CLINICAL SCENARIO
A 63-year-old female patient presents with abdominal pain, vomiting, and abdominal distention. She has previously had a cholecystectomy and hysterectomy. She has had no prior similar episodes, and denies fever, hematemesis, or diarrhea. She takes no medications. Vital signs include blood pressure 123/61 mm Hg, heart rate 97, oral temperature 37.2°C, respiratory rate 18, oxygen saturation 97% on room air. Her abdomen is diffusely tender and distended.
KEY CLINICAL QUESTIONS
- 1.
What does the literature suggest are the most reliable history and physical examination findings for small bowel obstruction?
The classic clinical picture of small bowel obstruction (SBO) is a patient with abdominal pain, distension, nausea and vomiting, and per os (PO) intolerance. Unfortunately, few studies evaluate the reliability of history and examination for diagnosis of SBO.Reference Taylor and Lalani1 Early in the obstruction, patients can pass stool and gas and even experience diarrhea. These symptoms should not be used to exclude SBO.Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2 Literature suggests patient gender, nausea, abdominal guarding, prior episodes of similar pain, and severity and duration of pain do not increase the pretest probability of SBO. Elements in the history with the highest likelihood of SBO include prior abdominal surgery (+likelihood ratio [LR] 3.86) and history of constipation (+LR 8.8).Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2
Clinicians should evaluate for hemodynamic instability, fever, and peritonitis, which can occur in later stages of SBO and suggest intestinal strangulation or perforation.Reference Taylor and Lalani1–Reference Maung, Johnson and Piper3 Pain that is persistent or out of proportion to examination is concerning for strangulation and perforation.Reference Long, Koyfman and Gottlieb2,Reference Maung, Johnson and Piper3 Examination findings most suggestive of SBO include abdominal distension (+LR 5.64–16.8 and -LR 0.34–0.43).Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2 Generalized tenderness has poor sensitivity for SBO. While abnormal bowel sounds may be suggestive of SBO (+LR 6.33), inter-observer agreement is poor, and they should not be used to exclude SBO.Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2 Evaluation for hernia is also recommended, as hernia is the second most common cause of SBO after intra-abdominal adhesions.
- 2.
Can ultrasound be used at the bedside to diagnose SBO?
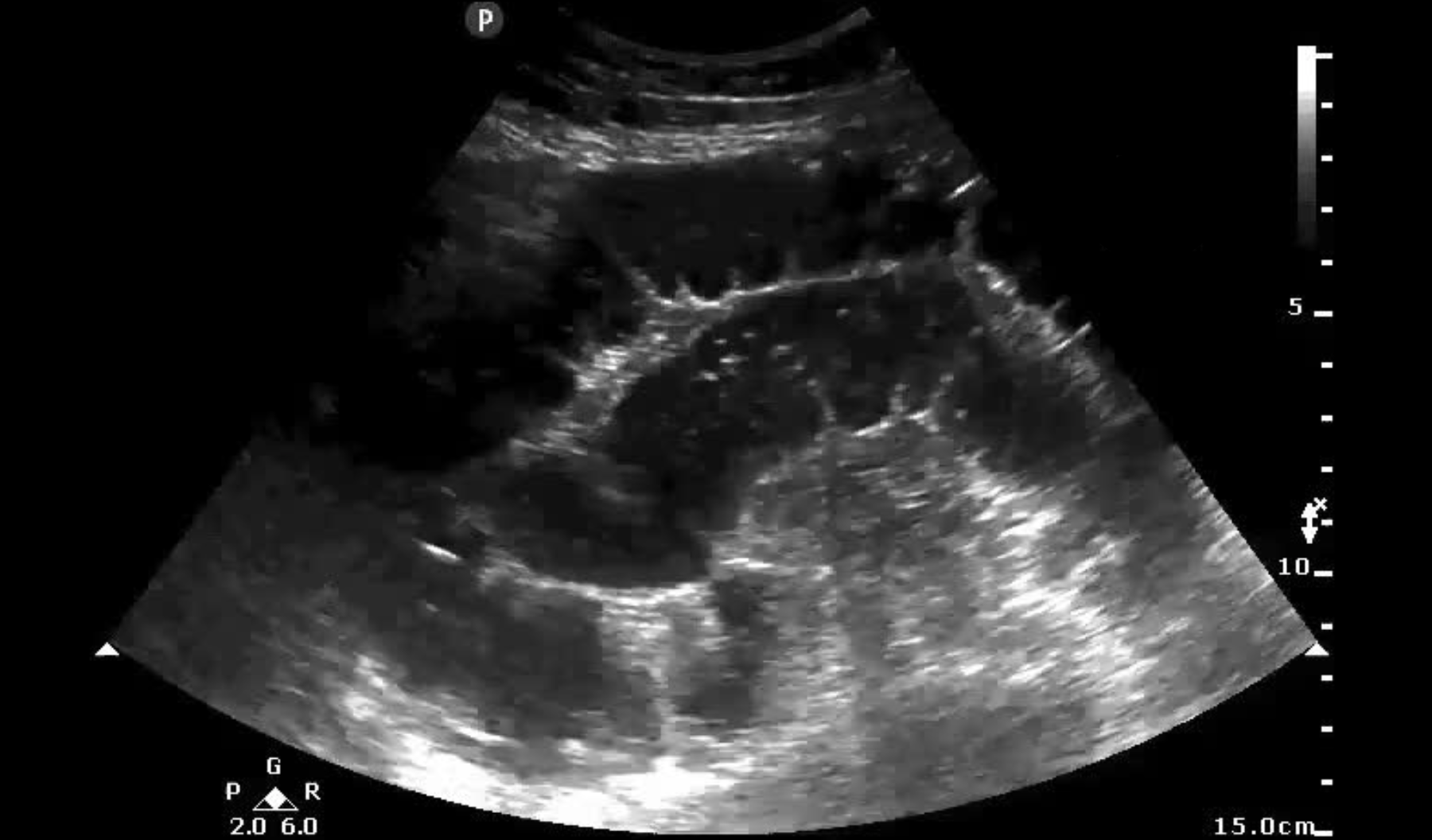
Ultrasound (US) is a rapid and reliable test for SBO. Fluid filled loops of bowel (> 2.5 cm in the jejunum or 1.5 cm in the ileum in three or more loops of bowel), ineffective peristalsis with whirling movements, and collapsed colonic lumen distal to a transition point are findings consistent with SBO (online Supplemental File).Reference Taylor and Lalani1–4 Sensitivity of US for diagnosis of SBO is over 94%, with a -LR of 0.04. Specificity ranges from 81–100%, with a + LR of 9.55 for emergency department (ED) point-of-care US (POCUS).Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2 Trained providers can incorporate US into their assessment for SBO and expedite care and reduce patient length of stay.Reference Long, Koyfman and Gottlieb2 If SBO is present based on US, further testing may be unnecessary, particularly in centers without access to advanced imaging such as computed tomography (CT).
To perform POCUS for SBO, the curvilinear probe with sequential, graded compression is recommended, beginning in the lower right quadrant. The probe is then moved longitudinally back and forth, evaluating for dilated and collapsed loops of bowel. Large bowel has visible haustra, while the jejunum possesses valvulae conniventes on the interior part of the intestinal wall. SBO involving the jejunum may result in the keyboard sign as a result of valvulae conniventes floating within fluid, similar to the black and white keys on a piano. The ileum does not have haustra or valvulae conniventes (Supplemental Figure). Free fluid, mural gas, and bowel wall edema (> 2 mm thickness) are associated with ischemia and worse prognosis.Reference Taylor and Lalani1,Reference Long, Koyfman and Gottlieb2
- 3.
What diagnostic modalities are most reliable?
While US is reliable, several other imaging modalities are available, including plain radiograph, CT, and magnetic resonance imaging (MRI). Plain radiographs are widely available and can be used to follow disease progression.Reference Taylor and Lalani1,Reference Maung, Johnson and Piper3,4 Findings of SBO on plain radiograph include dilated loops proximal to the obstruction (> 3 cm for the small bowel), visible valvulae conniventes, predominantly central dilated loops of bowel, and horizontal or oblique air fluid levels in the abdomen. However, radiographs cannot be used to exclude SBO, as sensitivity ranges from 59 to 85%, and they are normal in 20–30% of cases.Reference Taylor and Lalani1–4 CT with intravenous (IV) contrast is the imaging modality of choice and diagnostic with dilated small intestine proximal to a transition point with distal collapsed bowel.Reference Taylor and Lalani1–4 Current generation CT (third generation or greater) with IV contrast demonstrates a sensitivity over 93% for diagnosis of SBO, with a specificity over 96%.Reference Taylor and Lalani1 PO contrast limits evaluation for ischemia and does not improve the diagnostic accuracy of CT.4 MRI has similar test characteristics compared with CT, but it is the least feasible test in the ED setting.Reference Long, Koyfman and Gottlieb2–4 It is recommended for pregnant patients, but without gadolinium contrast.
- 4.
Should all patients with SBO have an nasogastric tube placed?
The patient should be nil PO (NPO), as oral intake will increase proximal intestinal content and intraluminal pressures.Reference Maung, Johnson and Piper3 Nasogastric (NG) tube placement was previously considered integral. Except in certain situations, routine placement is no longer recommended, as NG tube placement is not associated with reduction in bowel ischemia, need for operative therapy, complication rates, or length of stay.Reference Long, Koyfman and Gottlieb2,Reference Fonseca, Schuster, Maung, Kaplan and Davis5 Patients with severe abdominal distension, pain, and vomiting may benefit from decompression with NG tube, but evidence to support this recommendation is limited.Reference Long, Koyfman and Gottlieb2 NG tube placement should also be considered in the patient requiring transport for further management of SBO.
- 5.
When should the surgeon be involved, and what are the indications for operative therapy?
While many patients with partial and even complete obstruction will improve with fluid resuscitation and symptomatic therapy, consultation with surgery is recommended for patients with SBO. Surgical service admission is associated with lower mortality rates and shorter lengths of stay compared with medical service admission.Reference Long, Koyfman and Gottlieb2,Reference Maung, Johnson and Piper3 Patients with hemodynamic instability, fever, peritonitis, perforation or strangulation on imaging, or closed loop SBO or internal hernia should go to the operating room (OR).Reference Long, Koyfman and Gottlieb2,Reference Maung, Johnson and Piper3 Patients who do not improve symptomatically after 3 days should be considered for operative therapy.Reference Maung, Johnson and Piper3 
SUMMARY/CONCLUSIONS
Clinicians should evaluate for hemodynamic instability, prior abdominal surgery, constipation, and abdominal distension in patients with suspected SBO. US and CT are reliable imaging modalities. Management includes symptomatic therapy, fluid rehydration, and determination of the need for operative therapy. NG tubes should not be routinely placed for SBO. Admission to a surgical service is associated with improved patient outcomes.
CASE RESOLUTION
The emergency clinician provides analgesics and antiemetics, as well as 1 L of normal saline. CT with IV contrast demonstrates a complete obstruction with transition point in the ileum. The patient does not have peritonitis or hemodynamical instability. The surgeon agrees to admit the patient.
Supplemental material
The supplemental material for this article can be found at https://doi.org/10.1017/cem.2020.393.
Competing interests
None declared.