



Over the centuries, the twinning phenomenon has fascinated humans, and perceptions toward it have changed with societal evolution (Bhalotra & Clarke, Reference Bhalotra and Clarke2019; Chauhan et al., Reference Chauhan, Scardo, Hayes, Abuhamad and Berghella2010; Duncan, Reference Duncan1865; Newman, Reference Newman1941; Parisi, Reference Parisi2004; Polderman et al., Reference Polderman, Benyamin, De Leeuw, Sullivan, Van Bochoven, Visscher and Posthuma2015; Segal, Reference Segal2017; Smits & Monden, Reference Smits and Monden2011; Zeleny, Reference Zeleny1921). Some societies revered it in ancient times, whereas some were skeptical about it. In modern times, it has become a means for advancing genetic research to understand the role of nature and nurture (Boomsma et al., Reference Boomsma, Busjahn and Peltonen2002; Galton, Reference Galton1876). Moreover, the increased risk of prenatal and postnatal maternal complications and higher perinatal, neonatal and infant mortality rates associated with multiple births have made it a rising public health issue (Alam et al., Reference Alam, Van Ginneken and Bosch2007; Bdolah et al., Reference Bdolah, Lam, Rajakumar, Shivalingappa, Mutter, Sachs, Lim, Bdolah-Abram, Epstein and Karumanchi2008; Choi et al., Reference Choi, Bishai and Minkovitz2009; Guo & Grummer-Strawn, Reference Guo and Grummer-Strawn1993; Katz et al., Reference Katz, West, Khatry, LeClerq, Christian, Pradhan and Shrestha2001; Monden et al., Reference Monden, Pison and Smits2021; Pison et al., Reference Pison, Monden and Smits2015; Rauh-Hain et al., Reference Rauh-Hain, Rana, Tamez, Wang, Cohen, Cohen, Brown, Ecker, Karumanchi and Thadhani2009).
It is well known that the incidence of twinning varies across different demographic and geographic domains (Bulmer, Reference Bulmer1959, Reference Bulmer1970). In 1980−1985, Africa had the world’s highest twinning rate (16 per 1000 deliveries), followed by North America (9.9), Europe (9.1), South America (8.7), and lastly, Asia (7.0) (Monden et al., Reference Monden, Pison and Smits2021). Although in 2010-2015, ranks remained unchanged, North America and Europe witnessed tremendous growth of 1.7 times (9.9 to 16.9) and 1.6 times (9.1 to 14.4) respectively. In the meantime, Asia’s twinning rate grew only by 1.3 times (7 to 9.2), most of which can be attributed to East and West Asia. This makes South Asia one of the regions with the world’s lowest twinning rate (8.7), and Bangladesh is a part of it.
Twins can be monozygotic (same zygote) or dizygotic (different zygotes) (Hall, Reference Hall2003). The monozygotic (MZ) twinning rate is notably constant within the range of 3.5−4 twins per 1000 deliveries (Bulmer, Reference Bulmer1970). However, it is the dizygotic (DZ) twinning rate that varies with different factors such as maternal age, health, parity, education level, social class, ethnicity, season, and others. (Bortolus et al., Reference Bortolus, Parazzini, Chatenoud, Benzi, Bianchi and Marini1999; Duncan, Reference Duncan1865; Hall, Reference Hall2003; Nylander, Reference Nylander1981; Pison & d’Addato, Reference Pison and d’Addato2006; Shipley et al., Reference Shipley, Wray, Hechter, Arellano and Borhani1967). In addition, since 1970, medically aided reproduction has emerged as a prominent factor in the rise of twinning rate, especially for the global north (Blondel & Kaminski, Reference Blondel and Kaminski2002; Fell & Joseph, Reference Fell and Joseph2012; Monden et al., Reference Monden, Pison and Smits2021).
Twins are anticipated to be marginally compressed because they occupy a space that would ordinarily accommodate one child (Hall, Reference Hall2003). This is reflected in prematurity, fetal defects, low birth weight, undernutrition, respiratory and immunological problems (Gebremedhin, Reference Gebremedhin2015; Hong, Reference Hong2006; Suder et al., Reference Suder, Gniadek, Micek and Pawlik2021). As a result, neonatal, infant, and under-five mortality rates are found to be way higher in twins than in singletons, posing serious public health challenges in both the developing and developed world.
There are limited studies on twin births and their survival from the global south. Though few such studies exist for Bangladesh (Alam et al., Reference Alam, Van Ginneken and Bosch2007; Hong, Reference Hong2006; Nabeen & Akanda, Reference Nabeen and Akanda2017; Rahman et al., Reference Rahman, Islam and Howlader2020; Razzaque et al., Reference Razzaque, Ahmed and Wai1990), all of them are either spatially or temporally limited in extent. To fill this gap, this study analyzes the evolution of the twinning phenomenon over the last five decades (1970−2018) in Bangladesh. We compiled a database of about 0.29 million live births from all eight rounds of the Bangladesh Demographic and Health Survey (BDHS). First, we explored the decade-wise trend in twin, triplet and quadruplet births. We checked decadal twinning rates across different determining factors and quantified the association of a few at-birth demographic factors with twin maternities in Bangladesh. Second, we computed the decade-wise neonatal, infant and under-five mortality rates and estimated the survival pattern of singleton and multiple births using the Kaplan-Meier method. We also quantified the extent to which deaths in multiple births challenge Bangladesh’s exceptional progress in lowering child mortality. Lastly, we discuss the implications of a future scenario of multiple births in Bangladesh. To the best of our knowledge, this is the first country-level study from South Asia, a historically low twinning region, which utilizes half a century of evidence.
Materials and Methods
We constructed a database of 289,122 deliveries (unweighted) that occurred from 1970 to 2018 by pooling all eight BDHS rounds (1993−2018; NIPORT, Mitra and Associates, & Macro International., 1994, 1997, 2009; NIPORT, Mitra and Associates, & ICF International, 2013, 2016, 2020; Mitra and Associates, & ORC Macro, 2001, 2005). The BDHS used a two-stage sampling scheme to select households. The National Institute of Population Research and Training (NIPORT) implemented these surveys. Ethical approval was acquired from the National Research Ethics Committee of the Ministry of Health. A unique feature of BDHS data is sampling weights, which represent how many similar units in the target population are represented by each sample unit (ICF International, 2012). In general, these weights make the sample more like the target population. Hence, we considered them to make meaningful interpretations.
For analysis, we defined the decade-wise twinning rate as the number of deliveries resulting in twin births per 1000 deliveries of live births during a specific decade. The rate for triplet and quadruplet births is calculated for 100,000 deliveries. The BDHS does not contain information on the DZ and MZ twins. To estimate DZ and MZ twinning rates, we used Weinberg’s Differential Method, which identifies all the mixed-sex twins and an equal number of same-sex twins as DZ and the rest of same-sex twins as MZ (Weinberg, Reference Weinberg1901). This method’s assumption of an equal sex ratio at birth strongly exists in Bangladesh. We also checked the conformity of these rates with Hellin’s law, which states that if the frequency of twin birth is 1 per X births, then there will be one triplet birth per X2 births (Sel, Reference Sel2020).
To examine how twin births vary over different factors, we analyzed decade-wise twinning rates across maternal age at birth, parity, and season of birth. These are the only variables that contain at-birth information. Other factors, such as maternal BMI (a measure of body fat based on height and weight), education, household wealth status, geographic region, and locality (urban or rural), captured information at survey time. As a result, there is a time gap between the birth and data in these variables. For example, one third of Dhaka city’s population growth in the last three decades can be attributed to internal migration (Begum & Hossain, Reference Begum and Hossain2023), meaning maternal location at birth and survey might differ. This uncertainty grows as the time gap between birth and survey widens. The same applies to BMI, education, wealth status and locality, none of which are warranted to remain constant over time. In such a scenario, there is a high chance of underestimating or overestimating the rates. To overcome this issue, we restricted the sample to births that occurred a maximum of five years before the respective surveys (unweighted n = 57,333) to calculate twinning rates across these variables. We acknowledge that the aforementioned uncertainty also exists in this setup, but in a lower portion, as for most of the sample these variables should not drastically change in five years. In addition, we quantified the association of at-birth demographic variables — maternal age, parity, and season — with the incidence of twin births, using multivariate logistic regression. It is worth noting that these rates would have been higher if frequency of stillbirths were included, which is unavailable in the BDHS.
Next, we focused on neonatal, infant and under-five mortality between singleton and multiple births (not deliveries). Multiple births include twins, triplets and quadruplets, but as the frequency of triplet and quadruplet births is very low, the multiple birth rate is almost the same as the twinning rate. We explored how decade-wise survival probability varies over singleton and multiple births by examining Kaplan-Meier curves. We also checked the decade-wise share of multiple births in child mortality during neonatal, post-neonatal infant and post-infant under-five periods.
We concluded the study by discussing the future scenario of multiple births in Bangladesh in the face of changing maternal age at birth, parity, and socioeconomic conditions.
Results
Trends and Patterns in Twin Births
Table 1 presents decade-wise trends in Bangladesh’s singleton, twin, triplet and quadruplet birth rates for the last 50 years. The singleton birth rate largely remained constant over this period, whereas the twinning rate exhibited an upward trend. The twinning rate was 5.8 per 1000 deliveries in the 1970s and gradually rose to 8.6 in the 2010s. Still, it has one of the lowest twinning rates in the world (Monden et al., Reference Monden, Pison and Smits2021). Both types of twin births, MZ and DZ, increased over the last five decades. The MZ twinning rate ranged between 2.6 and 3.8. The DZ twinning rate jumped from 3.2 to 4.8 during this period.
Table 1. Singleton and multiple birth rate in Bangladesh, 1970−2018

Note:
* Rate per 100,000 deliveries for triplet and quadruplet;
** Parenthesis contains 95% confidence intervals.
In the weighted survey data, there were 4362 twin births and 60 triplet births out of 293,366 live births. This implies that there was one twin birth per 67 live births. Then, as per Hellin’s law, there should be one triplet birth per 4489 live births. In the weighted data, we found one triplet birth per 4889 live births, which is only 9% higher than Hellin’s prediction. So, our result is well in line with Hellin’s law. The number of quadruplets is too low to draw any meaningful conclusion.
Table 2 shows the variation in decade-wise twinning rates over different determining factors. The rate increased with advancing maternal age at birth. In the under-18 group, the twinning rate does not differ much by parity. But, in the 18−30 age group, the rate is higher for multiparae over decades. The twinning rate is highest for the over-30 multiparae group. There is an upward trend in the twinning rates by birth seasons, but not much difference is seen within them. Using the under-five sample, we observed that the twinning rate is higher for mothers who had higher body mass index (BMI) over the last three decades. We did not find any specific trends in twinning by maternal education. The twinning rate is somewhat higher for women living in rich households. The rate does not differ much between urban and rural localities.
Table 2. Twinning rate across different determining factors

Note:
* Under-five sample.
Figure 1 depicts the division-wise twinning rate for the time period 1990−2018. In this period, Sylhet had the highest twinning rate at 11 twin pairs per 1000 deliveries. Following Sylhet, Chittagong and Khulna had a twinning rate of about nine; Rajshahi and Mymensingh had a rate of about eight. In contrast, Rangpur had the lowest twinning rate of five and a half, followed by Dhaka and Barishal, with about seven twin pairs per 1000 deliveries. It seems the twinning rate is higher in bordering divisions (except for Rangpur).

Figure 1. Twinning rate across different administrative divisions in Bangladesh (pooled 1990−2018).
The extent to which three at-birth variables, maternal age at birth, parity and season impact twin births in Bangladesh are presented in Table 3. The odds of twin births gradually rise with age and peak beyond age 30. Smits and Monden (Reference Smits and Monden2011) noted that this rise starts to decline after age 38. However, we could not disaggregate our estimate for late reproductive age (40 and above) because only 0.34% of the births in our sample occurred in that maternal age group. The odds of twinning increase at higher parities. But, the seasons of births altogether remain insignificant.
Table 3. Impact of at-birth demographic variables on twinning

Note: Standard errors in parentheses.
***p < .001, **p < .01, *p < .05
Survival of Multiple Births
In the 1970s, the neonatal mortality rate in singletons was 89 per thousand live births, whereas the same for multiple births was 448 (Table 4). Both decreased over the next decades and in the 2010s, it was 27 for singletons and 180 for multiple births. So, neonatal mortality for both groups fell over the decades. However, neonatal mortality in multiple births was five times higher than in singletons in the 1970s, and this became seven times higher in the 2010s. A similar trend was also observed for infant and under-five mortality.
Table 4. Neonatal, infant, and under-five mortality rate by type of birth
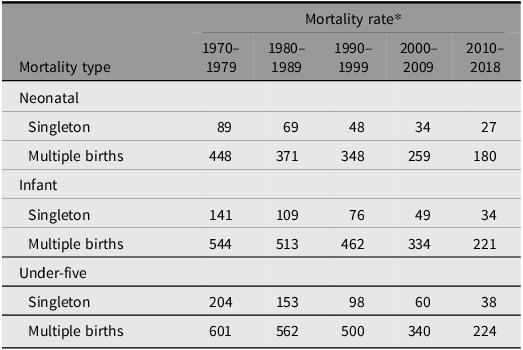
Note:
* Per thousand live births of a specific type.
A distinctive feature that can be observed in Table 4 is that in the 1970s, 75% of the under-five mortality in multiple births occurred in the neonatal period, whereas the same was 45% for singletons. In the 2010s, 80% and 71% of the under-five mortality in multiple births and singletons respectively occurred in the neonatal period. So, the share of neonatal mortality increased for both groups, though absolute size decreased.
Figure 2a shows that the percentage share of neonatal deaths in singleton births is on the rise. However, the share of singleton child deaths in post-neonatal infant (1−12 months) and post-infant under-five (12−60 months) period is falling. A similar trend is observed for multiple births in Figure 2b. As per Figure 2c, the share of multiple births in all different types of deaths is on the rise.

Figure 2. Percentage distribution of different types of deaths of singleton and multiple births.
The Kaplan-Meier curves in Figure 3 vividly illustrate the wide difference in survival probability over singleton and multiple births. From the infant survival probability plot, we observe that survival probability for multiple births, regardless of birth decades, drastically falls during the neonatal period (first month) compared to singletons. In the 1970s, at the end of the under-five period, the cumulative survival probability was as low as .43 for multiple births compared to .80 for singletons. In the 2010s, this stood at .97 and .85 respectively for the two groups. It indicates the closing of the wide gap in survival probability between these two groups.

Figure 3. Different types of decadal cumulative survival probability of singleton and multiple births.
Changing Determinants
Maternal age at birth is an important determinant of multiple births. Figure 4 shows that the average maternal age at birth has risen by 3.2 years, from 20.4 to 23.6, in the last five decades. Moreover, the average maternal age at first birth is also on the rise.

Figure 4. Trends in decade-wise average maternal age.
Figure 5 presents another set of interesting features. In the 1970s, approximately 70% of the first birth occurred when mother’s age was below 18. However, in the 2010s, the scenario reversed, as 70% of the first births occurred during the maternal age of 18−30. The percentage of second births occurring at the maternal age of 18−30 and above 30 increased from 74 to 90% and 0.11 to 6% respectively during the same period. Third and higher order births seem to be occurring more beyond the age of 30, as the share increased from 4% to 32% over the last five decades.

Figure 5. Decade-wise distribution of parity over age groups.
Discussion
From 1970 to 2018, Bangladesh’s twinning rate increased by 1.5 times, from 5.8 to 8.6 twin deliveries per 1000 deliveries, resulting in live births. This is at the same level as South Asia but well below the world’s average of 12. This study reveals that the rise is due to an increase in both DZ and MZ twinning. However, no consistent trend was observed for other higher order multiple births. Bangladesh’s twinning phenomenon varies over maternal age, parity, maternal BMI and household wealth index. It might be thought that the rise in twinning with maternal age is intertwined with higher parities. However, the results from the multivariate logistic regression confirm their independent effect. We also observed variation across geographic divisions.
Balasch (Reference Balasch2010) noted that advancing education, career prospects and contraceptive use all together drive the delay in childbearing. Since independence, Bangladesh has witnessed tremendous growth in female education at all levels (Mannan et al., Reference Mannan, Alam, Roy, Alam, Ashrafuzzaman, Khorshed, Karim and Abdullah2015). Since 1990, the female labor-force participation rate has grown by 12%, from 26% to 38%. During the past 20 years, contraceptive usage also increased by 10%, from 54% to 64% (NIPORT & ICF, 2023). Hence, the rise in average maternal age at birth (Figure 4) in Bangladesh is more likely driven by these factors. As Bangladesh is still progressing in these underlying factors, it is easy to anticipate that maternal age at birth will rise even further in the coming decades. This means more births will occur at higher maternal ages, and the risk of multiple births will increase. Moreover, this risk will increase further as higher parity (two and above) births occurring at ages beyond 30 are also rising (Figure 5).
Unlike the global north, assisted reproductive technology (ART) is yet to become popular, reliable, affordable and readily available in Bangladesh (Hossain, Reference Hossain2023). An implication of rising maternal age at birth is rising infertility (Lemoine & Ravitsky, Reference Lemoine and Ravitsky2015). During the last two decades, such infertility rose by 12%, from 18% to 30% (Riese, Reference Riese2021). With rising per capita income, we anticipate more demand and supply regarding ART will be realized in the coming decades. As a result, multiple births will rise from this source, too.
With such an increase in multiple births from multiple sources along existing hereditary components, several matters of concern emerge. First, advanced maternal age is related to increased maternal death, prematurity, fetal and neonatal death (Liu et al., Reference Liu, Case, Cheung, Sierra, AlAsiri, Carranza-Mamane, Case, Dwyer, Graham and Havelock2012). Second, the share of multiple births in neonatal, post-neonatal infant, and post-infant under-five mortality will keep rising, given the trend of the last five decades. Third, three quarters of the deaths in multiple births are concentrated in the neonatal period over the last five decades.
To mitigate these concerns, special focus has to be put on perinatal, neonatal and post-neonatal care and their availability to mothers with multiple births. Continued monitoring of the trend in multiple births and their impact on child mortality is warranted. Otherwise, the expected rise in multiple births might reverse Bangladesh’s success in lowering child mortality in the decades to come.
Acknowledgment
We thank the DHS Program for making the datasets available for this research.
Competing interests
None.










 Open access
Open access