averdijk, Eisner, Luciano, Valdebenito and Obsuth2020; Cox et al., Reference Cox, Leung, Baksheev, Day, Toumbourou, Miller and Walker2016). There was evidence of effectiveness for Preventure in reducing overall aggression, and both reactive and proactive aggression over time. There is overlap between reactive and proactive aggression subtypes; however, research suggests they are quite different in how they are preceded, associated, and driven (Hubbard et al., Reference Hubbard, McAuliffe, Morrow and Romano2010). Preventure appeared to have a stronger impact on reactive aggression compared to proactive aggression which may be explained by additional overlap for reactive aggression in the shared psychopathology with other risk dimensions targeted by the program (e.g. emotional distress) (Fite et al., Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010).
The benefits of the Preventure program for reducing proactive aggression are particularly noteworthy given these youth tend to be difficult to engage in treatment and evidence on what works with this population is lacking (Caldwell & Van Rybroek, Reference Caldwell and Van Rybroek2013). Proactive aggression is driven by a perception that aggressive behavior will lead to positive outcomes, so programs that target young people's reward systems may be more effective for these individuals because they respond less to costs and more to the benefits in perceived courses of action (Fite et al., Reference Fite, Hendrickson, Evans, Rubens, Johnson-Motoyama and Savage2014). It is possible that the Preventure focus on goal-setting and challenging cognitive distortions so as to increase the chances of achieving their goals was helpful for adolescents high in proactive aggression.
The effects of Preventure on aggression may be mediated (at least partially) by the effectiveness of Preventure on other risk factors, such as mental health (Newton et al., Reference Newton, Stapinski, Slade, Champion, Barrett, Chapman and Castellanos-Ryan2018), personality (Kelly et al., Reference Kelly, Grummitt, Birrell, Stapinski, Barrett, Boyle and Newton2021), and harmful alcohol use (Newton et al., Reference Newton, Conrod, Slade, Carragher, Champion, Barrett and Teesson2016). Symptoms of anxiety and depression are associated with reactive aggression among young people, and some young people drink alcohol to self-soothe or cope with distress related to their aggressive behavior which can lead to significant related and compounding consequences (Fite et al., Reference Fite, Raine, Stouthamer-Loeber, Loeber and Pardini2010; Øverup, DiBello, Brunson, Acitelli, & Neighbors, Reference Øverup, DiBello, Brunson, Acitelli and Neighbors2015). In Preventure, young people are guided through relevant personality-specific situations where they discuss and challenge cognitive and behavioral tendencies typical of key personality traits. Gaining insight into their maladaptive coping strategies and learning how to consider alternate thoughts and behaviors may lead to a reduced likelihood of reacting aggressively. It is beyond the scope of this study; however, future mediation analyses in larger samples would be beneficial to identify underlying mechanisms.
This study has some limitations to acknowledge. As discussed above, there was a significantly higher proportion of male young people in the Preventure intervention relative to control which limits the interpretability of these findings. The analysis models aim to account for this by modeling change from participant-specific starting points and controlling for gender as a covariate. Nevertheless, this potential bias should be considered when interpreting the results and future school-based trials should employ stratified randomization by school type (all male, all female, co-educational) to avoid any potential imbalance between groups. Given ethical restrictions precluded analysis of data for public schools, it would be important for this study to be replicated in schools with varying SESs. Future research should examine the mechanism through which Preventure is differentially effective for reactive and proactive aggression behavioral subtypes, and investigate potential underlying mechanisms such as reductions in hazardous alcohol use. Underreporting is a potential source of bias in all self-report studies. Lastly, the subsample analyzed was not powered to examine the effects of the intervention for each of the four personality traits on aggression. It would be worthwhile exploring which personality traits benefited most from Preventure in relation to aggression outcomes.
Notwithstanding these limitations, the inclusion of general aggression and subtypes of proactive and reactive aggression in young adulthood allows for a sensitive and developmentally appropriate exploration of the nature and severity of these risk behaviors in youth. The study is the first to assess the long-term impacts of a school-based brief intervention on aggression into adulthood and identify a prevention program that may effectively reduce aggression over a 7-year period. The analysis found that young people who received Preventure showed significantly greater reductions in total, reactive, and proactive aggression from baseline to 7-year follow-up compared to control, providing support for school-based prevention of maladaptive aggression. The effects of Preventure in reducing proactive aggression is of particular interest, given the multiplex challenges and costs associated with adult antisocial behavior that can ensue when this risk is not addressed early.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291724000989.
Acknowledgments
The authors acknowledge Julia Rosenfeld, Natasha Nair, and Lucie Swaffield for research assistance in the original CAP trial as well as the schools, students, and teachers who participated in this research. The research team also acknowledges the assistance of the NSW Department of Education and Communities for access to its schools (SERAP 2011201). Trial registration: This trial was prospectively registered in the Australian New Zealand Clinical Trials Registry (ACTRN12612000026820) on January 6th, 2012.
Funding statement
The study was funded through a project grant from the Australian National Health and Medical Research Council (NHMRC; App1124958), and an NHMRC Centre of Research Excellence grant (PREMISE; GNT1134909). A/Prof. Barrett has received support from an NHMRC Emerging Leadership Fellowship (GNT1195852). Prof. Teesson has received support from an NHMRC Principal Research Fellowship (GNT1041756; GNT1078407). Dr Champion has received support from an NHMRC Early Career Fellowship (GNT1120641). Prof. Newton has received support from an NHMRC Career Development Fellowship (APP1166377). A/Prof. Stapinski has received support from an NHMRC Translating Research into Practice Fellowship (GNT1132853). The NHMRC played no role in the study design, data collection, extraction, interpretation, or writing of this manuscript.
Competing interests
Dr Conrod reported ownership of the Preventure trademark, being the original developer of the Preventure program, and licensing the program to community organizations, which are offered on a fee for service basis by her research and knowledge dissemination team. All other authors declare no competing interests.
Ethical standards
Ethical approval was granted by the University of New South Wales Human Research Ethics Committee (HREC 2018/845), the University of Sydney (2018/845), the Sydney Catholic Education Office (Ref: 772), and the New South Wales Department of Education and Training (SERAP 2011201). The trial is registered with the Australian New Zealand Clinical Trials Registry (ACTRN12612000026820).






 Open access
Open access