



Introduction
Subglottic stenosis is a rare condition characterised by narrowing of the subglottic region of the larynx. The hallmark symptom is breathing difficulty (dyspnoea); however, patients may also experience stridor, chronic cough and wheezing.Reference Aravena, Almeida, Mukhopadhyay, Ghosh, Lorenz and Murthy1 This narrowing can be acquired, congenital or idiopathic in nature.Reference Aravena, Almeida, Mukhopadhyay, Ghosh, Lorenz and Murthy1 The most common cause of acquired subglottic stenosis is post-intubation injury as a result of trans-laryngeal intubation or tracheostomy. The incidence of tracheal stenosis after laryngotracheal intubation has been reported to be between 6 and 21 per cent.Reference Farzanegan, Farzanegan, Zangi, Golestani Eraghi, Noorbakhsh and Doozandeh Tabarestani2 Other causes of subglottic stenosis include trauma to the airway, inhalation burns, irradiation, tracheal infections (bacterial tracheitis, tuberculosis, histoplasmosis and diphtheria) and collagen vascular diseases (granulomatosis with polyangiitis, relapsing polychondritis, polyarteritis and scleroderma).Reference D'Andrilli, Venuta and Rendina3 Rarely, subglottic stenosis can be congenital in nature. Congenital narrowing of the subglottic region is a well-known cause of stridor in infants.Reference Manickavasagam, Yapa, Bateman and Thevasagayam4 Congenital subglottic stenosis may manifest by itself, or, more commonly, in tandem with a variety of congenital anomalies or syndromes.Reference Manickavasagam, Yapa, Bateman and Thevasagayam4 These include tracheomalacia, campomelic syndrome, trisomy 21, laryngotracheoesophageal clefts, ulnar mammary syndrome and oesophageal atresia.Reference Manickavasagam, Yapa, Bateman and Thevasagayam4 Although familial occurrence of congenital subglottic stenosis is rare, there are a few reports in the literature.Reference Manickavasagam, Yapa, Bateman and Thevasagayam4,Reference Linna, Hyrynkangas, Kaukola and Pajunen5
Idiopathic cases account for only a minority of all subglottic stenosis cases and are commonly termed idiopathic subglottic stenosis. A diagnosis of idiopathic subglottic stenosis cannot be reached until all the above known causes of subglottic stenosis have been carefully eliminated. Idiopathic subglottic stenosis is a rare disease of unknown aetiology, with an incidence estimated to range between 0.2 per 100 000 and 1 per 400 000 persons per year.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6,Reference Aarnæs, Sandvik and Brøndbo7 The annual incidence rate of 0.2 per 100 000 persons was determined by a retrospective study of patients in south-eastern Norway.Reference Aarnæs, Sandvik and Brøndbo7 Previous studies have demonstrated a strikingly homogeneous population afflicted by idiopathic subglottic stenosis, generally healthy women in their fifties.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6–Reference Benjamin, Jacobson and Eckstein9 The disease is characterised by progressive submucosal fibrotic tissue deposition that manifests as laryngeal and upper airway obstruction.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6,Reference Aarnæs, Sandvik and Brøndbo7 The mean duration of time between symptom onset and diagnosis is approximately 3.1 years.Reference Aarnæs, Sandvik and Brøndbo7 Dedo and Catten, in a study of 52 idiopathic subglottic stenosis patients, demonstrated that 12 (23 per cent) were wrongfully diagnosed with asthma, and the correct diagnosis was delayed up to 18 months.Reference Dedo and Catten8 Flexible laryngoscopy is required to confirm the diagnosis.Reference Aarnæs, Sandvik and Brøndbo7
In contrast to traumatic subglottic stenosis, which can generally be cured with resection, idiopathic subglottic stenosis is characterised by spontaneously regenerating submucosal fibrotic tissue.Reference Dedo and Catten8 As this is a progressive and recurrent condition, treatment goals are directed at maintaining airway patency, to reduce symptoms and avoid tracheostomy. Repeated surgical intervention is often needed to mitigate airway obstruction and prevent respiratory difficulty.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6 Treatment options include surgical resection, as well as interventional bronchoscopic treatments such as laser, mechanical dilation and stenting.Reference Farzanegan, Farzanegan, Zangi, Golestani Eraghi, Noorbakhsh and Doozandeh Tabarestani2 Aarnæs et al. demonstrated that among patients who underwent surgical treatment for idiopathic subglottic stenosis, 21.1 per cent required a single procedure, while 78.9 per cent underwent multiple operations, and the mean time interval between procedures was one to three years for all age groups.Reference Aarnæs, Sandvik and Brøndbo7 The significant psychological and physical stress is compounded by having multiple operations.
A few reports in the literature also suggest that an underlying genetic predisposition may exist for the development of subglottic stenosis.Reference Linna, Hyrynkangas, Kaukola and Pajunen5,Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6,Reference Dumoulin, Stather, Gelfand, Maranda, Maceachern and Tremblay10 The first series of cases to suggest a genetic predisposition described two pairs of sisters and a mother and daughter, all adult patients who presented with idiopathic subglottic stenosis in the absence of all other contributing factors.Reference Dumoulin, Stather, Gelfand, Maranda, Maceachern and Tremblay10 Additionally, a recent report presented twin sisters discovered to have idiopathic subglottic stenosis in their forties.Reference Abbasi Dezfouli, Shadmehr and Sheikhy11 Cases of congenital subglottic stenosis have also been described in two unrelated pairs of siblings from unrelated parents,Reference Linna, Hyrynkangas, Kaukola and Pajunen5 as well as in three children born to consanguineous parents.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6 These reports strengthen the hypothesis that there may be a genetic component to the development of subglottic stenosis.
Hutterite Brethren
The Hutterite Brethren are a communal branch of Anabaptists living in the North American prairies, the majority of whom are descendants of just 89 founders.Reference Nimgaonkar, Fujiwara, Dutta, Wood, Gentry and Maendel12 The Hutterites share their Anabaptist origins with the Mennonites and the Amish, but their principle of holding all things in common makes them unique.Reference Evans and Peller13 What further separates the Hutterites is the degree to which they have maintained their culture. Their language, school and socialisation process, clothing, and lifestyle persist.Reference Evans and Peller13 Almost all the Hutterites live in rural communes called ‘colonies’ in Western Canada and the upper Great Plains of the USA.Reference Nimgaonkar, Fujiwara, Dutta, Wood, Gentry and Maendel12 When a colony reaches a threshold population size of 120–150 inhabitants, it is split into two, and half of the members move to a daughter colony.Reference Evans and Peller13
According to the 2016 Canadian census by Statistics Canada, the Hutterites number 6250 people, who live in 66 colonies within the province of Saskatchewan and constitute approximately 0.57 per cent of the total population of Saskatchewan (Figure 1).14 With a total population now surpassing 40 000 people in North America, their isolated social characteristics have produced a founder effect and a unique genetic history demonstrated by the over-representation of several Mendelian genetic disorders.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15,Reference Hostetler16
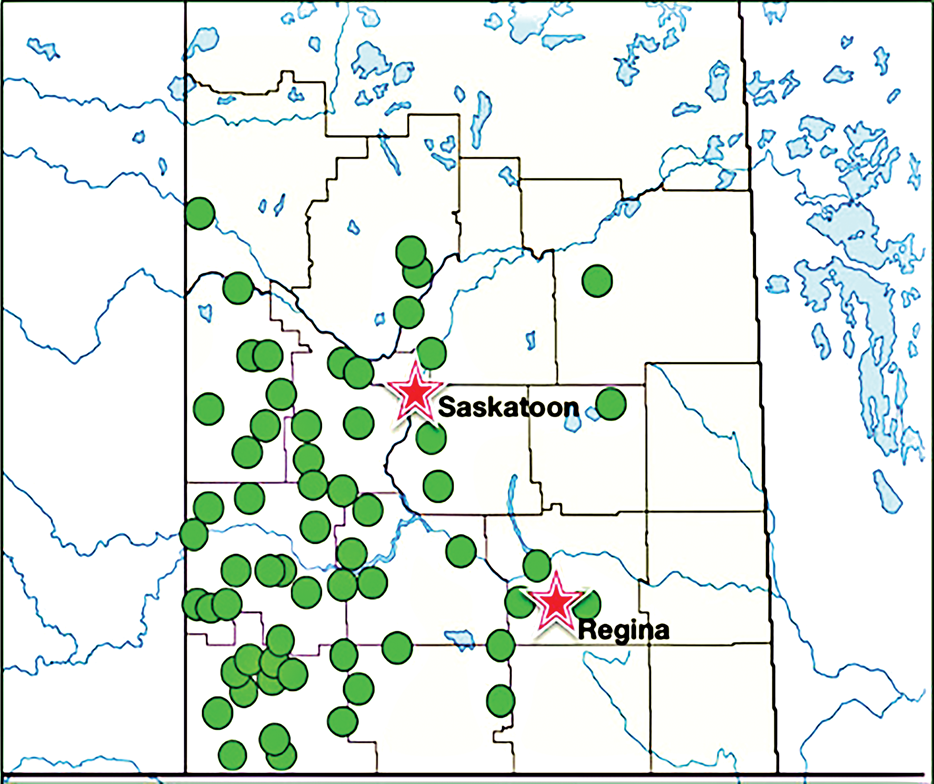
Fig. 1. A map of southern and central Saskatchewan, depicting locations of Hutterite colonies (green dots) in relation to the two major population centres, Saskatoon and Regina (pink stars).
The current study sought to shed light on the aetiology and epidemiology of idiopathic subglottic stenosis by investigating a possible connection between the Hutterite population and the development of idiopathic subglottic stenosis. By demonstrating that the cumulative incidence is higher in the Hutterite population than in the general population of Saskatchewan, we may be able to strengthen the hypothesis that a genetic predisposition exists for the development of idiopathic subglottic stenosis. Developing a greater understanding of the aetiology of idiopathic subglottic stenosis may help clinicians to prevent, diagnose and treat this rare condition more effectively.
Materials and methods
The study was found to be acceptable on scientific and ethical grounds, and received a Certificate of Approval from the University of Saskatchewan Biomedical Research Ethics Board through the delegated (subcommittee) review process.
Data handling
Data were accessed through a secure health authority network, and stored on an encrypted, password-protected external drive. Participants were assigned a participant number and no specific identifying data were recorded. The master list was stored separately from the study data on a separate encrypted, password-protected external drive. Data will be stored for five years from the onset of the study date and eliminated from the drive after this period.
A retrospective chart review examined the medical records of all adult patients (aged over 18 years) treated for subglottic stenosis in Saskatchewan, the population of which is 1.1 million, between the years of 2008 and 2018. As idiopathic subglottic stenosis is a very rare condition with an annual incidence of just 0.2 per 100 000 and 1 per 400 000 persons,Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6,Reference Aarnæs, Sandvik and Brøndbo7 we used all available cases for this study. Cases with known causes of subglottic stenosis were not considered further in this study. Known causes of subglottic stenosis that were removed included: intubation-related airway stenosis, granulomatosis with polyangiitis, irradiation and/or cancer to larynx, sarcoidosis, tracheostomy, inhalation burns, and bilateral vocal fold immobility.
The following data were collected: age at time of diagnosis, gender, presence or absence of family history, presence or absence of gastroesophageal reflux disease, and location (rural or urban). Postal codes collected from each patient were searched in the Canada Post database (the primary postal operator in Canada) to determine the corresponding address. Cases were determined to be urban or rural based on criteria set out by Statistics Canada.17
Hutterites live in colonies that have been listed in the Canadian Hutterian Brethren Directory for Saskatchewan.18 In order to determine the Hutterite status of a case, we matched the address and postal code of each patient to the address and postal codes of the colonies listed in the directory. We believe this to be a reliable way of ascertaining whether or not someone belongs to the Hutterite group, as it is extremely rare, if not virtually unheard of, for an outsider to reside within a Hutterite colony.Reference Evans and Peller13 Furthermore, it is uncommon for Hutterites to leave their colony and live elsewhere. A previous study examining psychoses among the Hutterite population in Manitoba utilised a similar method to elucidate Hutterite status using postal codes and addresses of known colonies.Reference Nimgaonkar, Fujiwara, Dutta, Wood, Gentry and Maendel12
Analysis
We used a multistep approach to stratify and analyse the data collected from the retrospective chart review. Only data from de-identified cases of subglottal stenosis between the years of 2008 and 2018 (10-year period) were collected, along with the age at time of diagnosis, postal code of the home address provided (location), gender and previous family history of idiopathic subglottic stenosis. We then determined the Hutterite status of the patient by matching the address and postal code of each patient to the address and postal codes of the colonies listed in the directory, and subsequently grouped the patients as Hutterite and non-Hutterite. Similarly, the rural and urban distribution of the patients based on the postal codes was determined, and patients were grouped into rural and urban, respectively. Based on the family history, patients were grouped into those with and without family history.
Descriptive statistics were used for data stratification by calculating measures of central tendency (mean) and measures of spread (range, frequency distribution, quartiles). Mean age at the time of idiopathic subglottic stenosis diagnosis in the Hutterite and non-Hutterite groups was determined. Similarly, the number of cases and the range of age (maximum age minus minimum age) at the time of idiopathic subglottic stenosis diagnosis, for the Hutterite and non-Hutterite groups and the groups based on family history, were determined. One-way analysis of variance tests were conducted to determine whether a significant difference existed in mean age at diagnosis between different groups. These groups included Hutterite versus non-Hutterite and positive family history versus negative family history. The Shapiro–Wilk test was employed as the test of normality.
As descriptive statistics only allowed us to make summations about the cases that had been actually studied, inferential statistics were used, in which data were taken from the samples to make generalisations about a larger population and its groups (Hutterite and non-Hutterite groups). Inferential statistics were used to determine the likelihood of occurrence by calculating the cumulative incidence and the measure of association, as reflected by odds ratio and risk ratio values.
Results
Of the 80 subglottic stenosis patients (66 females and 14 males) included in the study, 36 cases (45.0 per cent) were determined to be idiopathic. All of the idiopathic patients were female. Despite the Hutterites accounting for only 0.57 per cent of the Saskatchewan population, they represented 11.1 per cent of cases (4 out of 36 cases). Additionally, 30.6 per cent of patients with idiopathic subglottic stenosis (11 out of 36) had a concurrent diagnosis of gastroesophageal reflux disease or were being treated for a suspected case.
Age-based distribution
The mean, median and range (maximum minus minimum) of age values at diagnosis for the Hutterite group were 50, 47 and 34 years, respectively. In the non-Hutterite group, the mean, median and range of age values at diagnosis were 50.1, 50.5 and 48 years. There was no significant difference in age at diagnosis between the two groups (p = 0.98409).
Family-based distribution
A positive family history was only observed in the Hutterite population. Three out of four patients reported a positive family history (75 per cent). One pair of sisters was captured in this study. Cases with a positive family history demonstrated mean, median and range of age values at diagnosis of 43.3, 37 and 21 years, respectively. In the group with a negative family history, the mean, median and range of age values at diagnosis were reported as 50.7, 51 and 48 years, respectively. Family history was not associated with an earlier age at the time of diagnosis (p = 0.29566).
Location-based distribution
Eighteen of 36 cases (50 per cent) occurred rurally, and the remaining 18 cases (50 per cent) were found in the urban setting. In the urban group, the mean, median and range of age values at diagnosis were 47.3, 46.5 and 48 years, respectively. The mean, median and range of age values at diagnosis in the rural group were 52.8, 52 and 42 years. Location was not associated with an earlier age at diagnosis (p = 0.15225).
Cumulative incidence
The cumulative incidence of idiopathic subglottic stenosis was 0.00064 (n = 6250) in the Hutterite population and 0.000029 (n = 1 093 750) in the remainder of the Saskatchewan population. Belonging to the Hutterite group influenced the development of idiopathic subglottic stenosis in an individual (chi-square (1 degree of freedom) = 70.832, p < 0.001).
Odds ratio and risk ratio
The odds ratio of 21.89 indicates that the odds of developing idiopathic subglottic stenosis are 21.89 times higher in Hutterites than in non-Hutterites (95 per cent confidence interval = 7.74–61.9). A risk ratio of 21.88 was also calculated. It is assumed that the prevalence of a rare disease like idiopathic subglottic stenosis is low and therefore the odds ratio approaches the relative risk or risk ratio if the rare disease assumption holds.
Discussion
Our results are similar to previous studies that demonstrate a strikingly homogeneous population afflicted by idiopathic subglottic stenosis, generally healthy women in their fifties.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6–Reference Benjamin, Jacobson and Eckstein9 While the pathophysiology remains uncertain, female preponderance and the age at diagnosis of approximately 50 years suggest involvement of menopause-associated hormonal changes.Reference Dedo and Catten8,Reference Benjamin, Jacobson and Eckstein9 It has been postulated that oestrogen and/or progesterone act as mediators promoting collagen deposition in the upper airway. Imbalance between oestrogen and progesterone receptors in idiopathic subglottic stenosis patients has been demonstrated through surgical specimen analysis.Reference Fiz, Bittar, Piazza, Koelmel, Gatto and Ferone19
Other hypotheses, though not proven, include sequela of gastroesophageal reflux, subtle manifestations of collagen vascular disease, immunoglobulin G4 related disease, and an anatomically smaller and susceptible female subglottic region.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6 In our study, 11 of the 36 patients with idiopathic subglottic stenosis (30.6 per cent) had a concurrent diagnosis of gastroesophageal reflux disease or were being treated for a suspected case. Interestingly, these patients did not demonstrate more aggressive or severe stenosis. Furthermore, the absence of idiopathic subglottic stenosis in men and the rarity of idiopathic subglottic stenosis make gastroesophageal reflux disease an unlikely cause.Reference Aarnæs, Sandvik and Brøndbo7
• Idiopathic subglottic stenosis is a rare disease characterised by narrowing of the subglottic region of the larynx, most commonly found in peri-menopausal women
• The cumulative incidence of idiopathic subglottic stenosis is much higher in the Saskatchewan Hutterite population than the general population
• The unique genetic isolation of the Hutterite population may be contributing to development of this condition
• The study results strengthen the hypothesis of a genetic predisposition for idiopathic subglottic stenosis development
A founder effect in the Hutterite population has been suggested to account for the over-representation of several genetic diseases.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15 The small number of common ancestors likely accounts for the introduction of rare alleles and the manifestation of autosomal recessive conditions in the Hutterite population.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15,Reference Hostetler16 Furthermore, the Hutterites are known to keep extensive genealogical records, which have facilitated the mapping and identification of a number of autosomal recessive genes in their population.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15 Examples include the genes for limb-girdle muscular dystrophy (LGMD2H) and Usher syndrome (USH1F), among others.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15,Reference Shokeir and Rozdilsky20 Additionally, a number of autosomal recessive conditions and complex disorder traits have been studied.Reference Boycott, Parboosingh, Chodirker, Lowry, McLeod and Morris15,Reference Hostetler16,Reference Lowry, Morgan, Holmes and Gilroy21,Reference Pearce, Mackay, Holmes, Morgan, Fowlow and Shokeir22
As mentioned before, several cases in the literature have emerged suggesting an underlying genetic predisposition for the development of idiopathic subglottic stenosis.Reference Linna, Hyrynkangas, Kaukola and Pajunen5,Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6,Reference Dumoulin, Stather, Gelfand, Maranda, Maceachern and Tremblay10,Reference Abbasi Dezfouli, Shadmehr and Sheikhy11 Our results strengthen this hypothesis by presenting yet another pair of sisters afflicted by idiopathic subglottic stenosis, and by demonstrating that the cumulative incidence of idiopathic subglottic stenosis is much higher in the genetically isolated Hutterite population than in the Saskatchewan general population. However, the typical mature age of presentation for idiopathic subglottic stenosis argues against a sole genetic cause.Reference Gelbard, Donovan, Ongkasuwan, Nouraei, Sandhu and Benninger6 Furthermore, no specific gene has been identified in the development of idiopathic subglottic stenosis.
It is likely that the aetiology of idiopathic subglottic stenosis is multi-factorial and that genetics may simply predispose a patient to the development of subglottic stenosis later in life, when the body undergoes dramatic fluctuations in hormone levels. Possible genetic mechanisms may include abnormal cartilage growth and deposition, increased susceptibility to autoimmune or inflammatory mediators, action of specific growth factors, and/or different responses to chondral and mucosal injury.Reference Manickavasagam, Yapa, Bateman and Thevasagayam4 Perhaps the imbalance between oestrogen and progesterone receptors that has been demonstrated in idiopathic subglottic stenosis specimen analysis has an underlying genetic link. Identifying a specific gene and the exact physiological process through which it influences the development of idiopathic subglottic stenosis represents an interesting research challenge. Working with the Hutterite population could be an exciting next step in understanding idiopathic subglottic stenosis and its resolution.
Limitations
Patients with mild disease were likely missed in our study as they would not have been referred to our centres for management by an otolaryngologist. This would estimate the incidence to be slightly lower than it actually is. Furthermore, the small number of patients with idiopathic subglottic stenosis resulted in an odds ratio with a large confidence interval, making it difficult to precisely determine the increased odds of a Hutterite developing idiopathic subglottic stenosis. Nevertheless, our results indicate that development of idiopathic subglottic stenosis is significantly more likely in the Hutterite population compared with the Saskatchewan general population.
Conclusion
Idiopathic subglottic stenosis is a recurring, dangerous and costly disease that afflicts a very small percentage of the population. Research for rare conditions is often overlooked, as the vast majority of resources are used to investigate common diseases and conditions. This means that patients afflicted by rare diseases such as idiopathic subglottic stenosis are at a significant disadvantage when it comes to novel therapies, basic understanding of their particular condition and provision of support.
Our study aimed to provide insight into the aetiology and epidemiology of idiopathic subglottic stenosis among the Saskatchewan population. The study demonstrates, for the first time, that the cumulative incidence of idiopathic subglottic stenosis is much higher in a specific subpopulation, the Saskatchewan Hutterite population, when compared with the general population. We hypothesise that the unique genetic isolation of the Hutterite population may be contributing to the development of this condition. Our results strengthen the existing hypothesis that there is a genetic predisposition for the development of idiopathic subglottic stenosis. Together, the increased cumulative incidence, the positive family history for three of our four Hutterite cases, and a pair of afflicted sisters are in line with findings of previous studies. This leads us to hypothesise a putative genetic component to idiopathic subglottic stenosis.
Further research into identifying the exact genetic link for the development of idiopathic subglottic stenosis is the next step, for which work with the Hutterite population is warranted. This future research has the potential to improve the quality of life for patients affected by idiopathic subglottic stenosis, by providing future clinicians with new tools for prevention and treatment.
Competing interests
None declared


 Open access
Open access