



Chronic low-grade inflammation, also termed ‘inflammaging’, plays a crucial role in aging, triggering the development of various age-related diseases and functional decline(Reference Franceschi and Campisi1,Reference Furman, Campisi and Verdin2) . Dietary components (e.g. nutrients or food items) either promote or suppress inflammation by influencing the immune system(Reference Noor, Piscopo and Gasmi3–Reference Ramos-Lopez, Martinez-Urbistondo and Vargas-Nuñez5). The balance between pro- and anti-inflammatory dietary components determines overall dietary inflammatory status, which can be quantified using the Dietary Inflammatory Index (DII)(Reference Shivappa, Steck and Hurley6). Research on the relationship between DII scores and disability, conducted both in Japan and elsewhere, has focussed principally on impairments in basic physical and cognitive functions(Reference Frith, Shivappa and Mann7–Reference Tomata, Shivappa and Zhang13). Our previous study added to existing knowledge by revealing an association between DII scores and reduced everyday competence (the ability to engage in complex processes that are indispensable when living independently). In increasing order of complexity, everyday competence includes instrumental activities of daily living (IADL), intellectual activities and social participation(Reference Masuda, Natsuhara and Sueyoshi14). This implies that dietary inflammation should be reduced to prevent declines not only in basic physical and cognitive functions but also in the complex practical activities that require such functions in the older population.
However, our earlier study had certain limitations. The sample size was relatively small (n 1642), and sampling was not systematic; the recruitment procedures differed among the five participating municipalities. Also, examination of whether DII scores are associated with subjective health would reveal the extent to which dietary inflammation affects the predictors of disability development(Reference Fong and Kok15,Reference Tas, Verhagen and Bierma-Zeinstra16) . Subjective health is a subjective assessment of health status, encompassing both mental and physical well-being. A systematic review revealed that subjective health was one of the most important prognostic factors in IADL disability, which considers the most basic components of everyday competence(Reference Tas, Verhagen and Bierma-Zeinstra16). A recent longitudinal study in Korea also suggested that poor subjective health predicted future IADL disability(Reference Fong and Kok15).
Based on our previous study, we systematically sampled a larger number of older adults living in non-urban municipalities in Japan to examine the link between DII scores and disability in everyday competence. We enrolled a more general population of older Japanese adults from six municipalities that vary in terms of regional characteristics. We also included subjective health as an outcome, which has been suggested to predict IADL disability. As in our previous study, we also explored the various determinants of DII scores(Reference Masuda, Natsuhara and Sueyoshi14).
Methods
Participants
Participants were recruited from six non-urban municipalities that differed in terms of regional characteristics. The municipalities were those of two Japanese prefectures: Suzu-shi in Ishikawa Prefecture and Unzen-shi, Shimabara-shi, Hasami-cho, Matsuura-shi and Minamishimabara-shi in Nagasaki Prefecture. The inclusion criteria were all residents of the target municipalities who were enrolled in the National Health Insurance system and aged 40–74 years at the time of the survey. For Shimabara-shi and Unzen-shi, of the residents who met the inclusion criteria, 50 % were randomly selected (with consideration of age and sex) and sent questionnaires due to the relatively larger population size and budgetary constraints. For the other municipalities, questionnaires were sent to all residents who met the inclusion criteria. Although this discrepancy in the sampling strategy could potentially affect the representativeness of the descriptive statistics of the entire study population, it should have minimal impact on the association analyses and the comparability between municipalities, as the eligible individuals in Shimabara-shi and Unzen-shi were randomly selected. Questionnaires were distributed in Hasami-cho, Matsuura-shi and Minamishimabara-shi in 2020, in Unzen-shi and Shimabara-shi in 2021 and in Suzu-shi in 2022. Questionnaires were sent to 30 558 eligible individuals across the six municipalities; 14 127 responded (46 %). After excluding individuals aged ≤ 64 years (n 4662), those aged ≥ 75 years (n 158), those with missing questionnaire data (n 1299) and those with energy intakes > 3 standard deviations from the mean (n 78), 7930 individuals were included in analysis.
Dietary Inflammatory Index
DII scores were calculated based on the intakes of twenty nutrients(Reference Masuda, Natsuhara and Sueyoshi14) detailed using a short FFQ validated for middle-aged and older Japanese adults(Reference Tokudome, Goto and Imaeda17). DII scores were calculated via the following steps: using a global dietary database(Reference Shivappa, Steck and Hurley6), nutrient intakes were converted to Z-scores and then to percentile scores that were in turn multiplied by the ‘inflammatory effect scores’ of the nutrients to yield ‘food parameter-specific DII scores’, which were summed to obtain the final DII scores. Previous studies have validated the use of DII scores in Japanese populations(Reference Kotemori, Sawada and Iwasaki18–Reference Yang, Hozawa and Kogure20).
Tokyo Metropolitan Institute of Gerontology Index of Competence
The Tokyo Metropolitan Institute of Gerontology Index of Competence is widely used to assess the everyday competence of Japanese populations(Reference Koyano, Shibata and Nakazato21). The index covers three components of competence: IADL, intellectual activities and social participation. Disabilities in everyday competence reflect the early development of disability (as explained elsewhere(Reference Masuda, Natsuhara and Sueyoshi14)). The Tokyo Metropolitan Institute of Gerontology Index of Competence questionnaire explores the ability to perform thirteen activities in the abovementioned three categories. Overall disability and disabilities in each component of competence were assessed in this study. In terms of overall disability, a participant was considered ‘disabled’ if s/he could not perform at least one of the thirteen activities. Similarly, in terms of disability in each component, a participant was considered ‘disabled’ if s/he could not perform at least one of the activities included in the corresponding component. Those lacking any disability were considered ‘healthy’ in terms of both overall disability and disability in each component.
Subjective health
Subjective health was assessed based on the answer to the following question: ‘In general, how do you feel about your own health?’ The responses were provided via a four-point scale: (1) excellent, (2) good, (3) poor and (4) very poor. Participants who reported excellent or good health were combined into the ‘good subjective health’ group, and all other participants comprised the ‘poor subjective health’ group. Poor subjective health, as assessed by a single-item question, has been associated with mortality in a meta-analysis of community-based prospective cohort studies from multiple countries published in English(Reference DeSalvo, Bloser and Reynolds22), as well as in a longitudinal study among older adults in rural Japan(Reference Okado, Bin and Tomoyama23), providing evidence that supports the predictive validity of this single-item question. Three studies conducted in Australia(Reference Crossley and Kennedy24), Sweden(Reference Lundberg and Manderbacka25) and the USA(Reference Zajacova and Dowd26) have demonstrated moderate reliability within repeated assessments of subjective health using a single-item question.
Statistical analysis
Factors influencing DII scores were sought using two regression models: Model 1 examined the association of each individual variable with the DII score, whereas Model 2 included all variables simultaneously. The variables included were sex (male, female); age (years); BMI (kg/m2); municipality (Suzu-shi, Unzen-shi, Shimabara-shi, Hasami-cho, Matsuura-shi and Minamishimabara-shi); living alone (yes, no); education level (≤ 9 years, ≥ 10 years); economic status (constrained, normal or good) and frequency of shopping (1–2 times per week or less, 3–6 times per week or more). Energy intake was included as a covariate in both models.
Subsequently, the associations between DII scores and everyday competence (i.e. overall disability and disability in each component of competence) and subjective health were examined via logistic regression analysis. The OR for being ‘disabled’ or having ‘poor subjective health’ were calculated. The covariates were sex, age, BMI, economic status, education level and energy intake. Analyses stratified by municipality were also conducted to examine the robustness of the results.
All statistical analyses were performed using R ver. 4·3·1 (R Project for Statistical Computing, Vienna, Austria). The significance level was set to P < 0·05.
Results
Table 1 shows the descriptive statistics. The mean (sd) age was 69·9 (2·7) years, and the mean (sd) DII score was 0·19 (1·36). In total, 60 % of the participants exhibited overall disability, and 18 %, 37 % and 41 % had disabilities in IADL, intellectual activities and social participation, respectively; 23 % reported poor subjective health.
Table 1 Descriptive statistics of participants’ characteristics, Dietary Inflammatory Index (DII) scores(Reference Shivappa, Steck and Hurley6), disability assessed using the Tokyo Metropolitan Institute of Gerontology Index of Competence (TMIG-IC)(Reference Koyano, Shibata and Nakazato21) and subjective health status (n 7930)

IADL, instrumental activities of daily living.
The associations of participants’ characteristics with the DII scores are shown in Table 2. In the model that included all variables (Model 2), they were all associated with the DII scores. Female sex, older age, more education, higher economic status and more frequent shopping were associated with lower DII scores. A higher BMI, living alone and residency in Matsuura-shi or Minamishimabara-shi were associated with higher DII scores.
Table 2 Associations between participants’ characteristics and Dietary Inflammatory Index (DII) scores(Reference Shivappa, Steck and Hurley6) (n 7930)

* The association of participants’ characteristics with DII scores was examined via regression analysis with energy intake as a covariate.
† Multiple regression analysis including all participants’ characteristics as explanatory variables was performed to examine the associations between the characteristics and DII scores. Energy intake was included as a covariate.
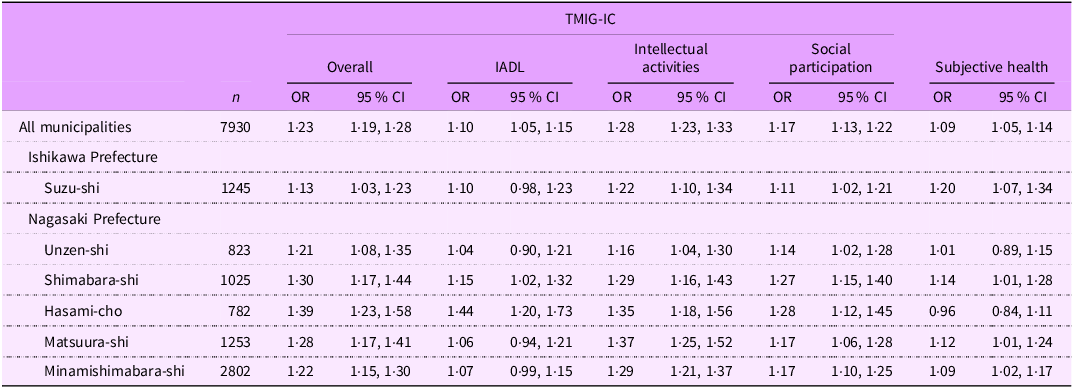
Table 3 shows the associations of the DII scores with disability and subjective health. In the entire population, the OR of disability was positively associated with the DII scores for overall disability (OR (95 % CI) = 1·23 (1·19, 1·28)) and disabilities in IADL (OR (95 % CI) = 1·10 (1·05, 1·15)), intellectual activities (OR (95 % CI) = 1·28 (1·23, 1·33)) and social participation (OR (95 % CI) = 1·17 (1·13, 1·22)). The OR for poor subjective health was also positively associated with DII scores (OR (95 % CI) = 1·09 (1·05, 1·14)). In the analysis stratified by municipality, DII scores were positively associated with the OR for overall disability and disabilities in intellectual activities and social participation (all six municipalities). Associations between DII scores and IADL disabilities were apparent only in Shimabara-shi and Hasami-cho, whereas associations with poor subjective health were seen only in Suzu-shi, Shimabara-shi, Matsuura-shi and Minamishimabara-shi.
Table 3 The associations of Dietary Inflammatory Index (DII) scores(Reference Shivappa, Steck and Hurley6) with overall disability and disabilities in each component of everyday competence assessed using the Tokyo Metropolitan Institute of Gerontology Index of Competence (TMIG-IC)(Reference Koyano, Shibata and Nakazato21) and subjective health status (n 7930) *
IADL, instrumental activities of daily living.
* The associations of DII scores with overall disability, disabilities in each component of everyday competence (IADL, intellectual activities and social participation) and subjective health were determined via multiple logistic regression analyses using the data for the entire study population, followed by analyses stratified by municipality. Sex, age, BMI, educational and economic status and energy intake were included as covariates. The OR are for disability or poor subjective health. Overall disability was defined as an inability to perform at least one of the activities in the TMIG-IC questionnaire. Disability in a given component of everyday competence (IADL, intellectual activities and social participation) was defined as an inability to perform at least one of the activities in the corresponding component. The following question was used to assess subjective health: ‘In general, how do you feel about your health?’ Participants who answered (1) excellent or (2) good were considered to have good subjective health, while those who answered (3) poor or (4) very poor were considered to have poor subjective health.
Discussion
The factors associated with inter-individual variations in DII scores were similar to those in our previous study(Reference Masuda, Natsuhara and Sueyoshi14); in both studies, male sex, living alone, less education, lower economic status and lower shopping frequency were associated with higher DII scores. This implies that these factors and dietary inflammation may be commonly associated in the non-urban Japanese population.
Additionally, older age, higher BMI and residence in Matsuura-shi or Minamishimabara-shi were associated with higher DII scores. Previous Japanese studies reported lower DII scores in older participants(Reference Son, Akishita and Yamanaka11,Reference Son, Lyu and Tanaka12,Reference Suzuki, Shivappa and Kawado19,Reference Yang, Hozawa and Kogure20) . Appetite loss associated with ageing can reduce the intake of certain pro-inflammatory nutrients, such as fat and protein, resulting in malnutrition(Reference Fielding, Landi and Smoyer27). Recent studies have suggested a bidirectional relationship between BMI and inflammation(Reference de Mello, de Gois and Kravchychyn28). The higher DII scores in Matsuura-shi and Minamishimabara-shi may be explained by lower adherence to the typical Japanese diet, which is high in seafood and plant food and reduces mortality(Reference Tsugane29). Lower intakes of the following anti-inflammatory nutrients best explained the higher DII scores in these municipalities: PUFA, n-6 fatty acids and vitamin D (all found in seafood) and dietary fibre and β-carotene (found in vegetables) (see online supplementary material, Supplemental Table 1). In Minamishimabara-shi, a higher fat intake (typical of a Western diet)(Reference Malesza, Malesza and Walkowiak30) also contributed to higher DII scores (see online supplementary material, Supplemental Table 1). Although moderate Westernisation of the traditional Japanese diet has improved the nutritional status of the postwar Japanese population(Reference Tsugane29), certain features of a Western diet, such as low fibre intake and excessive fat intake, can promote inflammation(Reference Malesza, Malesza and Walkowiak30,Reference Patry and Nagler31) . The differences in nutrient intakes among municipalities highlight the importance of targeting populations that diverge from the typical Japanese diet, i.e. those following a Western diet, when planning public health interventions to reduce dietary inflammation in Japan.
DII scores were positively associated with both overall disability and components thereof, as reported in our previous study(Reference Masuda, Natsuhara and Sueyoshi14). Other Japanese studies have linked DII scores mainly to disabilities in the basic functions required for everyday competence. One study used the disability certifications of the long-term care insurance system, which assesses impairments in physical and cognitive functions(Reference Tomata, Shivappa and Zhang13). Others focused on sarcopenia, i.e. pathologically impaired physical function(Reference Son, Akishita and Yamanaka11), or frailty defined by the five components of the Cardiovascular Health Study Index(Reference Son, Lyu and Tanaka12). In terms of everyday competence, two European studies reported associations between DII scores and IADL disabilities(Reference Laclaustra, Rodriguez-Artalejo and Guallar-Castillon32,Reference Assmann, Adjibade and Shivappa33) , but few relevant studies have been performed in Asia (including Japan). Our study adds to previous knowledge, focusing on the inability to perform complex activities. This has received minimal attention, especially in Asian populations.
To the best of our knowledge, this is the first study to reveal an association between DII scores and subjective health. Poor subjective health may reflect prodromal disease status(Reference Idler and Benyamini34) and has been associated with increased levels of C-reactive protein, an inflammatory biomarker(Reference Leshem-Rubinow, Shenhar-Tsarfaty and Milwidsky35). Poor subjective health may predict future IADL disability(Reference Fong and Kok15,Reference Tas, Verhagen and Bierma-Zeinstra16) , and our study implies that dietary inflammation influences this risk factor.
Our analysis stratified by municipality yielded generally consistent results, strengthening our evidence. However, no associations of DII scores with IADL disability or subjective health were apparent in certain municipalities. Associations between DII scores and certain variables may thus be region-specific.
The strengths of our study include the relatively large sample size, the systematic sampling method employed and the younger age of the study population. We previously evaluated adults aged > 65 years(Reference Masuda, Natsuhara and Sueyoshi14), whereas here we studied only those aged 65–74 years, who may be in earlier stages of disability development. The findings of this study should be interpreted in light of the following limitations. Due to the relatively moderate response rate (46 %), there is a potential for nonresponse bias in the study population, such as the healthy volunteer effect, where individuals who are healthier may be more likely to respond to the questionnaire. The potential issue of multiple testing is another limitation of this study. Given the multiple statistical analyses conducted across several health outcomes and subgroup analyses within individual municipalities, there is a potential risk of increased Type 1 errors (false positives), highlighting the need for careful interpretation of the findings.
Longitudinal studies are required to define causal relationships. In addition, the biological basis of the observed associations should be ascertained using measures of inflammatory biomarkers, including C-reactive protein.
Conclusion
This study highlights the importance of reducing dietary inflammation in the early stage of disability development. We have identified the determinants of dietary inflammation in older Japanese adults living in non-urban municipalities, which may aid the development of appropriate interventions.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980025000424
Acknowledgements
We acknowledge the study participants and the offices of the municipalities involved in this study (Suzu-shi, Unzen-shi, Shimabara-shi, Hasami-cho, Matsuura-shi and Minamishimabara-shi). We thank the Bureau of Public Health and Welfare Office of Nagasaki Prefecture and the Nagasaki National Health Insurance Organizations. The datasets used in this study can be obtained from the corresponding author upon reasonable request.
Authorship
M.M. performed data analysis and wrote the first draft. C.G. calculated energy and nutrient intakes using data from the FFQ. H.I. and M.O. contributed to the study conception, design and data collection. S.S., M.H., H.U. and R.N. were involved in data collection. M.U. contributed to the study conception and design and edited the manuscript.
Financial support
This work was supported by the Bureau of Public Health and Welfare of Nagasaki Prefecture and by JSPS KAKENHI Grant Numbers 20H05127, 20K21443 and 19H03315. The study was conducted under the cooperative research programme of the Institute of Nature and Environmental Technology, Kanazawa University <23027>. All the funders mentioned above had no role in the design, analysis or writing of this article.
Competing interests
There are no conflicts of interest.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethics Committee of the Faculty of Medicine of the University of Tokyo (approval number: 11095-(4)). Written informed consent was obtained from all subjects.






 Open access
Open access