INTRODUCTION
Healthcare costs are on the rise in Canada, and the sustainability of our healthcare system is at risk. Healthcare in Canada is delivered through a group of publically funded health insurance plans that provide all Canadian citizens with universal coverage. Funding is administered by individual provinces and territories based on guidelines set by the federal government. Over the last 15 years, total federal healthcare expenditures have more than doubled from just under $100 billion in 2001 to $215 billion in 2014. 1 The Canadian Society of Actuaries suggested that at current growth rates 97% of total revenues available to Canadian provinces and territories would be spent on healthcare by 2037, compared to 44% in 2012. 2 As the Canadian population ages, a growing number of patients are seeking immediate and unscheduled medical care through our emergency departments (EDs). The ED is an expensive alternative to other forms of primary care, and Canadians are among the most frequent users of EDs worldwide. 3 - 5 Given these trends, physicians and hospital administrators must identify innovative and cost-efficient approaches to healthcare delivery.
Previous studies have discussed system-level changes to help control costs, but physician-level solutions have not been well-explored. As gatekeepers to patient care, ED physicians have a significant and direct influence on the cost of healthcare.Reference Taheri, Butz, Griffes, Morlock and Greenfield 6 However, the Canadian healthcare system is not designed to encourage physicians to manage resources and costs. A curriculum review of Canadian medical schools reveals no formal training on healthcare costs. Several studies in the United States, Israel, and Sweden have shown that physicians respond to increased cost awareness by significantly reducing the number of investigations ordered, which results in significant cost savings.Reference Nougon, Muschart and Gerard 7 - Reference Agarwal, Agarwal, Mazurkiewicz, Wecht and Friedlander 12 In over a decade, there have been no Canadian studies evaluating ED physician cost awareness across the four main categories of day-to-day ordering: imaging investigations, materials, laboratory tests, and pharmaceuticals. Older Canadian studies demonstrate poor cost awareness among ED physicians.Reference Allan, Lexchin and Wiebe 13 - Reference Allan and Lexchin 15 More recent studies from the United States show a similar trend.Reference Vijayasarathi, Duszak, Gelbard and Mullins 16 The recent advent of electronic medical systems can allow for access to cost information at the point of care, which could be used to facilitate cost-conscious clinical decision making.Reference DeMarco, Paul and Kilpatrick 17 , Reference Schilling 18 A recent study of residents at an academic hospital in the United States demonstrated that by incorporating cost information into electronic medical records, residents were more likely to estimate the costs of laboratory tests correctly.Reference Long, Bongiovanni and Dashevsky 19 With a growing number of high-cost diagnostic tools and pharmaceutical options at the disposal of ED physicians,Reference Lysdahl and Hofmann 20 , Reference Kinch, Haynesworth, Kinch, Kinch and Hoyer 21 differences in cost could become an important consideration when choosing between similar options. Given the demonstrated deficits in physician awareness of healthcare costs in prior studies, we aim to characterize current levels of cost awareness among ED physicians at our center. By understanding the current level of physician cost awareness, we hope to identify areas where cost education would provide the greatest benefit in reducing ordering costs at our hospital and indirectly reduce costs to the healthcare system.
METHODS
Study design and setting
We conducted a cross-sectional survey evaluating current awareness of common ordering costs among ED physicians—both department staff and emergency medicine residents—from two campuses of a tertiary-care teaching hospital in Ottawa, Ontario. The two EDs have an annual patient census of 150,000 visits and serve as regional centres for cardiac care, trauma, stroke, and cancer.
Study population
Our survey population was made up of 124 certified emergency medicine staff physicians and emergency medicine resident physicians. Approval from The Ottawa Hospital (TOH) Research Institute Ethics Board was obtained (protocol no. 20140871).
Data collection
We considered ED costs as subdivided into four categories: imaging investigations, materials, laboratory tests, and pharmaceuticals. Cost information for items in these categories was collected from the finance and performance measurement departments at TOH. Costs are reported in 2014 Canadian dollars. For the purposes of the present study, actual costs were defined as “total direct costs” to TOH. “Total direct” costs included “fixed” costs (e.g., overhead, technician salary) and “direct variable” costs (e.g., reagents). They did not include any “indirect” costs (e.g., administration) or physician billings (e.g., radiologist interpretation). Laboratory tests and pharmaceuticals did not include collection materials (e.g., test tubes) or medication delivery materials (e.g., needles).
A total of 41 items across each of the four categories (imaging investigations, materials, laboratory tests, and pharmaceuticals) were selected for the survey based on high frequency of use, availability of cost-effective alternatives, and tests considered to be “low-yield.” The survey was created using Survey Monkey’s online platform and distributed via email to ED staff physicians and resident physicians by the chief of the department. Three reminder emails were sent over a two-month period. Participants were asked to estimate the cost of the 41 items and input their estimates using “free-text” fields that allow entry of values precise to the cent. An explanation of “total direct costs” was provided for each category. Participants were asked not to include indirect costs or physician billings. The survey could be exited at any time, but questions could not be skipped, and the data were only collected once participants submitted a fully completed survey.
Outcome measures
The primary outcome was percentage of correct estimates, underestimates, and overestimates of cost across the four categories of day-to-day ordering among ED physicians. Correct estimates are defined as estimates within 25% above or 25% below actual cost, overestimates are defined as estimates greater than 25% above the upper limit of actual cost, and underestimates are defined as estimates more than 25% below the lower limit of the actual cost. Specifically, we were interested in the percentages of correct estimates, underestimates, and overestimates of the cost of items with cost-effective alternatives and low-yield tests.
Analysis
The percentage of underestimates, correct estimates, and overestimates was reported for each item. Data were analyzed using descriptive analyses as appropriate for the type of data. Data analysis was performed using SAS and Microsoft Excel®.
RESULTS
The survey was distributed to 124 ED staff physicians and resident physicians by email. Our response rate was 58%. Of the 72 ED physicians who responded to the survey, 43 were ED staff physicians and 29 were ED resident physicians. The participants provided 2,952 cost estimates for 41 items. Participating physicians answered each survey question, and no data were missing (a completion rate of 100%).
There was no significant difference in correct estimates between ED staff and ED residents (p=0.64) or between staff with ≤5 years of experience and staff with >5 years of experience (p=0.23).
Table 1 describes the survey participant demographics and the percentage of participants who answered “yes,” “likely,” “unsure,” “unlikely,” or “no” to the question “Would better access to cost information impact your practice?” The majority of participants (67%) answered “likely” or “yes,” and no participants (0%) answered “no.”
Table 1 Survey participant demographics
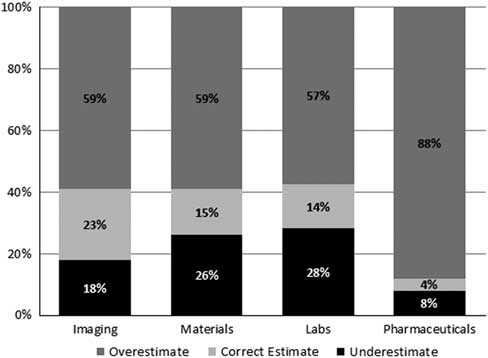
Figure 1 provides an overview of the percentage of correct estimates, overestimates, and underestimates for each of the four categories. The percentage of correct cost estimates among ED physicians did not exceed 25% in any of the four categories. The pharmaceuticals category was the most overestimated at 88% and was also the least accurate, with 4% accurately estimated costs.
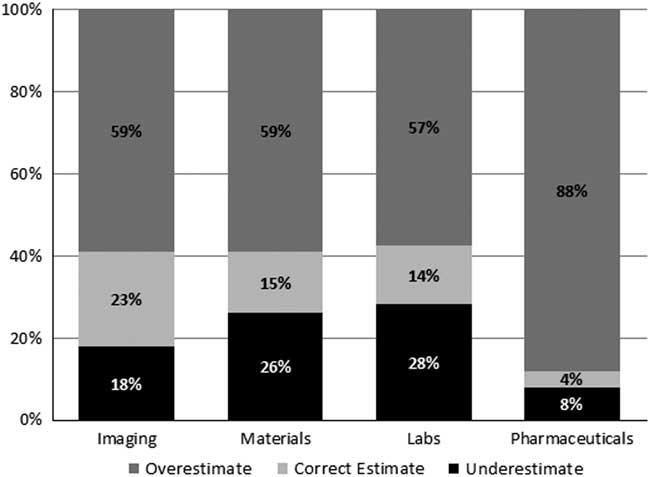
Figure 1 Percentages of ED physician under-, correct, and overestimates for cost across the four categories surveyed.
Table 2 provides actual cost information as well as the median, range, and interquartile range (IQR) for ED physician cost estimates and the percentage of correct estimates for each item surveyed. There were some notably high overestimates among these items—for example, a CT head without contrast was estimated to cost $1,500 (3,276% higher than the actual price). Notably low estimates were also seen—for example, an ipratropium inhaler was estimated to cost $0.05 (37,840% lower than the actual price).
Table 2 Proportion of physician underestimates, correct estimates, and overestimates
* The percentage of physicians who provided a correct estimates, where correct estimates are defined as within 25% above or 25% below actual cost, overestimates are defined as greater than 25% upper limit of actual cost, and underestimates are defined as less than 25% lower limit of actual cost.
CBC=complete blood count; CHEM–7=includes: sodium, potassium, chloride, bicarbonate, blood urea nitrogen, creatinine, glucose; CT=computed tomography; IM=intramuscular; Inh=inhaler; IQR=interquartile range; IV=intravenous; MRI=magnetic resonance imaging; PO=by mouth; R&M=routine and microscopy; U/S=ultrasound.
Table 3 highlights cost-effective alternatives. It outlines the absolute and relative cost differences between comparable items.
Table 3 Absolute and relative cost difference between comparable items

IM=intramuscular; Inh=inhaler; IV=intravenous; LP=lumbar puncture.
Figure 2 shows a breakdown of correct estimates, overestimates, and underestimates for each item in the imaging category. The cost of most imaging items was overestimated by ED physicians, but the cost of “X-ray: abdomen/KUB” and “X-ray: lumbosacral spine” were notably underestimated.
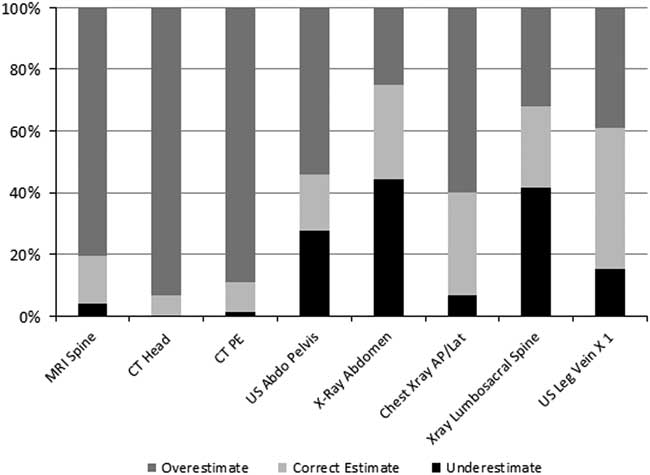
Figure 2 Percentages of ED physician under-, correct, and overestimates for cost of various imaging investigations.
Figure 3 shows a breakdown of correct estimates, overestimates, and underestimates for each item in the materials category. Of note, 56% underestimated the cost of topical skin adhesive, while over 47% underestimated the cost of cervical spine collars.
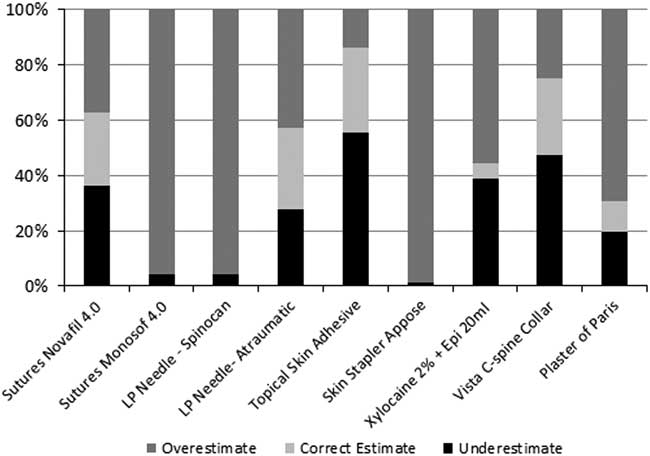
Figure 3 Percentages of ED physician under-, correct, and overestimates for cost of various materials.
Figure 4 shows a breakdown of correct estimates, overestimates, and underestimates for each item in the laboratory tests category. The costs of the CBC and differential, CHEM-7, INR, PTT, and urine culture were underestimated by a large percentage of physicians compared to other tests in this category.
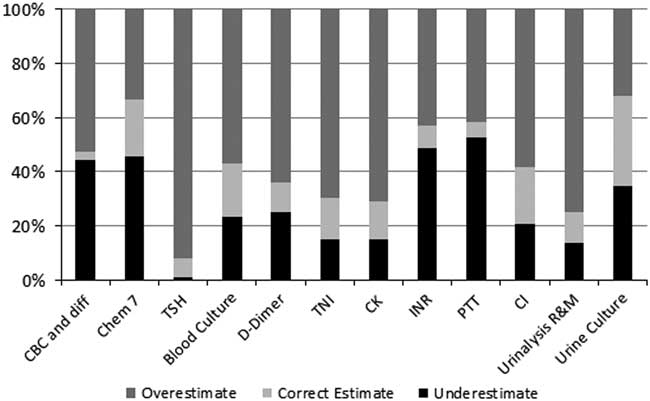
Figure 4 Percentages of ED physician under-, correct, and overestimates for cost of various laboratory tests.
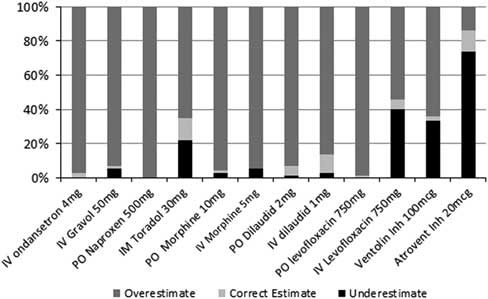
Figure 5 shows a breakdown of correct estimates, overestimates, and underestimates for each item in the pharmaceuticals category. As mentioned, ED physicians grossly overestimated the cost of most items. Exceptions included IV levofloxacin, salbutamol, and ipratropium, where a large percentage of physicians underestimated the cost. Some 99% of ED physicians overestimated the cost of PO levofloxacin, and none underestimated its cost. Similarly, 22% of cost estimates for IM ketorolac were underestimates, while 100% of estimates for the cost of PO naproxen were overestimates.
Figures 6–9 depict the range of physician cost estimates compared to the actual cost for each item across all four ordering categories. These figures highlight the large range of physician to physician cost estimates.
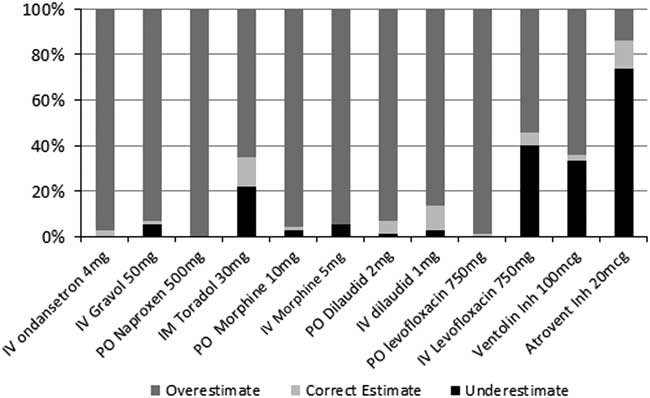
Figure 5 Percentages of ED physician under-, correct, and overestimates for cost of various pharmaceuticals.
DISCUSSION
Interpretation of results
We discovered that ED physicians at our two tertiary-care teaching hospitals in Ottawa had limited cost awareness with regard to imaging investigations, materials, laboratory tests, and pharmaceuticals. Among the four categories surveyed, imaging investigation costs had the greatest number of correct cost estimates, but also the greatest range of cost estimates. Pharmaceuticals had the smallest percentage of correct cost estimates.
Most ED physicians in our study overestimated costs across all four categories. As with most industries, cost overestimation has been shown to decrease utilisation of resources in healthcare.Reference Long, Cummings and Frisof 22 Thus, greater cost awareness in the setting of physicians who tend to overestimate cost could create an unintended increase in resource utilisation across all four categories. However, we believe that the overestimation seen in our results could be attributed to selective perception and impact biases. By conducting a survey of hospital costs, the participants’ perceptions of our hypothesis might be that physicians undervalue the healthcare costs. This creates a “selective perception bias” whereby the expectation that physicians undervalue healthcare costs changes the participant’s perception, leading to an overcorrection of cost estimates. An “impact bias” could also contribute to these survey findings; participants are biased toward overestimating cost because that is the more acceptable alternative to undervaluing cost, which is regarded as being less resource-conscious.
Previous studies
Overall, our findings are in keeping with previous studies,Reference Allan, Lexchin and Wiebe 13 , Reference Allan and Innes 14 , Reference Innes, Grafstein and McGrogan 23 suggesting that physicians continue to lack cost awareness of the care they provide. Only 14% of all cost estimates across the four categories were considered correct, which is lower than expected compared to similar studies. Innes et al.Reference Innes, Grafstein and McGrogan 23 also considered estimates within 20 or 25% of the actual cost to be “good knowledge” and reported 25–47% of ED physician cost estimates to be correct. The low percentage of correct cost estimates found in our study may be reflective of the rising number of available and advanced imaging investigations, materials, laboratory tests, and pharmaceuticals available to ED physicians.
STRENGTHS
Our study provides an updated analysis of ED physician awareness of the common ordering costs of all major ED cost categories across two tertiary-care teaching hospitals. It is the first study to investigate cost awareness across the four main categories of day-to-day ordering and the first to evaluate ED physician cost awareness of cost-effective alternatives.
LIMITATIONS
The generalizability of our study results is limited given the modest sample size of academic emergency staff and residents and the 58% response rate. While the costs were specific to our urban hospital network, the large variance in physician cost estimates at our centre would support the need for increased cost awareness irrespective of actual costs at other centers.
In addition, total direct costs were used to represent “actual costs” in our study. This excludes indirect costs associated with each item, which significantly underestimates the true total cost. However, by removing indirect costs from our study, respondents were able to estimate a more tangible component of cost, and our finance department was able to provide a more accurate figure for the cost of each item. While there is no guarantee that participants did not research pricing information while responding to the survey, this information is difficult to obtain. Prices are unique to our hospital, with no such data available publically or internally without formal written requests. Finally, as mentioned in our interpretation of the results, the data were subject to selection perception and impact biases, which potentially resulted in overestimation of costs.
CLINICAL IMPLICATIONS
Our study highlights two areas where cost education programs might influence ordering behaviour: 1) items with cost-effective alternatives and 2) low-yield tests. Both are areas in which improved cost education with regard to only a few items may influence ordering habits on a large scale, which could result in significant cost savings without impacting patient care.
Where comparable items exist (see Table 3), ED physicians tended to overestimate the cost of the more cost-effective alternative. For example, levofloxacin, a commonly used antibiotic, has near identical bioavailability through the PO route compared to IV.Reference Cyriac and James 24 The perceived cost of the IV formulation of levofloxacin was largely underestimated compared to the equivalent PO dose, which was significantly overestimated. The absolute cost reduction for the equivalent dosing was $13.25 per dose. Similarly, the more cost-effective PO route for morphine and hydromorphone were overestimated to a greater degree than their equivalent IV dose. The absolute cost reduction for a single PO versus IV dose was $0.53 for morphine and $0.67 for hydromorphone. When comparing naproxen and ketorolac, two common nonsteroidal anti-inflammatory drugs (NSAIDs), our study demonstrated a relative overestimation of the inexpensive naproxen compared to ketorolac. The absolute cost reduction for equivalent dosing was $3.44 per dose. Studies have demonstrated no significant difference between the two NSAIDs.Reference Wright, Price and Watson 25 These findings highlight an area where cost education can assist physicians in choosing the cost-effective alternative from among the clinically equivalent options.
Several items in the survey were selected for their increased ordering frequency, as well as for their low-yield diagnostic utility. Interestingly, ED physicians underestimated the cost of some of these items. For example, lumbosacral X-rays are frequently ordered in the ED, yet their diagnostic utility in the majority of patient presentations is poor.Reference Chou, Qaseem and Snow 26 Coagulation screens ordered in adults often include partial thromboplastin time (PTT), which, despite limited diagnostic value outside of heparinized patients or those with known bleeding disorders, are routinely performed with prothrombin times (PTs). Urine microscopies are often used to screen for urine infections. A negative urine microscopy is unlikely to yield a positive urine culture; however, urine cultures are commonly ordered in conjunction with the initial urine microscopy. If physicians delayed ordering urine cultures unless a urine microscopy was positive, an absolute cost reduction of $16.77 per test would be realized for each negative urine microscopy. Increasing physician awareness of the costs of these three low-yield investigations could prove to be an important area of waste reduction. Taken together, these findings suggest that those accountable for ED spending and utilization should perform their own practice and cost review and educate their physicians on areas where the greatest impact to cost savings can be achieved.
RESEARCH IMPLICATIONS
Developing and evaluating cost-awareness education programs may be an effective way to mitigate the rise of healthcare costs in Canada. Further studies that characterize utilization of hospital resources based on ED physician awareness of cost-effective alternatives and the cost of “low-yield” tests would help better characterize the need for educational intervention. Studies that evaluate cost utility and resource utilization at other centres across Canada are also warranted.
CONCLUSIONS
Canadian ED physicians demonstrated limited awareness of common healthcare costs used in day-to-day practice. Our study identifies two areas where cost education programs might influence ordering behaviour: 1) items with cost-effective alternatives and 2) low-yield tests. ED physicians tended to greatly overestimate the cost of the less-expensive option among items with comparable alternatives and underestimated the cost of low-yield testing modalities. Overall, this study highlights the need for cost-awareness education programs and better access to cost information that would equip physicians to manage cost and hospital resources more effectively.
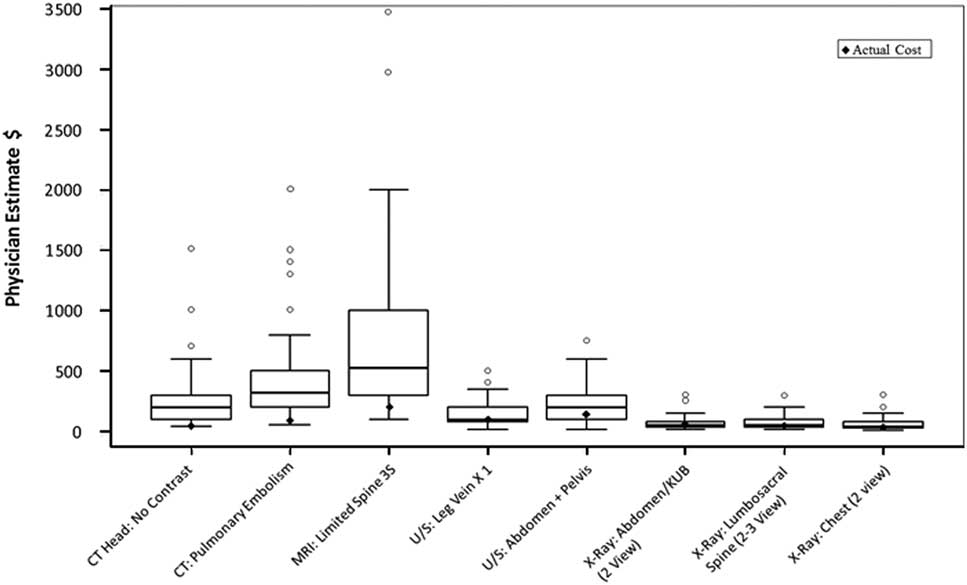
Figure 6 ED physician cost estimates of various imaging investigations.
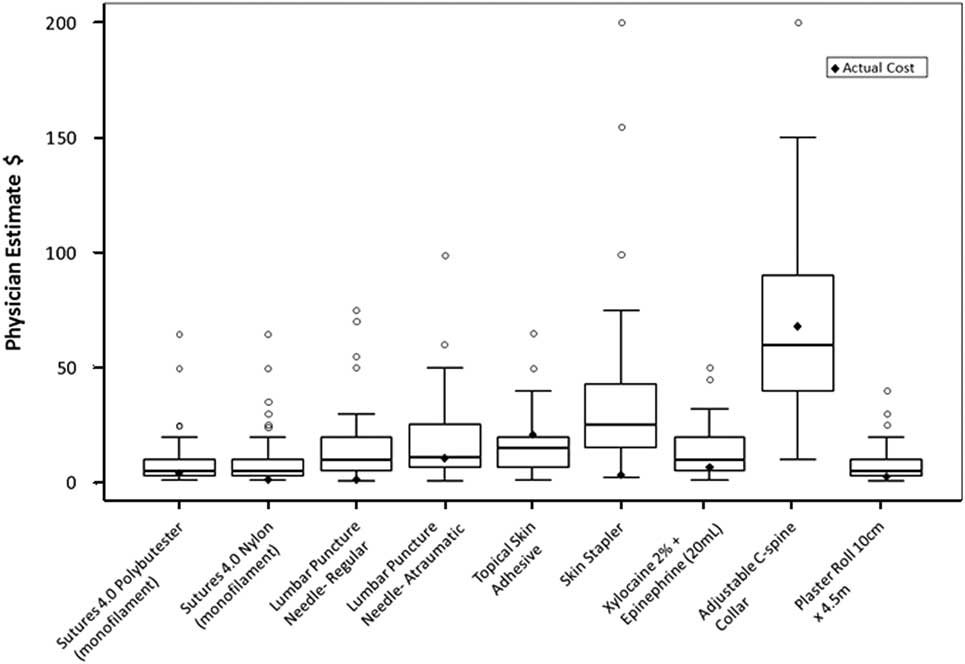
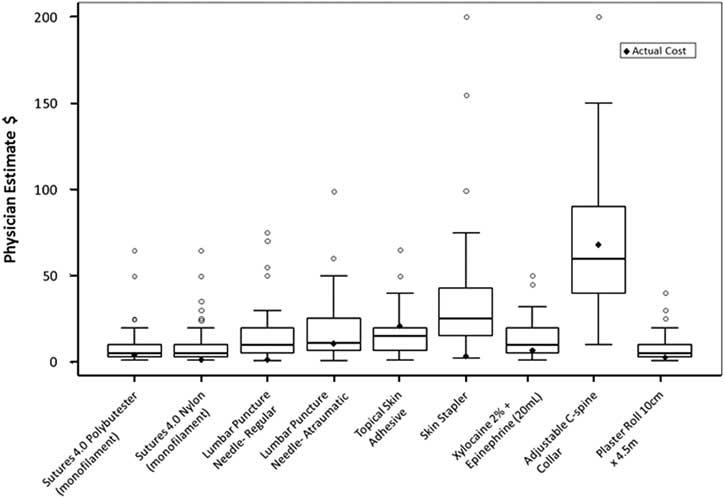
Figure 7 ED physician cost estimates of various materials.
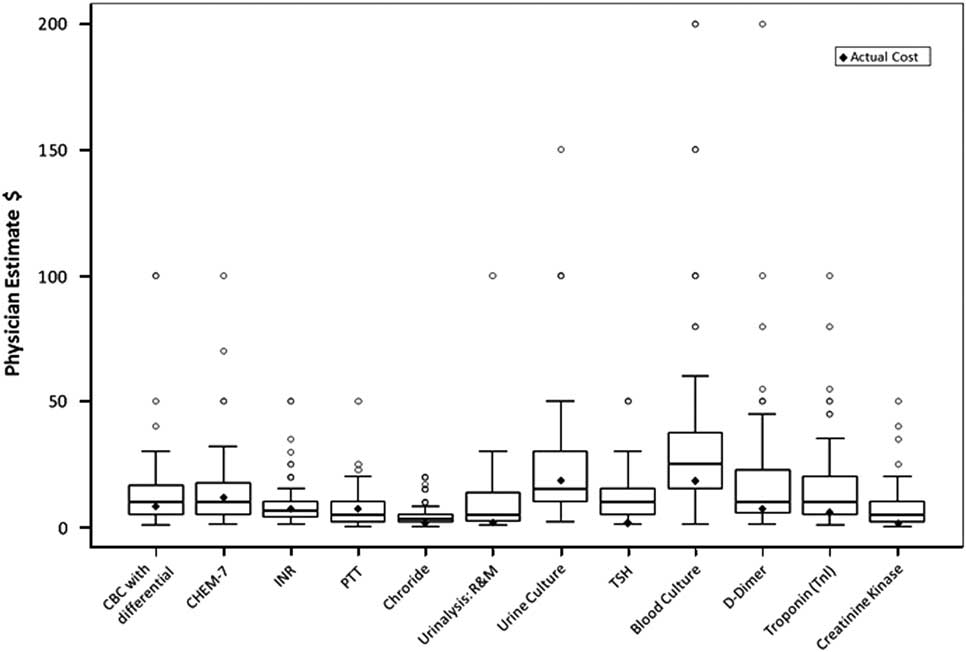
Figure 8 ED physician cost estimates of various laboratory tests.
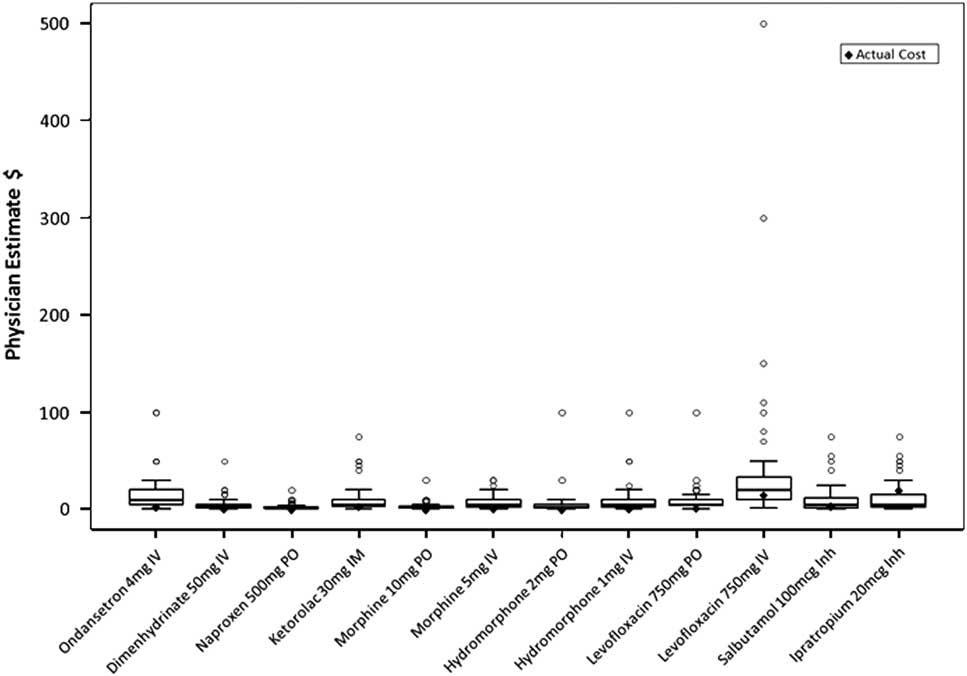
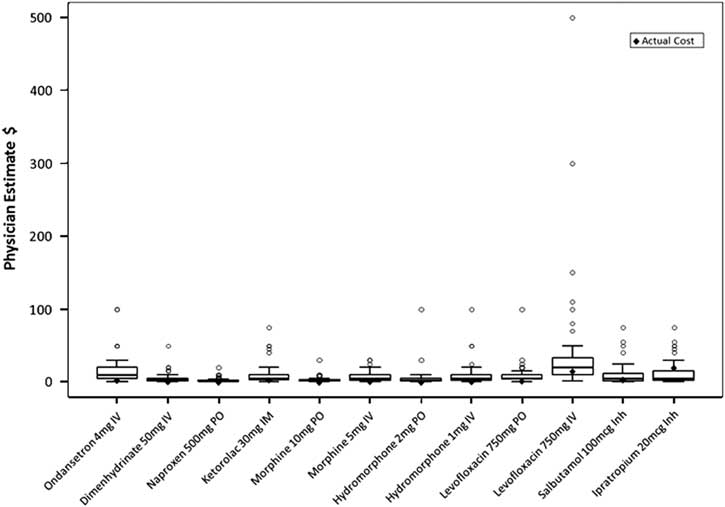
Figure 9 ED physician estimates of various pharmaceuticals.
Acknowledgements
RG participated in the design of the study, conducted the background literature review, managed the research ethics board application, collected the data, participated in the analysis and interpretation of the data, and wrote the final manuscript. Supervising Drs. JW, AF, and IS assisted with the design of the study and provided guidance throughout data collection and interpretation. MZ contributed to analysis and interpretation of data and critically revised the final manuscript. Data analysis was conducted by RM at The Ottawa Hospital Research Institute.
Appendix
Sample Survey Question