



Obesity is a major global health challenge, with more than one billion people estimated to live with obesity worldwide, and is a major driver of non-communicable diseases (NCD) such as CVD and some cancers(1). NCD contribute to 14 million deaths (71 % of all deaths) per year globally, and 77 % of these deaths occur in low- and middle-income countries (LMIC)(2). Overweight and obesity in Kenya and other LMIC are on the rise, particularly among urban populations(Reference Mkuu, Barry and Yonga3–Reference Abubakari, Lauder and Agyemang6). One-third of the adult population in Kenya is overweight or obese, and the rates are particularly high among urban residents, women and people with middle or higher wealth status(Reference Mkuu, Barry and Yonga3).
Among the four main risk factors for NCD, unhealthy diets have been identified as the major driver globally(Reference Charles, Boatemaa and Frempong7). In 2019, 7·9 million deaths and 187·7 million disability-adjusted life years were attributed only to unhealthy diets(Reference Qiao, Lin and Wu8). The global shift to increased consumption of ultra-processed foods (UPF) high in sugar and Na content and low intake of vegetables and whole grains have largely contributed to the rising overweight and obesity epidemic(Reference Qiao, Lin and Wu8,Reference Popkin, Adair and Ng9) . Urbanisation has caused the transformation of food environments through increased availability of modern retail food outlets, which mainly sell UPF(Reference Battersby10,Reference Berger and van Helvoirt11) , most of which are unhealthy. In most LMIC, there is a rapid increase in retail food outlets, sales and marketing strategies influencing dietary behaviours(Reference Kimenju, Rischke and Klasen12,Reference Demmler, Ecker and Qaim13) . The availability of modern retail food outlets has been positively associated with the purchase and consumption of unhealthy foods, and increased risk of overweight and obesity in Kenya and other LMIC(Reference Kimenju and Barling14–Reference Demmler, Klasen and Nzuma16). A GeoPoll survey among consumers in Kenya showed that 56 % of shoppers prefer shopping in supermarkets compared to traditional kiosks and informal vendors. Shopping in supermarkets has been associated with purchasing unhealthier food options(17). Identification of strategies used for marketing unhealthy foods in supermarkets is vital in informing regulatory interventions and consumer education(Reference Cameron18,Reference Young, Rosin and Jiang19) .
A study conducted in formal and informal food outlets in Uganda and South Africa showed a high level of promotion of unhealthy foods(Reference Spires, Berggreen-Clausen and Kasujja20). Studies conducted in Kenya on the retail food environments mainly focused on store access, food purchases and consumption, and their implication on the transition of dietary behaviours to consumption of processed foods, high adult BMI and prediabetes condition(Reference Demmler, Ecker and Qaim13,Reference Demmler, Klasen and Nzuma16,Reference Rischke, Kimenju and Klasen21) . Most studies have not examined in detail the relative shelf space allocation of healthy and unhealthy foods, the mapping of the food items available and the marketing strategies used to promote various food categories within the food outlets. One study conducted in Ghana assessed the in-store availability of unhealthy and healthy foods and the relative shelf space coverage of the foods in Accra(Reference Adjei, Amevinya and Quarpong22). However, this study only included urban areas and did not investigate the marketing of unhealthy and healthy foods in those outlets.
The main objective of this study was to assess the availability of various food types sold in food stores and the marketing of UPF in modern retail food outlets in urban and rural Kenya. We further explored the factors associated with the availability and marketing of UPF.
Methods
Study design and study site
This study was a cross-sectional study assessing the retail food environment in Kenya conducted from August 2021 to October 2021. For this study, a three-stage sampling approach was used. In the first stage, three Kenyan counties were purposively selected including Nairobi county (population: 4·397 million) representing an urban metropolitan setting, Mombasa county (population: 1·208 million) an urban coastal tourist city and Baringo (population: 666 763) county representing a predominantly rural setting in Kenya(23). The rationale for the selection of these counties was their diversity in socio-economic status (SES) as well as the level of urbanisation and geographical location. In stage two, sub-counties in each county were stratified into higher and lower socio-economically deprived areas using poverty-level data from the 2019 Kenya National Bureau of Statistics (KNBS) estimates(23). Areas with the highest number of people below the 10 % poverty line were classified as lower SES, while those with the lowest number of individuals living below the 10 % poverty line were classified as higher SES. From each SES level, one or two sub-counties were selected depending on the population size. Figure 1 shows the location of the selected counties in Kenya.

Figure 1. Map of Kenya showing the counties selected for assessing food availability and marketing at modern food retailers in 2021.
Modern retail food outlet identification
Trained field interviewers walked through the selected sub-counties and manually mapped and geocoded all the outlets that met the eligibility criteria set for this study. A food retail outlet was regarded as eligible if: (i) they were a self-service outlet, (ii) had at least one checkout point and (iii) had at least two stocked aisles. The inclusion criteria were based on the modern retail outlets landscape in Kenya. In Kenya, all self-service outlets are referred to as supermarkets; henceforth, we refer to them in this study as supermarkets or modern retail outlets. Food service restaurants such as fast-food joints and other non-self-service outlets such as shops, kiosks and informal vendors were excluded.
Data collection and measurements in modern retail food outlets
The International Network for Food and Obesity, Non-communicable Diseases Monitoring and Action Support (INFORMAS) protocol and tool on in-store food availability and marketing was adopted for data collection in the three counties(Reference Farley, Rice and Bodor24–Reference Vandevijvere, Waterlander and Molloy26). The INFORMAS protocol entails detailed research methodologies on monitoring, mapping and assessing food environments with the aim of promoting healthier food environments to reduce the risks of obesity and NCD(Reference Swinburn, Sacks and Vandevijvere27). The tool was piloted for 4 d prior to the actual data collection to adapt its use to the local context.
Food availability measurements (shelf space, floor space and location within modern retail outlets)
We identified all the food groups and the corresponding individual food items in the store and measured the shelf space for all the individual food items as follows: first, the food groups were identified and then the unique individual food and non-alcoholic beverages items were identified, and the allocated shelf space measured for each item. We excluded alcohol, infant formula and supplements from the measurements. The shelf space for each food item was determined by measuring the length (cm), width/breadth (cm) and height (cm) of the shelves and then multiplying these dimensions and the number of shelves occupied by the food items(Reference Farley, Rice and Bodor24,Reference Mhurchu25) . Since food items appeared in different locations in the supermarkets, we recorded the location along with measurement of the dimensions of the shelves and then aggregated the shelf area coverage by food groups(Reference Farley, Rice and Bodor24).
The total supermarket floor space was determined by requesting the measurements for the large supermarkets from the owners or by measuring floor space using the tape measures for the small supermarkets. For each supermarket, two research assistants were trained to take the measurements. A different pair of research assistants repeated these measurements to determine the inter-rater reliability score. The accepted inter-rater reliability was 90 %, failure to get this level of agreement prompted the repetition of measurements(Reference Mhurchu25).
The locations of all the food items based on their visibility were determined and recorded. The various locations include the endcap A, which is the end-of-aisles directly facing the entrance, and the centre of the supermarkets: endcap B represents the end-of-aisles facing the back of the store(Reference Mhurchu25,Reference Kerr, Sallis and Bromby28) . The island medium is the temporary aisles on the floor facing the centre, back or front of the retail food store(Reference Kerr, Sallis and Bromby28). These locations were then categorised using the Gro-Promo tool(Reference Kerr, Sallis and Bromby28) into various prominence levels pre-determined based on the individual level of placement and the visibility of the products(Reference Vandevijvere, Van Dam and Inaç29). Areas classified as high prominence included entrance, endcap A, checkout side, checkout edge and aisles. The medium prominence included endcap B, aisle medium and island medium, while low prominence included the edges of the store(Reference Mhurchu25,Reference Kerr, Sallis and Bromby28) .
Food marketing assessments
The food items advertised were recorded by observing the promotional flyers, posters and banners with food items inside the supermarket(Reference Mhurchu25). All the supermarket locations of the flyers were recorded, and all the food items advertised were recorded, as well as the promotional characters observed. The promotional characters observed on the promotional flyers in the supermarket include cartoon or company-owned characters, historical events such as Ramadhan and Christmas, licensed characters, for example, Mickey Mouse, amateur sports person (a person playing sports), famous sports person, for example, Dennis Oliech, sport events and celebrities.
Modern retail outlet size classification
The modern retail outlet size was subcategorised based on the number of checkout points(Reference Mhurchu25) as small (one checkout), medium (two checkouts) and large (more than two checkouts).
Food classification
The foods were classified based on the INFORMAS food categories(Reference Kelly30) and the NOVA classification(Reference Amevinya, Vandevijvere and Kelly31). The INFORMAS food categorisation classifies foods into core and non-core food categories(Reference Kelly30–Reference Monteiro, Cannon and Lawrence32). Examples of core food categories include healthier food options such as fruits and fruit products with no added sugars and salt, and vegetable and vegetable products with no added sugar and salts. Non-core food categories are unhealthy foods that include savoury snacks with added salts, sugars and fats and sugar-sweetened drinks including soft drinks such as sodas. The NOVA system classifies foods into (i) unprocessed/minimally processed which are foods in their raw state that have undergone no industrialisation processes and have no added sugars and salts such as fruits, vegetables, rice, beans and other unprocessed cereals, (ii) processed culinary ingredients which are additives and condiments added to foods during preparation such as oils and fats, (iii) processed foods, which are foods that have undergone minimal industrialisation process and have added salts, sugars and preservatives including jams and canned meat and fruits and (iv) UPF(Reference Mhurchu25), which are foods that have undergone numerous industrialisation processes and have a high level of sugar, fats, with low fibre and high energy density such as sugar-sweetened beverages. The food categories were further subcategorised into a binary variable: UPF and not UPF.
Statistical analysis
The analysis was guided by the INFORMAS protocol(Reference Mhurchu25). Descriptive statistics were used to show the distribution of these foods by counties, SES areas and prominence level/placement in the supermarkets. Ratios were used to compare the cumulative shelf length of UPF to unprocessed/minimally processed foods based on various store characteristics in the three counties.
The main outcome (dependent) variables were UPF availability for sale based on food counts and proportions, and shelf space of UPF and advertisements of foods in the store based on food counts and proportions. The independent variables included strategic placement/ prominence levels, SES levels and supermarket size.
Bivariate comparison between counties, SES areas, prominence level/placement in the supermarket of the proportions of UPF sold and advertised was conducted using χ 2 tests. Then univariate and multivariable Poisson regression models were used to determine the association between the count of foods available for sale and those advertised in the retail food outlets and the store characteristics. The store characteristics (independent variables) included the SES status, type of supermarket, levels of placement and the specific locations of the food items (prominence). For the cumulative shelf space (m2), which is a continuous outcome, we conducted bivariate and multivariable linear regression analysis to determine the predictors of the cumulative shelf space covered by different food groups. We adjusted for clustering within the individual modern retail outlets in all the regression models to account for the heterogeneity of the various settings. Post-estimations were conducted to assess the validity and fitness of the models.
Results
Store characteristics
In total, 252 modern retail food outlets met the inclusion criteria. Of these, 137 were excluded due to delays in getting permission from the store owners (110) or refusal to participate (27). All the exclusions were from Nairobi and Mombasa only. Table 1 shows the main store characteristics, while online Supplementary Table 1 details the store characteristics stratified by counties. Up to 70 % of the modern retail outlets were small-sized outlets, 22 % were medium and 8 % were large outlets. The mean surface area (floor coverage) of the outlets was different based on their county location. Nairobi had the highest mean food outlet floor size of 243 131 m2 (range 15 m2–15000 m2). Mombasa county had predominantly small-sized, outlets and a mean floor surface area of 68·21 m2 (range 10 m2–360 m2).
Table 1. Characteristics of modern retail outlets in Nairobi, Baringo and Mombasa counties

SES proportion: percentage (%) of individuals below poverty line.
In Baringo county, approximately 92 % of the outlets were small-sized, with an overall mean surface area of 206·91 m2 (range 15 m2–572 m2). Most of the small-sized outlets were found in low SES areas.
Food items available for sale in the modern retail food outlets and percent shelf space coverage
Overall food available for sale and shelf space coverage
We observed a substantial availability of unhealthier food options such as sugar-sweetened beverages and savoury snacks and a very low availability of healthier food categories such as fruits and vegetables. The oils high in mono- or polyunsaturated fats occupied the most shelf space within the supermarkets, namely 28·6 % (Fig. 2). The bread, rice, wheat, maize and other refined and whole cereals with no added salt or sugars group, representing approximately a mean (sd) of 18·6 (8·9) per cent of the total shelf space across the modern retail outlets, followed this (Table 2). The sugar-sweetened beverages, including soft and sweet drinks, occupied approximately 13 % of the total shelf space across the modern retail outlets. This was followed closely by sweet bread, cakes and high-fat savoury biscuits, which had 11 % overall coverage (Fig. 2). Vegetable and vegetable products, and fruits and fruit products with no added sugars and salts had the least shelf space of less than 2 % (Fig. 2 and Table 2).

Figure 2. Availability (measured by the proportion of total shelf space (%)) of different types of food items in modern retail outlets in Kenya.
Table 2. Shelf space coverage of food items in modern retail food outlets in the three counties

INFORMAS, The International Network for Food and Obesity, Non-communicable Diseases Monitoring and Action Support; SS coverage, shelf space coverage.
Sum, total shelf space surface area (m2) by county; total sum, total shelf space surface area (m2) in all counties.
Food availability by settings
A further categorisation using NOVA classification showed that UPF represented 40 % of all the food items available for sale in modern retail outlets varying across Nairobi (38·9 %), Mombasa (43·9 %) and Baringo (31·9 %), respectively (Fig. 3). There was a significant difference in the availability of different food products for sale in the three counties (P = 0·020, < 0·05), with the highest proportion of UPF being available for sale in the urban counties (Mombasa and Nairobi).

Figure 3. Unique food products displayed for sale and advertised in modern food outlets (food items available for sale N 3669, food items advertised N 992).
Food availability by prominence levels, SES settings and supermarket size
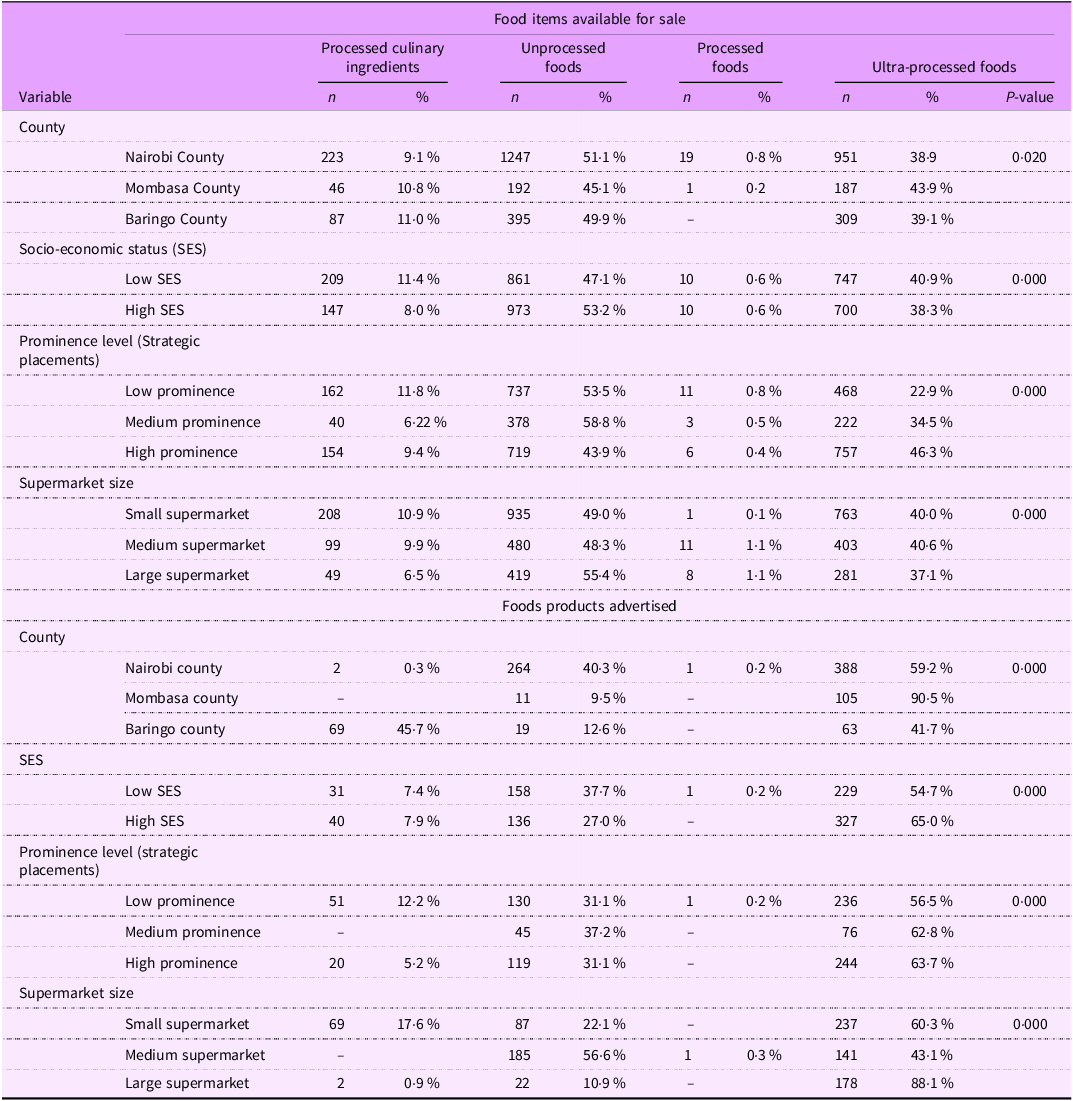
The bivariate comparisons showed food availability in the modern retail outlets were all significantly different by counties (P = 0·0020), prominence levels (P = 0·000), SES setting of the outlets (P = 0·000) and supermarket size (P = 0·000) (Table 3). The majority of the UPF were available in lower SES neighbourhoods (40·9 %) compared to higher SES neighbourhoods (39·1 %). The unprocessed/minimally processed foods were more available in higher SES neighbourhoods (53·2 %) compared to lower SES neighbourhoods. There was high availability of UPF in the high-prominence areas of the stores (46·3 %) and in small (40·0 %) and medium supermarkets (40·6 %).
Table 3. Distribution of food items available for sale and those advertised in the store
Ratios of the total cumulative shelf length and food items availability in modern retail outlets within the three counties
Table 4 shows the ratios corresponding to cumulative shelf space coverage and the food items available for sale in modern retail outlets. The shelf space coverage of the unprocessed/minimally processed foods was equal to that of UPF in all the counties, a ratio of 1:1. In small-sized modern retail outlets and low-prominence areas, unprocessed/minimally processed foods had more space coverage compared to UPF, a ratio of 2:1. We found equal shelf space coverage of the unprocessed/minimally processed foods to that of UPF (ratio of 1:1) in both high and low SES neighbourhoods. In low-prominence areas of the outlets, unprocessed/minimally processed foods had more space coverage compared to UPF, a ratio of 2:1.
Table 4. Ratio of the ultra-processed foods and unprocessed/minimally processed foods cumulative shelf space coverage and food items available in the modern retail outlets

SES, socio-economic status.
* Ratio of the total cumulative shelf space between ultra-processed foods and unprocessed/minimally.
† Ratio of the total ultra-processed foods and unprocessed/minimally processed food items available for sale.
Food items advertised in retail food outlets
Among the 922 food items advertised in the outlets through banners, posters and flyers, approximately 60 % were in the UPF category (Fig. 3). Of all the food items advertised in Nairobi, Mombasa and Baringo counties, 59·2 %, 90·5 % and 41·7 % of them were in the UPF, respectively. The majority of the foods advertised in the high-prominence areas of the supermarket were UPF (n 244, 63·7 %). Approximately 25 % of the advertisements had promotional characters. The most commonly used promotional characters were the cartoons or company-owned characters, observed among 18 % of the total advertisements. The bivariate comparisons of the food items advertised were all significantly different (P < 0·05) by counties, prominence levels, SES setting of the outlets and supermarket size (Table 3). There was a higher rate of advertisement of UPF in urban Mombasa county (90·5 %), higher SES area (65·0 %) and larger modern retail outlets (88·1 %). The medium- and high-prominence areas of the stores had a high proportion of advertisements of UPF, 62·8 % and 63·7 %, respectively.
Factor associated with UPF availability, advertisements and cumulative shelf space coverage
Food availability and advertisements as count outcome (Poisson regression)
There was a significantly higher rate of availability of UPF in Mombasa county (adjusted prevalence rate ratios (APRR): 1·13, 95 % CI 1·00, 1·26) compared to the rural Baringo county (Table 5). Conversely, there was no difference was observed in the availability of UPF in Nairobi county compared to rural Baringo county (APRR: 1·01, 95 % CI 0·88, 1·15) (Table 5). Further, there was a higher availability of UPF in medium prominence areas of the outlets (APRR: 1·14, 95 % CI 1·05, 1·25) and in high-prominence areas of the outlets (APRR: 1·69, 95 % CI 1·53, 1·86) (Table 4). There was a significantly increased rate of advertisement of UPF in Mombasa county (APRR: 2·18, 95 % CI 1·26, 3·79) compared to Baringo county and in the large-sized retail food outlets (APRR: 1·68, 95 % CI 1·06, 2·67) compared to small-sized outlets.
Cumulative shelf coverage as a continuous outcome (linear regression)
Table 6 shows the simple and multivariable linear regression analysis of the factors associated with the cumulative shelf space coverage of UPF in modern retail outlets. After adjusting for other predictors, there was a unit increase in cumulative shelf space coverage covered by UPF in Mombasa county by 96·9 units, in medium and large modern retail outlets by 231·6 and 220·4 units, respectively (Table 6). There was a significant unit decrease in cumulative shelf space coverage of UPF in high-prominence areas by 173·2 units.
Table 5. Poisson regression for factors associated with the UPF’s availability for sale and marketing in modern retail outlets

UPF, ultra-processed foods; PRR, prevalence rate ratios; APRR, prevalence rate ratio; SES, socio-economic status.
Table 6. Linear regression for factors associated with the cumulative shelf length coverage of different food groups in the three counties

SES, socio-economic status; ref, reference category.
The response variable is the cumulative shelf space (surface area coverage of the ultra-processed foods).
Discussion
We found that 40 % of all foods available for sale in modern food retail outlets were UPF and 60 % of the advertised foods were also in the UPF category. A higher level of advertisements and availability of UPF for sale were observed in urban counties and high-prominence areas of supermarkets. The majority of the shelf space was occupied by foods in the oils high in mono- or polyunsaturated fats category, followed by bread, rice and other refined and whole cereals category. There was a substantial coverage of unhealthier food options including sugar-sweetened beverages and sweet breads, cakes and high-fat savoury biscuits. Healthier food options including fruits and vegetables had very low shelf space coverage. There was a significant increase in cumulative shelf space coverage covered by UPF in Mombasa county, in medium and large modern retail outlets, respectively.
In a study conducted in Accra, Ghana, there was a 75 % availability of UPF for sale and a significant proportion of shelf space covered by UPF(Reference Adjei, Amevinya and Quarpong22). This was much higher compared to our study sites where our urban sites in Nairobi and Mombasa counties had 38·9 % and 43·9 % availability of UPF for sale, respectively. The cumulative shelf space allocation for UPF in the same Nairobi and Mombasa counties were 40 % and 10 %, respectively. The differences observed in the two studies may be due to the different dynamics of the retail food environment in Ghana and Kenya. The majority of the modern retail stores mapped in Kenya were small-sized stores, and we considered the inclusion of both rural and urban settings. Further, the differences in these settings could be attributed to the inclusion of two regions in the same counties representing both low SES and high SES settings. Previous studies have shown a link between consumption behaviours and geographic variability and quality and access to healthy foods with an increased accumulation of visceral and subcutaneous fats in people in urban areas(Reference Christensen, Eis and Hansen33). Our study findings further evidence the geographic variability in access to quality and healthy foods.
Our findings are consistent with findings from other studies in Kenya, Uganda and South Africa(Reference Spires, Berggreen-Clausen and Kasujja20,Reference Green, Pradeilles and Laar34) . This is an implication that Kenya is facing a nutrition transition and accelerated industrialisation, which is associated with the provision and consumption of UPF. The significant availability and marketing of UPF in medium- and large-sized modern retail outlets was also identified in a study conducted in two urban counties in Kenya and Brazil(Reference Gewa, Onyango and Opiyo35–Reference Costa, Claro and Martins37). This shows that the trends of the availability and marketing of unhealthier food options continue to grow with the evidence available in different countries. In this study, it was also evident that there was a relatively low shelf space allocation of the most recommended healthier food options, such as fruits and vegetables as found elsewhere in both high-income countries and LMIC(Reference Adjei, Amevinya and Quarpong22,Reference Green, Pradeilles and Laar34,Reference Costa, Claro and Martins37) . There are pronounced trends in the presence and preference for informal food vendors/wet markets for the purchase of fresh foods in Kenya, Ghana and Zambia(Reference Hannah, Davies and Green38–Reference Anku and Ahorbo40). This has been attributed to the convenience, accessibility and competitive pricing of wet markets and the prioritisation of fruits, vegetables and whole foods over processed foods in these settings(Reference Hannah, Davies and Green38). Therefore, the low shelf space allocation of healthier food options in Kenyan supermarkets could be due to low demand since people can purchase these products at better prices in wet markets and other informal outlets. In Ghana, the ratio of healthy foods to unhealthy/UPF was higher (1:5) implying that for every 1 m2 of shelf area for healthy foods, there was a 5 m2 cumulative shelf space area covered by unhealthy foods(Reference Adjei, Amevinya and Quarpong22). A study conducted in New Zealand supermarkets showed a close ratio of unhealthy to healthy foods as 1:0·42, with low-prominence areas having a ratio of 1:4(Reference Vandevijvere, Waterlander and Molloy26). In Kenya, the cumulative shelf space and food items availability for the UPF were not different from that of minimally processed foods. This means Kenya as compared to other countries still has a substantial amount of healthy foods available in the retail food outlets but an increasing proportion of unhealthy foods.
In Mombasa county, we had a higher availability and advertisement rate of UPF compared to other counties. This may be attributable to the urban-coastal setting in Mombasa harbouring tourism activities among other economic activities as a port city, with fewer commercial and subsistence farming activities. Accelerating urbanisation levels have been associated with nutrition transition and dietary shifts towards the provision, promotion and consumption of UPF(Reference Ren, Castro Campos and Peng41–Reference Karanja, Ickowitz and Stadlmayr43). Further, we observed that the cumulative shelf space coverage of the UPF increased significantly with supermarket size, SES status and prominence levels in the modern retail outlets in Kenya. The increasing availability of modern retail outlets, including supermarkets/minimarts and informal outlets, has been observed in other studies in Kenya and other low- and middle-income settings and has been associated with the provision of unhealthy foods(Reference Berger and van Helvoirt11,Reference Spires, Berggreen-Clausen and Kasujja20,Reference Adjei, Amevinya and Quarpong22,Reference Gewa, Onyango and Opiyo35,Reference Kroll, Swart and Annan44) . The availability of these outlets has been associated with the marketing of unhealthy foods in Uganda and South Africa(Reference Spires, Berggreen-Clausen and Kasujja20). This study evidences that exposure to unhealthy foods is linked with poor health outcomes among children and adults such as overweight/obesity and other nutrition-related NCD in Kenya. In Kenya, there are no specific regulations on supermarket food placement; however, a few policies are in development using some of this data as a reference. In LMIC, the introduction of food policies by introduction of taxes and tariff rates for unhealthy foods high in nutrients of concern such as sugars and salts consequently contributed to the reduction in overweight and obesity(Reference Abay, Ibrahim and Breisinger45). There is some progress regarding this policy in LMIC, and this evidence could serve as a benchmark to visualise the introduction of suggested policy guidelines to counter supermarket prominence of unhealthy foods in Kenya. In contrast, a study conducted in Australian supermarkets showed an increased availability of healthier food options such as fruits and vegetables in supermarkets(Reference Schultz, Cameron and Grigsby-Duffy46). The policy proposals in Australia on the restriction of the placement of food and beverage products in supermarkets may have caused the increased availability of healthier food options in supermarkets(Reference Cameron18). These policy recommendations can be suggested in Kenya as regulatory measures, as observed in high income countries (HIC) including Scotland and the UK where there are potential bans on the strategic placements of unhealthy foods and beverages in prominent areas of the stores such as the entrance and checkout sides(Reference Schultz, Cameron and Grigsby-Duffy46,47) . There needs to be proper contextualisation of these policy recommendations which are needed in a Kenyan setting.
Implication of findings
This study describes in detail the retail food environment encompassing food availability, placement and promotion in both rural and urban settings in Kenya. Although unprocessed/minimally processed healthier foods occupy substantial space in supermarkets, the higher level of promotion of UPF may shift food purchase decisions and influence consumption of UPF(Reference Popkin and Ng42,Reference Karanja, Ickowitz and Stadlmayr43) . There is a need to regulate the promotion of UPF in the food retail environment in Kenya. It is also important to take advantage of the availability of substantial amounts of healthier food options in Kenyan supermarkets by encouraging consumers to purchase them. Health education messages about healthier foods and appropriate labelling of foods as healthy or non-healthy can help inform consumers to make appropriate choices. While arguments surrounding personal responsibility persist, policymakers need to consider the critical role that food environments play in consumer habits. The development of policies around food marketing in retail environments may be a useful strategy to mitigate this issue. Such interventions could be developed against Kenya’s nutrition profile model and front-of-pack labels systems. The policymakers can benchmark and implement policy suggestions utilised in high-income countries such as Australia and the UK on the restriction of promotion and strategic placement of food and beverage food products in supermarkets(Reference Schultz, Cameron and Grigsby-Duffy46,47) . These policies will be relevant, particularly in rapidly urbanising urban areas as studies show a high prevalence of overweight and/or obesity in these areas due to the exposure of populations to obesogenic environments.
Study strengths and limitations
The strength of this study lies in selecting diverse settings including rural and urban settings varying in SES for the assessment of in-store food availability, advertisements and cumulative shelf space coverage. We used standardised tools of INFORMAS methodology enabling us to compare our studies internationally. However, we had a few limitations in our study. There was only a 46 % response rate from the modern retail outlets mapped in Mombasa and Nairobi counties, and most of the supermarkets included were small-sized supermarkets, and only 8 % were large supermarkets. The lack of access to large outlets, especially in the urban areas, may have led to an underestimate of the level of advertising for UPF. However, most outlets in Kenya fall in the category of small or medium size, especially in areas of low SES where the majority of the population in urban areas purchase food. The outlets that were accessed may therefore be more representative of the true distribution of outlets in Kenya.
Conclusion and recommendations
This study shows a substantial availability of UPF and a high level of advertisements of UPF in modern retail outlets in Kenya. We observed a significant association between the availability and advertisement of UPF in medium- and high-prominence areas of the outlets and increased shelf space coverage of UPF in the modern retail outlets in Kenya. This study shows cause for concern for Kenya as it suggests that in the absence of policy interventions as the country continues to develop and increasingly becomes a target for the food industry; the trends of an increased prevalence of NCD are likely to continue. The development of policies around food marketing and availability will address the high level of availability of unhealthier food options. Fiscal policies and marketing regulations on UPF and incentives for the consumption of fruits and vegetables may encourage consumers to make healthier choices, particularly in urban areas as supermarkets continue to take root.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980024002155
Acknowledgements
The authors acknowledge the stores that supported the data collection in Kenya, the Ministries of Health and Education in Kenya, and the county governments of Nairobi, Mombasa and Baringo for supporting the research in the country and in specific counties.
Financial support
This research is funded by The International Development Research Centre, Canada, to African Population and Health Research Centre (APHRC) and The SA MRC Centre for Health Economics and Decision Science/PRICELESS, grant number: 1019132-001.
Competing interests
There are no conflicts of interest.
Authorship
G.A., C.A., S.V., M.H. and A.L. designed and planned the study. M.N.W., C.H.K., V.O. and S.M. supported project implementation, data collection and monitoring. G.A., S.V., C.A. and R.E.S. advised and discussed the data analysis. C.H.K. analysed the data and drafted the manuscript, which was reviewed and edited by G.A., C.A., S.V. and R.S. All the authors approved the final version of the manuscript.
Ethics of human subject participation
This study was conducted according to the African Medical and Research Foundation (AMREF) ethics guidelines to ensure the appropriate consenting procedures from the storeowners. The approvals were given by both AMREF (approval number: ESRC P901/2020) and National Commission for Science, Technology & Innovation (NACOSTI) (licence number: NACOSTI/P/21/8429). Verbal and written consent was obtained from the store owners prior to accessing the stores for in-store food mapping and assessment.












 Open access
Open access