



Twin pregnancy represents a health issue as it is well known to be more prone to maternal and fetal complications and perinatal mortality than a singleton pregnancy (Cheetham, Reference Cheetham2007; Rankin et al., Reference Rankin, Pearce, Bell, Glinianaia and Parker2005; Vogel et al., Reference Vogel, Torloni, Seuc, Betran, Widmer, Souza and Merialdi2013). Furthermore, during the last 40 years, a marked increase in the incidence of twin pregnancies — in particular, dizygotic ones — has been observed in most industrialized countries (Dawson et al., Reference Dawson, Tinker, Jamieson, Hobbs, Rasmussen and Reefhuis2015; Eriksson & Fellman, Reference Eriksson and Fellman2007), due to the widespread use of assisted reproductive technologies (ART; Dawson et al., Reference Dawson, Tinker, Jamieson, Hobbs, Rasmussen and Reefhuis2015; Fuster et al., Reference Fuster, Zuluaga, Colantonio and de Blas2008). Given the diffusion and the clinical implications, the study of twin pregnancies is of utmost epidemiological interest.
Among other adverse conditions typical of twin pregnancies, birth weight discordance (BWD), defined as the disparity of 15% and 40% in birth weights between the larger and the smaller twin respectively (Breathnach et al., Reference Breathnach, McAuliffe, Geary, Daly, Higgins, Dornan, Morrison, Burke, Higgins, Dicker, Manning, Mahony, Malone and Ireland Research Consortium2011; Breathnach & Malone, Reference BreathnachMd and Malone2012), complicates about 10% to 29% of pregnancies, according to the cut-off value used to describe discordance (Blickstein & Goldman, Reference Blickstein and Goldman2003; Miller et al., Reference Miller, Chauhan and Abuhamad2012). Up to a certain degree of discordance, the discrepancy in the birth weights of twins should be considered physiological; the mechanism whereby two fetuses exposed to the same intrauterine environment adopt significantly different growth patterns represents a final common pathway for several twin pregnancy conditions.
The presence of opposite-sex twins (Azcorra et al., Reference Azcorra, Rodriguez and Mendez2021; Blickstein & Weissman, Reference Blickstein and Weissman1990), placental dysfunction (Victoria et al., Reference Victoria, Mora and Arias2001), older maternal age, (Konar et al., Reference Konar, Sarkar and Paul2016; Sannoh et al., Reference Sannoh, Demissie, Balasubramanian and Rhoads2003; Tan et al., Reference Tan, Wen, Fung, Walker and Demissie2005) low maternal socioeconomic profile (Azcorra et al., Reference Azcorra, Rodriguez and Mendez2021; Kim et al., Reference Kim, Caughey, Yee and Cheng2019; Luo et al., Reference Luo, Wilkins and Kramer2006; Tan et al., Reference Tan, Wen, Fung, Walker and Demissie2005), primiparity (Blickstein et al., Reference Blickstein, Goldman and Mazkereth2000; Sannoh et al., Reference Sannoh, Demissie, Balasubramanian and Rhoads2003), and lower total twin birth weight (Blickstein et al., Reference Blickstein, Goldman, Smith-Levitin, Greenberg, Sherman and Rydhstroem1999; Tan et al., Reference Tan, Wen, Fung, Walker and Demissie2005) are factors that have been associated with BWD. Also chorionicity represents a relevant factor influencing BWD; in monochorionic pregnancies, vascular anastomoses due to the sharing of a single placenta may lead to an unbalanced intertwin transfusion and consequent asymmetric growth of twins (Denbow et al., Reference Denbow, Cox, Taylor, Hammal and Fisk2000; Homola et al., Reference Homola, Florjanski, Krolak-Olejnik, Fuchs, Lachowska and Bek2019; Lewi et al., Reference Lewi, Cannie, Blickstein, Jani, Huber, Hecher, Dymarkowski, Gratacos, Lewi and Deprest2007).
Further, given the significant contribution of ART to twin pregnancies, it appears interesting to investigate the role of ART on BWD. An increased risk of BWD was reported in ART versus spontaneous twins (Daniel et al., Reference Daniel, Ochshorn, Fait, Geva, Bar-Am and Lessing2000; Koudstaal et al., Reference Koudstaal, Bruinse, Helmerhorst, Vermeiden, Willemsen and Visser2000; Pinborg et al., Reference Pinborg, Loft, Rasmussen, Schmidt, Langhoff-Roos, Greisen and Andersen2004; Zadori et al., Reference Zadori, Kozinszky, Orvos, Katona, Kaali and Pal2004; Zhang et al., Reference Zhang, Liu and Zeng2013), but the evidence is still scarce and controversial (Suzuki & Murata, Reference Suzuki and Murata2007; Yang et al., Reference Yang, Choi, Nam, Kwon, Park and Kim2011).
Some studies have identified discordant twin growth as an independent risk factor for adverse perinatal consequences (Blickstein et al., Reference Blickstein, Mincha, Goldman, Machin and Keith2006; Harper et al., Reference Harper, Weis, Odibo, Roehl, Macones and Cahill2013; Wen et al., Reference Wen, Fung, Huang, Demissie, Joseph, Allen, Kramer and Cana2005; Yinon et al., Reference Yinon, Mazkereth, Rosentzweig, Jarus-Hakak, Schiff and Simchen2005), neonatal morbidity (D’Antonio, Thilaganathan et al., Reference D’Antonio, Thilaganathan, Laoreti, Khalil, Bahamie, Bhide, Deans, Egbor, Ellis, Gandhi, Hamid, Hutt, Matiluko, Morgan, Pakarian, Papageorghiou, Peregrine and Roberts2018; Di Mascio et al., Reference Di Mascio, Acharya, Khalil, Odibo, Prefumo, Liberati, Buca, Manzoli, Flacco, Brunelli, Benedetti Panici and D’Antonio2019), and intrauterine death (D’Antonio, Odibo et al., Reference D’Antonio, Odibo, Prefumo, Khalil, Buca, Flacco, Liberati, Manzoli and Acharya2018). Others have attributed the morbidity and mortality observed in discordant pairs to confounding factors (Cooperstock et al., Reference Cooperstock, Tummaru, Bakewell and Schramm2000; Fraser et al., Reference Fraser, Picard, Picard and Leiberman1994; Frezza et al., Reference Frezza, Gallini, Puopolo, De Carolis, D’Andrea, Guidone, Luciano, Zuppa and Romagnoli2011; Konar et al., Reference Konar, Sarkar and Paul2016; Patterson & Wood, Reference Patterson and Wood1990), such as gestational age at delivery, as a strong association between BWD and preterm births was observed, actual birth weight, gender discordance, and chorionicity. However, no clear picture of this issue has been defined.
In order to shed more light on this unfavorable condition, we analyzed the prevalence, potential risk factors and consequences of BWD in a cohort of same-sex twins in Lombardy, Northern Italy, during the period 2007 to 2021. In addition, we evaluated whether ART influences the outcomes of BWD twins.
Methods
Data Source and Study Cohort
Data for this study were retrieved from the automated system of healthcare utilization (HCU) databases from Lombardy, the largest region of Italy (about 10 million inhabitants), which includes a variety of information on residents who receive National Health System (NHS) assistance. We collected data about maternal sociodemographic characteristics, reproductive history, the current mode of conception, pregnancy course, delivery and newborns’ outcomes from the certificate of delivery assistance (Certificato di Assistenza Al Parto [CedAP]) database. We linked records from CedAP and standard discharge form (Scheda di Dimissione Ospedaliera [SDO]) databases through a unique anonymized identification code for each subject. The analysis of the anonymous administrative database does not require ethics committee approval in Italy.
We identified twin births in Lombardy between January 1, 2007 and December 31, 2021. We included deliveries for which there was a SDO related to childbirth coded according to the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) and/or the Diagnosis-Related Groups (DRG) code, of mothers aged 15 to 55 years, and occurring between 22 to 42 gestational weeks. Deliveries with a lack of information concerning the mode of conception (i.e., spontaneous, nonspontaneous), birth weight, sex of at least one of the twins, and opposite-sex deliveries were excluded. For the cohort selection, the regional databases were accessed until March 2023.
Birth Weight Discordance (BWD) Definition
Information about the birth weight of each twin was collected from CedAP. Intertwin discordance was obtained by the formula
 $$100*{{larger\;twin\;weight - smaller\;twin\;weight} \over {larger\;twin\;weight}}.$$
Pregnancy was considered complicated by the BWD when the disparity was 30% or more (Jahanfar et al., Reference Jahanfar, Lim and Oviedo-Joekes2016; Vergani et al., Reference Vergani, Locatelli, Ratti, Scian, Pozzi, Pezzullo and Ghidini2004).
$$100*{{larger\;twin\;weight - smaller\;twin\;weight} \over {larger\;twin\;weight}}.$$
Pregnancy was considered complicated by the BWD when the disparity was 30% or more (Jahanfar et al., Reference Jahanfar, Lim and Oviedo-Joekes2016; Vergani et al., Reference Vergani, Locatelli, Ratti, Scian, Pozzi, Pezzullo and Ghidini2004).
Statistical Analysis
First, univariate and multivariate logistic regression were performed to determine the potential factors (i.e., maternal age; nationality; level of education — university, high school, middle or primary school; parity; and mode of conception) associated with BWD. Odds ratios (ORs) and 95% confidence intervals (CIs) were subsequently calculated. Stratified analysis by sex was also conducted.
Second, we compared the distribution of the adverse neonatal outcomes of interest, including preterm birth (36 gestational weeks or less), low birth weight (2500 grams or less), small for gestational age (SGA; having a birth weight below the 10th percentile for gestational age, according to the sex-specific Italian reference curve for normal fetal growth; Parazzini et al., Reference Parazzini, Cortinovis, Bortolus, Fedele and Decarli1995), low Apgar score (7 or less), perinatal mortality, according to the BWD level (i.e., ≤20%, 21–29%, and ≥30%). The trend test was used to test differences in the above-mentioned outcomes according to the BWD’s levels. The same analysis was repeated, excluding preterm births from the cohort (N = 7009 pairs of twins).
Finally, we assessed the relative risks (RRs) and 95% CIs of the neonatal outcomes of interest and the mode of conception according to the presence or absence of BWD. Models were adjusted by maternal age, nationality, level of education, and parity.
We performed analysis using the Statistical Analysis System Software (version 9.4; SAS Institute, Cary, NC, USA).
Results
We identified 17,786 twin births that occurred in Lombardy between January 1, 2007 and December 31, 2021. Of these, we subsequentially excluded: 145 deliveries that did not match with a SDO related to childbirth and/or with the DRG code, 13 deliveries of mothers aged less than 15 years or more than 55 years of age, 32 deliveries occurred before 22 completed weeks or after 42 completed weeks. Out of 17,596 twin births, 89 without information concerning the mode of conception, birth weight, or sex of at least one twin were excluded. Finally, we considered only same-sex twins for a total of 11,096 deliveries.
Couples of females twins were 5620 (50.6%), and ones of males were 5476 (49.4%). In general, males were heavier in comparison to females; the average birth weight was 2309.2 g and 2232.8 g, respectively (p < .0001).
Births affected by BWD (i.e., discordance of 30% between the largest and smallest twin weight) were 556 (5.0%), 279 (5.0%) among females and 277 (5.0%) among males (p = .8204). More in particular, 6,175 (55.7%) twin deliveries presented a discordance of less than 10%, 3144 (28.3%) between 10 and 19%, 1221 (11.0%) between 20 and 29%, 377 (3.4%) between 30 and 39% and 179 (1.6%) over 40%.
ORs of BWD cases according to selected potential risk factors are provided in Table 1. Maternal age >35 years (OR 1.23, 95% CI [1.01, 1.50]), parous (OR 0.73, 95% CI [0.61, 0.88]), and non-spontaneous conception (OR 1.33, 95% CI [1.10, 1.61]) were significant factors for BWD in univariate analysis. After adjusting for all potential risk factors, gestational age >35 years (OR 1.26, 95% CI [1.05, 1.51]), low level of education (OR 1.34, 95% CI [1.05, 1.70]), and parous (OR 95% CI [0.73, 0.60, 0.89]) were significantly associated with BWD. However, nonspontaneous conception was confirmed as a risk factor even if the estimate was not statistically significant due to the low statistical power (OR 1.16, 95% CI [0.94, 1.44]). The results were consistent in the subsets of males and females; however, most of the significance was lost, probably due to the lower statistical power.
Table 1. Odds ratios (ORs) of birth weight discordance (BWD) couples of twins according to selected potential risk factors. Lombardy, 2007–2021

Note: BWD, birth weight discordance.
a Univariate logistic regression model.
b Multivariate logistic regression model.
c 9 missing values.
Lowering the cut-off of discordance — BWD defined as 20% or more disparity in birth weights — in the multivariate analysis, advanced maternal age (OR 1.19, 95% CI [1.07, 1.33]) and ART (OR 1.17, 95% CI [1.03, 1.32]) remained associated with an increased risk of BWD and parity (OR 0.77, 95% CI [0.69, 0.87]) with a reduced risk (data not shown).
Table 2 shows the distribution of the modality of delivery and the adverse neonatal outcomes according to the degree of weight discordance. Regarding the modality of delivery, in the group of BWD equal to 30% or more, cesarean sections during labor and cesarean sections without labor were over two-fold more common in comparison to the group of non-BWD. Preterm birth (61.2% vs. 69.0% vs. 83.6%, p trend ≤ .0001), low birth weight (when both twins experienced the outcome, 52.5% vs. 51.4% vs 67.7%, p trend ≤ .0001), small for gestational age (at least one twin, 17.9% vs. 46.7% vs. 80.8%, p trend ≤ .0001), low Apgar score (7 or less; at least one twin, 6.9% vs. 10.7% vs. 23.4%, p trend ≤ .0001), and perinatal mortality (at least one twin, 0.6% vs. 1.2% vs. 10.1%, p trend ≤.0001) were more common in twins with a discordance equal to 30% or more with respect to those with discordance between 20−29%, with respect to those with a discordance less then 20%. Excluding preterm births from the cohort, the positive association between adverse outcomes and BWD was still observed (data not shown).
Table 2. Modality of delivery and adverse neonatal outcomes according to the degree of birth weight discordance (BWD), Lombardy, 2007−2021
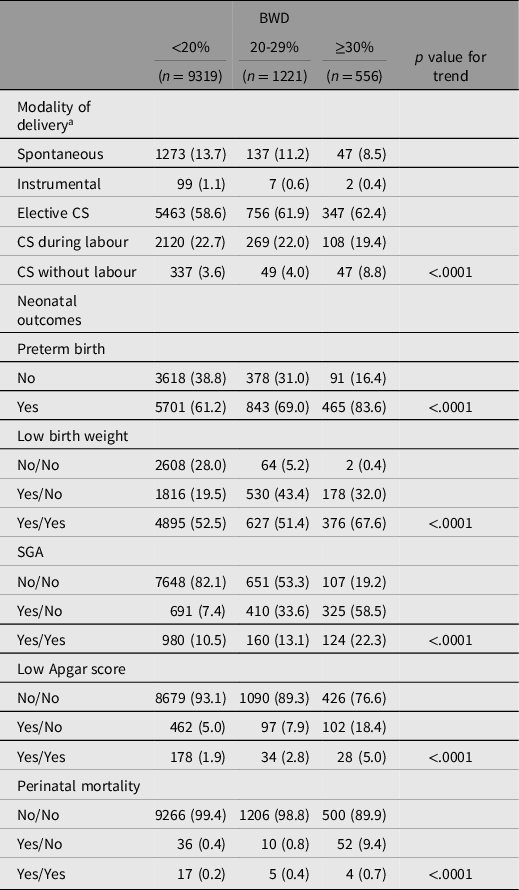
Note: SGA, small for gestational age; CS, cesarian section.
a The sum did not add up to the total because of missing data.
ART was inversely related to worst outcomes among both non-BWD and BWD twins (RR ranging from 14% to 6% from small for gestational age to preterm birth). No association was observed for perinatal mortality, probably due to the low statistical power (Table 3). Results were confirmed, also lowering the cut-off of discordance to 20% (data not shown).
Table 3. Adverse neonatal outcomes among birth weight discordance (BWD) and non-BWD pairs of twins according to mode of conception (i.e., spontaneous and after assisted reproductive technologies [ART]), Lombardy, 2007−2021

Note: RR, relative risk.
Discussion
In the current study, pairs of twins affected by a 30% or more disparity in birth weights between the larger and the smaller twin represented about 5% of a cohort of same-sex twins in Lombardy, Northern Italy, during the period 2007–2021. BWD was more common in women aged 35 years or more and those undergoing ART, but less frequent in parous women. The adverse neonatal outcomes observed (i.e., preterm birth, low birth weight, low Apgar score, SGA, and perinatal mortality) were more frequent among BWD twins.
As a concern for potential risk factors, we found that advanced maternal age (i.e., ≥35 years) was related to proneness to have a BWD, even if the association was of borderline significance. This finding is consistent with previous analyses conducted in populations from the United States and, more recently, from a tertiary care center in India (Konar et al., Reference Konar, Sarkar and Paul2016; Sannoh et al., Reference Sannoh, Demissie, Balasubramanian and Rhoads2003; Wen et al., Reference Wen, Fung, Huang, Demissie, Joseph, Allen, Kramer and Cana2005). All over the world, especially in high-income countries, maternal age at birth is rising. Thus, the evaluation of the consequences of this trend represents an issue of utmost importance because older maternal age has been associated with an increased risk of several adverse perinatal outcomes (Frick, Reference Frick2021). We also observed a positive relation between lower educational levels and BWD, as previous studies found (Azcorra et al., Reference Azcorra, Rodriguez and Mendez2021; Kim et al., Reference Kim, Caughey, Yee and Cheng2019; Luo et al., Reference Luo, Wilkins and Kramer2006; Tan et al., Reference Tan, Wen, Fung, Walker and Demissie2005). This condition may reflect lower incomes and unhealthier behaviors and influence the access to perinatal care, compromising the management of the course of pregnancy and delaying appropriate interventions. We also found that advanced maternal age (i.e., ≥35 years) was related to proneness to have a BWD, even if the association was of borderline significance. Regarding the use of ART, we confirmed the previously observed (Koudstaal et al., Reference Koudstaal, Bruinse, Helmerhorst, Vermeiden, Willemsen and Visser2000; Pinborg et al., Reference Pinborg, Loft, Rasmussen, Schmidt, Langhoff-Roos, Greisen and Andersen2004; Zadori et al., Reference Zadori, Kozinszky, Orvos, Katona, Kaali and Pal2004) increased risk of BWD among women undergoing these techniques versus those conceiving spontaneously. In addition, we also confirm primiparity findings (Blickstein et al., Reference Blickstein, Goldman and Mazkereth2000; Sannoh et al., Reference Sannoh, Demissie, Balasubramanian and Rhoads2003); in our cohort, parous women had about 25% reduced risk of BWD. Regarding the chorionicity, if dichorionic twins have completely separate circulation systems during intrauterine life, about 95% of monochorionic twins have vascular anastomoses on the single placental surface that connects the two circulations (Denbow et al., Reference Denbow, Cox, Taylor, Hammal and Fisk2000; Lewi et al., Reference Lewi, Cannie, Blickstein, Jani, Huber, Hecher, Dymarkowski, Gratacos, Lewi and Deprest2007). In monochorinic pregnancies, placental vascular anastomoses leads to twin-to-twin transfusion in 15% of cases, resulting in an assymetric growth of the fetus (Hack et al., Reference Hack, Nikkels, Koopman-Esseboom, Derks, Elias, van Gemert and Visser2008). On the other hand, opposite-sex twins also showed an increased risk for BWD compared to same-sex twins (Azcorra et al., Reference Azcorra, Rodriguez and Mendez2021), and it has been reported that females of opposite-sex twin pairs have a significantly increased risk of being growth discordant (Blickstein & Weissman, Reference Blickstein and Weissman1990); this finding may be justified by the higher measures of males in terms of birth weight and length (Parazzini et al., Reference Parazzini, Cortinovis, Bortolus, Fedele and Decarli1995). The debate regarding the influence of the own sex and also of the sex of cotwin on the birth weight is still ongoing.
The management of BWD is challenging since no evidence assessing the different management options (expectant and intervention management) is available. In particular, prenatal identification of BWD may lead to a iatrogenic delivery before the term of pregnancy, attributing the aftermath of prematurity on both twins, regardless of whether one of the two may have a physiological growth.
Although some studies have identified BWD as an independent risk factor for adverse perinatal consequences (Blickstein et al., Reference Blickstein, Mincha, Goldman, Machin and Keith2006; D’Antonio, Odibo et al., Reference D’Antonio, Odibo, Prefumo, Khalil, Buca, Flacco, Liberati, Manzoli and Acharya2018; D’Antonio, Thilaganathan et al., Reference D’Antonio, Thilaganathan, Laoreti, Khalil, Bahamie, Bhide, Deans, Egbor, Ellis, Gandhi, Hamid, Hutt, Matiluko, Morgan, Pakarian, Papageorghiou, Peregrine and Roberts2018; Di Mascio et al., Reference Di Mascio, Acharya, Khalil, Odibo, Prefumo, Liberati, Buca, Manzoli, Flacco, Brunelli, Benedetti Panici and D’Antonio2019; Harper et al., Reference Harper, Weis, Odibo, Roehl, Macones and Cahill2013; Hartley et al., Reference Hartley, Hitti and Emanuel2002; Wen et al., Reference Wen, Fung, Huang, Demissie, Joseph, Allen, Kramer and Cana2005; Yinon et al., Reference Yinon, Mazkereth, Rosentzweig, Jarus-Hakak, Schiff and Simchen2005) others have attributed the morbidity and mortality observed in discordant pairs to confounding factors (Cooperstock et al., Reference Cooperstock, Tummaru, Bakewell and Schramm2000; Fraser et al., Reference Fraser, Picard, Picard and Leiberman1994; Frezza et al., Reference Frezza, Gallini, Puopolo, De Carolis, D’Andrea, Guidone, Luciano, Zuppa and Romagnoli2011; Konar et al., Reference Konar, Sarkar and Paul2016; Patterson & Wood, Reference Patterson and Wood1990), especially to preterm birth.
In our study we also evaluated the relationship between BWD and selected adverse outcomes. As shown previously by other studies and as can be expected from BWD management alternatives mentioned above, we observed that preterm births were more common among BWD twins compared with non-BWD twins. In general, all the other outcomes considered (i.e., low birth weight, SGA, low Apgar score, and perinatal mortality) were more frequent among BWD births. A recent study found that BWD infants had a higher antibiotic prescription rate than the concordant ones, even though the strep test results and newborn septicemia rates were similar, showing that BWD twins required early respiratory support (Jahanfar et al., Reference Jahanfar, Lim and Ovideo-Joekes2017). As we found that BWD twins frequently obtained a low Apgar score, our results are consistent with this finding. We also observed a higher proportion of perinatal deaths among BWD twins. A systematic review investigating perinatal mortality reported that both dizygotic and monozygotic twin pregnancies discordant were at higher risk of intrauterine death but not of neonatal death compared with pregnancies with concordant ones, especially when at least one fetus was SGA (D’Antonio, Odibo et al., Reference D’Antonio, Odibo, Prefumo, Khalil, Buca, Flacco, Liberati, Manzoli and Acharya2018).
Given the widespread use of ART, its great contribution to the conception of twins, and the evidence that ART may increase the risk of BWD (Daniel et al., Reference Daniel, Ochshorn, Fait, Geva, Bar-Am and Lessing2000; Koudstaal et al., Reference Koudstaal, Bruinse, Helmerhorst, Vermeiden, Willemsen and Visser2000; Pinborg et al., Reference Pinborg, Loft, Rasmussen, Schmidt, Langhoff-Roos, Greisen and Andersen2004; Zadori et al., Reference Zadori, Kozinszky, Orvos, Katona, Kaali and Pal2004; Zhang et al., Reference Zhang, Liu and Zeng2013), we investigated the role of ART on BWD outcomes. An analysis focusing on this topic suggested that the possible differences in the management of pregnancies after ART and spontaneous ones could moderate the sequelae of BWD (Zadori et al., Reference Zadori, Kozinszky, Orvos, Katona, Kaali and Pal2004). In our cohort, the proportion of all adverse outcomes investigated was higher among spontaneous than ART pregnancies in both discordant and nondiscordant twins.
Some study limitations need to be considered. First, data for this study were exclusively based on inpatient information, thus clinical diagnoses given in an outpatient setting or not recorded as one of the patient diagnoses in hospitalizations for delivery or during pregnancy were missing. Thus, no hypotheses could be made about the pathophysiological clinical pathway leading to BWD, such as unequal placental sharing, abnormalities of umbilical cord insertion, placental dysfunctions, and twin-to twin-transfusion. We tried to identify births reported in the corresponding SDO a code, in the main or in the secondary diagnoses, related to such conditions, but often even if reporting poor fetal growth, the underlying mechanism was not specified. Second, we decided to include only same-sex twins in the study cohort due to the well-known disparity in terms of birth weight and length between males and females. In this way, we included all the monochorionic pregnancies in a higher proportion than in the general population. In addition, another limitation of the study was the inability to distinguish the dizygotic from monozygotic pregnancies. According to the probabilistic Weinberg’s method (Weinberg, Reference Weinberg1901) assuming that sex gender is independently distributed in dizygotic, compared to monozygotic pregnancies, in our cohort, the difference between the total number of twins and twice the number of opposite-sex twins provides an estimated number of monozygotic twins of 4460, resulting in a proportion of 40.2%, higher compared with the proportion observed in the general population (31.7% estimated in spontaneously conceived twins in Lombardy, 2007–2017; Esposito et al., Reference Esposito, Dalmartello, Franchi, Mauri, Cipriani, Corrao and Parazzini2022). The major strength of the study is its population-based design, whereby a large cohort of twins is available over a span of more than 10 years.
In conclusion, the presence of BWD complicates twin pregnancies, compromising neonatal outcomes. Further evidence is needed to better identify potential risk factors and interventions to limit adverse consequences in order to improve the management strategy in BWD twins.
Availability of data and materials
The data that support the findings of this study are available from Lombardy Region, but restrictions apply to the availability of these data, which were used under license for the current study. The data used in this study cannot be made available in the manuscript, the supplemental files or in a public repository due to Italian data protection laws. The anonymized datasets generated during and/or analyzed during the current study can be provided on reasonable request, from the corresponding author, after written approval by the Lombardy region.
Funding
This work was supported by a research grant from the Italian Ministry of Education, University and Research (“PRIN” 2017, project 2017728JPK). The grant provides financial support for the analysis of data.
Disclosure of interests
Giovanni Corrao received research support from the European Community (EC), the Italian Agency of Drugs (AIFA), and the Italian Ministry for University and Research (MIUR). He took part in a variety of projects that were funded by pharmaceutical companies (i.e., Novartis, GSK, Roche, AMGEN and BMS). He also received honoraria as a member of the advisory board to Roche. The other authors declare that they have no conflicts of interest to disclose.
Ethics approval and consent to participate
According to Italian law, studies based entirely on registry data do not require approval from an ethics review board.




 Open access
Open access