



Consequences of twinning in later life have become an important public health issue in recent decades as twinning rates have increased in many industrialized countries due to increased maternal age and the use of medically assisted reproduction (Pison et al., Reference Pison, Monden and Smits2015). The increase has been most dramatic in dizygotic (DZ) twin pregnancies, but the proportion of monozygotic (MZ) twin pregnancies of all pregnancies has also increased (Imaizumi, Reference Imaizumi2003). This is because medically assisted reproduction increases not only DZ but also, to a lesser extent, MZ rates (Knopman et al., Reference Knopman, Krey, Oh, Lee, McCaffrey and Noyes2014). The general increase in twin pregnancies and the different trends according to the type of twinning emphasize the need to understand risks related to different types of twin pregnancies to optimize medical treatment during pregnancy and provide parental support after delivery.
Twin pregnancies are characterized by higher pre- and postnatal risk factors compared to singleton pregnancies (Weitzner et al., Reference Weitzner, Barrett, Murphy, Kingdom, Aviram, Mei-Dan, Hiersch, Ryan, van Mieghem, Abbasi, Fox, Rebarber, Berghella and Melamed2023), which can also affect neurodevelopmental outcomes (Luu & Vohr, Reference Luu and Vohr2009). Previous studies have suggested that twins may exhibit slight delays in cognitive development compared to singletons, with some studies showing lower IQ scores persisting into adulthood, although this difference has decreased in recent birth cohorts (Voracek & Haubner, Reference Voracek and Haubner2008). However, it is not well understood whether there are differences in neurodevelopment between different types of twin pregnancies. Monochorionic (MC) twins, in particular, are believed to have a higher risk of developmental delay due to specific prenatal risk factors, with twin-to-twin transfusion syndrome being one of the most severe complications (Murgano et al., Reference Murgano, Khalil, Prefumo, Mieghem, Rizzo, Heyborne, Melchiorre, Peeters, Lewi, Familiari, Lopriore, Oepkes, Murata, Anselem, Buca, Liberati, Hack, Nappi, Baxi and D’antonio2020). Research has indicated that MC twins are more likely to experience neurodevelopmental impairments compared to dichorionic (DC) twins (Yan et al., Reference Yan, Wang, Chen and Zhang2023). However, existing evidence has primarily focused on severe neurodevelopmental impairments, such as cerebral palsy, and there is limited information on more subtle differences in neurodevelopment between MC and DC twins and how they compare to singletons.
Neurodevelopment is a process that starts during fetal life and continues throughout childhood, emphasizing the need for longitudinal studies. Since most studies comparing MC twins, DC twins, and singletons are based on cross-sectional data, we decided to analyze these associations using large longitudinal data of Japanese children including a significant number of MC and DC twins. Based on our data, we can compare several dimensions of psychomotor development in MC and DC twins to singletons from 6 months to 3 years of age. Building on previous evidence, we propose the following hypotheses: (1) Twins exhibit a delay compared to singletons in psychomotor development; (2) This delay is more pronounced in MC twins than in DC twins; and (3) The delay is most significant at 6 months of age and decreases, but remains present until 3 years of age.
Materials and Methods
The data were derived from the Japan Environment and Children’s Study (JECS) described in detail elsewhere (Kawamoto et al., Reference Kawamoto, Nitta, Murata, Toda, Tsukamoto, Hasegawa, Yamagata, Kayama, Kishi, Ohya, Saito, Sago, Okuyama, Ogata, Yokoya, Koresawa, Shibata, Nakayama and Michikawa2014; Michikawa et al., Reference Michikawa, Nitta, Nakayama, Yamazaki, Isobe, Tamura, Suda, Ono, Yonemoto, Iwai-Shimada, Kobayashi, Suzuki and Kawamoto2018). Briefly, the data were collected in 15 regional centres in Japan representing the Japanese geography from Hokkaido to Kyushu and Okinawa. The target population was pregnant women residing in the selected areas between January 2011 and March 2014. The present study was based on the jecs-ta-20190930 dataset, released in October 2019 and revised in November 2022. The selection of the participants for the current study is described in Supplementary Figure 1. The total number of fetal records was 104,062. After removing stillbirths as well as triplets and those with missing information on sex, chorionicity, maternal age or gestational age, we ended up with 99,670 children (49% females), who form the basic study cohort invited to clinical exams. Twin pregnancies were classified as MC (577 children) and DC (1051 children) based on ultrasound images and, if needed, complemented by the postnatal pathological examination of the placenta.
Children’s psychomotor development was assessed using the Japanese version of the Third Edition of Ages and Stages Questionnaires (ASQ-3) until the age of 3 (Squires & Bricker, Reference Squires and Bricker2009). The mailed questionnaire at 6, 12, 18, 24, 30, and 36 months were completed by caregivers, consisting of 30 questions across five domains of psychomotor development: communication, gross motor development, fine motor development, problem-solving, and personal-social development. Each question was coded with yes = 10 points, sometimes = 5 points, and not yet = 0 points, resulting in scores ranging from 0 to 60. Children with incomplete ASQ-3 information (one or more missing items) were coded as missing for that domain. The number of children with valid responses varied from 74,574 to 83,603 depending on the survey age and domain. Response rates for twins were lower than for singletons at 6 months of age but converged by age 3 as the number of singletons decreased and twins increased (Supplementary Figure 1). This suggests that mothers of twins may face challenges in participating in clinical examinations when their children are infants but find it easier as they grow older.
The data were analyzed using a linear regression model with the ASQ-3 scores as the response variables and chorionicity (singletons, MC twins and DC twins) as the explanatory variable. Separate models were conducted for each domain from 6 months to 3 years of age. The initial model adjusted the results only for children’s age at the time of the survey to demonstrate the net effects of twinning and chorionicity on psychomotor development (Model 1). Instead of the official age (days after birth), we used age corrected for prematurity, essentially showing age calculated from conception. This corrected age was also used when inviting mothers for the clinical exams; premature children were invited at an older official age than full-term born children. Second, the results were adjusted for maternal age, the use of reproductive technology (based on questions about the use of artificial insemination, external fertilization, or other fertility treatment dichotomized as yes or no), parity (0 or ≥1), gestational age, and birth weight as covariates in the model to analyze how much of the twinning effect is due to these other factors associated with twinning (Model 2).
We then tested the hypothesis that if twinning is associated with lower psychomotor development in infancy, twins may show catching up as they grow older. This was studied by subtracting the scores at each age from the score at the subsequent age and using this difference as the response variable in the regression model. In this modeling, we first adjusted the results for corrected age (age difference between the two surveys) and then for the other covariates. All analyses were conducted using Stata/SE 13.1 for Windows statistical software (StataCorp, College Station, TX, USA). The effect of intrapair correlations on standard errors for twin participants, that is, sampling twin pairs rather than independent individuals, was taken into account using the cluster option of Stata (Williams, Reference Williams2000).
Results
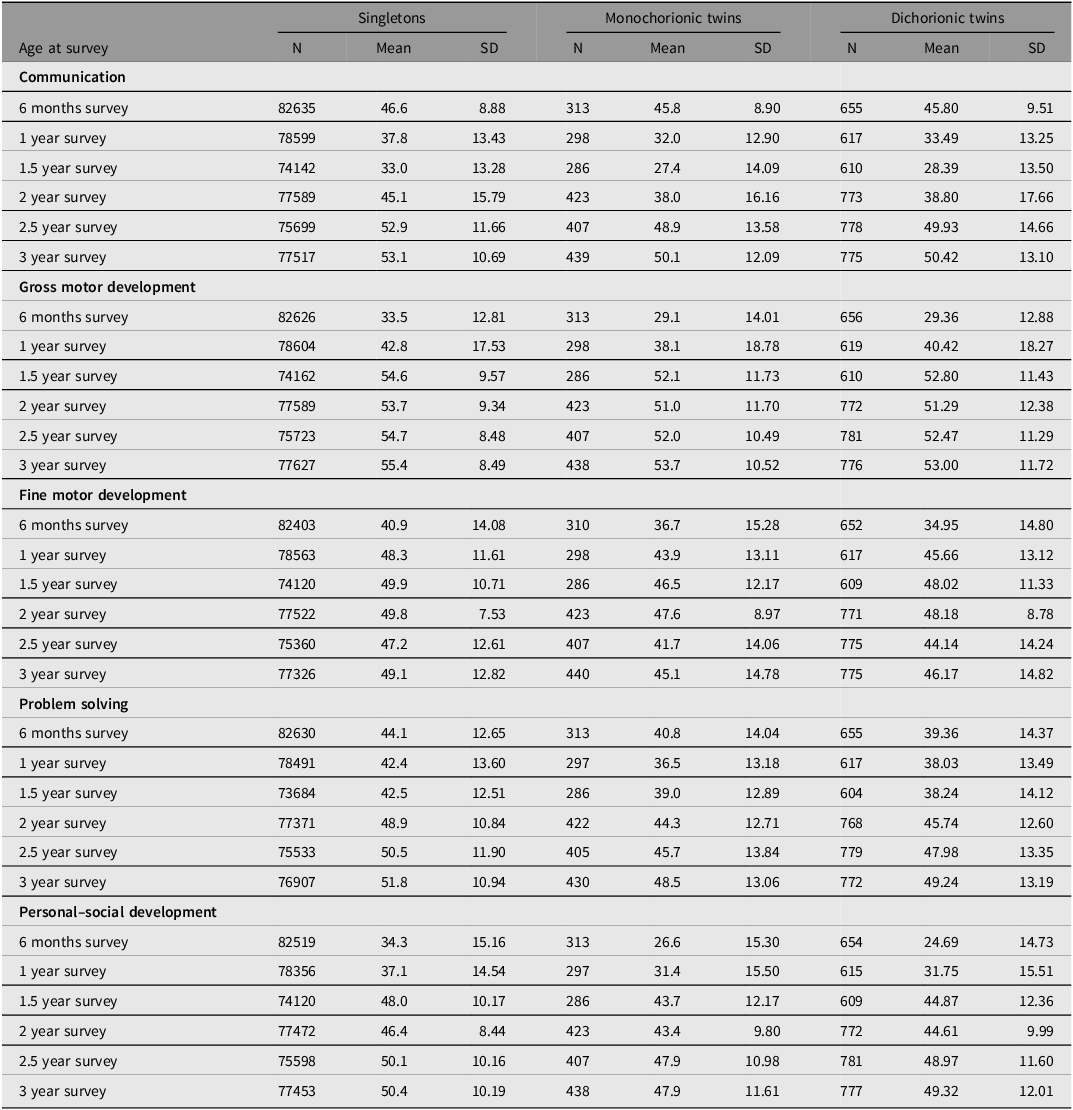
Table 1 presents the descriptive statistics of child psychomotor development by chorionicity status. In each survey and psychomotor domain, twins were slightly delayed compared to singletons. Between MC and DC twins, the differences were small. However, for most of the tests, the test scores were slightly higher for DC twins compared to MC twins.
Table 1. Descriptive statistics of psychomotor development of children from 6 months until 3 years of age by chorionicity
Next, we conducted linear regression models using singletons as the reference category (Table 2). In the model adjusted for age (Model 1), both MC and DC twins showed delay in all domains of psychomotor development. The differences were smallest for communication (-0.85 for MC and -0.89 in DC twins) and largest for personal-social development (-9.07 and -10.27 respectively) at 6 months of age. The differences between twins and singletons tended to systematically diminish over aging, and they were lowest at 3 years of age. The exception was communication, where the difference for both MC and DC twins was largest at 2 years of age and then diminished until 3 years of age. However, the differences did not disappear, and at 3 years of age, twins still lagged behind singletons in all domains of psychomotor development. The differences were roughly similar in the different domains of psychomotor development (the regression coefficient varied between -1.76 and -4.17). Adjusting the results for the covariates explained a remarkable part of the delay of twins compared to singletons (Model 2). On average, the effect sizes declined by 66%. No systematic differences were seen in the effect of covariates over ages or between MC and DC twins. However, for most of the tests, twins still showed some delay compared to singletons after adjusting for these covariates, even when only some of the regression coefficients were statistically significant.
Table 2. Regression coefficients of psychomotor development in mono- and dichorionic twins as compared to singletons from 6 months until 3 years of age
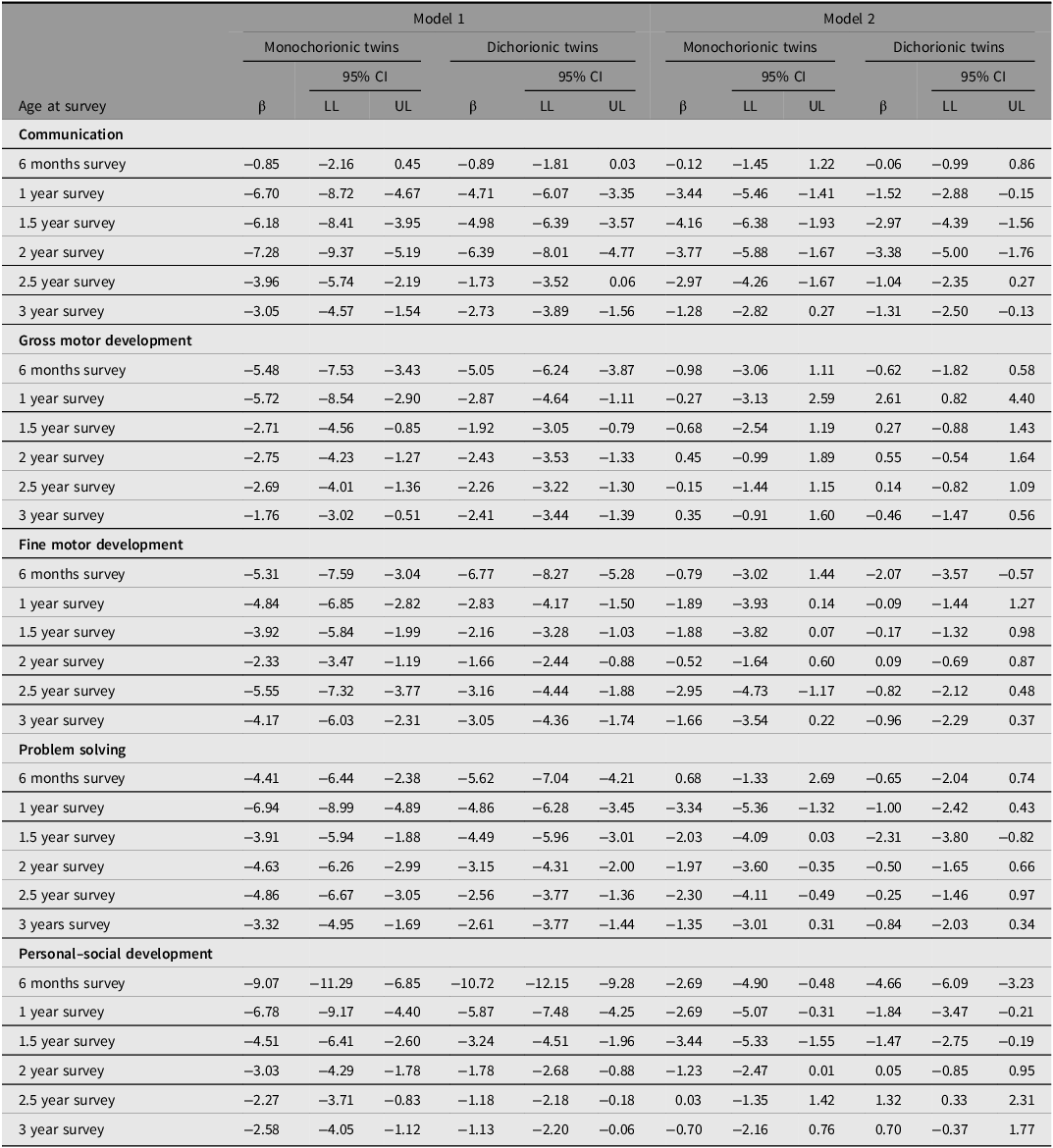
Note: LL, lower level; UL, upper level.
Model 1: adjusted for corrected children’s age.
Model 2: adjusted for corrected children’s age, mother’s age, the use of assisted reproductive technology (yes/no), parity (0/≥1), gestational age and birth weight.
When we compared MC and DC twins in more detail, we found that in nearly all tests, DC twins were slightly more advantaged than MC twins (the regression estimates for DC twins compared to MC twins are presented in Supplementary Table 1). Out of 30 tests conducted, DC twins were more advantaged in 24 tests when adjusted for age (Model 1). However, the effect sizes were modest (2.66 or smaller), and nearly all regression coefficients were not statistically significant. In contrast to the analyses between twins and singletons, adjusting the results for covariates had weak effects on the regression coefficients (Model 2), and in many cases, they even slightly increased compared to Model 1.
Finally, we analyzed how psychometric development between singletons and twins changed over ages (Table 3). Between 6 months and 1 year, we found that both MC and DC twins were delayed compared to singletons in some domains, as indicated by negative regression coefficients. After 1 year of age, nearly all of the regression coefficients were positive, indicating that twins caught up to singletons in all domains of psychomotor development. However, the confidence intervals were wide, and most of the regression coefficients were not statistically significant. Adjusting the results for the covariates decreased the regression coefficients corresponding to smaller differences in test scores between singletons and twins (Model 2).
Table 3. Regression coefficients of change of psychomotor development measures in mono- and dichorionic twins as compared to singletons between consequent surveys from 6 months until 3 years of age
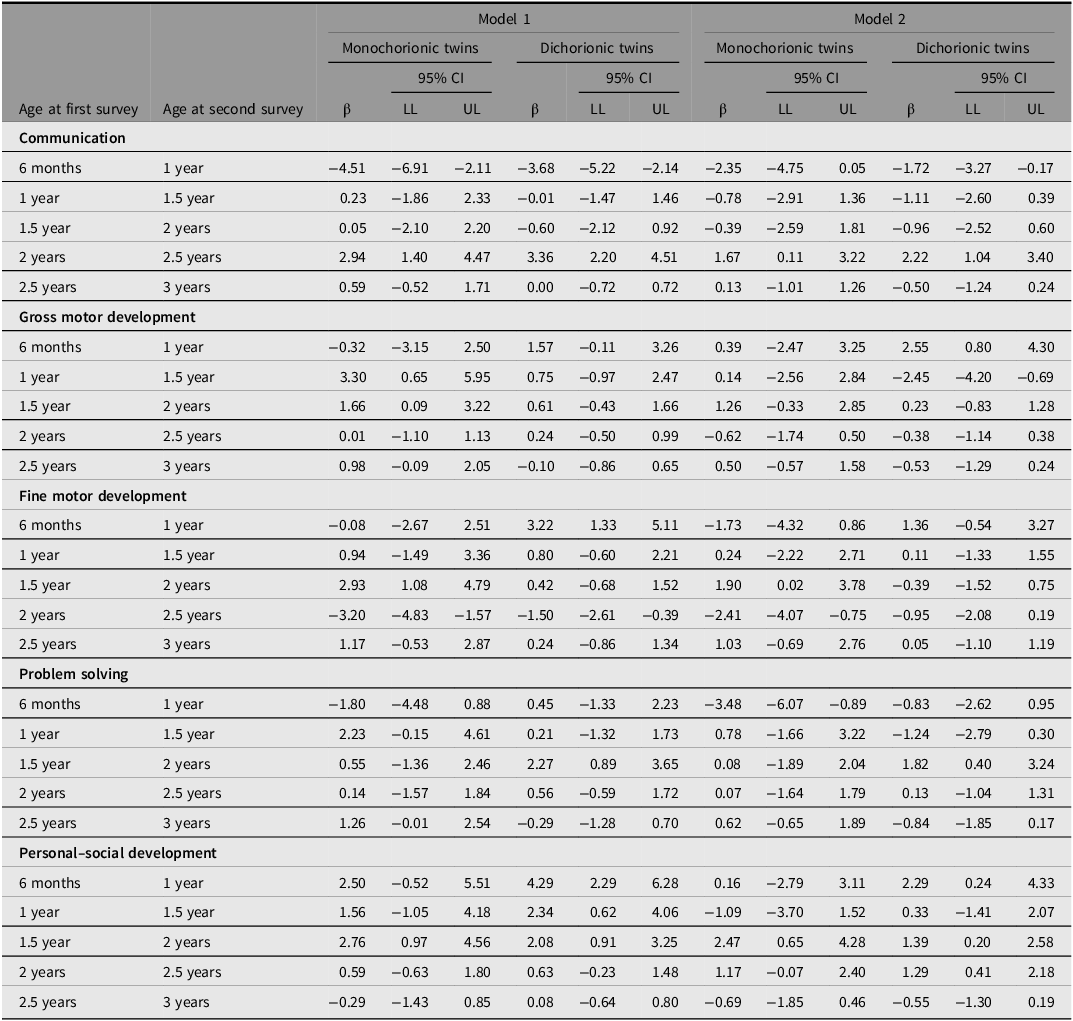
Note: LL, lower level; UL, upper level.
Model 1: adjusted for the difference in corrected children’s age between the surveys.
Model 2: adjusted for the difference in corrected children’s age between the surveys, mother’s age, the use of assisted reproductive technology (yes/no), parity (0/≥1), gestational age and birth weight.
Discussion
In this large nationwide cohort study of Japanese twins and singletons, we found that twins lagged behind singletons in their psychomotor development, as measured by ASQ-3 scores, even at 3 years of age. This difference was consistent across all five domains of psychometric development: communication, gross motor development, fine motor development, problem-solving, and personal-social development. Our results align with previous studies from Japan (Yokoyama et al., Reference Yokoyama, Wada, Sugimoto, Saito, Matsubara and Sono2007) and Taiwan (Lung et al., Reference Lung, Shu, Chiang and Lin2009), which also reported slower motor development in twins compared to singletons during infancy and early childhood. However, these studies were smaller in scale than ours and did not consider chorionicity.
In our study, postnatal risk factors associated with lower psychomotor development, including earlier gestational age and lower birth weight, accounted for more than half of the differences between twins and singletons. This finding is consistent with previous studies (Lung et al., Reference Lung, Shu, Chiang and Lin2009; Yokoyama et al., Reference Yokoyama, Wada, Sugimoto, Saito, Matsubara and Sono2007) and reflects the known differences in gestational age and birth weight between twins and singletons (Pascal et al., Reference Pascal, Govaert, Oostra, Naulaers, Ortibus and van den Broeck2018). These factors have a significant impact on psychomotor development in early life and can affect neurocognitive outcomes into adulthood (Heinonen et al., Reference Heinonen, Lahti, Sammallahti, Wolke, Lano, Andersson, Pesonen, Eriksson, Kajantie and Raikkonen2018). Our results suggest that while twin and singleton pregnancies have distinct characteristics and different risk factors (Hiersch et al., Reference Hiersch, Barrett, Fox, Rebarber, Kingdom and Melamed2022), neonatal risk factors still play a significant role in explaining neurodevelopmental delay in twins. Therefore, standards developed for singletons are relevant for evaluating the risks of neurodevelopmental delays in twins as well. However, even after accounting for these adjustments, we observed slight delay in psychomotor development in twins, indicating that there may be twin-specific effects beyond gestational age and birth weight that influence early psychomotor development.
Even when twins were delayed compared to singletons at 3 years of age, the differences were generally even larger at earlier ages. In general, we found a steady decline in the gap between twins and singletons from 6 months to 3 years of age. This shows that twins catch up to singletons during early childhood, as we demonstrated by studying the change in psychomotor skills in the same children. Catch-up of twins is well demonstrated in height and other physical measures (van Dommelen et al., Reference van Dommelen, de Gunst, van der Vaart, van Buuren and Boomsma2008), but our results demonstrate that this applies also to psychomotor development. The background of this catch-up is not clear. It can reflect the catching up of physical development but may also be related to familial interaction. In a previous experimental study, infant twins engaged more with their mother than with the co-twin, suggesting that the basic child-caregiver dynamic is not different in twins than in singletons (Aldrich et al., Reference Aldrich, Brooks, Yuksel-Sokmen, Ragir, Flory, Lennon, Karmel and Gardner2015). However, this change can still be related to family dynamics if parents have limited resources to take care of two neonates affecting their psychomotor development in early life, but the family situation improves as children grow older. This was suggested by our results showing that the difference between twins and singletons increased from 6 months to 1 year of age and only after that age started to diminish. More studies, preferably having longitudinal observations of families with twins, would be needed to further clarify the role of family environment and dynamics behind these differences.
Our most novel results concerned the effect of chorionicity on psychomotor development in twins. We found that MC twins were slightly delayed compared to DC twins in their psychomotor development. This result is in concordance with previous studies showing a higher risk of severe neurodevelopmental impairments in MC twins compared to DC twins (Yan et al., Reference Yan, Wang, Chen and Zhang2023). Thus, our results demonstrate that this also applies to more subtle differences between MC and DC twins. Lower birth weight and earlier gestational age (Ghi et al., Reference Ghi, Prefumo, Fichera, Lanna, Periti, Persico, Viora and Rizzo2017), as well as a higher risk of birth defects, have been demonstrated in MC twins than in DC twins (Weitzner et al., Reference Weitzner, Barrett, Murphy, Kingdom, Aviram, Mei-Dan, Hiersch, Ryan, van Mieghem, Abbasi, Fox, Rebarber, Berghella and Melamed2023). However, in our study, adjusting the results for gestational age and birth weight did not explain the difference between MC and DC twins. Previous Japanese studies have also found a higher rate of severe neurodevelopmental impairment in MC twins compared to DC twins in low birth weight children (<1500 g), suggesting that the effect of chorionicity on neurodevelopmental delay is not solely due to birth weight (Ichinomiya et al., Reference Ichinomiya, Maruyama, Koizumi, Inoue, Fukuda, Kaburagi and Miyakawa2018; Kawamura et al., Reference Kawamura, Ishii, Yonetani, Mabuchi, Hayashi and Mitsuda2015). However, in our study, the difference in psychomotor development between MC and DC twins was much smaller than the difference between all twins and singletons. Thus, chorionicity seems to play a relatively minor role when assessing the psychomotor outcomes of twin pregnancies.
Our study has both strengths and weaknesses. Our main strength is the large, nationwide cohort of 1628 twins and 98,042 singletons, which allows us to generalize our results to the whole Japanese population. We have measures of chorionicity based on ultrasound images and postnatal placenta examination, which is rare in epidemiological settings. Furthermore, we have six longitudinal measures on five domains of psychomotor development from 6 months to 3 years of age, allowing us to analyze psychomotor development from infancy to early childhood. Additionally, we had information on key risk factors for psychomotor development. Our main weakness is that we did not have detailed information on pregnancy, such as twin-to-twin transfusion syndrome. Therefore, we cannot analyze in detail the causes behind the differences found between singletons, MC twins and DC twins. Moreover, severe neurodevelopmental impairments, such as cerebral palsy, may have prevented families from participating in the clinical exams. Thus, our results should mainly generalize to the children without severe neurodevelopmental delays.
In conclusion, we found that twins lagged behind singletons in their psychomotor development. The delay was most significant in infancy and decreased over early childhood but was still evident at 3 years of age. A significant proportion of this delay was due to the earlier gestational age and lighter birth weight of twins compared to singletons, but there may also be some effect related to twinning itself. MC twins showed a slight delay compared to DC twins, but this effect of chorionicity was relatively minor when compared to the difference between twins and singletons. Twins are at risk of slightly slower psychomotor development in early life. However, this effect is not specific to MC twinning.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/thg.2024.39.
Data availability
Data are unsuitable for public deposition due to ethical restrictions and legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No. 57 of 30 May 2003, amendment on 9 September 2015) to publicly deposit the data containing personal information. Ethical Guidelines for Medical and Health Research Involving Human Subjects enforced by the Japan Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Health, Labour and Welfare also restricts the open sharing of the epidemiologic data. All inquiries about access to data should be sent to: [email protected]. The person responsible for handling enquiries sent to this e-mail address is Dr Shoji F. Nakayama, JECS Programme Office, National Institute for Environmental Studies.
Acknowledgments
We thank all participants in the JECS. We wish to express our sincere appreciation to the collaborating hospitals and clinics. We also express our gratitude to all the JECS staff members in Hokkaido, Miyagi, Fukushima, Chiba, Kanagawa, Koshin, Toyama, Aichi, Kyoto, Osaka, Hyogo, Tottori, Kochi, Fukuoka, and South-Kyushu and Okinawa Regional Centres and national center for JECS (Programme Office), and the Medical Support Centre.
Financial support
This study was funded by the Ministry of the Environment, Japan. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the above government.
Competing interests
None to declare.
Ethical standards
The JECS protocol was reviewed and approved by the Ministry of the Environment’s Institutional Review Board on Epidemiological Studies and the Ethics Committees of all participating institutions (#100910001). Written informed consent was obtained from all participants in the study, and they gave the consent also behalf of their children.
Appendix
Members of the JECS Group as of 2024: Michihiro Kamijima (Principal Investigator, Nagoya City University, Nagoya, Japan), Shin Yamazaki (National Institute for Environmental Studies, Tsukuba, Japan), Maki Fukami (National Center for Child Health and Development, Tokyo, Japan), Reiko Kishi (Hokkaido University, Sapporo, Japan), Chiharu Ota (Tohoku University, Sendai, Japan), Koichi Hashimoto (Fukushima Medical University, Fukushima, Japan), Chisato Mori (Chiba University, Chiba, Japan), Shuichi Ito (Yokohama City University, Yokohama, Japan), Ryoji Shinohara (University of Yamanashi, Chuo, Japan), Hidekuni Inadera (University of Toyama, Toyama, Japan), Takeo Nakayama (Kyoto University, Kyoto, Japan), Ryo Kawasaki (Osaka University, Suita, Japan), Yasuhiro Takeshima (Hyogo Medical University, Nishinomiya, Japan), Seiji Kageyama (Tottori University, Yonago, Japan), Narufumi Suganuma (Kochi University, Nankoku, Japan), Shoichi Ohga (Kyushu University, Fukuoka, Japan), and Takahiko Katoh (Kumamoto University, Kumamoto, Japan).






 Open access
Open access