


Suicidal behaviour is frequent among patients with schizophrenia (Reference TsuangTsuang, 1978; Reference KingKing, 1994; Heila et al, Reference Heila, Isometsa and Henriksson1997, Reference Heila, Heikkinen and Isometsa1999; Reference King, Baldwin and SinclairKing et al, 2001; Reference Walsh, Harvey and WhiteWalsh et al, 2001). Several countries have mentioned those with mental illness in national prevention strategies as an important group (Reference Taylor, Kingdom and JenkinsTaylor et al, 1997; Sundhedsstyrelsen (National Board of Health), 1998). Analysis of the occurrence of Danish suicides shows that 27% has been admitted during the year before suicide (Reference Mortensen, Agerbo and EriksonMortensen et al, 2000). The great Finnish psychological autopsy study, investigating all suicides in Finland in 1988, showed that 24% had been treated as psychiatric in-patients during the 12 final months (J. Lönnqist, personal communication, 2001).
High risk of suicidal behaviour
Increased risk of suicide is associated with all diagnoses except dementia (Reference Harris and BarracloughHarris & Barraclough, 1997; Reference Mortensen, Agerbo and EriksonMortensen et al, 2000). Danish analyses show that the rate of suicide among patients with schizophrenia has increased, simultaneously with a decline in the suicide rate in the general population (Reference MortensenMortensen, 1995; Reference Rossau and MortensenRossau & Mortensen, 1997). Suicide rates are highest during the first week or month after discharge (Reference Goldacre, Seagroatt and HawtonGoldacre et al, 1993; Reference Rossau and MortensenRossau & Mortensen, 1997). For the majority of patients who die from suicide shortly after discharge, prevention would have been possible had there been sufficient support and treatment facilities (Reference Burgess, Pirkis and MortonBurgess et al, 2000). A comprehensive analysis of Danish suicides shows that young people with first-episode severe mental illness form a particularly high-risk group (Reference Mortensen and JuelMortensen & Juel, 1993; Reference Rossau and MortensenRossau & Mortensen, 1997).
Risk factor for suicide
Few randomised controlled trials of treatment that might reduce suicidal behaviour have been conducted (Reference Hawton, Arensman and TownsendHawton et al, 1998), and to our knowledge none among patients with first-episode psychosis.
In several studies, a previous suicide attempt was identified as a risk factor for ultimate suicide, as was suicidal ideation and hopelessness (Reference Hu, Sun and LeeHu et al, 1991; Reference Heila, Isometsa and HenrikssonHeila et al, 1998; Reference King, Baldwin and SinclairKing et al, 2001). The psychopathology of patients with schizophrenia who ultimately commit suicide has been investigated and presence of psychotic symptoms and presence of depression were identified as the two most important predictors (Reference Heila, Isometsa and HenrikssonHeila et al, 1997; Reference De Hert, McKenzie and PeuskensDe Hert et al, 2001).
Aims
OPUS is a randomised controlled trial of integrated treatment compared with standard treatment among patients with first-episode psychosis. Analyses of data from the OPUS study show that the integrated treatment has positive effects on positive and negative symptoms and patient satisfaction (Reference Nordentoft, Jeppesen and KassowNordentoft et al, 2002).
The present paper focuses on suicidal behaviour. The purpose of this part of the OPUS project is to characterise the group of patients with high-risk for suicidal behaviour, to examine the effect of integrated treatment on suicidal behaviour, suicidal ideations and hopelessness, and to identify predictive factors, such as symptoms and other characteristics, for preventive purposes.
METHOD
Patient sample
The inclusion criteria were:
-
(a) age 18 to 45 years and a legal residence in the catchment areas;
-
(b) a diagnosis of schizophrenia, schizotypal disorder, delusional disorder, acute or transient psychosis, schizoaffective psychosis, induced psychosis, or unspecific non-organic psychosis according to ICD-10 (World Health Organization, 1993) research criteria, based on present state examination;
-
(c) exposure to antipsychotic medication has never exceeded 12 weeks of continuous medication in antipsychotic dosage;
-
(d) absence of ‘mental retardation’ (learning disability), organic mental disorder and psychotic condition because of acute poisoning or a withdrawal state;
-
(e) familiarity with the Danish language;
-
(f) written informed consent.
The use of psychoactive drugs did not cause exclusion. Subjects were referred to the study from all in-patient and out-patient mental health services in Copenhagen (Copenhagen Hospital Corporation) and Aarhus County (Northern Aarhus, Western Aarhus, Djursland, Silleborg and Randers). The study sites in Copenhagen included 6 university hospitals and 11 community mental health centres, and the sites in Aarhus included 1 university hospital and 5 community mental health centres. The population size of the total catchment area is 1 040 000 persons, which represents more than one-sixth of the total Danish population. When clinicians in the mental health service found a candidate for the study, the research team began the diagnostic assessment with Schedules for Clinical Assessment in Neuropsychiatry (SCAN) version 2.0 (Reference Wing, Babor and BrughaWing et al, 1990).
This article is a preplanned interim analysis of baseline and 1-year follow-up data for the 341 patients recruited and randomised in the first 20 months of the study, i.e. from 1 January 1998 to 1 September 1999.
Sample attrition
A flow chart of the project is shown in Fig. 1. A total of 341 patients were included in the first 20 months of the study, but information about suicidal behaviour and ideations was collected in only 321 cases. For 304 patients, information gathered in the SCAN 2.0 interview allowed assessment of the presence of depression or hopelessness. Analyses of these clinical items from the baseline interview are based on this group of 304 patients. At the 1-year follow-up interview, 275 patients participated, all of whom reported information about suicidal behaviour. For 227 patients, complete information from the baseline interview and the follow-up interview were available, and analyses, which include both the baseline and the 1-year follow-up data on suicidal behaviour, SANS and SAPS (Reference Andreasen, Flaum and SwayzeAndreasen et al, 1990) and SCAN 2.0 are thus based on 227 patients, 121 from the integrated treatment group and 106 from the standard treatment group. Two patients died during the follow-up period; one suicide in the OPUS team-treated group and one unaccounted death in the standard group. Both were men.
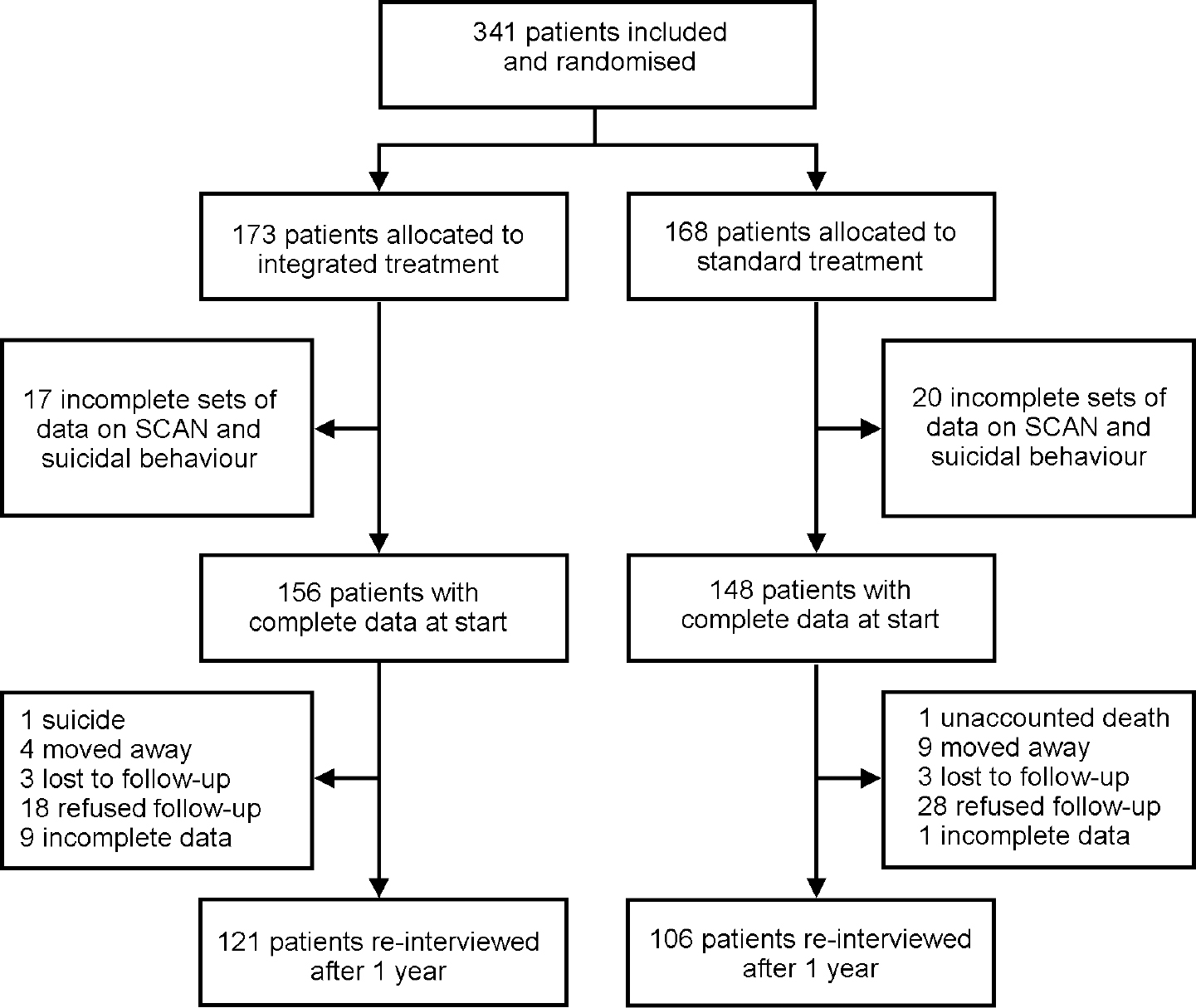
Fig. 1 Trial profile. SCAN, Schedules for Clinical Assessment in Neuropsychiatry.
Design
In a randomised controlled trial, integrated psychiatric treatment was compared with standard treatment. Patients were followed up after 1 year.
Integrated treatment
The OPUS project was funded by the Danish Ministry of Health and the Ministry of Social Affairs for the purpose of addressing some of the well-known, very poor outcomes (homelessness, crime and suicide) and to increase the quality of treatment for patients with first-episode psychosis (Reference Jorgensen, Nordentoft and AbelJorgensen et al, 2000). The project is a randomised controlled trial in which standard treatment is compared with integrated treatment. The integrated treatment consists of the following elements:
-
(a) assertive community treatment (ACT);
-
(b) antipsychotic medication;
-
(c) psychoeducational family treatment;
-
(d) social skills training.
All patients are offered ACT and are encouraged to participate with their relatives in psychoeducational family treatment. Social skills training is offered to those who, after assessment with the World Health Organization's (1988) Disability Assessment Schedule (WHO/DAS), are judged to need social skills training. Antipsychotic medication is offered to the majority of the patients after consultation with the psychiatrist in the team.
Assertive community treatment
Three multi-disciplinary psychosis teams were established, two in Copenhagen and one in Aarhus, and trained to provide integrated treatment, modelled on ACT. The teams consist of the following professional groups: psychiatrist; psychologist; nurse; vocational therapist; and social worker. The case-load is shared and does not exceed 10:1. The cornerstone of the treatment is a supportive and outreaching contact. Each patient is allocated a primary contact to one team member, who is responsible for maintaining contact and securing coordination of the treatment across different treatment facilities and across the social sector and the health sector. Home visits are preferred but the patient can also be seen at other places in the community or at the office. If in hospital, the patient is visited weekly. During in-patient treatment, the treatment responsibility is transferred to the hospital and the team maintains contact with those responsible for treatment and discharge plans. The opening hours are Monday to Friday from 08.00h to 17.00h. All team members have a mobile phone with a message function; patients are encouraged to call at any time if they need help or advice. Out of hours, they can leave a message and know that the team will respond the next morning. A crisis plan is developed for each patient, often including calling significant others and, in emergency cases, visiting the local psychiatric emergency room or calling psychiatric emergency outreach.
The integrated treatment is offered for 2 years. If the patient wants to discontinue the contact in order to avoid psychiatric treatment, the team will try to motivate the patient to continue treatment, keep in contact with the patient and try to find a common focus for therapy. If the patient continuously avoids treatment appointments, it is evaluated whether it is necessary to admit the patient compulsorily. If treatment is still needed after 2 years of integrated treatment, the patient is transferred to standard treatment in the relevant facilities.
Antipsychotic medication
As a part of the integrated psychiatric treatment, patients were offered antipsychotic medication according to guidelines from the Danish Psychiatric Society (1998), which recommend a low-dose strategy for patients with first-episode psychosis and use of second-generation antipsychotic drugs as first choice. Psychoeducation was carried out along with antipsychotic medication, and team members paid much attention to possible side-effects.
Psychoeducational family treatment
Most often, family treatment involves parents, but other relatives such as siblings, boy- or girlfriends, or other friends can be involved. The family treatment is mainly conducted in multi-family groups, as described in the manual developed by McFarlane et al (Reference McFarlane, Lukens and Link1995). The treatment has three components starting as soon as possible after the patient's inclusion.
-
(a) At least three individual family meetings without the patient.
-
(b) A survival skills workshop. Members of 4-6 families are given formal education about psychosis and its management, aetiology and prognosis, through lectures and discussions.
-
(c) The multi-family group is formed of 4-6 families and includes the patients and two family therapists. The group meets for 1.5 hours every second week for 18 months. Groups focus on problem-solving and development of skills to cope with the illness. Suicidal thoughts and suicidal behaviour can be an issue for problem-solving in the multifamily group.
For patients who do not take part in the psychoeducational family groups, the team offers to contact their relatives and to be available for contacts from relatives throughout the 2-year intervention period, through consultations or telephone calls. Relatives who live far from the patient are invited to participate in the survival skills workshop, even though they are unable to follow the rest of the multi-family group treatment.
Social skills training
Early in the out-patient phase of treatment, the patient's social skills are assessed with the WHO/DAS. The patients who lack basic skills for independent living are offered individual training and practical help in their homes. Other patients with impaired social skills are offered training in a group of at most six patients and two therapists. The training programme is organised in modules to overcome the patient with schizophrenia's symptomatic and cognitive barriers to learning. The five chosen modules are medication self-management, coping with symptoms, conversational skills, problem-solving skills and conflict-solving skills. Suicidal thoughts and suicidal behaviour can be dealt with in social skills training, especially in the coping-with-symptoms module.
Standard treatment
In standard treatment, the patient is usually offered treatment at a community mental health centre. The case-load of the staff in the community mental health centres varies between 1:20 and 1:30. The work is organised differently than in the OPUS team. Most patients are seen in the office and each patient is likely to be in contact with a physician, a community mental health nurse and a social worker. Some community mental health centres offer 8- to 10-week modules for participation in psychoeducational groups by relatives without participation of the patient. Social skills training is not offered in community mental health centres. The antipsychotic medication is based on the same principles in the OPUS team and the standard treatment.
Measures
All patients included in the sample were interviewed by independent interviewers at baseline and invited for a 1-year follow-up interview. The interview consisted of a comprehensive package of instruments. At baseline and 1-year follow-up, information was collected about socio-demographic factors, Global Assessment of Functioning (GAF; American Psychiatric Association, 1994) function and symptoms, suicidal behaviour, suicidal ideation and planning of suicide, and symptoms during the past month with SCAN 2.0 and SAPS and SANS. Analyses of SAPS and SANS were based on global scores and divided into three levels: no symptoms; questionable or mild symptoms; and moderate, marked or severe symptoms.
Analyses of hopelessness were based on a rating of 2 or 3 in the question about loss of hope for the future in SCAN 2.0. With algorithms based on ratings of 2 or 3 in selected items in the section covering depressed mood and ideation, thinking, concentration, energy, interests and bodily functions, it was investigated whether subjects fulfilled general criteria for depression in ICD—10.
Selected questions from the European Parasuicide Study Interview Schedule (EPSIS II) were used in investigating tedium vitae, suicidal thoughts and plans and suicide attempts (Reference Kerkhkof, van Egmond and Bille-BraheKerkhkof et al, 1991). All patients were asked at baseline and at 1-year follow-up about the frequency of tedium vitae (thoughts that life is not worth living), suicidal thoughts and suicidal plans during the past week and suicidal attempts during the past year. The answers were dichotomised into ‘not present’ and ‘present at least once’.
Duration of untreated psychosis was assessed with the Interview for Retrospective Assessment of Onset of Schizophrenia (IRAOS; Reference Hafner, Riecher-Rossler and HambrechtHafner et al, 1992). The IRAOS was conducted together with the SCAN interview.
Reliability of diagnoses and SAPS scores
Prior to the study, all assessors had participated in a 5-day, WHO-certified, training course in SCAN. The measure of reliability was 0.74 (kappa value) between the two researchers (P.J. and M.A.) who jointly assessed 15 interviews for agreement on the specific ICD—10 diagnosis. During the study, all assessors in Copenhagen met bimonthly and scored SAPS, based on the live interview. Pairwise kappa for agreement on psychosis versus remission, based on dichotomised SAPS scores, was in the range 0.72-1.0. Most pairs had perfect agreement.
Statistical methods
Categorical response data were analysed using the Pearson χ2. Differences for continuous responses were assessed using Student's t-test for normally distributed data. Logistic regression analyses were carried out, using stepwise backward regression based on the Wald test. All variables tested in the univariate analysis were entered into the backward stepwise regression analysis. Level of significance was 0.05.
Power calculation
With α=0.05 and β=0.90, a sample of 262 patients is necessary to detect a difference (20% v. 10%) in the proportion of patients reporting moderate or severe hopelessness at 1-year follow-up. To detect a difference between 12% and 6% in the proportion attempting suicide during the first year after inclusion, a sample of 425 patients is necessary (Reference PocockPocock, 1996). Thus, the study has sufficient power to detect changes in hopelessness but not to detect possible differences in suicide attempts during the follow-up period.
RESULTS
Baseline
The basic characteristics of the population are shown in Table 1. Table 2 shows the occurrence of previous suicide attempts (ever) in different socio-demographic and clinical groups. A strong association was found between previous suicide attempts and reported tedium vitae, suicidal thoughts, or suicidal plans during the week before the baseline interview.
Table 1 Socio-demographic and clinical characteristics for 321 patients with first-episode psychosis
| Total (n=321) | |
|---|---|
| Socio-demographic characteristics | |
| Males | 60.1% |
| Females | 39.9% |
| Age (mean, s.d.) | 27.0 (6.3) |
| Brought up with both parents | 63.8% |
| 11, 12 or 13 years' school education | 34.1% |
| Married | 6.2% |
| Being a parent | 16.5% |
| Having an intimate relationship | 26.5% |
| Diagnosis | |
| Schizophrenia | 66.3% |
| Schizotypal disorder | 11.1% |
| Delusional disorder | 6.2% |
| Brief psychosis | 9.4% |
| Schizoaffective disorder | 5.3% |
| Unspecified non-organic psychosis | 1.8% |
| Comorbidity | |
| Harm or dependence syndrome | 22.1% |
| Depression1 | 24.9% |
| Suicidal behaviour and ideation, baseline | |
| Tedium vitae at least once last week | 36.6% |
| Suicidal thoughts at least once last week | 26.2% |
| Suicidal plans at least once last week | 12.8% |
| Suicide attempt last year | 19.6% |
| Suicide attempt ever | 25.8% |
| Hopelessness, moderate or severe1 | 13.5% |
| Social functioning | |
| GAF, symptoms (mean, s.d.) | 32.9 (10.4) |
| GAF, function (mean, s.d.) | 41.1 (13.0) |
Table 2 Frequency of suicide attempts in different clinical and social groups for patients with first-episode psychosis at baseline interview and 1-year follow-up
| Attempts reported at baseline (n=321) | Attempts during first year of treatment (n=275) | |||||
|---|---|---|---|---|---|---|
| Attempts | χ2/t-test2 | P | Attempts | χ2/t-test | P | |
| n (%) | 83 (25.8%) | 31 (11.3%) | ||||
| Socio-demographics | ||||||
| Males | 19.2% | 11.28 | 0.001*** | 6.2% | 9.95 | 0.002** |
| Females | 35.9% | 18.4% | ||||
| Age (years) | 25.7 (5.8) | 2.22 | 0.02* | 25.03 (5.56) | 1.732 | 0.09 |
| Brought up with both parents | 23.0% | 1.97 | 0.16 | 11.7% | 0.09 | 0.76 |
| Not brought up with both parents | 30.2% | 10.5% | ||||
| 11, 12 or 13 years' school education | 20.2% | 2.57 | 0.11 | 9.3% | 0.62 | 0.43 |
| Less than 11 years' school education | 28.4% | 12.4% | ||||
| Married | 35.0% | 0.93 | 0.33 | 20.0% | 1.64 | 0.2 |
| Unmarried | 25.2% | 10.6% | ||||
| Being a parent | 26.4% | 0.01 | 0.92 | 19.0% | 3.00 | 0.08 |
| Not being a parent | 25.7% | 9.0% | ||||
| Having an intimate relationship | 32.9% | 3.02 | 0.08 | 19.2% | 6.2 | 0.01** |
| Not having an intimate relationship | 23.3% | 8.4% | ||||
| Diagnosis | ||||||
| Schizophrenia | 25.2% | 9.45 (d.f. 5) | 0.09 | 12.6% | 5.30 (d.f. 5) | 0.38 |
| Schizotypal disorder | 29.7% | 6.9% | ||||
| Delusional disorder | 22.2% | 13.3% | ||||
| Brief psychosis | 10.7% | 0.0% | ||||
| Schizoaffective psychosis | 50.0% | 17.6% | ||||
| Unspecified non-organic psychosis | 33.3% | 20.0% | ||||
| Comorbidity | ||||||
| Harm or dependence syndrome | 26.8% | 0.39 | 0.84 | 17.1% | 1.62 | 0.20 |
| No harm or dependence syndrome | 24.2% | 10.3% | ||||
| Depression, baseline1 | 28.2% | 0.53 | 0.47 | 16.0% | 2.65 | 0.10 |
| No depression, baseline1 | 24.2% | 9.0% | ||||
| Suicidal behaviour and ideation | ||||||
| Tedium vitae last week | 39.0% | 12.59 | <0.001*** | 19.4% | 6.99 | 0.008** |
| No tedium vitae last week | 19.8% | 8.0% | ||||
| Suicidal thoughts last week | 37.8% | 6.97 | 0.008** | 23.8% | 8.19 | 0.004** |
| No suicidal thoughts last week | 22.1% | 8.7% | ||||
| Suicidal plans last week | 50.0% | 11.92 | 0.001*** | 29.0% | 46.13 | <0.001*** |
| No suicidal plans last week | 22.9% | 1.7% | ||||
| Previous suicide attempt | 20.6% | 10.21 | 0.001*** | |||
| No previous suicide attempt | 6.9% | |||||
| Social functioning | ||||||
| GAF, symptoms | 31.5 (9.9) | 1.52 | 0.11 | 31.7 (10.4) | 0.802 | 0.42 |
| GAF, function | 41.4 (12.2) | 0.72 | 0.94 | 42.0 (11.6) | 0.332 | 0.74 |
| Other | ||||||
| Hopelessness, moderate or severe, baseline1 | 39.0% | 4.70 | 0.03* | 11.8 | 0.22 | 0.88 |
| Hopelessness, none or mild, baseline1 | 23.2% | 10.9 | ||||
| Standard treatment | 25.8% | 0.001 | 0.97 | 10.4% | 0.18 | 0.68 |
| Integrated psychiatric treatment | 12.0% | |||||
| Duration of untreated psychosis2 | 213 weeks | 0.14 | 0.88 | |||
Predictors of suicidal ideation and suicide attempts during the past year, reported at baseline interview, were examined in univariate and multivariate analyses. The variables examined were SAPS and SANS, harm or dependence syndrome, depression or hopelessness and socio-demographic factors. Suicidal thoughts and suicidal plans were predicted by the degree of hallucinations and the presence of hopelessness and inversely associated with the degree of formal thought disorder and delusions. Degree of negative symptoms was not associated with suicidal thoughts or suicidal plans. Analyses of single items in the subscales in SAPS revealed commenting voices as a significant predictor of suicidal thoughts, while delusions of reference, somatic delusions and illogicality were inversely correlated with suicidal thoughts.
Suicide attempt the year before baseline was associated with younger age, presence of depression, hopelessness and global score of hallucinations. When the single items in the hallucination sub-scale were analysed, auditory hallucinations were positively correlated with suicidal attempts, whereas somatic delusions were negatively correlated.
One-year follow-up
During the first year of follow-up, there was one suicide in the OPUS team group, and in the standard group, one unaccounted death by drowning, where the cause of death was either suicide or accident.
At 1-year follow-up 11.3% (31/275) of the patients (Table 2) who attended the 1-year follow-up interview reported that during the first year of treatment they had attempted suicide. In the OPUS team-treated group, the frequency was 12.0% (18/150) and in the standard group 10.4% (13/125), which is not a statistically significant difference. Suicide attempt during the first year of treatment was more frequent among the females, among those who had an intimate relationship and among those who at the 1-year follow-up interview reported tedium vitae, suicidal thoughts or suicidal plans during the week before the interview. Suicide attempt during the first year of treatment was much more likely among those who at the baseline interview reported previous suicide attempt. Table 3 shows the frequency of tedium vitae, suicidal thoughts, suicidal plans, suicidal attempts, hopelessness and depression at the 1-year follow-up interview. This table only includes patients for whom we had information about suicidal behaviour and ideation and SCAN interview items both at baseline and follow-up. Hopelessness was very significantly less common among patients who received integrated psychiatric treatment in the OPUS team. For both treatment groups, suicidal ideation, hopelessness and attempted suicide during the past year were at a substantially lower level at the 1-year follow-up than at the baseline interview; however, the frequency of depression in the group receiving standard treatment was at the same level throughout the study period.
Table 3 Frequency of suicidal behaviour, suicidal ideation, hopelessness and depression in different treatment groups at 1-year follow-up
| OPUS Team | Standard treatment | χ2 | P | |
|---|---|---|---|---|
| n=121 | n=106 | |||
| Tedium vitae at least once last week | 25.9% | 27.4% | 0.78 | 0.78 |
| Suicidal thoughts at least once last week | 15.4% | 14.4% | 0.84 | 0.87 |
| Suicidal plans at least once last week | 7.0% | 9.6% | 0.60 | 0.44 |
| Suicidal attempt during last year | 10.3% | 10.5% | 0.003 | 0.96 |
| Loss of hope for the future, moderate or severe | 8.3% | 19.8% | 6.39 | 0.01** |
| Depression | 17.4% | 26.4% | 2.74 | 0.09 |
Suicidal thoughts at the 1-year follow-up were in univariate analyses found to be associated with hallucinations, delusions, hopelessness and depression reported at the 1-year follow-up interview and with suicidal thoughts reported at the baseline interview (Table 4). Depression and hopelessness rated at baseline was not predictive of suicidal thoughts at the 1-year follow-up. In the multivariate analysis, presence of hopelessness and the global rating of delusions at 1-year follow-up were the only significant items. Global rating of hallucinations became non-significant in the multivariate analysis, when hopelessness was entered into the model.
Table 4 Correlation between positive and negative symptoms and suicidal thoughts, suicide plans and suicidal attempts at 1-year follow-up. Univariate and multivariate backwards stepwise regression models

| Suicidal thoughts, last week | Suicidal plans, last week | Suicide attempt, last year | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | Univariate | Multivariate | |||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Male | 0.84 | 0.43-1.62 | 0.75 | 0.32-1.77 | 0.29 | 0.13-0.65 | ||||||
| Age (increasing) | 0.96 | 0.91-1.01 | 0.92 | 0.85-1.06 | 0.94 | 0.68-1.01 | ||||||
| Hopelessness, baseline | 0.92 | 0.33-2.54 | 1.50 | 0.48-4.27 | 2.89 | 1.34-6.23 | ||||||
| Hopelessness, 1 year | 3.68 | 1.54-8.82 | 4.41 | 1.71-11.37 | 2.93 | 1.04-8.31 | 2.93 | 1.04-8.31 | 1.89 | 0.69-5.09 | ||
| Depression, baseline | 1.77 | 0.78-3.18 | 1.79 | 0.73-4.38 | 1.92 | 0.87-4.24 | ||||||
| Depression, 1 year | 3.69 | 1.67-8.19 | 2.08 | 0.78-5.53 | 2.46 | 1.04-5.80 | ||||||
| Harm or dependence | 1.11 | 0.57-2.16 | 0.96 | 0.34-2.71 | 0.89 | 0.29-2.45 | ||||||
| Affective flattening1 | 1.09 | 0.67-1.76 | 1.62 | 0.80-3.05 | 1.58 | 0.72-2.73 | ||||||
| Alogia1 | 1.08 | 0.68-1.70 | 1.20 | 0.67-2.13 | 1.07 | 0.66-1.72 | ||||||
| Avolition1 | 1.53 | 0.98-2.39 | 2.24 | 1.20-4.17 | 0.81 | 0.49-1.34 | ||||||
| Anhedonia1 | 1.48 | 0.90-2.45 | 2.03 | 0.99-4.15 | 0.77 | 0.47-1.25 | ||||||
| Hallucinations1 | 2.00 | 1.34-2.97 | 1.68 | 1.02-2.76 | 2.77 | 1.53-5.02 | 2.51 | 1.33-4.74 | ||||
| Delusions1 | 1.79 | 1.18-2.70 | 1.94 | 1.13-3.32 | 1.58 | 0.94-2.66 | 1.02 | 0.61-1.71 | ||||
| Bizarre behaviour1 | 1.70 | 0.90-3.18 | 1.96 | 0.93-2.10 | 0.67 | 0.36-1.23 | ||||||
| Thought disorder1 | 0.67 | 0.34-1.31 | 1.19 | 0.58-2.43 | 0.49 | 0.26-0.87 | ||||||
| Baseline value | 2.07 | 1.00-4.32 | 1.70 | 0.55-5.48 | 3.52 | 1.49-8.32 | 2.72 | 1.12-6.63 | ||||
| Standard treatment | 0.86 | 0.44-1.67 | 1.30 | 0.55-3.06 | 0.85 | 0.40-1.80 | ||||||
In the analyses of suicidal plans, hopelessness, avolition and hallucinations rated at the 1-year interview were significant in univariate analyses, and in the final multivariate model, the 1-year rating of hopelessness was the only significant variable.
In the analyses of suicidal attempts during first-year follow-up, the baseline values of SANS, SAPS and SCAN 2.0 were examined. Being female, hopelessness expressed at the baseline interview, global rating of hallucinations and reporting a suicide attempt the year before the baseline interview were significantly positive in association with suicidal attempt in the follow-up period, whereas global rating of thought disorder was negatively associated with suicidal attempt. In the multivariate analysis, only global rating of hallucinations and suicide attempts in the year preceding the baseline interview were significant variables. When age and gender are not significant in the final model, it is most likely because the baseline reporting of previous suicide attempt is included in the model.
DISCUSSION
Suicidal ideation and reports of suicide attempt during the past year were significantly reduced in both treatment groups, but were still at a high level compared with the general population. Thus, an important finding in the study is that suicidal behaviour and suicidal ideation occur very frequently among patients with first-episode psychosis in the schizophrenia spectrum. Both at baseline and at the 1-year follow-up, these very unwanted phenomena were occurring in a substantial proportion of the patients, much more frequently than generally assumed in this age group (Sundhedsstyrelsen (National Board of Health), 1998). This finding is in accordance with the findings of others (Reference Addington and AddingtonAddington & Addington, 1992; Reference Young, Nuechterlein and MintzYoung et al, 1998) and confirms the observation that patients with first-episode psychosis are a high-risk group with regard to suicidal behaviour.
One suicide and one unaccounted death, where suicide could not be excluded, occurred in the sample during the follow-up period. The annual suicide rate is thus found to be 0.3%. Epidemiological studies suggest that suicide could be expected in 1-2% of patients with first-episode schizophrenia during the first year after first admission to a psychiatric department (Reference MortensenMortensen, 1995). Although the study group might not be completely comparable with the epidemiological sample studied by Mortensen, the number of suicides is possibly lower than to be expected in this high-risk group. A preventive effect of participating in a scientific study with repeated interviews could be a possible explanation for this finding.
Limitations
Previous reports from the OPUS project have shown positive effects of the integrated psychiatric treatment on positive and negative symptoms and on patient satisfaction (Reference Nordentoft, Jeppesen and KassowNordentoft et al, 2002). It could be anticipated that these promising results would also influence suicidal behaviour, but this interim analysis of the sample is too small to detect possible differences. However, in many studies, hopelessness has been found to be an important predictor of suicide and suicide attempt, and it is promising that it was reduced significantly in the integrated treatment group. Hopelessness was significantly lower at the 1-year follow-up in the group receiving integrated psychiatric treatment than in the standard treatment group. Assessment of hopelessness was based on the answer to one specific item in SCAN, and although this might be representative, the Hopelessness Scale (Reference Bech, Weissmann and LesterBech et al, 1974) would most likely be a more valid measure of this variable.
Previous studies
Hawton and co-workers found in their comprehensive review of the literature on the effect of repeated deliberate self-harm that, among psychosocial treatment programmes, only dialectical behaviour therapy has a documented positive effect, and there remains considerable uncertainty about which forms of psychosocial and physical treatments of patients who harm themselves are most effective (Reference LinehanLinehan, 1991; Reference Hawton, Arensman and TownsendHawton et al, 1998). The integrated treatment in the OPUS project, although also dealing with suicidal ideation, was not focused especially on this subject. When the subject was discussed in individual treatment or in multi-family groups, crisis plans were often developed together with the patient but the staff members had not received training in any specific treatment developed with the aim of reducing suicidal thinking.
Characteristics of the population
The finding that suicide attempts were more likely to precede contact with mental health services among younger patients implies that a suicide attempt is likely to ‘push’ a young person into treatment at an early phase. However, this is contradictory to the finding of no significant differences between patients with and without previous suicide attempts with regard to duration of untreated psychosis.
Several studies of attempted suicide have found that female gender and previous suicide attempts occur more frequently among those attempting suicide than in the general population. Some studies have reported that being a parent, being married, or having an intimate relationship are protective concerning suicidal behaviour. In our study, the finding that women are over-represented among patients attempting suicide could be replicated, but no protective effect of being a parent, being married, or having an intimate relationship was found. On the contrary, attempted suicide during the follow-up period occurred more frequently among patients who had an intimate relationship. This finding might suggest that risk factors in this selected population are different from those often identified in studies of suicide attempts in a defined catchment area.
Predictors of suicidal behaviour
The finding of thought disorder being inversely associated with suicidal thoughts, suicidal plans and suicide attempt during follow-up might suggest that the most disturbed patients were too impaired concerning cognitive function to form suicidal thoughts and suicidal plans and to conduct an attempted suicide. This is in agreement with the observation of Fenton (Reference Fenton2000) that patients with schizophrenia who are most likely to recover or experience a good outcome are those who also have the greatest risk for suicide. Several previous studies have pointed out that psychosis, hopelessness and depression are important correlates to suicidal behaviour and suicidal ideation (Reference Drake and CottonDrake & Cotton, 1986; Reference Hu, Sun and LeeHu et al, 1991; Reference Addington and AddingtonAddington & Addington, 1992; Reference Bartels, Drake and McHugoBartels et al, 1992; Reference Shuwall and SirisShuwall & Siris, 1994; Reference Young, Nuechterlein and MintzYoung et al, 1998; Reference Saarinen, Lehtonen and LonnqvistSaarinen et al, 1999; Reference Taiminen, Huttunen and HeilaTaiminen et al, 2001). In our study, we found that hopelessness, depression and hallucinations and delusions were associated with suicidal ideation or suicidal behaviour.
One possible explanation for the finding that thought disorder was inversely associated with suicidal ideation and suicide attempt is that the patients with thought disorder represent a group with long duration of untreated psychosis, and thus are selected positively by surviving a long risk-period (healthy worker effect). This hypothesis was tested by examining the association between suicidal behaviour and duration of untreated psychosis. No association with suicidal behaviour was found, either in univariate analysis or in the analysis of possible interactions between duration of untreated psychosis and the sub-scales of SAPS. There was no statistically significant difference between patients with and without thought disorder with regard to duration of untreated psychosis.
Drake et al (Reference Drake, Gates and Whitaker1985) found that predictors of suicide and suicide attempt were different. In our study, we found that correlates of suicide attempt and suicidal ideation were different, thus indicating that even though suicidal ideation and suicidal attempts are predictors of later suicide, prediction of suicide remains very complex. There is therefore a need for the development of special treatment programmes focused on suicidal behaviour.
CLINICAL IMPLICATIONS
-
▪ Integrated psychiatric treatment was superior to standard treatment concerning hopelessness. There is a need for the development of special treatment programmes focused on suicidal behaviour.
-
▪ Suicidal ideation and suicidal behaviour were very common in the study group of young, patients with first-episode psychosis.
-
▪ Being a female, having attempted suicide the year before the baseline interview and hopelessness and hallucinations reported at the baseline interview were predictors of suicide attempts during the follow-up period. Hallucinations and attempted suicide were the most important predictors of suicide attempts in the follow-up period.
LIMITATIONS
-
▪ The integrated treatment, although more intensive, was not especially focused on suicidal behaviour and ideation.
-
▪ The sample size is too small to allow evaluation of suicide as an outcome measure.
-
▪ Reports of suicide attempts were based solely on patients' information.
Acknowledgements
The OPUS study was funded by grants from the Danish Ministry of Health (jr. nr. 96-0770-71), Danish Medical Research Council (jr. nr. 9601612 and 9900734) and Copenhagen University. Kenn Schultz Nielsen assisted with computer programming and Philip Hougaard supervised the statistical analyses.






eLetters
No eLetters have been published for this article.