


Although several studies have shown that, at arrival, US immigrants weigh less and have a lower prevalence of overweight than the native born individuals(Reference Singh and Siahpush1), this apparent health advantage declines with increased length of residence. Specifically, a significant, positive relationship has been observed between the length of residence and BMI(Reference Goel, McCarthy and Phillips2–Reference Oza-Frank and Argeseanu-Cunningham4). Similarly, age at arrival has been hypothesised to be an important determinant of weight change among immigrants(Reference Kaushal5). For example, it has been shown that immigrants who arrive to the United States at younger ages are at higher risk of overweight or obesity with increasing length of residence than immigrants who arrive at older ages(Reference Roshania, Venkat Narayan and Oza-Frank6).Consequently, length of residence and age at the arrival are often used in health research as indicators of acculturation to host country lifestyles. We previously reported that overweight prevalence among US immigrants varies by region of birth(Reference Oza-Frank and Narayan7). However, there is little research examining the combined effect of these migrant-specific characteristics (length of residence, age at arrival and region of birth) on overweight. By examining these variables simultaneously, additional insight can be provided into why and how patterns of overweight differ among immigrants.
The number of immigrant people in the United States has increased in recent decades, resulting in over 38·1 million immigrant individuals living in the United States (over 12 % of the population)(8). These individuals arrive from all over the world, with approximately 50 % coming from Latin America and 25 % coming from Asia(9). Grouping immigrants together into one large category may mask important heterogeneity with regard to specific health conditions, especially weight, which is driven by contemporary urban lifestyles in addition to genetic susceptibility(10). Therefore, the objective of this study was to use nationally representative data to estimate associations between the length of residence and overweight by region of birth and age at arrival among immigrants living in the United States.
Methods
Data source
Data on immigrant (defined as people living in the United States who were not US citizens at birth(Reference Schmidley11)) adult respondents aged 18–74 years were analysed from the nationally representative National Health Interview Survey (NHIS), pooling years 1997–2005 (n 33 299). The NHIS is a continuous, in-person health survey of civilian, non-institutionalised adults of 18 years and older, administered by the US Bureau of the Census for the National Center for Health Statistics (NCHS)(12). The survey uses a multistage probability design, with oversampling of Hispanics and blacks, and includes approximately 43 000 households and about 106 000 persons annually(12). Respondents provide self-reported information about basic measures of health status, utilisation of health services and social and demographic characteristics. In addition, one randomly selected adult per household is asked to complete the Sample Adult Module that elicits more detailed information on health-care services, behaviour and health status including height and weight.
Data were pooled to improve reliability of statistical estimates(13). To pool data, we first merged the sample adult file with the person-level file for each year included. Then, using NCHS guidelines for combining NHIS data with the same sample design, years 1997–2005 were concatenated into one data set(13). For this analysis, 2001 was the midpoint of the time interval included in the pooled data, and thus the estimates are representative of this point in time(13).
Sample weights provided by NCHS account for the complex sampling design of NHIS and for unequal probabilities of selection resulting from sample design, non-response and planned oversampling of certain subgroups. The survey is administered in Spanish or English languages and does not allow proxy respondents for sample adult questions. Family members may translate for a non-English- or non-Spanish-speaking respondent who is present in the home.
Definition of immigrant and the region of birth
The terms ‘immigrant’ and ‘migrant’ are used interchangeably in the text and refer to persons who were not US citizens at birth(14). All naturalised citizens, legal permanent residents, undocumented immigrants and persons on long-term temporary visas (such as students or guest workers) also fall into this category. Region of birth data are provided by NHIS from 2002 to 2005 based on the question ‘Where were you born?’ Before 2002 this information is not publicly available, and thus the use of this variable was requested through the NCHS Research Data Center(15). The nine mutually exclusive regions of birth categories used in this analysis, as provided by NCHS, were Mexico, Central America, Caribbean Islands (hereinto referred to as Mexico in the text), South America, Europe, Russia (and former USSR areas), Africa, Middle East, Indian Subcontinent, Central Asia and Southeast (SE) Asia.
Outcome of interest
Overweight and obesity were combined into one category and referred to as overweight, and defined as BMI ≥ 25 (measured as weight in kilograms divided by the square of height in metres) among adults(16). The NHIS calculates BMI from self-reported information on height (‘How tall are you without shoes?’) and weight (‘How much do you weigh without shoes?’), measures previously established as largely valid when used in combination with adjustments for age(Reference Kuczmarski, Kuczmarski and Najjar17).
Length of residence and age at arrival
Length of residence in the United States was determined based on the answer to the question ‘About how long have you been in the United States?’ This variable was then categorised by NCHS into one of the five following categories: <1, 1–<5, 5–<10, 10–<15 and 15+ years. On the basis of the distribution of responses, the first two categories were collapsed, resulting in four residence categories used in these analyses. Age at arrival was calculated by subtracting length of residence from the current age, and subsequently creating four age-at-arrival categories based on frequency distributions (<18, 18–24, 25–44 and 45–74 years). The length of residence information is not publicly available as a continuous variable and thus the continuous variable was accessed through the NCHS Research Data Center(12).
Covariates of interest
Sociodemographic characteristics included sex, poverty income ratio (PIR; <1·00 (below federal poverty line), 1·00–1·99, 2·00–2·99, 3·00–4·99 and ≥5·00), education (<high school, high school graduate, some college and college graduate). Lifestyle characteristics included marital status, smoking status and physical activity level. Other variables considered but not included in the analyses due to the lack of association were alcohol-drinking status, region of residence in the United States, metropolitan statistical area size and insurance status.
Statistical analysis
Sampling weights were adjusted to account for the pooled data(13). To assess differences in sample characteristics by region of birth, we used χ 2 tests for categorical variables and ANOVA for continuous variables. Two-tailed P values of ≤0·05 were considered significant for all analyses.
We performed multivariable logistic regression analyses and stratified models in two separate ways: (i) stratified by region of birth (interaction term length of residence × region of birth P = 0·01); and (ii) stratified by age at arrival and sex (interaction terms length of residence × age at arrival and age at arrival × sex P < 0·01). Earlier literature has shown differences in overweight by sex(Reference Ogden, Fryar and Carroll18). We also computed predictive marginals (with se) to estimate the multivariable-adjusted prevalence of overweight by region of birth. Predictive marginals are a type of direct standardisation in which the predicted values from the logistic regression models are averaged over the covariate distribution of the population(Reference Graubard and Korn19, Reference Saaddine, Cadwell and Gregg20). Because of the mathematical relationship, age at arrival = age − length of residence, these three variables could not all be entered in the same models. se were calculated with SAS-callable SUDAAN software version 9·0 (Research Triangle Institute, Research Triangle Park, NC, USA).
Results
The majority of migrants were born in Mexico (48 %), followed by migrants from all regions in Asia (∼20 %; Table 1). The mean age ranged from 38·0 (se 0·5) years (Africa) to 45·8 (se 0·3) years (Europe). Migrants from the Indian subcontinent had the highest proportion with a college degree (65·7 (se 2·0) %). Migrants from Mexico had the highest proportion living below the federal poverty line (25·0 (se 0·6) %) and the highest mean BMI (27·0 (se 0·1) kg/m2). Migrants from Russia, Africa and the Indian subcontinent had higher proportions of individuals residing in the United States <15 years, whereas the majority of migrants from the other regions had resided in the United States for at least 15 years at the time of interview. Migrants from Europe had the highest proportion of individuals who arrived <18 years of age.
Table 1 Sample characteristics by region of birthFootnote *,Footnote †
* Percentages based on weighted, unadjusted data.
† All P values <0·01 while comparing each row of data across migrant subgroup.
‡ Overweight defined as BMI >25 kg/m2; estimates from Oza-Frank and Narayan(Reference Oza-Frank and Narayan7).
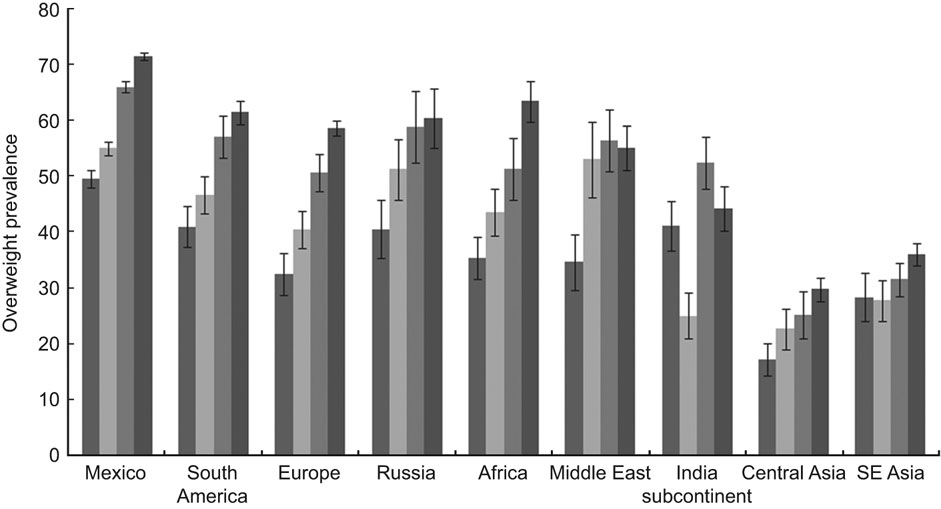
Fig. 1 Overweight prevalence by length of residence (![]() <5 years,
<5 years, ![]() 5 –< 10 years,
5 –< 10 years, ![]() 10 –< 15 years,
10 –< 15 years, ![]() >15 years) and region of birth. Overweight defined as BMI >25 kg/m2. Estimates are adjusted for sex, age at arrival, education, poverty income ratio, marital status, smoking status and physical activity level. P for trend is <0·01 for all regions except Indian subcontinent and Southeast Asia, where P = 0·06 for both regions. Error bars represent se
>15 years) and region of birth. Overweight defined as BMI >25 kg/m2. Estimates are adjusted for sex, age at arrival, education, poverty income ratio, marital status, smoking status and physical activity level. P for trend is <0·01 for all regions except Indian subcontinent and Southeast Asia, where P = 0·06 for both regions. Error bars represent se
Multivariate-adjusted analyses indicated that overweight prevalence increased by length of residence for all regions (P < 0·01) except for the Indian subcontinent and SE Asia, where no significant trend was observed (Fig. 1). For these latter two regions, the percentage point difference in overweight prevalence between <5 and >15 years residence was less than 10 %, whereas for all other regions, the difference ranged from 13 (Central Asia) to 29 % (Africa).
Furthermore, the odds of being overweight were three times higher in migrants from Mexico, South America, Europe, Russia, Africa and the Middle East residing in the United States for >15 years than their counterparts residing in the United States for <5 years (adjusted for sex, education, PIR, age at arrival, marital status, smoking status and physical activity level); the odds of being overweight among migrants from Central Asia was approximately two times higher (Table 2). Again, migrants from the Indian subcontinent and SE Asia had no associations between length of residence and overweight prevalence.
Table 2 Adjusted OR of overweight stratified by region of birthFootnote *
Bold values are significant at the 95 % confidence level.
* Models are additionally adjusted for age at arrival, marital status, smoking status and physical activity level.
Stratified by age at arrival (Table 3), among men and women aged <45 years at arrival with >5 years residence, the odds of overweight was generally higher than for those residing in the United States for <5 years (adjusted for region of birth, education, PIR, marital status, smoking status and physical activity level). A dose–response relationship was strongly evident among men and women arriving at 18–24 years such that effects of duration began as early as 5-year duration. In addition, the odds of being overweight was higher among Hispanic men arriving before 18 years of age than the European migrants, while the odds of being overweight was lower among those from Africa and SE Asia. The odds of overweight among women from Mexico who arrived at <45 years of age was higher than the Europeans (OR 1·3–1·9), and the odds of overweight among those from Central and SE Asia was consistently lower across all age at arrival categories (OR 0·1–0·5). Among women who arrived at 25–44 years of age, the odds of overweight was higher among those from Africa and the Indian subcontinent.
Table 3 Adjusted OR of overweight stratified by sex and age at arrivalFootnote *
Bold values are significant at the 95 % confidence level.
* Models are additionally adjusted for education, poverty income ratio, marital status, smoking status and physical activity level (data not shown).
Discussion
We found the association between the length of residence and overweight to be consistently positive across different regions of birth, except among Asian migrants, where minimal or no association was observed. In men and women, effects of duration began as early as 5 years after arrival among those arriving at 18–24 years of age. Younger ages at arrival and longer length of residence appear to be most important for Hispanics. In addition, arriving during child-bearing years increases the odds of being overweight among African and Indian immigrant women.
Consistent with earlier studies, length of residence was positively associated with weight among immigrants(Reference Goel, McCarthy and Phillips2, Reference Koya and Egede3, Reference Antecol and Bedard21, Reference Barcenas, Wilkinson and Strom22). Also consistent with earlier studies, region of birth was associated with overweight/obesity. For example, one study showed a significant, positive association between being born in Mexico and obesity(Reference Barcenas, Wilkinson and Strom22). Other studies have assessed this relationship by race/ethnicity and found significant weight increases among Hispanics, but mixed results among white, black and Asian immigrants(Reference Goel, McCarthy and Phillips2, Reference Kaushal5, Reference Park, Neckerman and Quinn23). The inconsistency of results by race/ethnicity might reflect the use of this variable as a socio-cultural construct rather than as a biological variable, whereas using region of birth may better represent the combination of genetic and cultural factors within each ethnic group(Reference Singh and Siahpush24).
Two earlier studies found that the relationship between overweight/obesity and length of residence varied by age at arrival. Specifically, arrival at younger ages was associated with higher prevalence of overweight with increased length of residence compared to arrival at older ages(Reference Roshania, Venkat Narayan and Oza-Frank6). Not only did our study have better precision than this one, but our study also showed that this relationship was consistent among men and women. Another study(Reference Kaushal5) assessing this relationship by race/ethnicity observed no association between age at arrival and obesity among Asians. Because we stratified by region of birth, we were able to differentiate Asian migrants and found that although men and women from Asian regions generally had a lower odds of overweight regardless of age at arrival, women from the Indian subcontinent arriving at 25–44 years of age showed increased odds.
There are several potential explanations for our findings. First, as suggested earlier, region of birth may be specific to genetics(Reference Singh and Siahpush24), which entails that our study may be revealing genetics as a stronger influence on weight than exposure to the US environment(Reference Oza-Frank and Narayan7, Reference Barcenas, Wilkinson and Strom22). Immigrants may have predispositions to particular health conditions(Reference Goel, McCarthy and Phillips2). For example, Hispanic whites and Asian Indians are most positively selected for health, but Mexicans are the least selected(Reference Jasso, Massey and Rosenzweig25).
Another explanation is that there is an interaction effect, with the effect of US exposure differing by country of birth(Reference Gordon-Larsen, Harris and Ward26, Reference Huh, Prause and Dooley27). For example, countries that have started sending immigrants to the United States recently may be increasingly similar to the United States in terms of dietary and physical activity norms, and thus the effects of US exposure may be lesser for more recent waves of migrants(Reference Park, Neckerman and Quinn23). On the other hand, recent migrants (e.g. migrants from the Indian subcontinent and Central Asia) may not have been exposed to the US environment sufficiently to experience the effect of US exposure on weight(Reference Sanchez-Vaznaugh and Kawachi28).
Some of the differences across regions of birth may also be due to differences in education. The association of length of residence with overweight has been shown to be particularly large for immigrants with lower education levels(Reference Kaushal5, Reference Sanchez-Vaznaugh and Kawachi28). This could be a reason for the significant results we observed between the length of residence and overweight among Mexican migrants, as more than half of migrants from Mexico in our sample have less than a high school education. Finally, changes in diet may explain the observed results. Higher levels of self-reported dietary change after migration have been shown to be significantly and independently associated with overweight after adjusting for age at arrival, length of residence, sex and education(Reference Roshania, Venkat Narayan and Oza-Frank6). In addition, immigrants who have resided the longest in the United States or arrived at younger ages were significantly more likely to report high dietary change from pre-migration diets than recently arrived immigrants(Reference Roshania, Venkat Narayan and Oza-Frank6). Dietary data were not available in the data set used in these analyses.
Immigrant neighbourhoods may also be associated with weight. Specifically, urban form, norms, expectations and resources may impact physical activity and diet(Reference Garn29, Reference Golan and Crow30) in ways that promote unhealthy weight gain (i.e. eating outside the home and consuming fast food and soft drinks(Reference Johnson-Taylor and Everhart31)). In addition, access to low-cost healthy foods may be more difficult in poorer neighbourhoods, and immigrants tend to live in such neighbourhoods initially(Reference Powell, Slater and Mirtcheva32). Despite the potential role of neighbourhood and environmental conditions as risk factors for obesity among residents of the United States, few studies consider them. One study(Reference Park, Neckerman and Quinn23) found no change in the relationship between duration and weight after inclusion of neighbourhood-level characteristics (immigrant density and linguistic isolation). Another study of found that immigrant men living in high immigrant areas were more likely to be obese than those living in low immigrant areas(Reference Grafova, Freedman and Kumar33). Yet another study(Reference Dubowitz, Subramanian and Acevedo-Garcia34) specific to immigrant women living in the Boston area found that a higher neighbourhood proportion of foreign-born individuals was associated with higher individual daily fruit and vegetable consumption. The latter result suggests that immigrant neighbourhoods may have better availability of produce, or the healthier diets from countries of origin are preserved in areas with higher immigrant density, but these hypotheses have yet to be tested.
Finally, globalisation is likely making it more difficult to measure acculturation, and challenging the assumption that acculturation is a post-migration process(Reference Park, Neckerman and Quinn23). What are considered to be post-migration effects might actually be a reflection of changes that are taking place in home countries. The current study is based on the assumption that life/environment in the country of origin/before moving to the United States is different from life in the United States. The only true way to assess this is to systematically measure conditions of interest (access/availability of specific foods, urbanisation, etc.) before and after migration.
The main limitation of our study is the use of cross-sectional data, making it difficult to disentangle age/period/cohort effects. For example, the use of cross-sectional data may result in the length of residence and age at arrival variables being confounded with cohort effects; i.e. individuals who arrived during the same period may be more similar to each other, and cross-sectional data cannot be used to distinguish between this and the effects of years of residence and age at arrival(Reference Lauderdale and Rathouz35). The complex relationships between the length of residence, age at arrival and overweight would be best examined with longitudinal data, which would allow the examination of relationships between change in BMI since arrival and the contribution of changing lifestyle factors, such as diet and physical activity.
Another limitation is the use of self-reported height and weight. An earliers study analysing data from adults in NHANES III found that the average immigrant woman under-reported her weight less than the average native woman. On the other hand, average native and immigrant men both under-reported their actual weight equally(Reference Antecol and Bedard21). Finally, NHIS data do not differentiate between types of migrants and thus naturalised citizens, legal permanent residents, unauthorised immigrants and temporary immigrants (students, visitors, guest workers, etc.) are all grouped in the same category. Despite these limitations, NHIS is the only nationally representative survey that provides information on both health and migration in this level of detail. The availability of such data have allowed researchers to move beyond comparing migrants to native born, and allowed us to examine characteristics specific to migrants that make them a distinct subgroup of the US population.
The main strength of our study was the use of a nationally representative annual survey with standardised variables. Pooling data across years resulted in relatively large sample of nationally representative immigrant adults. This allowed us to stratify results by region of birth and age at arrival, variables that remain understudied in the current body of migrant literature. Finally, although the length of residence and age at arrival are proxy measures of acculturation, these variables place minimal burden on respondents and are relatively easily translated(Reference Salant and Lauderdale36).
Conclusion
Increases in overweight prevalence among immigrants with longer duration of residence in the United States, possibly as a result of adoption of US lifestyles, is concerning given the adverse health consequences associated with excess weight(Reference Mokdad, Marks and Stroup37). Our study highlights the importance of migrant-specific characteristics, such as length of residence, age at arrival and region of birth, in assessing overweight risk and in identifying post-migration time points to target overweight prevention efforts. Further investigations aimed at disentangling the reasons for this may provide clues to the roles of genes and environment on the aetiology of overweight and to potential mechanisms for prevention.
Acknowledgements
R.O.-F. was supported by Grant/cooperative agreement no. 1R36SH000008-01 from the Centers for Disease Control and Prevention (CDC). The paper’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC. Both authors contributed to the study design, data analyses and interpretation, and manuscript preparation. The results of the study were presented in part at the 69th Annual Scientific Sessions of the American Diabetes Association, 5–9 June 2009, New Orleans, LA, USA. The authors would like to acknowledge Solveig A. Cunningham for her thoughtful review of the manuscript. The authors declare no conflict of interest.




