


Nutrition education is the key element in promoting sustainable healthy eating behaviours(Reference Foerster, Heimendinger, DiSogra and Pivonka1). Similarly, health promotion from early stages in life has a major impact on health and well-being during childhood and later stages of life(2). Community trials suggest that nutrition and health education is an accessible and effective tool in developing healthy nutrition-related practices(Reference Kelder, Perry, Lytle and Klepp3, Reference Aldinger and Jones4). Early learning of these aspects by the adolescent age group results in change of their attitudes and behaviours towards future health(Reference Tones and Tilford5). The adolescents and young adults who benefit from nutrition and health education can act as change agents by spreading the messages to a large segment of the population(Reference Lionis, Kafatos, Vlachonicolis, Vakaki, Tzorttizi and Petraki6, Reference Green and Iverson7). Research also indicates that through adolescents, their younger siblings, families and other community members may be reached(Reference Delisle, Mouli and Benoist8). If such change agents are community service volunteers, the benefits are likely to be more. The National Service Scheme (NSS), a student youth service programme that has been in operation in colleges of India for over three decades, aims at creating social consciousness among youth with an overall objective of personal development (holistic development through experiential exposure) of the students through community service(9). Developing appropriate communication strategies for providing nutrition and health education to the student volunteers to disseminate the nutrition knowledge to the community is the need of the hour. In many of the earlier studies, assessment of the impact of nutrition education (and/or health education) interventions was done using parametric approaches such as paired t tests and ANOVA(Reference Vijayapushpam, Menon, Raghunatha Rao and Antony10–Reference Subba Rao, Raghunatha Rao, Venkaiah, Dube and Sarma12). By employing these tests one can only determine the overall impact on knowledge levels due to the education interventions used. In such cases, there is a possibility that certain individual topics on which the education intervention failed to bring about significant knowledge improvement are masked if the overall knowledge improvement comes out to be statistically significant. There is a need to assess the impact of an educational intervention on bringing about knowledge improvement of the group in relation to each of the individual topics covered in the educational intervention, because this enables suitable modification of the educational intervention. The McNemar test – a non-parametric test – is an appropriate test for identifying the symmetrical change among those cases in which change actually occurred after intervention. It was also reported that this test is suitable to evaluate the change in a pre-test and post-test design for assessing the effectiveness of an intervention, with scope to compare the increment in the responses to individual questions separately(Reference Parmenter13, Reference Williams, Aleong, Merrow and Morse14). Therefore, in the present study, knowledge increments were assessed using the non-parametric approach also with the following objectives:
1. To assess the nutrition- and health-related knowledge of undergraduate students.
2. To provide nutrition and health education using different communication materials.
3. To assess the impact of an intervention tool in improving knowledge on individual nutrition and health topics.
Materials and methods
Study design and setting
After obtaining the approval of the Scientific Advisory Committee of the National Institute of Nutrition, a prospective follow-up study with a before–after design was carried out among undergraduate NSS volunteers belonging to various streams of study in Arts (Humanities & Social Sciences), Commerce and Science. The study was conducted in the colleges affiliated to Osmania University, Hyderabad, Andhra Pradesh.
Sample
The operational area of Osmania University covers six districts in Andhra Pradesh with over 350 affiliated colleges offering undergraduate programmes(15). Among these colleges, about half offer the NSS programme. A district-wise list of colleges offering the NSS programme was procured from the NSS Programme Officer of the University and one college from each of the six districts was randomly selected for the study. From each of the six colleges, the complete unit of NSS volunteers was selected. Each unit contained over 100 student volunteers. The total number of study subjects was 687.
Necessary approvals were taken from the NSS Programme Co-ordinator of Osmania University, the college authorities and the respective NSS programme officers. Informed consent was also obtained from the student volunteers.
Data collection
A validated knowledge assessment questionnaire (KAQ) used in an earlier study(Reference Vijayapushpam, Subba Rao, Antony and Raghunatha Rao16) was used in the current study to collect baseline data on socio-economic characteristics and nutrition- and health-related knowledge levels of the 687 subjects. The KAQ consisted of thirty-one closed-ended multiple-choice questions pertaining to nutrition (n 18), adolescent phase (n 2), infectious diseases and health (n 9) and lifestyle diseases (n 2). A score of 2 was assigned to every correct answer and 0 for an incorrect answer. The maximum total score possible was 62. When the knowledge scores at baseline of the present group were compared with the baseline scores of two similar groups of the earlier study(Reference Vijayapushpam, Subba Rao, Antony and Raghunatha Rao16) they were found to be comparable, thus validating the knowledge scale.
The questionnaire was self-administered by the subjects under the supervision of the investigators. The subjects could complete the questionnaire in about an hour.
The same KAQ was used to collect data two weeks after the nutrition and health education intervention in each college.
Nutrition and health education intervention
The classroom-based lecture method was adopted for imparting nutrition and health education. In each college, this educational intervention consisted of six lectures of about 45 min to 1 h duration each, spread over a week. The lectures were targeted to the group based on the baseline data. Different communication materials such as charts, colour folders, slides and transparencies were developed and pre-tested for use as teaching aids by the lecturers. Charts contained basic information related to nutrition and health. Seven different multi-colour folders on different themes like energy, proteins, fats, micronutrients (Fe, iodine and vitamin A), nutrition during adolescence, nutrition during pregnancy and obesity were used for the intervention. In addition, slides and transparencies were also used by the investigators in the classroom lectures to teach nutrition deficiency disorders and other health-related topics like communicable diseases, hygiene and food safety.
Statistical analysis
After the intervention, over 50 % of the students were available for follow-up. For the purpose of the current paper, only those who were available at the baseline and post-intervention were considered for analysis. Although the dropout rate was high, it did not affect the overall outcome of the study as the mean knowledge scores and other general characteristics such as age, gender and education level of the subjects available for follow-up were not significantly (P > 0·05) different from those of the original group assessed at baseline.
Statistical analysis was done using the SPSS statistical software package version 11·5 (SPSS Inc., Chicago, IL, USA). The overall impact of nutrition and health education was assessed using the paired t test. The McNemar test was used to assess the effectiveness of the teaching method in bringing about knowledge improvement on individual topics.
Results
General characteristics of the subjects
The sample (n 687) comprised 68 % boys and 32 % girls. The general characteristics of the subjects are provided in Table 1. The majority of the student NSS volunteers were from commerce (economics) and other social sciences. Only 7 % of the students were from science groups. The average age of the students was 19 years.
Table 1 General characteristics of the subjects: student volunteers under the National Service Scheme, Andhra Pradesh, India (n 687)

Impact of the nutrition and health education intervention
There was a significant (P < 0·001) improvement in the overall nutrition and health knowledge of the student volunteers after the intervention. Their mean score at baseline was 33·8 (sd 6·53) and it increased to 45·2 (sd 6·07) after the intervention (Table 2).
Table 2 Effect of the intervention on nutrition and health knowledge scores, using the paired t test, among student volunteers under the National Service Scheme, Andhra Pradesh, India
*Significance considered as P < 0·05.
Out of eighteen items related to nutrition, the paired t test showed that the improvement was significant (P < 0·001) in sixteen; there was no significant improvement in the remaining two items as the baseline knowledge related to milk, soyabean protein and sprouts was already very high. Assessing the impact of the intervention on individual themes using the McNemar test (Table 3) showed that baseline knowledge about the basics on energy and protein was negligible; however, after the intervention, the percentage of students who answered these questions correctly doubled. At baseline only about 7 % of the NSS volunteers answered correctly regarding the importance of using a combination of oils, which increased over eleven times (80 %) after the intervention. Knowledge levels pertaining to the adolescent phase of both genders showed a significant improvement (P < 0·001) after the intervention. Pertaining to lifestyle diseases, there was a significant improvement (P < 0·01) in the knowledge levels related to obesity. However, no significant (P > 0·05) improvement in the scores related to knowledge on hypertension was observed, as the baseline knowledge level was already high.
Table 3 Percentage and number correctly answering the different questions on nutrition and health aspects: student volunteers under the National Service Scheme, Andhra Pradesh, India
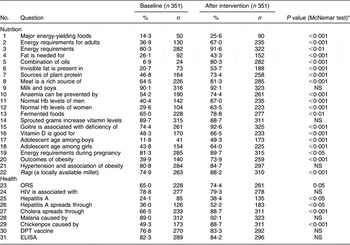
ORS, oral rehydration solution; DPT, diphtheria, pertussis and tetanus.
*Significance considered as P < 0·05; NS, P > 0·05.
Concerning the knowledge increment on infectious diseases, a significant improvement (P < 0·001) was observed in subjects’ knowledge related to cholera and chicken pox. However, there was no significant improvement in the remaining topics such as HIV/AIDS, ELISA, malaria and DPT (diphtheria, pertussis and tetanus) vaccine as the baseline knowledge in these areas was very high (Table 3).
Discussion
Nutrition and health education at a young age influences the attitudes of youngsters and enhances the knowledge and skills required for them to understand contemporary food and nutrition issues(Reference Lytle17). However, development of innovative nutrition education material is a continuous and demanding process(Reference Kreisel18). In such a scenario, the need to provide targeted (group-level customization)(Reference Kreuter and Skinner19) or tailor-made (individualized)(Reference Brug, Glanz, Van Assema, Kok and Van Breukelen20) education intervention programmes that focus on the specific topics (in nutrition and health) on which the target groups really need education becomes all the more important. If the effect of such nutrition and health education interventions is evaluated using parametric methods, only the overall impact can be assessed, which entails the researchers to know whether the intervention on the whole was successful or not. This poses a threat especially in cases where the nutrition and health education intervention has brought about statistically significant knowledge improvement, because there is every chance that the lacunae of the education method in not improving knowledge on certain individual topics are not brought to the fore. Results of the McNemar test make it possible to determine whether there is a significant difference between the pre-test and post-test scores of students on the dependent variable. A significant difference usually implies that an intervention or treatment has had an effect(Reference Ciechalski, Pinkney and Weaver21). In the present study, using the McNemar test we could assess the impact of an intervention on bringing about knowledge improvement of the group in relation to each of the individual topics/questions. Our knowledge intervention could not bring about significant (P > 0·05) improvement on certain topics like HIV/AIDS, ELISA, malaria, DPT vaccine, hypertension, milk, and soya products and sprouts. One reason for this could be that the average score at baseline on these questions was already high, which some studies have attributed to other factors such as previous health education in their curriculum, earlier exposure to various media and the influence of parents, teachers and peer groups(Reference Subba Rao, Raghunatha Rao, Venkaiah, Dube and Sarma12, Reference Clancy-Hepburn, Hickey and Nevill22).
Earlier studies indicated that in before–after designs where there is no control group available, the McNemar test makes it possible to determine whether there is a significant difference between the pre- and post-test scores after an intervention by using each subject as his or her own control(Reference Kreisel18, Reference Graham, Sketris, Burge and Edwards23, Reference Roth-Yousey, Caskey, May and Reicks24). In the Indian context, Malhotra et al. used McNemar’s test to evaluate their health education intervention among a group of food handlers (with no control group) and found this non-parametric approach useful in identifying the knowledge, attitudes and practices in which their intervention could bring about improvement(Reference Malhotra, Lal, Prakash, Daga and Kishore25). In the current study also we found that McNemar’s test was useful in determining the impact of our nutrition and health education intervention without having to use a control group.
Many before–after studies that assessed the impact of nutrition (and health education) on adolescents in India(Reference Raghunatha Rao, Vijayapushpam, Subba Rao, Antony and Sarma11, Reference Subba Rao, Raghunatha Rao, Venkaiah, Dube and Sarma12) have used at least two repeated measures of knowledge scores after the educational intervention to assess the improvement and retention in knowledge. In yet another study in a rural area of Andhra Pradesh, Bamji and Murthy have assessed the impact of nutrition education on knowledge and perceptions of school-going adolescents by only a single measure of knowledge score after the intervention(Reference Bamji and Murthy26). Although it is known that the validity of the results can be improved by including repeated measures, our study is limited by having only a single measure after the intervention and not being repeated.
Effective nutrition and health education should result not only in acquisition of knowledge and skills, but also in desirable changes in eating habits of the learners(Reference Smith27). Although the current study showed that providing nutrition and health education to the student volunteers by the lecture method is indeed an effective and efficacious way of imparting nutrition and health knowledge, it did not assess the changes in health and nutrition behaviour that such education would have resulted in. This may be an area for further research.
Study limitations
Although both the parametric and non-parametric tests in the present study indicated that the nutrition and health education intervention was effective in bringing about significant improvement in knowledge levels of the student volunteers, the results may be viewed with caution as the attrition rate was as high as 50 %.
To the best of our knowledge there were neither other nutrition and health education campaigns nor an increased focus on these topics in the mass media or in their curricula, other than the routine, during the period of the study. However, one cannot rule out the influence of such extraneous/confounding factors. The methodology of the present study does not offer a solution to eliminate the influence of such factors and future research can also look into these aspects.
Conclusions
The present study indicated that our targeted nutrition and health education intervention was effective in improving the knowledge of the student volunteers on almost all topics covered. However, using the McNemar test, we could identify the seven individual topics (four in health and three in nutrition) for which our educational intervention could not bring about a significant knowledge improvement. Suitable modifications could be carried out in the nutrition and health education material to strengthen the education intervention in these topics.
Acknowledgements
Sources of funding: The study was supported by the National Institute of Nutrition, Hyderabad. Conflict of interest declaration: None declared. Author contributions: T.V. developed the project proposal, secured funds and conducted the educational interventions; G.M.A. provided statistical design and assisted in data analyses and interpretation; G.M.S.R. was involved in development of the nutrition and health educational intervention and preparing the manuscript; D.R.R. supervised the study. Acknowledgements: We are grateful to the National Institute of Nutrition (ICMR) for supporting the study. We thank Dr B. Sesikeran, Director of the Institute, for his encouragement and Dr K.V.R. Sarma, former Head of the Extension and Training Division, for his timely suggestions. Our special thanks to the managements and students of all the colleges in which the study was conducted.



