



Although there is no generally accepted definition of weight cycling, it can be described as repeated periods of weight loss and regain that form a pattern(Reference Strohacker, Carpenter and McFarlin1). Weight cycling is a phenomenon that is common in people with obesity who want to lose weight. However, it is increasing in people with healthy weight (body mass index [BMI] within the range of 18·5–24·9), especially girls who are dissatisfied with their appearance(Reference Montani, Viecelli and Prévot2) and athletes who want to improve their competitive results(Reference Franchini, Brito and Artioli3). Research on the impact of weight cycling on health status has been mainly done in obese populations, focussing on post-diet weight maintenance(Reference Marquet, Brown and Tafflet4). However, athletes are a unique population characterised by specific physical and psychological characteristics and eating patterns which may be potentially influenced by the volume of training and competition loads(Reference Sabato, Walch and Caine5,Reference Peplonska, Adamczyk and Siewierski6) .
It is common practice in combat sports that athletes use various methods to reduce body mass in order to compete in lower weight categories, presumably to gain a size or leverage advantage over smaller opponents(Reference Reale, Burke and Cox7). The two basic strategies for reducing body mass are chronic or acute. Chronic weight loss strategies include various forms of dietary restriction (targeting total energy or specific macronutrients) alongside increased exercise. In contrast, acute strategies most commonly take the form of intentional dehydration(Reference Reale, Slater and Burke8). In combat sports athletes, relative body mass variation during the season is significantly higher than in other sports(Reference Hagmar, Hirschberg and Berglund9). Moreover, given the relatively long break between weigh-in and competition, which varies between 3 and 30 h across Olympic and professional combat sports, athletes often engage in a variety of extreme acute rapid weight loss procedures, followed by rapid weight regain after the official weigh-in. This cycle is repeated throughout the entire competitive season and potentially throughout their careers(Reference Matthews, Stanhope and Godwin10).
However, striving for leanness can impair performance and have adverse health consequences if chronic energy deficiency develops(Reference Fogelholm11–Reference Rankin13). The International Olympic Committee released a consensus statement regarding chronic energy deficits in athletes attempting to chronically manage body mass and the potential detrimental effects on lean mass maintenance, immune function, bone health, metabolic rate and hormonal processes(Reference Mountjoy, Sundgot-Borgen and Burke14). The acute effects of weight cycling, especially rapid weight loss practices, in different combat sports are well known(Reference Franchini, Brito and Artioli3,Reference Zubac, Karnincic and Sekulic15) . In short, it seems that combat sports athletes usually reduce 2–10 % of their body mass before the competition, mostly in 2–3 days before weigh-in(Reference Artioli, Saunders and Iglesias16). The most common weight cycling methods are dehydration and food restriction; however, extreme rapid weight loss methods such as laxatives, diuretics, diet pills and vomiting are often used(Reference Brito, Roas and Brito17,Reference Dugonjić, Krstulović and Kuvačić18) . These methods can be hazardous to athletes’ health and sometimes even fatal(Reference Crighton, Close and Morton19). It has also been found that weight cycling begins as early as puberty(Reference Brito, Roas and Brito17,Reference Kordi, Ziaee and Rostami20,Reference Steen and Brownell21) , which can negatively affect growth and development(Reference Roemmich and Sinning22). However, the few studies that have analysed the long-term effects of weight cycling in combat sports athletes found greater weight gain at a younger age for weight cyclers (boxers, wrestlers and weightlifters) when compared with other athletes and the non-athlete population(Reference Nitzke, Voichick and Olson23,Reference Saarni, Rissanen and Sarna24) .
Saarni et al.(Reference Saarni, Rissanen and Sarna24) found out that former athletes display greater weight gain than the non-athletes, which may be attributed to the constant weight loss and regain during a sports career. Authors hypothesised that although they were physically active, the former athletes probably had lower than expected basal energy expenditure and gained more body mass. Similar findings were found in a cross-sectional study on 16-year-old wrestlers, where weight cycling was also associated with a lowered resting metabolic rate (RMR)(Reference Steen, Oppliger and Brownell25). However, McCargar and Crawford(Reference McCargar and Crawford26) found no differences in RMR between weight cyclers and non-weight cyclers in the same sample of participants, so future research is needed to confirm this hypothesis. Another possible explanation for higher body mass in weight cyclers after a sports career is increased food intake due to increased meal size and energy density associated with bingeing as a consequence of repeated weight cycling(Reference Saarni, Rissanen and Sarna24).
Conversely, Marquet et al.(Reference Marquet, Brown and Tafflet4) concluded that weight cycling has no particular effect on the post-career BMI of retired elite athletes, independent of diets undertaken during their careers. Similar patterns of BMI changes were observed in retired athletes and the general population. The greater physical activity in former athletes was a possible cause of their relatively stable post-career body mass despite frequent weight cycling. Similar conclusions were obtained by Nitzke(Reference Nitzke, Voichick and Olson23) on a sample of sixty former college wrestlers. Therefore, it can be concluded that: (a) the effects of weight cycling on human health, eating habits and lifestyle are still insufficiently clear and insufficiently examined; (b) the population of athletes is specific in terms of physical and mental characteristics compared with the population of non-athletes and especially individuals with obesity, and therefore further research is needed on these individuals(Reference Miles-Chan and Isacco27) and (c) the weight cycling procedures for each combat sport are different due to considerable differences between sporting disciplines. It is likely that there are also differences in weight cycling methods between the population of athletes and non-athletes. The long-term effects of weight cycling on health-related parameters could be different in all these subpopulations. To the best of authors knowledge, there is no developed instrument for assessing the long-term effects of weight cycling on health status, eating habits, physical activity and the lifestyle of former combat sports athletes. Therefore, this research aimed to develop and to assess the test–retest reliability of a new instrument that would determine the long-term effects of weight cycling on these parameters in an integrative and comprehensive way.
Material and methods
Study design
The Combat Sports Post-Career Health Questionnaire (CSPCHQ) construction and evaluation process consisted of three main stages: (1) Questionnaire development stage – the development of the questionnaire consisted of three parts, that is, scope/structure identification, content/face validity of the questionnaire and final questionnaire items; (2) Questionnaire translation stage – translation of developed questionnaire into different languages consisted of three parts, that is, forward translation, backward translation and panel group approval and (3) Reliability study stage – assessment of questionnaire reliability, where two aspects were addressed, that is, test–retest reliability and internal consistency.
The Ethical Committee of the Faculty of Kinesiology, University of Split, approved the study design and data collection (number: 2181-205-02-05-20-016; November 2, 2020). Participants acknowledged the approval form and consented to participate in this anonymous study by completing the survey voluntarily.
Questionnaire construction and evaluation
Questionnaire development stage
Scope and structure identification
CSPCHQ development centred on the long-term effects of weight cycling patterns on health status, eating habits and lifestyle combat sports athletes. Therefore, to define the scope and structure of the questionnaire, a literature review of health-related nutritional knowledge linked to weight cycling was conducted. Moreover, to get more in-depth information about the questionnaire structure, numerous meetings with dietitians, physicians and specialists in exercise sciences were conducted in-person and using online interviews. After this initial information was collected and the domain and concepts of the construct of interest were determined, the questionnaire was constructed using five sections (domains): (1) General information; (2) Weight cycling patterns; (3) Current lifestyle; (4) Eating habits and (5) Current health status. The questionnaire design aimed to be time-efficient, understandable and easy to complete. A total score was assigned to each domain (except for the General Information section).
Content and face validity of the questionnaire
Content validity refers to the extent to which the items in a questionnaire represent the subject (construct) matter, and it should be evaluated after the first draft is constructed(Reference Tsang, Royse and Terkawi28). Questionnaire items should cover crucial aspects of weight cycling patterns, health status, eating habits and lifestyle of the targeted population. Face validity refers to whether the questionnaire appears to measure what it claims to measure. Grammar, syntax, organisation and logical sequence of the statements must be evaluated to assess if the questionnaire is suitable for a given purpose(Reference Del Greco, Walop and McCarthy29). According to published guidelines(Reference Brod, Tesler and Christensen30), the questionnaire was sent to a panel group of nine experts with knowledge in psychometrics, nutrition, disordered eating, weight reduction, medical/health and exercise science to assess content and face validity. The panel group was requested to evaluate each question’s clarity, content, appropriateness and relevance. Additionally, experts were asked to give their opinion and suggestions about particular questions and the questionnaire as a whole. The CSPCHQ was designed with elements from already established/validated questionnaires combined with further newly constructed questions. In total, the first draft of the questionnaire that was sent to experts consisted of fifty-two items. During the judging process, changes in items included editing, removing and adding new questions relevant to the construct. The first review led to changes in sixteen items resulting in a second draft that consisted of fifty-five items. In the second review, experts changed five items resulting in the third and final draft that consisted of fifty-eight items.
Questionnaire items
The final CSPCHQ consisted of fifty-eight items divided into five sections online Supplementary Material. Only two items were open-ended. Expert opinion was that the questionnaire contains a sufficient number of items, has appropriate length and possesses a simple structure. Additionally, all items adequately represent the construct of interest. Longer and more complex questionnaires may elicit the loss of motivation and fatigue in participants during completion(Reference Tsang, Royse and Terkawi28). The sections with items of the CSPCHQ are as follows:
The General Information (eleven items) section requested personal information such as gender, body height, body mass and information relevant to combats sport and best-achieved results. The last item asked if participants had ever practiced weight cycling. If the answer was ‘No,’ participants skipped the Weight cycling patterns section and were redirected to the Current lifestyle section.
The Weight Cycling Information (eight items) section items were adopted from the Rapid Weight Loss Questionnaire (RWLQ), a self-reporting instrument initially designed for the evaluation of weight cycling patterns among judo competitors(Reference Artioli, Scagliusi and Kashiwagura31). The RWLQ has been shown as an excellent tool to determine the weight management patterns and behaviours and the risk related to weight cycling in heterogeneous and large samples of athletes in different combat sports(Reference Dugonjić, Krstulović and Kuvačić18,Reference Artioli, Gualano and Franchini32–Reference White and Kirk36) . The original question regarding methods of weight cycling had fourteen possible answers, but for this study, two additional answers were added (‘Hot tub’ and ‘Water overloading’). The total score for this question (Q19) was rated differently than in the original. Instead of a 5-point Likert scale rating, 0 point (Gradual dieting [weight loss in 2 or more weeks] and Increased exercise [more than usual]), 1 point (Skipping 1 or 2 meals; Fasting [all day without meals]; Restricting fluid ingestion; Training intentionally in heated training rooms; Saunas; Training with rubber/plastic suits; Use winter or plastic suits all day and/or night [without exercise]; Spitting; Hot tub; Water overloading) and 2 points (Laxatives; Diuretics; Diet pills; Vomiting) was assigned according to aggressiveness and harmfulness of each method. The maximum total score (RWLQScore) is 18 points.
The Current Lifestyle Information (five items) section aimed to assess the current lifestyle of participants. The first item was adopted from the Godin-Shephard Leisure-Time Physical Activity Questionnaire (GSLTPAQ) (Q20)(Reference Godin and Shephard37). Leisure-time physical activity is not essential for living and is considered as one of the most important for public health intervention and research(Reference Amireault and Godin38). Because the targeted population is former athletes, the GSLTPAQ item was modified by offering participants a maximum of ‘7 times or more’/week for a given activity. The second part of this section was items for assessing alcohol usage. For this purpose, a brief alcohol screening instrument, the Alcohol Use Disorders Identification Test-Concise (AUDIT-C)(Reference Bush, Kivlahan and McDonell39), was used (Q22–24). For the Q23, offered answers were modified. Rather than the ‘10 or more’ alcoholic drinks used in the original version, the highest number of drinks containing alcohol was modified to ‘7 or more’. The score for the GSLTPAQ was obtained by multiplying ‘times/week’ with 9 for strenuous exercise, 5 for moderate exercise and 3 for mild/light exercise. The answer ‘7 times or more’ was rated as eight times. The maximum total leisure activity score (GSLTPAQScore) is 136. The AUDIT-C scoring was as follows: 0 points for ‘Never’ and ‘0’ answers; 1 point for ‘Monthly or less,’ ‘1–2’ and ‘Less than monthly’ answers; 2 points for ‘2–4 times a month’, ‘3 to 4’ and ‘Monthly’ answers; 3 points for ‘2–3 times a week’, ‘5 to 6’ and ‘Weekly’ answers; 4 points for ‘4 or more times a week’, ‘7 or more’ and ‘Daily or almost daily’ answers. The maximum total score (AUDIT-CScore) is 12. Additionally, one item about smoking was added (Q21). The scoring was 1, 2, 0, for past smoker, current smoker and non-smoker, respectively.
The Eating Habits Information (seventeen items) section consisted of dietary and mindful eating assessment questions. The first eight items were adopted from Starting The Conversation (STC), a simplified food-frequency instrument designed for primary care and health-promotion settings (Q25–32)(Reference Paxton, Strycker and Toobert40). The second part of this section was the assessment of ‘Mindful Eating,’ awareness of physical and emotional sensations associated with eating without judgement. For this reason, the Disinhibition sub-scale from the mindful eating questionnaire (MEQd) consisting of eight items was used (Q34–41)(Reference Framson, Kristal and Schenk41). In addition to STC and MEQd, one item was added from Healthy Eating Assessment (HEA)(42) to rate participants’ overall habits of eating healthy foods (Q33). The scoring for the STC was as follows: 0 points for ‘5 or more’, ‘Less than 1’, ‘3 or more times’, ‘1 time or less’ and ‘Very little’ answers; 1 point for ‘1–3 times’, ‘3–4’, ‘1–2’, ‘1–2 times’, ‘2–3 times, and ‘Some’ answers; 2 points for ‘4 or more times’, ‘2 or less’, ‘3 or more’, ‘4 or more times’ and ‘A lot’ answers. For the answer ‘Less than 1 time’ 0 points were assigned in Q25 and 2 points in Q29. The maximum total score (STCScore) is 16 points. The scoring for the MEQd was as follows: 1 point for ‘Usually/Always’; 2 points for ‘Often’; 3 points for ‘Sometimes’; 4 points for ‘Never/Rarely’ answers in Q34–35 and Q40; 4 points for ‘Usually/Always’; 3 points for ‘Often’; 2 points for ‘Sometimes’; 1 point for ‘Never/Rarely’ answers in Q36–39 and Q41. Total score is divided with number of questions to get final score (MEDqScore). The scoring for Healthy Eating Assessment was 1, 2, 3, 4, 5 for ‘Poor’, ‘Fair’, ‘Good’, ‘Very good’, ‘Excellent’ responses, respectively
The Current Health Status Information (seventeen items) section (CHS) was a newly constructed part of the questionnaire to assess general health with no limitation for a specific age, disease or clinical group. The scoring for each question with categorical answers was as follows: 0 points for ‘No’ answers in all questions; 1 point for ‘Yes’ answers in Q46, Q51–52 and ‘Don’t know’ in Q42–44, 2 points for ‘Yes’ answers in Q42–44, Q47–50 and Q53–54; 3 points for Q45 and Q55. The Q57 was rated according to the Likert scale as follows: 0 points for 10–9 rate; 1 point for 8–7 rate; 2 points for 6–5 rate; 3 points for 4–3 rate; 4 points for 2–1 rate. The maximum total score (CHSScore) is 31 points. The Q56 and Q58 were open-ended questions that asked participants what type of cancer have they been diagonsed (if reported ‘Yes’ on previous question) and list of medications that they are currenly using (if any), respectively.
Questionnaire translation stage
The standard forward/backward translation protocol was applied to translate the CSPCHQ from English (ENG) to Portuguese (POR), Spanish (ESP) and Croatian (CRO). The translation aims to reduce the cognitive burden and overcome cross-cultural differences. The translation procedure was conducted following international guidelines as previously recommended(Reference Beaton, Bombardier and Guillemin43).
Forward translation
Three translators fluent in ENG and targeted languages (POR, ESP and CRO) performed forward translation. These translators were fully aware of the questionnaire concepts to provide a translation that more closely resembles the original text(Reference Tsang, Royse and Terkawi28).
Backward translation
A backward translation (from POR, ESP and CRO to ENG) was performed by a professional translator blinded to the original version of the CSPCHQ to avoid bias. The backward translations are performed to provide direct control over the quality of the translation(Reference Breslin, Looner and Berry44). This process establishes the same meaning between the original and translated questionnaire.
Panel group approval
The backward translation versions from POR, ESP and CRO languages were reviewed by a panel group of six experts consisting of three forward translators and three developers of the original questionnaire. The panel group was requested to determine whether the translated and original versions achieve semantic, idiomatic, experiential and conceptual equivalence and were free to modify/eliminate irrelevant, inadequate and ambiguous items(Reference Guillemin, Bombardier and Beaton45). After consensus among panel group members was reached, final versions of the CSPCHQ were approved.
Reliability study stage
The reliability of a questionnaire can be described as the consistency of the survey results, for example, the extent to which that same questionnaire would produce the same results under the same conditions when repeated(Reference Taherdoost46). The consistency of a CSPCHQ was evaluated using its test–retest reliability and internal consistency. For this purpose, participants completed the CSPCHQ on two occasions. In line with previous research(Reference Jones, Lamp and Neelon47,Reference Parmenter and Wardle48) , a time frame of 2–4 weeks between test and retest was chosen. Test–retest reliability can be affected by the length of time between the two test administrations. If the length interval is very short, it is more likely that carryover effects due to memory, practice or mood will occur, while a longer interval can increase the chances of changes in status(Reference Hart and Kang49). Participants were requested for their full attention, accuracy and seriousness on both occasions. Internal consistency assesses the degree to which items on a test are interrelated, that is, whether they are consistent in measuring the same construct(Reference Tavakol and Dennick50). Therefore, for all sub-scales used in this questionnaire, internal consistency was checked. Items in the STC and CHS sub-scales were not expected to intercorrelate significantly as sub-scales were designed to measure different constructs. Therefore, STC and CHS internal consistency was not measured.
Sample size calculation
The calculation of sample size was performed using Power Analysis and Sample Size software (PASS version 15 LLC, Kaysville, UT) and previously published recommendations(Reference Sim and Wright51,Reference Walter, Eliasziw and Donner52) . Power calculations reveal that a sample size of twenty-seven participants per sub-group (ENG, POR, CRO and ESP) is considered appropriate (P < 0·05; 80 % power) when assuming the ICC values of 0·75 and to be the minimally acceptable and expected levels of reliability, respectively(Reference Walter, Eliasziw and Donner52). This sample size would also be adequate to calculate κ coefficients to detect statistical significance at κ >0·6 with a proportion of positive ratings ranging from 0·1 to 0·9 and an 80 % power(Reference Sim and Wright51).
Data collection and management
This research used a convenience sampling technique. The data were collected through an online survey tool constructed after the final draft of the CSPCHQ was made. During the February 2021, participants were invited to complete a questionnaire sent to them by e-mail. The e-mails were collected through national association and authors’ personal contacts. A total of 190 questionnaires were mailed to study participants, 141 (74 %) were returned. Following 2 to 4 weeks, 118 participants filled out the CSPCHQ for the second time. Due to missing data, 8 (1 %) were excluded from further analysis. Therefore, the final sample consisted of 110 participants (ENG = 22, POR = 20, CRO = 44, ESP = 24). Questionnaire responses were checked and entered into a spreadsheet. The excel file was exported into the statistical software, where coding for categorical answers was conducted.
Statistical analysis
The CSPCHQ measurement properties evaluation was followed by the international consensus on terminology and definitions of measurement properties guidelines as suggested in the COnsensus-based Standards for selecting health Measurement INstruments (COSMIN)(Reference Mokkink, Terwee and Patrick53). A two-way random intra-class correlation coefficient (ICC 2,1a) for absolute agreement of single measures was used to determine the reliability of numerical data. A two-way random-effects model assumes that random error comes from both the raters and the participants(Reference Weir54). Additionally, the 95 % CI was calculated for each ICC. The percentage of agreement between the test and retest scores for all items was calculated. However, there is always a possibility of the chance agreement due to raters guessing. Therefore, Cohen’s κ for the dichotomous variables and weighted κ for variables with more than two categories were used to assess test–retest reliability for agreement beyond chance(Reference McHugh55). For both measures, a 95 % CI was calculated. ICC and κ values of ≤0·4, >0·4 and <0·59, >0·6 and <0·74 and >0·75 are considered as poor, fair, good and excellent, respectively(Reference Cicchetti, Bronen and Spencer56,Reference Landis and Koch57) . ICC values above 0·75 were considered acceptable for test–retest reliability. Cronbach’s α was used to assess internal consistency for GSLTPAQ, AUDIT-C and MEQd sub-scale scores. Alpha values between 0·70 and 0·95 are considered good. However, values > 0·90 may indicate redundant items as α is influenced by the number of items on a test; the more items, the higher the α (Reference Streiner58). Furthermore, to identify systematic biases, the RWLQ, GSLTPAQ, AUDIT-C, STC, MEQd and CHS sub-scale scores were tested using Wilcoxon’s signed rank test and effect sizes (ES) were calculated as r = Z/√n due to the skewed distribution of these data. An effect size of < 0·2 indicated a small, but meaningful magnitude of change, 0·2–0·7 a moderate change and > 0·7 a large change(Reference Cohen59). The significance level was set at P < 0·05. All data were analysed using SPSS statistical software version 26.0 (SPSS inc., Chicago, IL, USA) and GraphPad Prism software version 9.0 (GraphPad Software Inc., California, USA)
Results
Characteristics of the study population completing the CSPCHQ are presented in Table 1. The participants were mostly judo athletes (85 %), followed by boxers (5 %), wrestlers (5 %) and other combat sports athletes (5 %). Most of them were national medal holders (49), with 7 % having a World or Olympic medal.
Table 1. Characteristics of the study population completing the Combat Sports Post-Career Health Questionnaire
(Mean values and standard deviations)

ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
The test–retest reliability and internal consistency analysis of each CSPCHQ item are presented in Tables 2–6. Of the fifty-eight items and sub-items of the questionnaire, twelve were analysed by ICC, fourteen by Cohen’s κ, twenty-nine by weighted κ. The reliability of the open-text questions was not evaluated for reliability due to the nature of responses and the high likelihood of change between test and retest. Additionally, Q19 was also not evaluated because of the nature of the responses. With the majority of ICC values above 0·75, the questionnaire items were shown to be very stable. Additionally, according to κ values, the questionnaire has fair test–retest reliability, with only one coefficient being labelled as poor (Table 5; Q40 in ESP).
Table 2. Reliability of the General Information section of the Combat Sports Post-Career Health Questionnaire
(Coefficient values and 95 % CI)

% a: percentage of agreement; κ: Cohen’s kappa; wκ: weighted kappa; ICC: intra-class correlation coefficient; ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
Table 3. Reliability of the Weight Cycling Information section of the Combat Sports Post-Career Health Questionnaire
(Coefficient values and 95 % CI)

ICC: intra-class correlation coefficient; RWLQ: Rapid Weight Loss Questionnaire; ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
Table 4. Reliability of the Current Lifestyle Information section of the Combat Sports Post-Career Health Questionnaire
(Coefficient values and 95 % CI)

% a: percentage of agreement; wκ: weighted kappa; ICC: intra-class correlation coefficient; α: Cronbach alpha; GSLTPAQ: Godin-Shephard Leisure-Time Physical Activity Questionnaire; AUDIT-C: Alcohol Use Disorders Identification Test-Concise; ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
Table 5. Reliability of the Eating Habits Information section of the Combat Sports Post-Career Health Questionnaire
(Coefficient values and 95 % CI)
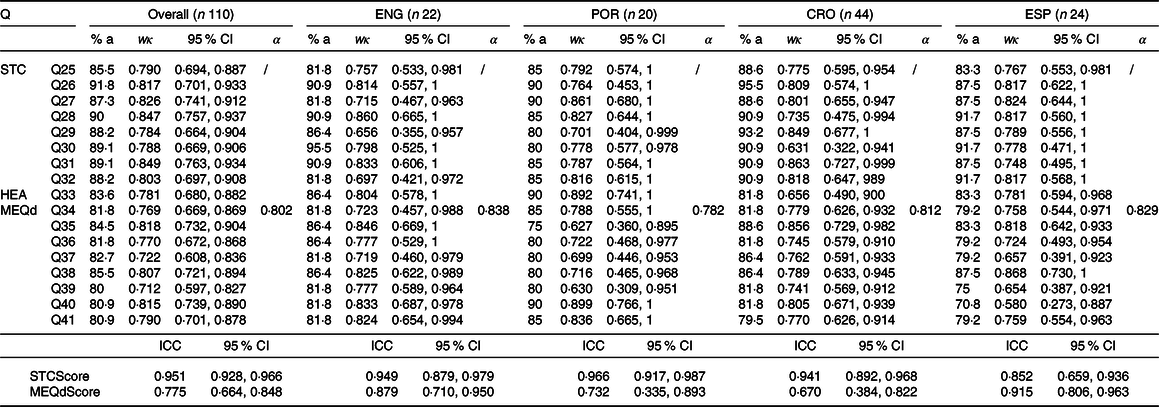
% a: percentage of agreement; wκ: weighted kappa; ICC: intra-class correlation coefficient; α: Cronbach alpha; STC: Starting The Conversation; HEA: Healthy Eating Assessment; MEQd: Mindful Eating Questionnaire disinhibition (MEQd); ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
Table 6. Reliability of the Current Health Status Information section of the Combat Sports Post-Career Health questionnaire
(Coefficient values and 95 % CI)

% a: percentage of agreement; κ: Cohen’s kappa; wκ: weighted kappa; ICC: intra-class correlation coefficient; ENG: English language; POR: Portuguese language; CRO: Croatian language; ESP: Spanish language.
All questionnaire sub-scales showed moderate to very good internal consistency when the overall sample was observed (α ranging from 0·605 to 0·802). Poor α values were found only in GSLTPAQ for CRO and ESP samples (Table 4).
Figures 1 and 2 represent scores of the questionnaire sub-scales obtained in test and retest. Wilcoxon’s Signed Rank Test revealed significant differences between test and retest scores only in the MEQd sub-scale (Fig. 2; overall: P = 0·002, ES = −0·208 [moderate]; CRO: P = 0·005, ES = 0·303 [moderate]).

Fig. 1. Rapid Weight Loss Questionnaire (RWLQ), Godin-Shephard Leisure-Time Physical Activity Questionnaire (GSLTPAQ) and Alcohol Use Disorders Identification Test-Concise (AUDIT-C) sub-scale scores obtained in the test and retest evaluation; ns – non-significant; / – analysis not performed due to the absence of variability; ENG – English language; POR – Portuguese language; CRO – Croatian language; ESP – Spanish language.

Fig. 2. Starting The Conversation (STC), Mindful Eating Questionnaire disinhibition (MEQd) and Current Health Status (CHS) sub-scale scores obtained in the test and retest evaluation; ns – non-significant; / – analysis not performed due to the absence of variability; ENG – English language; POR – Portuguese language; CRO – Croatian language; ESP – Spanish language.
Discussion
This research aimed to develop and assess the test–retest reliability of a new instrument created to determine the long-term effects of weight cycling on health status, eating habits, physical activity and the lifestyle of former combat sports athletes. Previous research on weight-cycling issues has been done mostly in one of two main ways using a cross-sectional survey model in humans (mostly individuals with obesity) or a longitudinal endpoint model in rodents(Reference Strohacker, Carpenter and McFarlin1).
In combat sports athletes, almost all investigations have dealt with the acute effects of weight cycling on various physiological and health-related dimensions; thus, long-term effects are still unknown(Reference Miles-Chan and Isacco27). Furthermore, this population lacks a unique measurement instrument to assess long-term effects on health status, eating habits, physical activity and lifestyle parameters. Therefore, this research provides an instrument that can add to both scientific advancement and professional intervention. The findings to date indicate possible adverse acute effects of weight cycling on physiological(Reference Fogelholm11,Reference Webster, Rutt and Weltman60) and health(Reference Mountjoy, Sundgot-Borgen and Burke14) status of athletes, as well as eating disorders of athletes(Reference Sudi, Ottl and Payerl61). The questions in the present questionnaire attempted to address these dimensions to determine the potential long-term risk of practicing weight cycling.
It is known that reliability is one of the most important characteristics of any valid measurement tool(Reference Weir54). The CSPCHQ is composed of different questions (numerical, categorical or on a 5-point ordinal scale). Different statistical procedures were applied to all of these types of questions (item-by-item analysis) to determine the reliability of this questionnaire. As previously stated by Artioli et al. (Reference Artioli, Scagliusi and Kashiwagura31), this approach avoids individual items with poor stability being overlooked when only summary statistics (e.g. general score of a sub-scale) is assessed. For this purpose, ICC, Cohen’s κ or weighted κ coefficients were calculated to indicate the stability of the questionnaire. The obtained results indicate that the CSPCHQ has acceptable to good test–retest reliability and internal consistency. In general, the sections with a larger number of questions, that is, a larger number of options within the question, had slightly worse reliability parameters, which is logical and expected.
It was hard to make direct comparisons with the findings of related investigations because of the novelty of the present study. Only comparisons of individual CSPCHQ segments with related questionnaires are possible. For example, the results of the test–retest reliability of the Weight Cycling Information section are very similar to those obtained in original RWLQ(Reference Artioli, Scagliusi and Kashiwagura31), designed to evaluate weight cycling patterns in judo players. Moreover, although Cronbach’s α was previously calculated for some validated sub-scales used in this questionnaire, internal consistency needed to be analysed within the CSPCHQ. Cronbach’s α indicates if the questionnaire is reliable for specific samples of participants and does not estimate reliability under all conditions(Reference Wilkinson62). Its estimation should be taken with care when calculating the same construct on different samples of participants(Reference Streiner58). However, Cronbach’s α values obtained in this research were similar to those previously calculated (GSLTPAQ = 0·64, AUDIT-C = 0·75, MEQd = 0·83). Poor α values were determined in GSLTPAQ for CRO and ESP. To assess the current lifestyle, we used the slightly modified GSLTPAQ, primarily constructed for the non-athlete population. Given that the CSPCHQ is designed for a sample of former athletes, more significant interventions in the above questionnaire are probably necessary to obtain better internal consistency.
Given that the questionnaire identified satisfactory reliability of the newly constructed questionnaire in four languages, future research could examine the metric characteristics of this questionnaire in other languages (e.g. Japanese, Russian). Also, it would be interesting to analyse former athletes of other (non-combat) sports and the population of non-athletes to determine possible differences in health status, eating habits, physical activity and lifestyle between these sub-populations.
The present research is not without limitations. One limitation was the inability to give more precise answers to some questions due to the structure of the questionnaire (e.g. blood pressure value). It would certainly be interesting in the future to interview the respondents in person and thus get better feedback. Also, although the total sample of respondents is relatively large, methodological procedures were done for each language separately, reducing the statistical power of obtained results. Although the calculated sample size needed was twenty-seven participants, three sub-groups failed to meet this number for calculations due to difficulties in adhering to the test–retest interval. Finally, this research did address the face and content validity of the instrument, but construct validity which is the correlation between responses to this questionnaire and other measurement methods was not assessed.
In summary, this research presents a novel questionnaire to assess the long-term effects of weight cycling on health status, eating habits, physical activity and the lifestyle of former combat sports athletes. Despite the limitations, valuable information on feasibility and reproducibility of the CSPCHQ was provided. Strong test–retest reliability parameters were determined in all four languages. More research is necessary to assess instrument validity.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114522001659
Acknowledgements
The authors would also like to express gratitude to all participants for their contribution to this research. The authors declare no specific funding for this work.
S. K. designed the study, supervised the data collection, wrote the manuscript and oversaw the manuscript preparation. E. F. designed the study, collected the data, wrote the manuscript and assisted with the manuscript preparation. D. H. F. designed the study, collected the data, wrote the manuscript and assisted with the manuscript preparation. J. R. S. designed the study, collected the data, wrote the manuscript and assisted with the manuscript preparation. O. D. A. collected the data, wrote the manuscript and assisted with the manuscript preparation. G. K. designed the study, supervised the data collection, analysed the data, wrote the manuscript and oversaw the manuscript preparation. All authors read and approved the final manuscript.
There are no conflicts of interest.










