



Introduction
Globally, one in six children are classified as overweight or obese(1) with higher rates reported in New Zealand and Australia where one in three children in New Zealand, and one in four children in Australia are classified as overweight or obese(1–3). Habitual dietary intakes and nutrition behaviours developed during childhood and adolescence pave the way for similar behaviours to manifest in adulthood(4,Reference Movassagh, Baxter-Jones and Kontulainen5) . However early modification in eating behaviours might decrease the risk of obesity and diet-related disease. Evidence suggests that altering the food environment offers opportunities for children to adopt healthier behaviours and seems to be an effective strategy to prevent childhood obesity(Reference Brug, van der Ploeg and Loyen6,Reference Sawyer, van Lenthe and Kamphuis7) . Given that children spend much of their weekday waking hours at school, alterations to the school food environment may provide an opportunity to improve dietary behaviours(Reference Carter and Swinburn8). School food provision in New Zealand and Australia is similar, where children may purchase food and beverages during break times (morning tea and lunch) from the school canteen which may be catered for internally by the school or by external food suppliers such as local bakeries and convenience stores. The majority of schools in New Zealand and Australia are publicly funded, meaning that government school food environment policies have significant potential to improve targeted dietary behaviours(Reference Micha, Karageorgou and Bakogianni9). However, in New Zealand and Australia, evidence suggests that schools do not encourage healthy food and drink consumption(Reference Carter and Swinburn8), with poor implementation of food policies(Reference Vandevijvere, Mackay and D’Souza10,Reference Mansoor, Ali and Richards11) , unhealthy food and drink availability using canteen profit models(Reference Carter and Swinburn8,Reference Wyse, Wiggers and Delaney12,Reference Billich, Adderley and Ford13) and a time-scarce curriculum with little room for nutrition education(Reference de Vlieger, Riley and Miller14,Reference Rapson, Conlon and Ali15) . It is therefore unsurprising that children consume more unhealthy foods on school days compared with non-school days(Reference Rockell, Parnell and Wilson16).
Within New Zealand, previous legislation sought to improve the food environment in schools. In 2008, all government-funded schools were required to promote healthy food choices and have only healthy options available where food and beverages were sold on school premises(Reference Gorton, Eyles and Mhurchu17,Reference Cushman18) . Despite a 66% uptake of this legislation(Reference Cushman18), following a change in government in 2009 the requirement for only healthy food options was removed, placing the onus on the school boards of trustees to mandate healthy food and drinks within schools(Reference Gorton, Eyles and Mhurchu17,Reference Cushman18) . More recently, New Zealand schools have used the Food and Beverage classification system (FBCS) to guide decisions about which foods to provide within schools, with the majority of schools still providing unhealthy food options at cheap prices(Reference Carter and Swinburn8,Reference D’Souza19) . The FBCS utilised a three-tier approach classifying foods as ‘every day’ (such as sandwiches and vegetables), ‘sometimes’ (such as pizza and muffins) and ‘occasionally’ (such as pastry and deep-fried items)(20).
Superseding the FBCS, the New Zealand government introduced the Healthy Food and Drink Guidance for Schools in 2020 with the aim to improve the food environment within schools(21). This voluntary guidance utilises a traffic-light classification system to categorise foods as ‘green’, ‘amber’ or ‘red’. Many Australian states have also adopted a state-school-mandated traffic-light system with varying recommendations for the degree of ‘green’, ‘amber’ and ‘red’ food availability (Table 1)(Reference Rosewarne, Hoek and Sacks22). Although one of the most effective food-labelling systems to aid consumer understanding of nutrition is the traffic-light system(Reference Borgmeier and Westenhoefer23,Reference Kelly, Hughes and Chapman24) , evidence suggests that this does not necessarily translate into healthy consumer purchasing and consumption behaviours(Reference Borgmeier and Westenhoefer23). Alternatively, the Healthy Food and Drink Guidance for Schools suggests increasing the availability of ‘green’ foods, which provide a good source of nutrition such as fruits, vegetables and wholegrains, limiting ‘amber’ foods, which provide some nutritional value (usually defined with a Health Star Rating >3·5) such as white bread and processed meats, and avoiding ‘red’ foods, which have poor nutritional value such as pastries, confectionary and sugar-sweetened beverages(21). Prediction models suggest that limiting unhealthy foods and increasing healthy food options to at least 70% of the total menu will result in the majority of children’s food purchases (>50%) being healthy(Reference Clinton-McHarg, Janssen and Delaney25). Previously however, even when New Zealand schools restricted the availability of foods considered ‘sometimes’ and ‘occasional’ foods, these still accounted for a high proportion of total sales(Reference Walton, Waiti and Signal26). Since its implementation, only one study has assessed school compliance with the new Ministry of Health Food and Drink Guidance for Schools in New Zealand(Reference Pillay, Piddington and Ali27). Similar traffic-light guidance has been implemented in Australia with variable uptake across states and territories despite being mandated in several states(Reference Silva-Sanigorski, Breheny and Jones28–Reference Woods, Bressan and Langelaan30).
Table 1. Food and drink policies in New Zealand and Australia for studies included in this review
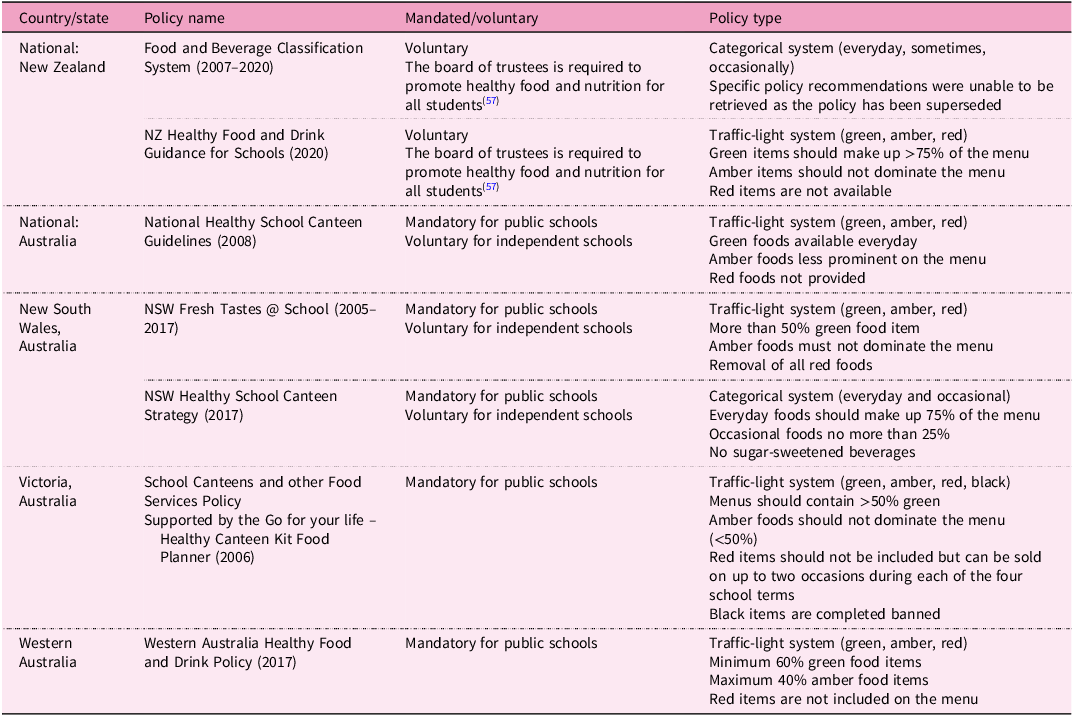
NZ, New Zealand; NSW, New South Wales.
Given that Australian schools closely resemble the structure of New Zealand schools with regard to canteen models and school hours, an assessment of the level of implementation of Australian traffic-light school policies may provide useful insights for expected implementation in New Zealand. A systematic review previously assessed the compliance of healthy canteen policies for Australian schools utilising data up to January 2015(Reference Lawlis, Knox and Jamieson31) but did not assess the implications for food purchase and consumption by students. Investigating to what extent government school food guidelines are implemented within schools and how this impacts children’s food choices can help inform future policy in New Zealand, particularly around mandating the Healthy Food and Drink Guidance and/or re-introducing the ‘healthy food only’ clause of the National Administration Guidelines in New Zealand.
Objectives
The aim of this review is to evaluate the effectiveness of government-implemented school food guidance on school food availability, canteen purchasing and consumption in New Zealand and Australian primary, intermediate and secondary schools. The following research questions were developed:
-
1. Do government-implemented school food guidelines increase the healthiness of the foods available for purchase by students from school canteens, vending machines and/or other outlets within New Zealand and Australian primary, intermediate and secondary schools, and what are the enablers and barriers to successful implementation?
-
2. Does improving the healthiness of foods available to purchase within New Zealand and Australian primary, intermediate and secondary schools decrease unhealthy food and drink purchasing and consumption (reduction of sugar-sweetened beverages and/or reduction of foods high in sugar/fat and/or ‘red’/‘amber’ traffic-light food) by students within school hours?
Methods
Study design
This study used a systematic approach to retrieve and select relevant literature. A guide to conducting integrative reviews was used to develop and inform the different sections of this review(Reference Toronto and Remington32).
Search strategy
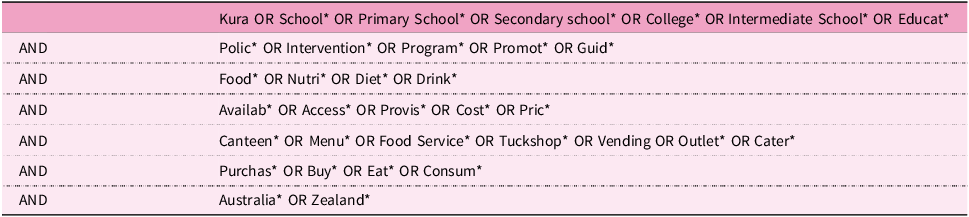
A search strategy was developed in consultation with the research librarian at Massey University. A comprehensive literature search was conducted on 2 February 2024 and updated on 8 August 2024 with three electronic databases, Scopus, PubMed and the Cochrane Library, and included published data up to August 2024. An advanced search of all fields including MeSH headings was conducted using the search terms and strings outlined in Tables 2 and 3 for each of the respective research questions. All results were exported into Endnote software, and duplicates were removed using automation and then manually verified to ensure accuracy. Studies were independently screened by two researchers on the basis of title and abstract. Any discrepancies were resolved through discussion to reach a unanimous decision. Full-text articles were sought for relevant literature. Forward and backward citation screening of the selected studies was used to identify additional studies.
Table 2. Search terms and strings used in the integrative review: food availability

Table 3. Search terms and strings used in the integrative review: food purchasing and consumption
Study selection
For all potentially relevant articles, full texts were retrieved and assessed against the inclusion and exclusion criteria. Studies were considered if they described school food availability and had school food guidelines, policies or programmes that were in line with government school food policies at the time of publication. Schools were defined as providing primary, intermediate or secondary education.
For inclusion, schools needed to provide a canteen-based or similar food-purchasing provision system such as tuck-shops and/or vending machines. When assessing food purchasing and consumption, studies were included if they described student food purchasing or consumption within the school with specific reference to a traffic-light scheme (‘red’, ‘amber’, ‘green’ categorised foods) or a clearly defined categorisation of healthy or unhealthy foods such as ‘foods high in sugar’, ‘foods high in fat’ and ‘sugar-sweetened beverages’ (SSB) as per country-/state specific guidelines. Studies were restricted to the New Zealand and Australian context. Studies were excluded if there was no assessment of food and beverage availability and/or they focused only on changes to knowledge/attitudes of key stakeholders within schools. Early childhood education and tertiary institutions were excluded. Schools provided with free school lunches or those that had described free food provision such as free fruit or charitable donations were excluded due to the reduced control that schools had over the provision of these foods. Review papers (systematic, meta-analyses, narrative) were removed during the screening process; however, the reference lists of relevant review articles were still assessed to identify additional studies pertinent to the present review. There were no restrictions on study design or publication date, except that grey literature was excluded to enhance the strength of the review by utilising peer-reviewed publications only. The inclusion criteria limited papers to those published in the English language.
The PRISMA flow diagram(Reference Page, McKenzie and Bossuyt33) was used to document the number of articles at each stage for the two separate searches regarding food availability, and food purchasing and consumption (Figure 1).
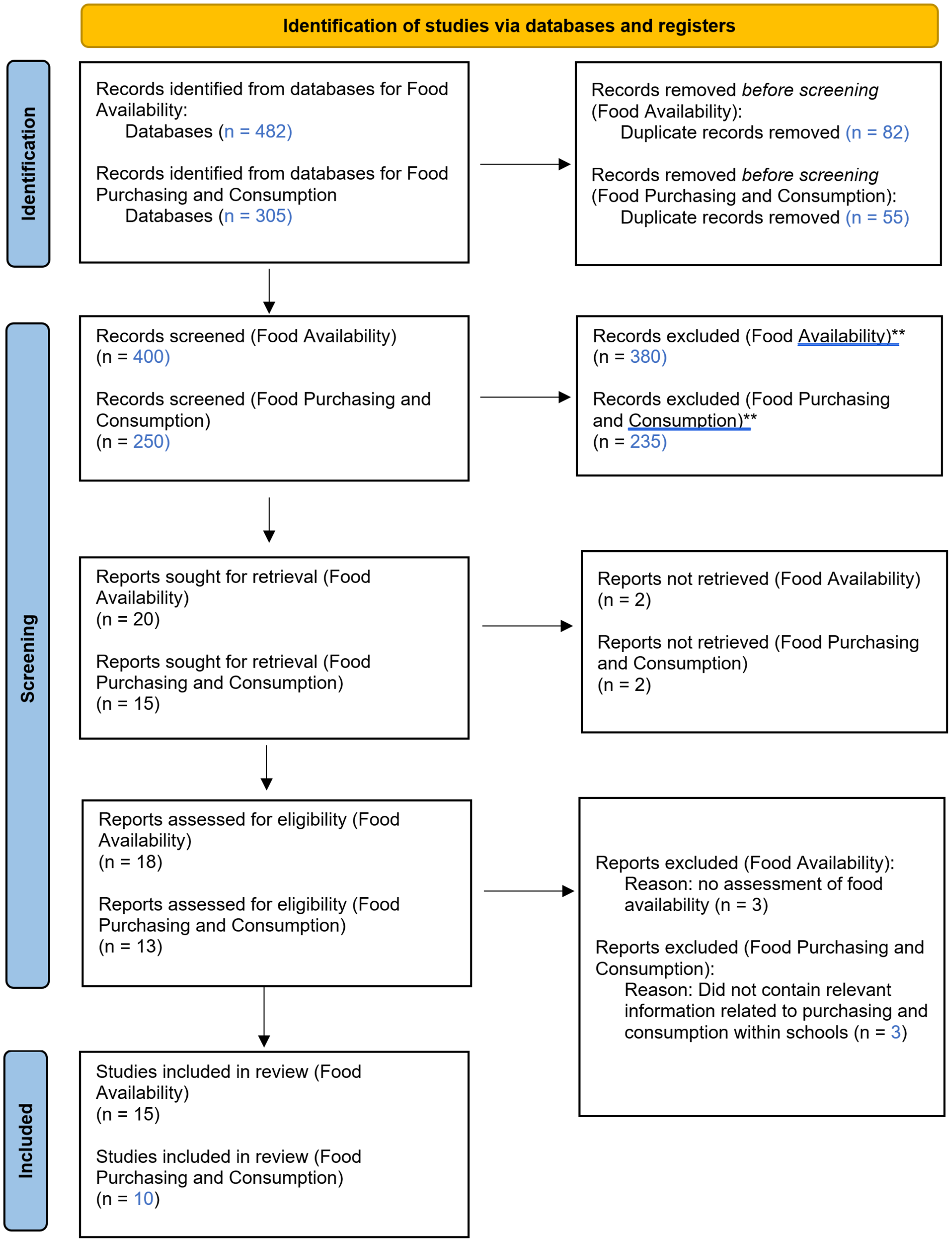
Figure 1. PRISMA flow diagram for study selection for (a) food availability and (b) food purchasing and consumption in New Zealand and Australian schools. **Records screened on the basis of title and abstract.
Methodological quality assessment
The studies included in this review were all assessed for methodological quality using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist(Reference Moola, Munn and Tufanaru34) for cross-sectional analyses, cohort studies and randomised controlled trials, as deemed appropriate. The risk-of-bias evaluation was used to help evaluate the quality of evidence from each study but not to exclude any studies from this review. This assessment was undertaken by the primary researcher.
Analysis
Data analysis was conducted by one researcher using a general inductive approach to systematically organise, analyse and describe the datasets. The process involved familiarisation with the dataset, generating initial codes and summarising key findings. NVivo version 13 (Lumivero 2020) software was used to assist in coding and organising the data. Coding was data-driven and guided by the review questions, with initial codes generated on the basis of recurring themes and concepts in the data. These codes were then refined to align with the research objectives. The data were then exported and aggregated manually to find commonalities and differences between the articles. Data were summarised and described in relation to the present research objectives, focusing on key barriers as factors that hinder or restrict effective school food availability and purchasing, and enablers as factors that enhance or support the school food environment.
Results
Food availability within schools
Study designs and population
The screening process revealed a significant gap in data on school food availability and compliance with healthy school food guidance in New Zealand. Most of the studies analysed focused on adherence to Australian school food guidelines (n = 13), while only two studies from New Zealand reported on food availability in schools(Reference Pillay, Piddington and Ali27,Reference Carter and Swinburn35) (Table 4). The number of menus analysed varied, with at least 38 schools(Reference Clinton-McHarg, Janssen and Delaney25) and up to 265 schools at most(Reference Hill, Nathan and Robinson36). While most studies examined compliance with territory-specific school food guidance, five also proposed interventions to promote healthy food environments within schools. These interventions included multi-component strategies that involved direct audit and feedback models for schools(Reference Reilly, Nathan and Wiggers37–Reference Yoong, Nathan and Wolfenden40), as well as incentive schemes such as the Heart Foundation Heartbeat Award (Reference Carter and Swinburn35). Dietitians and/or nutritionists were primarily involved in assessing and coding school menus on the basis of the specified criteria of the school food guidance.
Table 4. Studies assessing food policies and school food availability in New Zealand and Australia
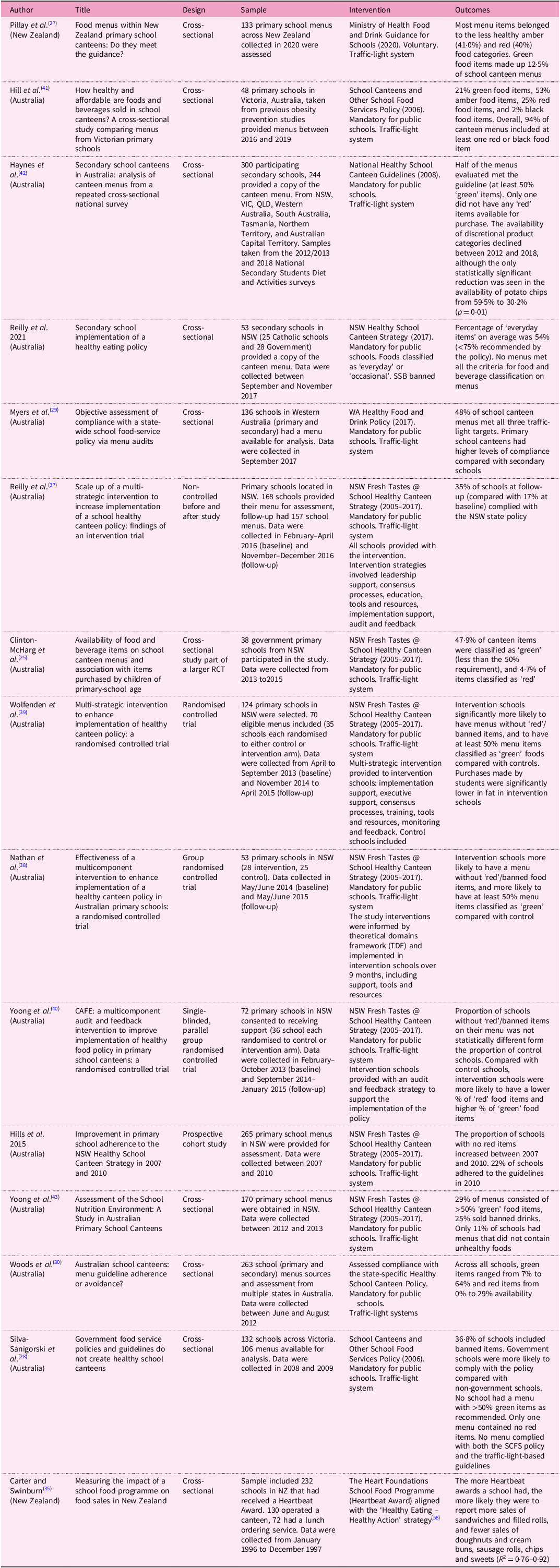
NZ, New Zealand; NSW, New South Wales; VIC, Victoria; QLD, Queensland; WA, Wales; RCT, randomised controlled trial; TDF, theoretical domains framework; SCFS, School Canteens and Other Food Services.
Study quality and risk of bias
Overall, the quality of the eleven cross-sectional studies was assessed as high, meeting more than 75% of the JBI(Reference Moola, Munn and Tufanaru34) criteria (Supplementary File A), with well-defined methodologies and appropriate analyses. The identification and control for confounding factors was limited among five of the included studies(Reference Pillay, Piddington and Ali27,Reference Myers, Sauzier and Ferguson29,Reference Woods, Bressan and Langelaan30,Reference Carter and Swinburn35,Reference Reilly, Nathan and Wiggers37) , whereas others employed multivariable regression models for better confounder control. Outcome measurements were consistently clear, assessing compliance with state-/country-specific healthy food and drink policies. There was only one cohort study assessed as having moderate levels of bias due to a lack of clarity around exposure measurements and follow-up(Reference Hill, Nathan and Robinson36). The three randomised controlled trials were assessed as having low levels of bias(Reference Nathan, Yoong and Sutherland38–Reference Yoong, Nathan and Wolfenden40). Due to the proposed interventions, it was not feasible for schools to be blinded to their ‘treatment’ arm. School canteen menus were provided by canteen managers, which may introduce reporting bias; however, this was done prior to randomisation into control or intervention arms, which may have lessened the effect. All menus were analysed by dietitians blind to allocation groups using validated methods to reduce assessment bias.
Compliance with government healthy food guidelines for schools
Compliance with healthy school food guidelines across all studies was low. On average, ‘green’ food items represented between 12·1% and 70·0%, ‘amber’ food items between 28% and 57·7% and ‘red’ food items between 2% and 40% on the basis of menu analyses completed by dietitians according to the state-/country-specific school food policy. New Zealand schools had the lowest compliance with the healthy food and drink policy with up to 40% of canteen menu items categorised as ‘red’ food items(Reference Pillay, Piddington and Ali27). In Australia, a recent assessment of Victorian schools found that 94% of school menus still contained a ‘red’ or ‘banned’ food item(Reference Hill, Blake and Alston41). Schools in Western Australia had the highest levels of compliance with healthy food and drink policy with 48% of school canteen menus meeting all three traffic-light targets (≥60% ‘green’ items, ≤40% ‘amber’ items and no ‘red’ items)(Reference Myers, Sauzier and Ferguson29). Western Australia is the only state to set clear targets on the proportion of menu items that may be offered in each traffic-light category as opposed to qualitative descriptions such as ‘majority to be green’(Reference Myers, Sauzier and Ferguson29), and this may have led to higher compliance.
Barriers to a healthy school canteen
Socioeconomic deprivation
Schools in affluent areas across Australia had lower odds of offering ‘red’ food items such as sugary drinks, meat pies and other savoury pastries(Reference Haynes, Morley and Dixon42). Similarly, logistic regression models found that schools in lower socioeconomic areas in Victoria, Australia were 1·3 times more likely to have ‘red’ food items on the menu compared with schools in higher-socioeconomic areas(Reference Hill, Nathan and Robinson36). A modest but significantly lower percentage of ‘green’ food items were also found in New Zealand schools in areas of high deprivation compared with those in areas of low deprivation (14·2% versus 8·6%)(Reference Pillay, Piddington and Ali27). Although not statistically significant, similar results were reported in New South Wales (NSW) schools, where a smaller proportion of schools in disadvantaged areas reported having a menu that primarily consisted of healthier items(Reference Yoong, Nathan and Wyse43).
School characteristics
Medium-sized schools across Australia had lower odds of offering potato chips and other packaged savoury snacks, as well as sugary drinks compared with small schools(Reference Haynes, Morley and Dixon42). Similarly, the odds of having a ‘red’ item on the menu was 1·9 times higher for small schools compared with large schools in Victoria(Reference Hill, Nathan and Robinson36). Small schools in New Zealand also provided a lower percentage of ‘green’ foods (7·1%) and a higher percentage of ‘red’ foods (61·5%) compared with medium and large schools(Reference Pillay, Piddington and Ali27). The odds of having ‘red’ food items were higher in non-government schools and rural schools in Victoria(Reference Hill, Nathan and Robinson36). However, an earlier and similar study in Victoria reported no significant differences in school food menus in government and non-government schools(Reference Silva-Sanigorski, Breheny and Jones28). Secondary schools across multiple Australian states were less likely than primary schools to meet the requirements of the healthy food and drink policy, and more likely to offer ‘red’ food items on their school menus(Reference Silva-Sanigorski, Breheny and Jones28–Reference Woods, Bressan and Langelaan30).
Variability in school guidelines
School-based guidelines and policies regarding the availability of nutritious food options show considerable variation(Reference Clinton-McHarg, Janssen and Delaney25,Reference Haynes, Morley and Dixon42) . Some policies prohibit the sale of specific products such as soft drinks, while others place limits on the proportion of unhealthy foods such as deep-fried items(Reference Clinton-McHarg, Janssen and Delaney25). Recommendations for menu composition also differ, ranging from strict requirements for a majority of ‘everyday’ options to more flexible guidelines suggesting at least 50% of healthier choices(Reference Haynes, Morley and Dixon42). However, all policies agree on not selling ‘red’ foods and certain energy-dense, nutrient-poor items like confectionery and sugary drinks. The classification of sugary drinks varied across Australian states, with some definitions encompassing a wider range of beverages(Reference Haynes, Morley and Dixon42). Notably, while the healthy food and drink policy for schools is mandated in most states of Australia, there is currently no monitoring or consequences in place for schools that fail to uptake and adhere with these guidelines(Reference Nathan, Yoong and Sutherland38).
Enablers of a healthy school canteen
Improved availability, clear targets and monitoring systems
Limiting the availability of foods and beverages with low nutritional value or increasing the availability of products with high nutritional value could have a positive impact on child nutrition. General linear models predicted that, as the availability of healthier items on a canteen menu increased, so did the purchasing of these items(Reference Clinton-McHarg, Janssen and Delaney25). It has been suggested that, for the majority of students to purchase healthier foods, a menu would need to consist of over 70% ‘green’ items(Reference Clinton-McHarg, Janssen and Delaney25). Many Australian states have a defined amount of ‘green’ food items that should be available on the menu ranging from 50% to >75%, yet few define the proportion of ‘amber’ foods that should follow (Table 1).
Western Australia stands out from other states in Australia by setting clear and stringent targets for the proportion of menu items that can be offered in each traffic-light category(Reference Myers, Sauzier and Ferguson29). The criteria imposed in Western Australia have shown that having quantifiable targets (>60% ‘green’ items, <40% ‘amber’ items, and no red items) led to a greater level of success in compliance with the policy, particularly in primary schools (89% meeting that target)(Reference Myers, Sauzier and Ferguson29). Additionally, school principals are mandated to assess canteen menus each year and submit findings to the relevant government department, which has contributed to a high level of compliance. Enforcement is critical for policy adoption, implementation and subsequent impact(Reference Myers, Sauzier and Ferguson29,Reference Nathan, Yoong and Sutherland38) . Only two other Australian states, New South Wales and Queensland, had implemented monitoring systems, albeit on a voluntary basis and utilising self-assessment tools(Reference Clinton-McHarg, Janssen and Delaney25,Reference Haynes, Morley and Dixon42) , which may explain the lower level of compliance with the subsequent healthy food and drink policies for schools.
School characteristics
The provision and promotion of healthy food and drinks in schools can be influenced by several school characteristics. For instance, larger schools and those situated in affluent areas in NSW and across New Zealand offered more ‘green’ food items(Reference Pillay, Piddington and Ali27,Reference Hill, Nathan and Robinson36,Reference Yoong, Nathan and Wyse43) . However, other studies in NSW, including those by Nathan et al. (Reference Nathan, Yoong and Sutherland38) and Reilly et al. (Reference Reilly, Nathan and Wiggers37), found no significant association between school size and the availability of healthy food. By contrast, Haynes et al. (Reference Haynes, Morley and Dixon42) reported that large schools across several Australian states had lower odds of meeting the menu guideline of at least 50% green items compared with small schools. Primary schools in Western Australia were found to have higher compliance with canteen guidelines and were more likely to offer plain milk and fruit than secondary schools(Reference Myers, Sauzier and Ferguson29).
Several studies across NSW and Victoria(Reference Silva-Sanigorski, Breheny and Jones28,Reference Reilly, Nathan and Wiggers37,Reference Yoong, Nathan and Wyse43) found that government schools were more likely to have menus that comply with policies than catholic or independent schools. Government schools in NSW were also more likely to prioritise healthy food placement at eye level and implement comprehensive canteen policies, whereas non-government schools had lower odds of doing the same(Reference Yoong, Nathan and Wyse43). Both medium and large schools in NSW were more likely to position healthy foods prominently, with medium schools also implementing comprehensive canteen policies that covered pricing, promotion and availability of healthy options(Reference Yoong, Nathan and Wyse43).
Feedback models and incentivisation
Findings suggest that a multi-strategy intervention which includes training, performance monitoring, feedback, telephone and text-messaging support can improve schools’ implementation of healthy canteen policies(Reference Reilly, Nathan and Wiggers37,Reference Nathan, Yoong and Sutherland38) . In one study conducted in NSW, this type of intervention was found to be helpful by over 45% of canteen managers surveyed, with menu audit and feedback reports rated as the most helpful component(Reference Wolfenden, Nathan and Janssen39). Feedback models have the potential to influence school food availability and food sales. In New Zealand, the introduction of the Heartbeat AwardFootnote 1 resulted in an increase in sales of sandwiches and filled rolls, and a decrease in sales of doughnuts and cream buns(Reference Carter and Swinburn35). Audit and feedback cycles implemented in several Australian states were shown to be positively associated with a higher proportion of schools having menus without ‘red’ or ‘banned’ items, and with menus where more than 50% of items were classified as ‘green’ compared with schools that did not have any feedback models(Reference Reilly, Nathan and Wiggers37–Reference Yoong, Nathan and Wolfenden40). It is likely that more than one contact is needed to maximise the effectiveness of audit and feedback interventions and the use of telephone and text messaging support can enhance the scalability of the intervention, making it easier to implement on a larger scale.
Food purchasing and consumption
Study design and population
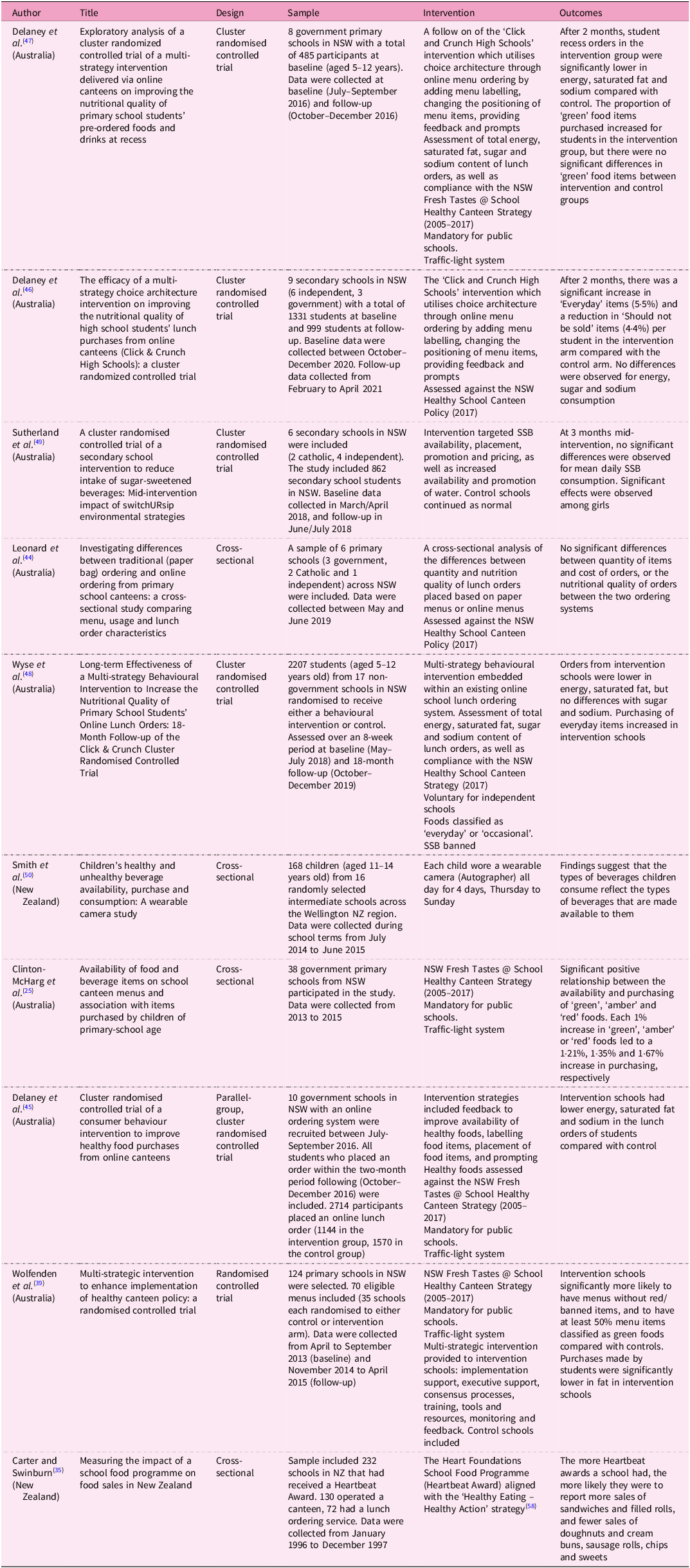
Ten studies were included in the exploration of strategies for enhancing school food environments and promoting healthier food purchasing and consumption (Table 5). Eight were conducted in Australia across several states, and two were conducted in New Zealand. One compared traditional and online canteen ordering, evaluating menu characteristics and nutritional content(Reference Leonard, Delaney and Seward44), while four studies modified online ordering systems to encourage healthier choices(Reference Delaney, Wyse and Yoong45–Reference Wyse, Delaney and Stacey48). Two studies implemented interventions using policy support, training and recognition(Reference Wolfenden, Nathan and Janssen39,Reference Sutherland, Ying Ooi and Finch49) . Additional studies employed implementation support strategies(Reference Carter and Swinburn35), used image data for assessment(Reference Smith, Stanley and Signal50) and conducted telephone interviews and menu audits to understand student purchasing behaviour and improve school food environments(Reference Clinton-McHarg, Janssen and Delaney25). Study populations differed depending on the aims of the intervention. Those where schools were the focus had a range of n = 6–202 schools participating, whereas those where students were the focus had a population of n = 158–2714 students.
Table 5. Studies assessing food policies and school food purchasing in New Zealand and Australia
NSW, New South Wales; SSB, sugar-sweetened beverages; NZ, New Zealand.
Study quality and risk of bias
Overall, the quality of the four cross-sectional studies were assessed as high, meeting 75% or more of the JBI criteria (Supplementary File A), with appropriate methodologies and analyses. Identification of confounding factors and controlling for these were limited in two out of the four studies(Reference Carter and Swinburn35,Reference Smith, Stanley and Signal50) , whereas the other two utilised multivariable regression models for better confounder control(Reference Clinton-McHarg, Janssen and Delaney25,Reference Smith, Stanley and Signal50) . There were six randomised controlled trials which were assessed as having low levels of bias(Reference Wolfenden, Nathan and Janssen39,Reference Delaney, Wyse and Yoong45–Reference Sutherland, Ying Ooi and Finch49) . Due to the type of interventions, which ranged from multicomponent feedback models for schools to modifications in online ordering systems, blinding of schools to their assigned ‘treatment’ arm was not feasible. Three studies used online software capturing student purchases which minimised reporting bias(Reference Leonard, Delaney and Seward44,Reference Delaney, Wyse and Yoong45,Reference Wyse, Delaney and Stacey48) , and four studies assessed purchasing through direct observation(Reference Clinton-McHarg, Janssen and Delaney25,Reference Wolfenden, Nathan and Janssen39,Reference Leonard, Delaney and Seward44) or wearable cameras(Reference Smith, Stanley and Signal50). One study used a validated online survey to assess nutritional intake(Reference Sutherland, Ying Ooi and Finch49), and another relied on staff-reported sales data(Reference Carter and Swinburn35) which may have introduced some reporting bias. To reduce assessment bias, all menus were analysed by dietitians who were blinded to the allocation groups and used validated methods.
Factors influencing food purchasing and consumption
Food availability
In a study involving thirty-eight schools in NSW, despite similar access to ‘green’ and ‘amber’ food items, ‘amber’ items were purchased at a significantly higher rate than ‘green’ items(Reference Clinton-McHarg, Janssen and Delaney25). General linear models indicated that, for students to favour ‘green’ items (>50% of purchases), the menu should consist of over 70% ‘green’ items (R 2 = 0·66). Additionally, each 1% increase in ‘green’, ‘amber’ or ‘red’ items led to a 1·21%, 1·35% and 1·67% increase in purchasing, respectively(Reference Clinton-McHarg, Janssen and Delaney25). The results suggest that restricting low-nutritional-value items or increasing high-nutritional-value options in a school canteen could significantly impact purchasing behaviours. An analysis where students in New Zealand used wearable cameras found that the availability of core drinks (water and milk) was twelve times that of non-core drinks (SSB: sugary carbonated beverages, flavoured milk, fruit juice or fruit smoothies) on school days and core beverages were more frequently consumed compared with non-core drinks(Reference Smith, Stanley and Signal50). Almost all (94·1%) the children’s purchases, however, were for non-core drinks whether within the school or outside the school(Reference Smith, Stanley and Signal50).
By contrast, in an analysis of online and paper-ordering canteen models in NSW, both systems offered similar proportions of ‘everyday’, ‘occasional’ and ‘should not be sold’ foods: online systems had 68% ‘everyday’, 17% ‘occasional’ and 15% ‘should not be sold’ foods, while paper systems had 67% ‘everyday’, 18% ‘occasional’ and 14.6% ‘should not be sold’ foods. There were no significant differences in the types of foods purchased between the two systems(Reference Leonard, Delaney and Seward44).
Healthy food promotion
Promoting healthy foods in canteens may have a positive effect on children’s food choices. Decreases in children’s consumption of saturated fat and total energy were observed when principles of ‘choice architecture’ were applied to online school-canteen ordering systems in NSW which included changes to menu labelling (using coloured symbols for ‘everyday’, ‘occasional’ and ‘caution’ or ‘green’, ‘amber’ and ‘red’ according to the state-specific food policy), positioning healthier foods more prominently, prompting for healthier food choices, incentives with a reward symbol or text and providing feedback to users on their choices(Reference Wyse, Wiggers and Delaney12,Reference Delaney, Wyse and Yoong45,Reference Delaney, Jackson and Lecathelinais47) . During an 8-week analysis of the intervention outcomes, notable differences emerged in the distribution of ‘green’ and ‘red’ items between the intervention and control schools(Reference Delaney, Wyse and Yoong45). Student purchases from the intervention schools displayed a significantly higher proportion of ‘green’ food items (51·21% compared with 37·93% in control schools) and a markedly lower proportion of ‘red’ food items (1·21% versus 11·11% in control schools)(Reference Delaney, Wyse and Yoong45). Despite similar availability in the online school-canteen ordering system, in a subsequent 18-month follow-up of the same intervention, the intervention schools exhibited a 3·8% increase in purchases of ‘everyday’ items and a corresponding 2·6% decrease in purchases of ‘caution’ items in contrast to the control schools, with no significant differences in ‘occasional’ food item purchasing(Reference Wyse, Delaney and Stacey48).
A similar intervention study in NSW which targeted an in-school canteen model aimed to change the availability and placement of SSB by removing them from eye level and displays, reducing the promotion of SSB, changing the price to make them more expensive compared with ‘occasional’ and ‘everyday’ beverages, and increasing the availability and promotion of water found that there were no significant changes to SSB consumption by students after a 3-month intervention period(Reference Sutherland, Ying Ooi and Finch49). Differences between the online-ordering system and the in-person canteen models could be attributed to consumption and environmental behaviours, particularly peer influence and personal preferences of students versus an online-ordering model where parents may have more control over foods purchased for the child.
School incentivisation
An evaluation of the Heartbeat Award, which New Zealand schools could earn if they improved the variety and nutritional value of the food provided within the school canteen, showed that more awards significantly correlated with increased sales of sandwiches and filled rolls (76·7% more), and decreased sales of unhealthy items such as doughnuts (28·4% less), pies (46·3% less), crisps (24·7% less) and sweets (26·8% less)(Reference Carter and Swinburn35). Schools participating in the programme over time and achieving subsequent Heartbeat awards reported further reductions in unhealthy food sales and increased sales of healthier options. Overall, the findings suggest that the Heartbeat Award programme in New Zealand positively impacted children’s food consumption by increasing the availability and sales of healthier options while reducing the consumption of unhealthy items.
Discussion
The aim of this review was to evaluate the effectiveness of government-implemented school food guidance on school food availability, canteen purchasing and consumption in New Zealand and Australian primary, intermediate and secondary schools. Findings revealed a low compliance with healthy school food guidelines across the studies, with few schools fully eliminating ‘red’/‘banned’ food items from school canteens. Contrasting guidelines across different territories meant that there were challenges to policy adherence and varying degrees of restrictions on specific products. However, there was an overall theme across the guidelines to remove ‘red’ and ‘caution’ foods altogether, making the healthy choice the only available option. Small schools, which tended to offer more ‘red’ food items on their menus, may need additional support compared with larger schools that generally have greater resources and capacity to implement healthy canteen initiatives.
Schools may have concerns that canteen profits and school revenue could be impacted by providing more healthy options and less unhealthy options which are more appealing to the demographic(Reference Ronto, Rathi and Worsley51). However, where canteen revenue was assessed in the present review, there were no significant changes to revenue over time between schools who had improved their school canteen, and those who had not(Reference Wolfenden, Nathan and Janssen39,Reference Delaney, Wyse and Yoong45–Reference Delaney, Jackson and Lecathelinais47) . This perceived school barrier could be appeased through pricing policies by implementing strategies to subsidise or reduce the cost of healthy menu items and disincentive ‘red’ food items by marking them up, subsequently encouraging healthier choices(Reference Billich, Adderley and Ford13).
The mode of delivery could also play a role in the food choices of children. Online versus in-person canteen models revealed differing outcomes from similar intervention strategies, possibly due to the influence of personal preferences, parental oversight and peer influences in the school environment. Online canteen ordering systems have the ability to implement promotional strategies, feedback and incentives and likely have parental oversight that would not be feasible for in-person models(Reference Delaney, Wyse and Yoong45,Reference Wyse, Delaney and Stacey48) . Peer modelling and education are potential strategies to work around this. Implementing peer-led campaigns showcasing healthy eating as the social norm could encourage students to opt for healthier choices at school as evidence suggests that children are more likely to engage in either healthy or unhealthy eating behaviours depending on what is favoured in their environment(Reference Ragelienė and Gronhoj52,Reference Smit, de Leeuw and Bevelander53) .
Concerningly, schools in marginalised areas were more likely to offer unhealthy food items on their school canteen menu compared with schools in affluent areas(Reference Pillay, Piddington and Ali27,Reference Hill, Nathan and Robinson36,Reference Haynes, Morley and Dixon42) . There is a strong association between neighbourhood deprivation and access to unhealthy food outlets in New Zealand(Reference Pearce, Blakely and Witten54). The density of junk food outlets and unhealthy food advertising around schools might create a challenging environment for school canteens, potentially discouraging the provision of healthy food items(Reference Walton, Pearce and Day55). Additionally, surveys indicate that children in areas of high deprivation are less likely to meet their fruit and vegetable intake targets and more likely to consume SSB and takeaways(56). This underscores the potential concerns in schools within the most neglected areas regarding the acceptability and familiarity of healthy foods. Addressing these disparities is essential for ensuring equitable access to nutritious food choices and could have the greatest positive impact in underprivileged areas.
Multi-component interventions are crucial given the complexity of implementing effective healthy food and drink policies in school settings. Theoretical frameworks such as the theoretical domains framework (TDF) and the diffusion of innovation theory provide a basis for understanding behavioural, contextual and organisational factors that influence policy implementation. The success of multi-component interventions that integrate leadership support and engagement, staff training and education, provision of tools and resources, and performance monitoring have been shown to improve the implementation of healthy food and drink policies within schools(Reference Reilly, Nathan and Wiggers37–Reference Wolfenden, Nathan and Janssen39). A key commonality among these theoretical frameworks for policy implementation is the use of feedback cycles and audits to support policy adoption and implementation. Addressing multiple elements, including the provision of necessary tools and human resources for monitoring rather than relying solely on policy implementation, can more effectively overcome barriers to change.
The Heartbeat Award programme in New Zealand highlighted the effectiveness of a school incentivisation scheme in promoting healthier options and reducing unhealthy consumption. Telephone-based monitoring and feedback systems could serve as a practical tool for ongoing support. Offering opt-in schemes that incentivise schools to participate could also foster a sense of accountability. Awards and recognition for schools that consistently maintain healthier canteen environments could further motivate schools to sustain their efforts. By coupling incentives with monitoring and feedback models, a culture of continuous improvement can be established, leading to lasting changes in school food environments.
Limitations
Several limitations must be considered when interpreting the findings of these studies. Self-selection bias is likely to have played a role in many of the reported studies. Self-report measures are susceptible to social desirability bias, wherein respondents may provide answers they perceive as aligning with the researcher’s expectations. As a result, school representatives and canteen managers providing reports on the healthfulness of their school menus and food availability may be more likely to be those who have a greater interest in health and nutrition and a stronger motivation to follow the policy compared with those who did not participate in the studies.
Although sourcing the menus directly from school websites/online sources may reduce self-reporting and sampling bias, it does then result in restrictions on the types of menus available. For example, not all schools have an online presence or their menu available for download, particularly under-resourced schools. Additionally, online menus may fail to display the full extent of the school menu, additional items for sale on certain days of the week and seasonal variances in menus, particularly in cross-sectional analyses taking data from one time point. This may provide bias towards a healthier canteen model, particularly if schools are aware that they are being monitored for their compliance of a healthy food and drink policy in that area.
All studies utilised a nutrition professional (either a nutritionist or dietitian) to analyse menus for compliance with a healthy food and drink policy. This is deemed the most appropriate way to accurately analyse a large group of menus. However, without additional information on ingredients, nutrient composition and cooking methods, many categorisations by the researchers were biased towards a more positive picture of the nutritional quality of canteen menus, particularly for ‘inconclusive’ menu items which in many circumstances were assigned to a healthier category/rating.
This review demonstrates several key strengths. It employed a systematic and comprehensive review approach which, developed in consultation with a research librarian, ensured a thorough examination of the literature. Selection bias was minimised through the independent screening of studies by two researchers which enhanced the reliability of study inclusion. The methodological quality of the included studies was also assessed using validated methods, adding robustness to the evaluation of the evidence. However, this review has several limitations that should be considered. The search strategy, although comprehensive, was restricted to three electronic databases which might not cover all relevant literature. Additionally, the decision to exclude grey literature might have overlooked valuable insights that are not published in peer-reviewed journals but still relevant to the topic such as PhD/Masters’ theses and government-led reports. The exclusion of early childhood and tertiary education institutions may also limit the generalisability of the findings. Due to the limited data available in New Zealand, and the significant contribution of data from Australia, in particular NSW, it is important to acknowledge that the findings may not reflect the unique context and challenges faced by schools in New Zealand.
Future directions
The generalisability of many of these studies is limited due to the variance in the healthy food and drink policies and small sample sizes. Although similarities in food provision systems in New Zealand and Australia are striking, the data suggest that there is a need for more comprehensive New Zealand-based studies to investigate food availability within schools, compliance with government guidance and the impact on student purchasing behaviours. Assessing the wider school food provision system may also provide insights particularly for special events, sports days and field trips where menu deviation may occur. Examining key stakeholder responses and canteen revenue in response to the school canteen policy changes may also yield valuable perspectives on acceptability and future compliance.
Recommendations for policy and practice
New Zealand’s limited research on school food environments highlights a need for more studies on this topic. Utilising data from Australian research provides valuable insights and strategies that can be applied to the New Zealand context, helping to improve the implementation and compliance with healthy school food policies. Key recommendations for policy and practice are outlined below:
-
Reinstate the clause in the National Administration Guideline for ‘only healthy food’ to be provided in schools, and mandate healthy food guidelines in schools.
-
Adopt stringent guidelines with clear targets for ‘green’, ‘amber’ and ‘red’ foods. Develop guidelines that help schools to strategically phase out unhealthy food items.
-
Increase targeted support and resources for schools in marginalised areas to address disparities and ensure equitable access to healthy food options.
-
Establish robust monitoring systems for compliance with healthy food policies such as annual or biannual reports and menu audits.
-
Provide schools with external support to implement healthy food policies including feedback models, training and resources, as well as support to assess the nutritional quality of foods available and to promote healthy foods in school canteens or through online-ordering systems.
-
Develop and encourage incentive schemes to motivate schools to comply with new food policies.
Conclusion
The analysis highlights the complexity of factors influencing school food availability, compliance with guidelines, and strategies to promote healthier food choices. While challenges such as varying guidelines and socioeconomic disparities persist, clear targets, multi-component interventions and school incentivisation emerge as promising strategies for creating healthier school food environments and influencing students’ food purchasing and consumption behaviours.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422424000362.
Authorship
D.P., C.W. and A.A. designed and conceptualised this review. D.P. and A.A. conducted the initial literature search. D.P. analysed the literature and wrote the first draft. D.P., C.W. and A.A. edited and reviewed the final version.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing of interests
The authors declare none.









 Open access
Open access