


Personality disorder can significantly affect the management and outcome of associated mental illness (Reference Patience, McGuire and ScottPatience et al, 1995; Reference Yonkers, Dyck and WarshawYonkers et al, 2000). An assessment of personality status should therefore ideally form part of the routine assessments conducted by psychiatric teams (Reference Moran, Walsh and TyrerMoran et al, 2003; Reference Tyrer and SimmondsTyrer & Simmonds, 2003). However, too often the assessment of personality disorder remains one of clinical judgement. Unfortunately, clinical diagnoses are unreliable (Reference Mellsop, Varghese and JoshuaMellsop et al, 1982), and although reliability can be improved by the use of standardised assessments, these assessments are lengthy and require training. Self-report questionnaires are useful research tools, but they can be tiring for patients because they require the ability to concentrate on written questions. A brief structured interview with the patient would overcome some of these problems provided it could be easily incorporated into a standard psychiatric interview. This paper reports on the preliminary validation of a brief structured interview for personality disorders that is feasible for use in routine clinical assessment.
METHOD
Participants
A non-random sample of 60 adult patients was recruited from out-patient clinics (n=24), in-patient units (n=24) and day units (n=12) within the South London and Maudsley National Health Service (NHS) Trust. No special attempt was made to select patients with known or suspected personality disorder; however, the sample was chosen to represent patients with a range of psychiatric problems. Patients were also chosen on the basis that they were stable and cooperative with being interviewed. None of the patients was acutely unwell at the time of recruitment. Out-patients and day patients were recruited directly at the time of clinic or day hospital attendance, and in-patients were interviewed on the hospital ward. The sample consisted of 34 women and 26 men, with a mean age of 43 years (s.d.=15.9). The clinical diagnoses of the sample were as follows: affective disorder (n=25), anxiety disorder (n=11), eating disorder (n=9), schizophrenia (n=9) and drug or alcohol dependence (n=6).
Measures
Screening questionnaire
The screening questionnaire consisted of eight dichotomously rated items taken from the opening section of an informant-based interview, the Standardised Assessment of Personality (SAP) (Reference Mann, Jenkins and CuttingMann et al, 1981; Reference Pilgrim and MannPilgrim & Mann, 1990; Reference Pilgrim, Mellers and BoothbyPilgrim et al, 1993). The SAP allows an ICD–10 or DSM–IV diagnosis of personality disorder to be made (World Health Organization, 1992; American Psychiatric Association, 1994). Each of the eight questions from the opening section of the SAP corresponds to a descriptive statement about the person and can be scored 0 or 1 (see Appendix). The scores on the eight items can be added together to produce a total score between 0 and 8.
An exploratory analysis of the SAP ratings of a sample of 303 primary care attenders (Reference Moran, Rendu and JenkinsMoran et al, 2001; Reference Rendu, Moran and PatelRendu et al, 2002) showed that the total score on these eight official probe items satisfactorily predicted the final SAP diagnosis of personality disorder obtained after more detailed questioning of the informant: area under the curve (AUC)=0.79, 95% CI 0.74–0.84. The performance of these eight items suggested that they might also act as a patient-based screen for a diagnosis of personality disorder. However, the SAP is an informant-based interview and it was unclear how well the probe items would perform when given to patients as opposed to informants. The examination of the psychometric properties of the patient-based screen, the Standardised Assessment of Personality – Abbreviated Scale (SAPAS), formed the basis of this study.
SCID–II
The Structured Clinical Interview for DSM–IV Personality Disorders (SCID–II) (Reference First, Gibbon and SpitzerFirst et al, 1997) is a 119-item semi-structured interview with the patient. Each item is scored as 1 (absent), 2 (sub-threshold) or 3 (threshold). Questions may necessitate further exploration by the interviewer in order to score a particular item. If a threshold is reached on a sufficient number of items, the category of personality disorder is deemed to be present. The SCID–II was designed to generate DSM–III–R (American Psychiatric Association, 1987) diagnoses; however, by eliminating items for passive–aggressive and depressive personality disorders, it can be used to generate DSM–IV personality disorder diagnoses. The instrument demonstrates acceptable test–retest (k=0.68) and interrater reliability (k=0.71) and takes up to 1 h to administer.
Procedure
A member of the clinical team (either a doctor or a nurse) interviewed the patient with the SAPAS, as part of routine clinical work. Shortly afterwards, the patient was interviewed with the SCID–II by one of the authors (P.M.). The majority (83%, n=50) of SCID–II assessments were conducted blind to the results of the screening mini-interview. In the case of 10 patient interviews, no staff member was available to conduct the SAPAS and P.M. therefore conducted both interviews. Approximately 3 weeks later (mean interval 20 days, s.d.=10), each patient was re-interviewed by the same person using the SAPAS.
Analysis
Analyses were performed using STATA version 7 (StataCorp, 1999). The main aim of analysis was to identify an appropriate cut-off score on the SAPAS for predicting a SCID–II (DSM–IV) diagnosis of personality disorder. This was achieved by undertaking an AUC analysis. The performance of the SAPAS at different cut-off scores was assessed by reference to the sensitivity, specificity and predictive values of the screening interview. The internal consistency of the SAPAS was assessed by calculating Cronbach's a on the total score after omitting each item and also overall. The test–retest reliability of each item was estimated by calculating the k coefficient, and the overall reliability of the total score was estimated using Lin's concordance coefficient (Reference LinLin, 1989). Interrater reliability is not a major issue since the questions are largely self-explanatory and no interpretation is placed on responses.
RESULTS
A total of 33 out of 60 patients received a SCID–II diagnosis of personality disorder, giving an overall prevalence of 55% (95% CI 42–68). The mean number of personality disorder diagnoses among those with any personality disorder was 2.1 (s.d.=1.2). Table 1 shows the α and κ coefficients of each item from the SAPAS and overall reliability coefficients. This shows that there is a moderate degree of overall internal consistency (0.68). ‘Normally impulsive’ and ‘Generally a perfectionist’ are the items least consistent with the rest. The test–retest reliability is reasonable and individual κ values are also acceptable, although the values for ‘Normally impulsive’ and ‘Normally a worrier’ are less. ‘Normally impulsive’ would seem to be the least satisfactory item, taking both internal consistency and test–retest reliability into account.
Table 1 Internal consistency and test–retest reliability of the Standardised Assessment of Personality – Abbreviated Scale items. The alpha coefficient for the total score is 0.68 and Lin's concordance coefficient for the total score is 0.89

| Item | Alpha coefficient if item omitted | Kappa coefficient |
|---|---|---|
| Difficulty making and keeping friends | 0.59 | 0.81 |
| Usually a loner | 0.63 | 0.83 |
| Trusting others | 0.57 | 0.79 |
| Normally loses temper easily | 0.66 | 0.83 |
| Normally impulsive | 0.72 | 0.61 |
| Normally a worrier | 0.62 | 0.62 |
| Depends on others a lot | 0.68 | 0.82 |
| Generally a perfectionist | 0.70 | 0.73 |
To investigate the use of alternative cut-off scores on the SAPAS, a logistic regression was employed with the SAPAS total score as predictor and SCID–II diagnosis as dependent variable. This analysis produced an AUC of 0.94 (95% CI 0.88–0.99). To assess the sensitivity and specificity of the SAPAS for various cut-off scores, a sensitivity–specificity plot was obtained (Fig. 1). This indicates that a probability cut-off of 0.65 for a positive SCID diagnosis (equivalent to a total SAPAS score of between 3 and 4) has approximately equal sensitivity and specificity, with both around 0.8. The performance of the SAPAS at a range of cut-off scores is displayed in Table 2; this shows that a cut-off score of 3 or 4 correctly classified over 80% of the patients. Although both thresholds performed similarly, arguably the cut-off score of 3 offers the best balance of sensitivity (0.94) and specificity (0.85) and gives the maximum total of these two measures. When the ten non-blind assessments were excluded the AUC was 0.92 (95% CI 0.85–0.99), and at a cut-off of 3 the sensitivity was 92% and the specificity was 84%, indicating that the full sample had not been biased by the inclusion of these cases.
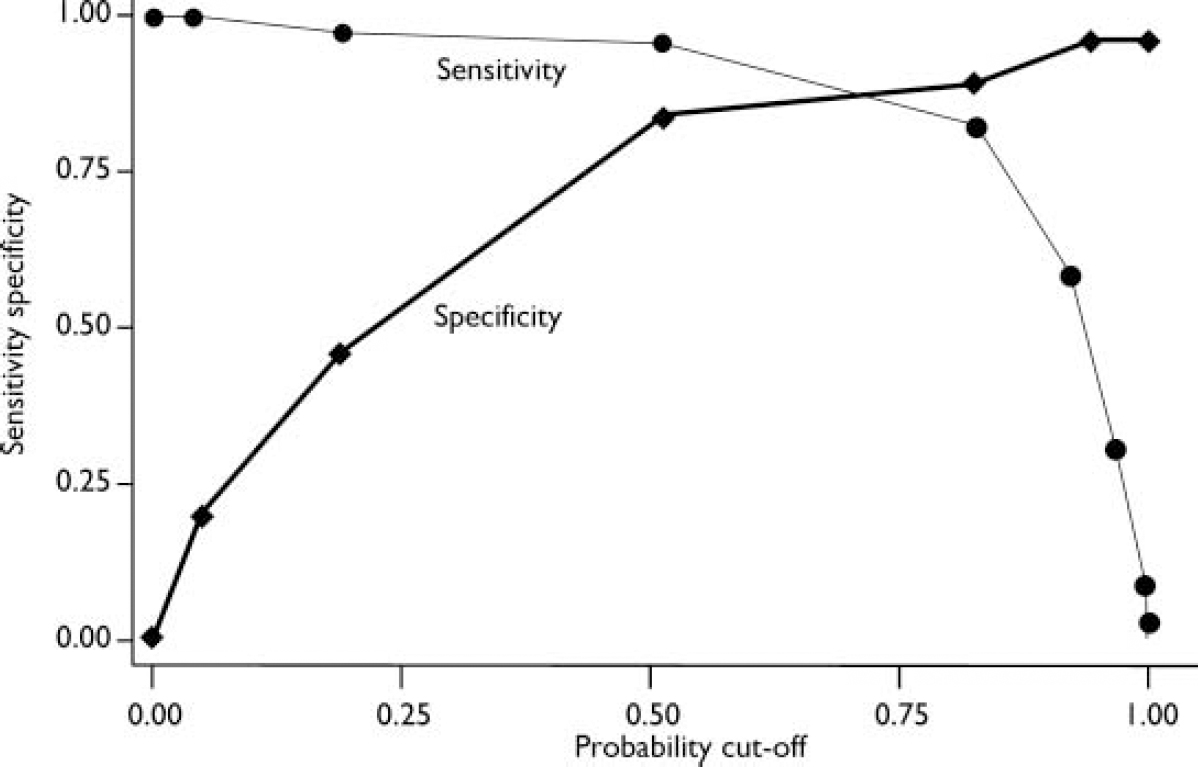
Fig. 1 Sensitivity–specificity plot relating Structured Clinical Interview for DSM–IV Personality Disorders positive diagnosis to total score on the Standardised Assessment of Personality – Abbreviated Scale.
Table 2 Sensitivity, specificity and power to predict personality disorder at different cut-off scores of the Standardised Assessment of Personality – Abbreviated Scale
| Cut-off score | Sensitivity | Specificity | Positive predictive value | Negative predictive value | Correctly classified (%) |
|---|---|---|---|---|---|
| 2 or more | 0.97 | 0.44 | 0.68 | 0.92 | 73 |
| 3 or more | 0.94 | 0.85 | 0.89 | 0.92 | 90 |
| 4 or more | 0.82 | 0.89 | 0.90 | 0.80 | 85 |
| 5 or more | 0.58 | 1.0 | 1.0 | 0.66 | 77 |
A scatter plot showing the positive predictive value of the screen at different cut-off scores of the SAPAS (Fig. 2) allows the effect of assuming various levels of population prevalence to be judged.
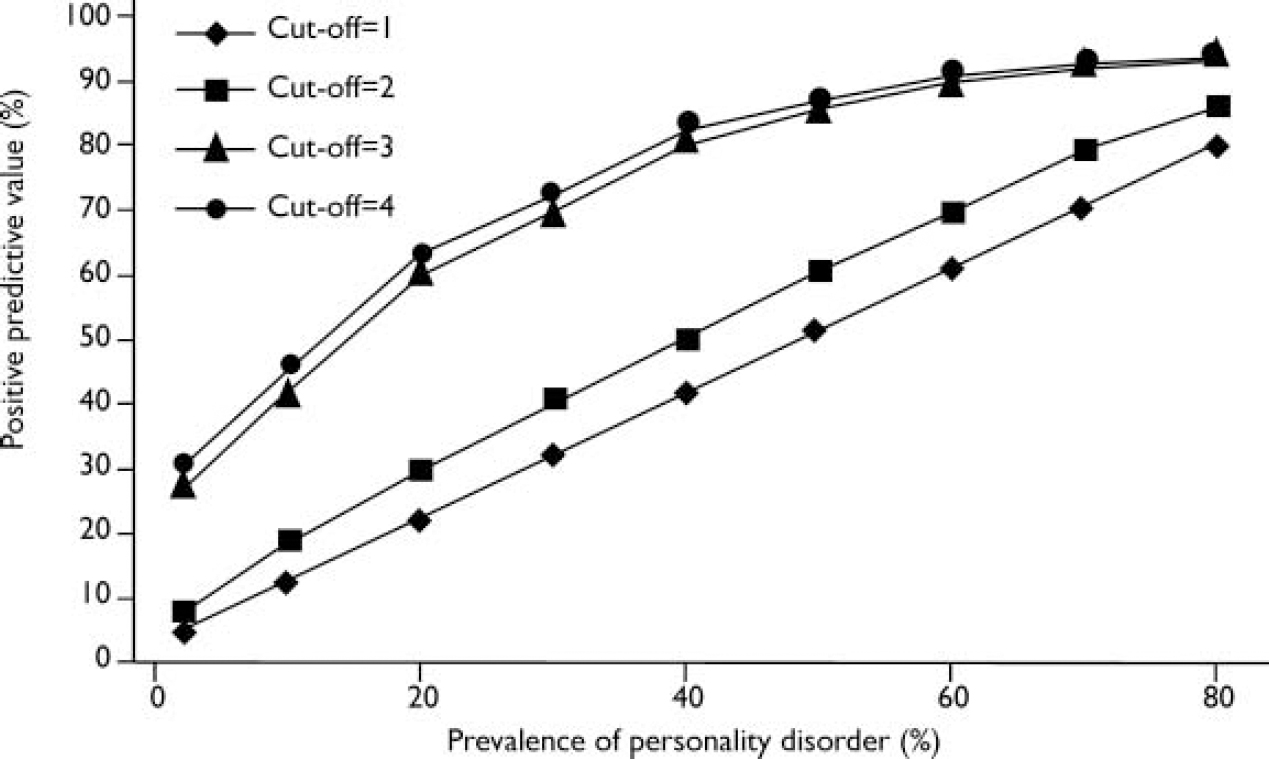
Fig. 2 Scatter plot showing the effect of prevalence of personality disorder on the positive predictive value of the Standardised Assessment of Personality – Abbreviated Scale.
DISCUSSION
Performance of the SAPAS
A score of 3 or 4 on the SAPAS correctly identified the presence of personality disorder in over 80% of participants. The study therefore provides preliminary evidence of the usefulness of the SAPAS as a screen for personality disorder in routine clinical settings. The findings should, however, be treated with caution, taking into account a number of limitations.
First, the study relied on a small, non-random sample of stable and cooperative patients with a high prevalence of personality disorder. Although the screen performed acceptably in this population, if it were to be applied to a population with a lower prevalence of personality disorder, its predictive power would diminish (Fig. 2). Consequently, the screen is probably not suitable for use in general community or primary care settings, where the prevalence of personality disorder is in the range 10–20%. Samuels et al (Reference Samuels, Eaton and Bienvenu2002) estimated that the prevalence of DSM–IV personality disorders in a community sample was 9%. Thus, from Fig. 2, based on this prevalence, the positive predictive power of the SAPAS in a community sample would be between 40% and 50%. In addition, although sensitivity and specificity are independent of the prevalence of a disorder in a population, measures may be more or less applicable to different populations. The findings therefore require replication in larger and more diverse populations of psychiatric patients.
Second, our choice of the SCID–II as the criterion for validation of the SAPAS may be questioned. However, the validity of the assessment measures for personality disorder has yet to be firmly established and none has been proved superior to any other (Reference ZimmermanZimmerman, 1994). The SCID–II was chosen as the gold standard because it has been widely used and its psychometric properties are well established (Reference ZimmermanZimmerman, 1994).
Third, we did not examine the ability of the SAPAS to discriminate between either sub-categories or clusters of personality disorder. In clinical practice, patients with personality disorders usually fulfil diagnostic criteria for more than one sub-category of disorder (Reference McGlashan, Grilo and SkodolMcGlashan et al, 2000) and it therefore makes little sense to screen for individual categories of personality disorder. In addition, the identification of sub-categories and clusters of personality disorder requires a more sophisticated diagnostic approach than that afforded by the SAPAS.
Comparison with existing screening methods for personality disorder
A number of self-report questionnaires are available for the purpose of screening for personality disorder. These include the International Personality Disorder Examination Screen (Reference Lenzenweger, Loranger and KorfineLenzenweger et al, 1997), the Personality Diagnostic Questionnaire–Revised (Reference Hyler, Skodol and OldhamHyler et al, 1992) and the SCID–II Screen (Reference Ekselius, Lindstrom and Von KnorringEkselius et al, 1994). Although these instruments are of some value to researchers interested in identifying ‘high-risk’ populations, when compared with a structured interview their specificity is invariably poor. In addition, they require the ability of the respondent to concentrate on a long set of questions.
To the best of our knowledge, only two other interviewer-administered screens for personality disorder have been published. Langbehn et al (Reference Langbehn, Pfohl and Reynolds1999) have developed the Iowa Personality Disorder Screen (IPDS) to provide a mini-structured interview that the authors estimate can be completed in 5 min. The IPDS consists of 11 questions that address general personality disorder criteria as well as specific criteria. The instrument has been validated against the Structured Interview for DSM–IV Personality Disorders (SIDP–IV) (Reference Pfohl, Blum and ZimmermanPfohl et al, 1997). The authors reported excellent sensitivity (92%) and good specificity (79%), although the validation was a somewhat circular exercise, as the IPDS items were derived from the DSM–III–R version of the SIDP. Van Horn et al (Reference Van Horn, Manley and Leddy2000) have developed a structured patient interview for personality disorders, the Rapid Personality Assessment Schedule (PAS–R). However, the PAS–R requires staff training and performs moderately well as a screen for personality disorder when compared with the full version of the PAS (sensitivity 64%, specificity 82%).
In this preliminary validation exercise, the SAPAS showed superior psychometric performance compared with both the IPDS and the PAS–R. In addition, the SAPAS is short (no interview took longer than 2 min to complete), does not require training, is simple to use, and was acceptable to the respondents in this study. It therefore fulfils many of the criteria for a desirable screening test (Reference Brewin, Rose and AndrewsBrewin et al, 2002).
Potential applications of the SAPAS
The SAPAS could be used to identify individuals who are at potentially high risk of having any type of personality disorder in a general adult psychiatric setting. The screen itself should not be used to make a diagnosis of personality disorder or cluster of personality disorders, and we would advise that a person scoring more than 3 on the SAPAS should be interviewed with a detailed structured assessment of personality. Clinicians and investigators might wish to adopt higher or lower thresholds, depending on the nature of the sample and the relative importance to them of sensitivity and specificity.
We think that the screen could have both clinical and epidemiological applications. It is feasible for use in busy clinical settings and could therefore be used to identify individuals in need of a more detailed personality assessment. Although the assessment of personality soon after presentation might result in inflated estimates of personality disorder, this is often the time when treatment decisions are made, and if personality assessments are to have useful treatment implications, arguably they should be made at an early stage (Reference ZimmermanZimmerman, 1994). From an epidemiological perspective, the SAPAS could be used as a first-stage screen as part of a two-stage procedure for case identification (Reference Lenzenweger, Loranger and KorfineLenzenweger et al, 1997; Reference Mann, Raven and PilgrimMann et al, 1999).
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ Personality disorder can be predicted effectively with an eight-item screening interview, the Standardised Assessment of Personality – Abbreviated Scale (SAPAS).
-
▪ A score of 3 on the screening interview correctly identified the presence of DSM–IV personality disorder in 90% of participants.
-
▪ The SAPAS is feasible for use in routine clinical settings, where it could be used to identify individuals at risk of personality disorder. It could also be used in epidemiological research as part part of a two-stage procedure for case identification.
LIMITATIONS
-
▪ The findings need to be replicated on larger samples of psychiatric patients.
-
▪ The findings need to be replicated in different samples of psychiatric patients.
-
▪ The SAPAS may not be suitable for use in populations where the prevalence of personality disorder is lower.
Acknowledgements
The research upon which this publication is based has been supported by funding from the NHS National Programme on Forensic Mental Health. However, the views expressed in this publication are those of the authors and not necessarily those of the Programme or the Department of Health. The authors thank the patients and staff who participated in this study.
APPENDIX
Standardised Assessment of Personality – Abbreviated Scale
Only circle Y (yes) (or N (no) in the case of question 3) if the patient thinks that the description applies most of the time and in most situations.
-
1. In general, do you have difficulty making and keeping friends?...................... Y/N
(yes=1, no=0)
-
2. Would you normally describe yourself as a loner?.............................. Y/N
(yes=1, no=0)
-
3. In general, do you trust other people?..... Y/N
(yes=0, no=1)
-
4. Do you normally lose your temper easily?.. Y/N.
(yes=1, no=0)
-
5. Are you normally an impulsive sort of person?............................. Y/N
(yes=1, no=0)
-
6. Are you normally a worrier?............. Y/N.
(yes=1, no=0)
-
7. In general, do you depend on others a lot?.. Y/N.
(yes=1, no=0)
-
8. In general, are you a perfectionist?........ Y/N.
(yes=1, no=0)





eLetters
No eLetters have been published for this article.