


On the morning of 11 September 2001 four aeroplanes were hijacked by 19 terrorists who transformed them from a means of mass transportation to a means of terror and destruction, killing themselves, a total of 233 passengers, 33 crew members and some 3000 on the ground in the USA (Reference Alexander and SwetnamAlexander & Swetnam, 2001). The 11 September 2001 attack on the World Trade Center was probably the largest disaster caused by humans in the history of the USA (Reference Galea, Vlahov and ResnickGalea et al, 2002). In the first four days after the attack it became clear that the scope of the four separate attacks (including loss of life, property damage and financial consequence) was unprecedented and could result in substantial psychological sequelae, not just in the USA but in other countries (Reference Galea, Vlahov and ResnickGalea et al, 2002). Lee et al (Reference Lee, Isaac and Janca2002) reported that more than 40% of people across the USA experienced substantial symptoms of stress after the attacks of 11 September 2001. Post-traumatic stress disorder (PTSD) and depression among residents of Lower Manhattan, New York, were twice the borderline rates 5–8 weeks after the attack (Reference Lee, Isaac and JancaLee et al, 2002). People who were not directly exposed to the terrorist attack were also at a significant risk of developing PTSD (Reference Lee, Isaac and JancaLee et al, 2002). The repeated showing of the tragic events of 11 September 2001 on television world-wide – scenes of deliberate acts of simultaneous homicide and suicide with unedited live scenes of victims jumping from the World Trade Center towers – is expected to have had an impact on the behaviour of some people, particularly those who harbour suicidal ideation or homicidal tendencies. There is no currently available psychiatric literature on the effect of such suicide terrorism on suicide and homicide. The aim of this observational study is to explore the effect of 11 September 2001 on the rate of suicide and homicide in England and Wales.
METHOD
Design and data collection
An observational study was made using routinely collected data. Daily counts of suicide (ICD–9 codes: E950–E959), death from undetermined injury (E980–E989) and homicide (E960–E969) (World Health Organization, 1977), reported in England and Wales between 1 June to 31 December for the years 1999, 2000 and 2001 were obtained from the Office for National Statistics. I used suicide and homicide data for England and Wales for 1979–2001 (requested previously from the Office for National Statistics for an unrelated study) to provide annual and monthly counts of suicide, undetermined death and homicide. The term ‘suicide’ used in the study refers to suicide and undetermined death combined. The nationally collected routine data from the Office for National Statistics were accepted as being as reliable and complete as possible.
Daily counts of suicide and homicide were aggregated into weekly counts from Tuesday to Monday, so that they would contain the week starting with Tuesday 11 September 2001. Aggregation of data was carried out for the three years 1999, 2000 and 2001.
Statistical analysis
Weekly means of suicide and homicide before and after the week of 11 September 2001 were compared. Any differences were compared with figures observed during the same periods in 1999 and 2000 as a means of adjusting for seasonal variations and the recent decline in suicide (Reference Kelly and BuntingKelly & Bunting, 1998).
The goodness-of-fit χ2-test was used to compare observed and expected counts of monthly and annual suicides and homicides. The Kruskal–Wallis test was used to compare counted weekly data during the 3 months before and after 11 September and to compare daily, weekly and monthly means when applicable (e.g. means of suicide and homicide computed for previous years).
Daily variations in suicides occurring in September for 2001 and previous years and variations in observed weekly counted mortality data for 2001 compared with expected data based on figures from previous years were assessed by applying control chart statistics: application of time-series methods to assess the occurrence of events such as suicide and homicide over a period of time based on the Poisson mean. If the data follow a distribution that indicates a regular occurrence of events (such as suicide) over a period of time then the variance is equal to the mean (C) and the standard deviation is equal to the square root of the average C, that is:
Variation in data over a period of time is assessed within an upper control limit and a lower control limit (Reference Wetherill and BrownWetherill & Brown, 1994):
Data occurring between the upper and lower control limits are expected to include 99% of the total data and the variability occurs by chance. Observed suicide data that fall outside these limits are unlikely to have occurred by chance (P < 0.01) and indicate significant deviation from the expected.
RESULTS
Suicide
Examination of suicides and undetermined deaths reported in the month of September for each year between 1979 and 2001 revealed that suicide reported in September 2001 had the lowest frequency compared with previous years (χ2=107; d.f.=22; P < 0.0001) (Table 1). With a single degree of freedom contrast for 2001 v. all other years, this yielded χ2=14 (P < 0.001). Total annual suicides over the same period did not differ significantly (P > 0.05) but there is an overall reduced rate trend since 1992 (Fig. 1). Figure 2 shows monthly suicides in 2001 compared with the monthly means computed for ten years in the 1980s and 1990s, respectively. The number of suicides reported in September 2001 appears to be significantly lower than in other months within 2001 (χ2=30, d.f.=11; P < 0.01) and compared with September means in the previous two decades (P < 0.05). The number of daily suicides reported in the month of September and the daily mean values for 1999 and 2000 are shown in Fig. 3. The mean daily suicide rate in 2001 was 13.8 (s.d.=3), which is significantly lower than the daily mean of 16.8 (s.d.=4) reported in previous years, with a mean difference of 3 (P < 0.05). On 11 September 2001 there was an interesting drop in the number of daily suicides to eight incidents. It should be noted that the event of 11 September was reported in the UK on the afternoon of the same day. However, the variation did not reach statistical significance, not exceeding the lower control limit computed as the Poisson mean of expected daily suicide minus three standard deviations (P > 0.01).
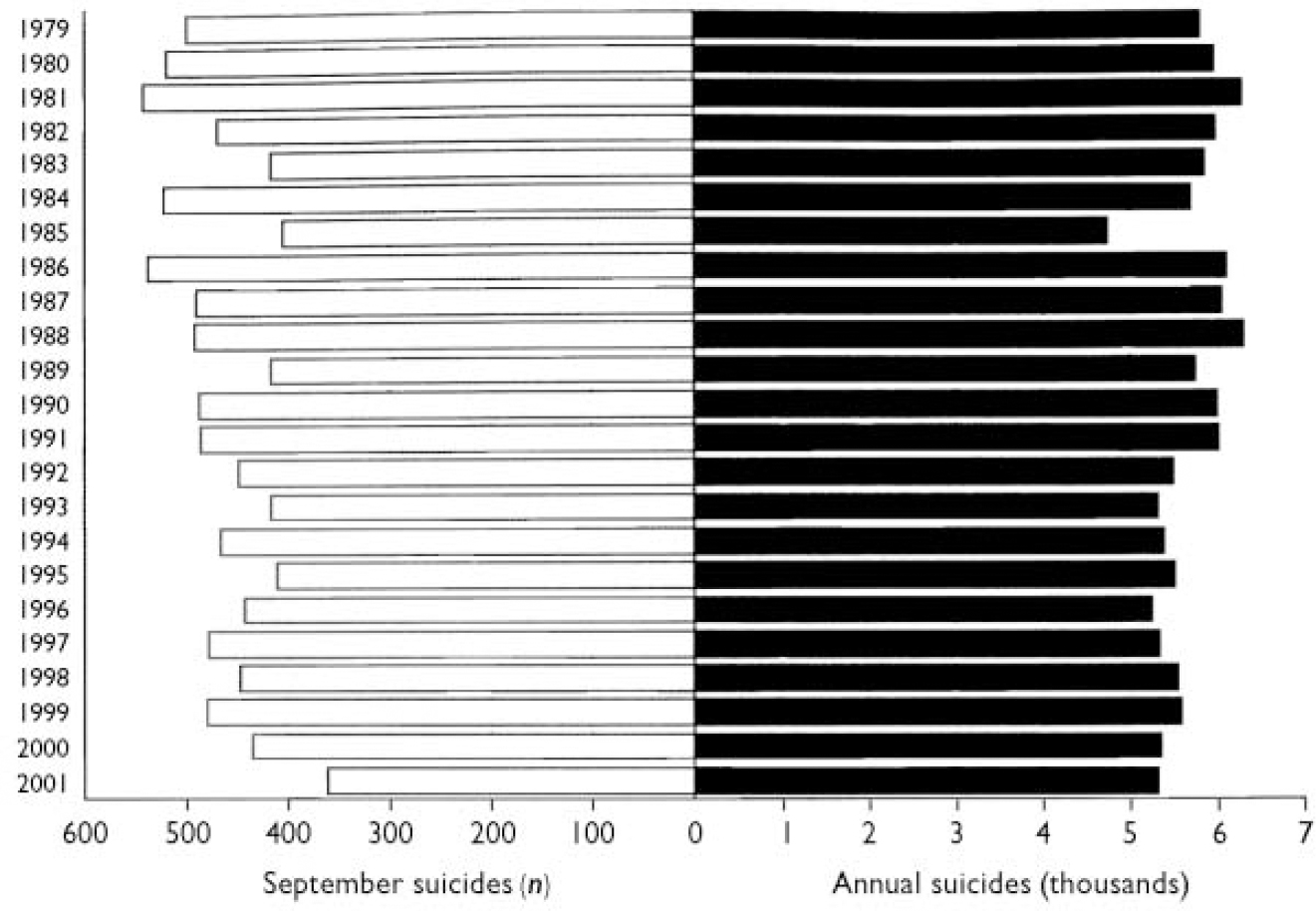
Fig. 1 September suicides and annual suicides in England and Wales 1979–2001.
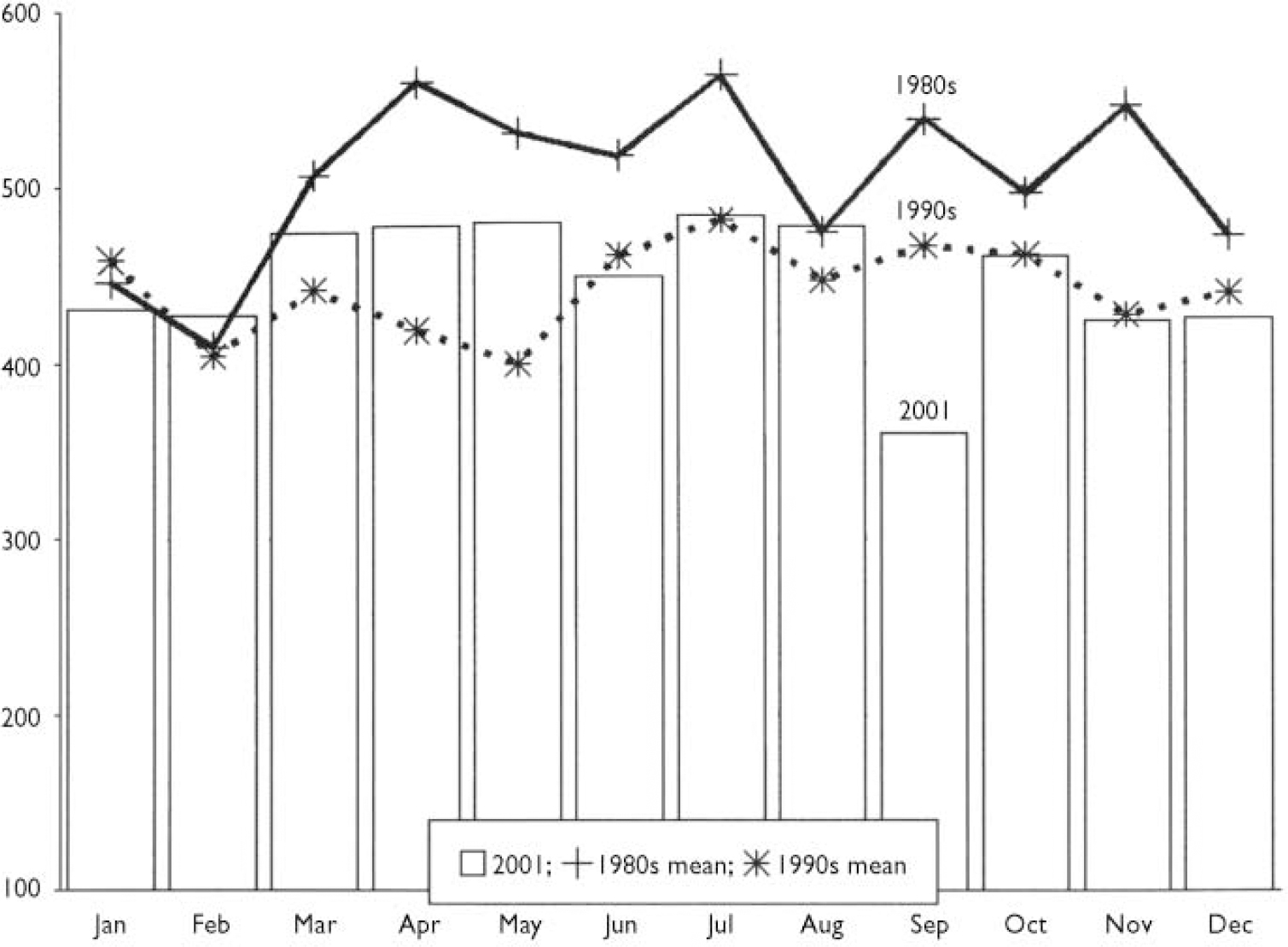
Fig. 2 Mean monthly suicides in England and Wales in the 1980s, 1990s and 2001.
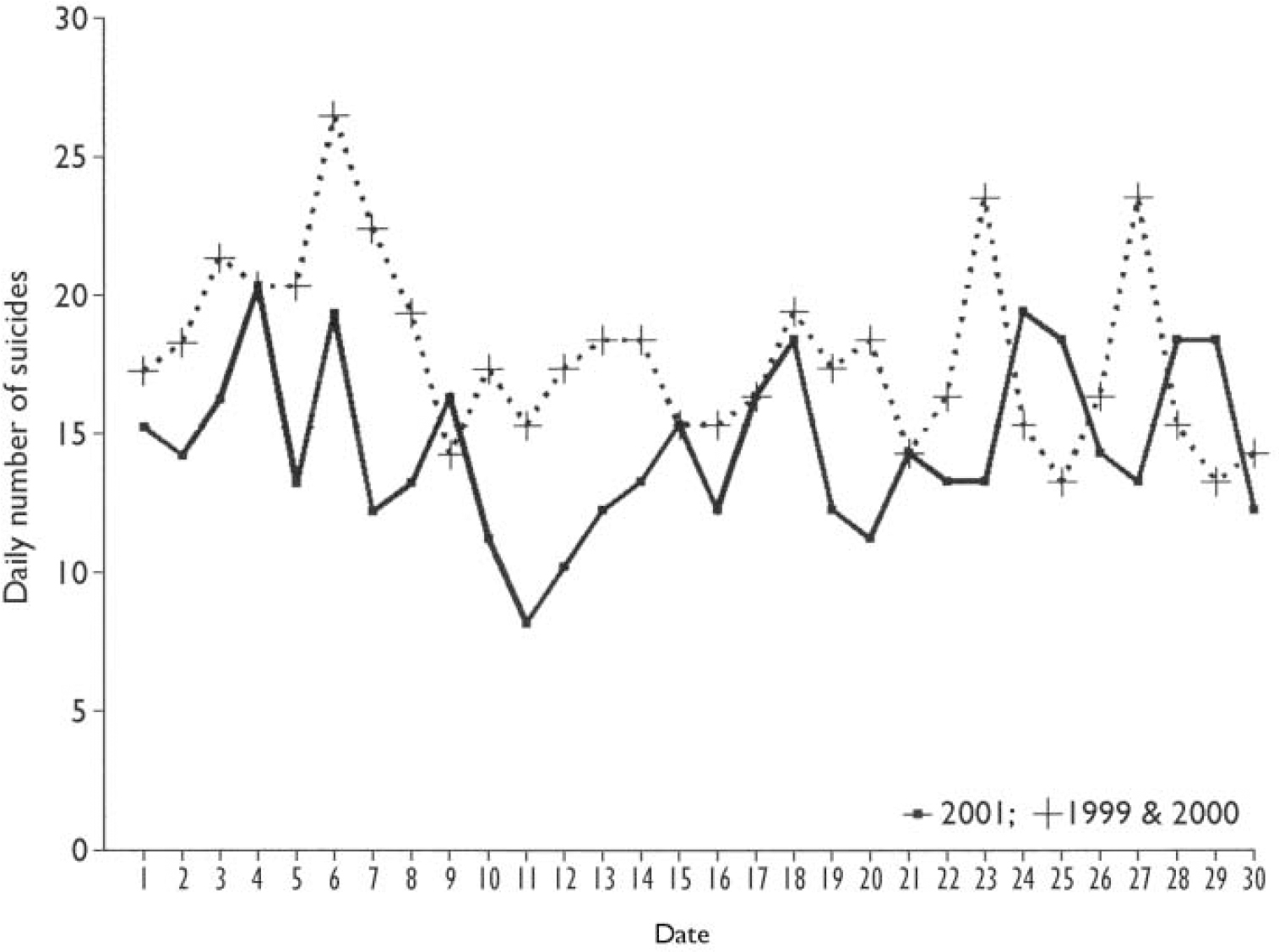
Fig. 3 September daily suicides in England and Wales in 2001 compared with 1999 and 2000.
Table 1 September suicide and undetermined death and homicide in England and Wales 1979-2001
| Year | Suicides and undetermined deaths | Homicides | ||
|---|---|---|---|---|
| September | Total annual | September | Total annual | |
| 1979 | 500 | 5802 | 40 | 524 |
| 1980 | 520 | 5948 | 24 | 377 |
| 1981 | 542 | 6267 | 25 | 192 |
| 1982 | 469 | 5967 | 18 | 367 |
| 1983 | 417 | 5849 | 16 | 306 |
| 1984 | 522 | 5689 | 17 | 357 |
| 1985 | 404 | 4739 | 21 | 347 |
| 1986 | 538 | 6095 | 16 | 340 |
| 1987 | 491 | 6044 | 14 | 346 |
| 1988 | 492 | 6286 | 10 | 286 |
| 1989 | 416 | 5744 | 18 | 276 |
| 1990 | 488 | 5982 | 17 | 130 |
| 1991 | 486 | 6003 | 15 | 132 |
| 1992 | 448 | 5502 | 16 | 138 |
| 1993 | 416 | 5323 | 29 | 521 |
| 1994 | 466 | 5383 | 17 | 364 |
| 1995 | 411 | 5516 | 22 | 353 |
| 1996 | 442 | 5243 | 22 | 313 |
| 1997 | 479 | 5338 | 14 | 290 |
| 1998 | 447 | 5545 | 27 | 285 |
| 1999 | 480 | 5576 | 24 | 293 |
| 2000 | 434 | 5352 | 26 | 380 |
| 2001 | 360 | 5324 | 18 | 276 |
Figures 4, 5, 6 show the reported mean number of weekly suicides for men and women 12 weeks before and after the week of 11 September 2001. The average total number of suicides in the week starting 11 September 2001 was 100, which is not significantly different from the overall mean in the 12 weeks before and after the event: 109 and 102, respectively (P > 0.05). However, this was significantly lower than the observed value of 120 during the same September week in the previous years (P < 0.05).
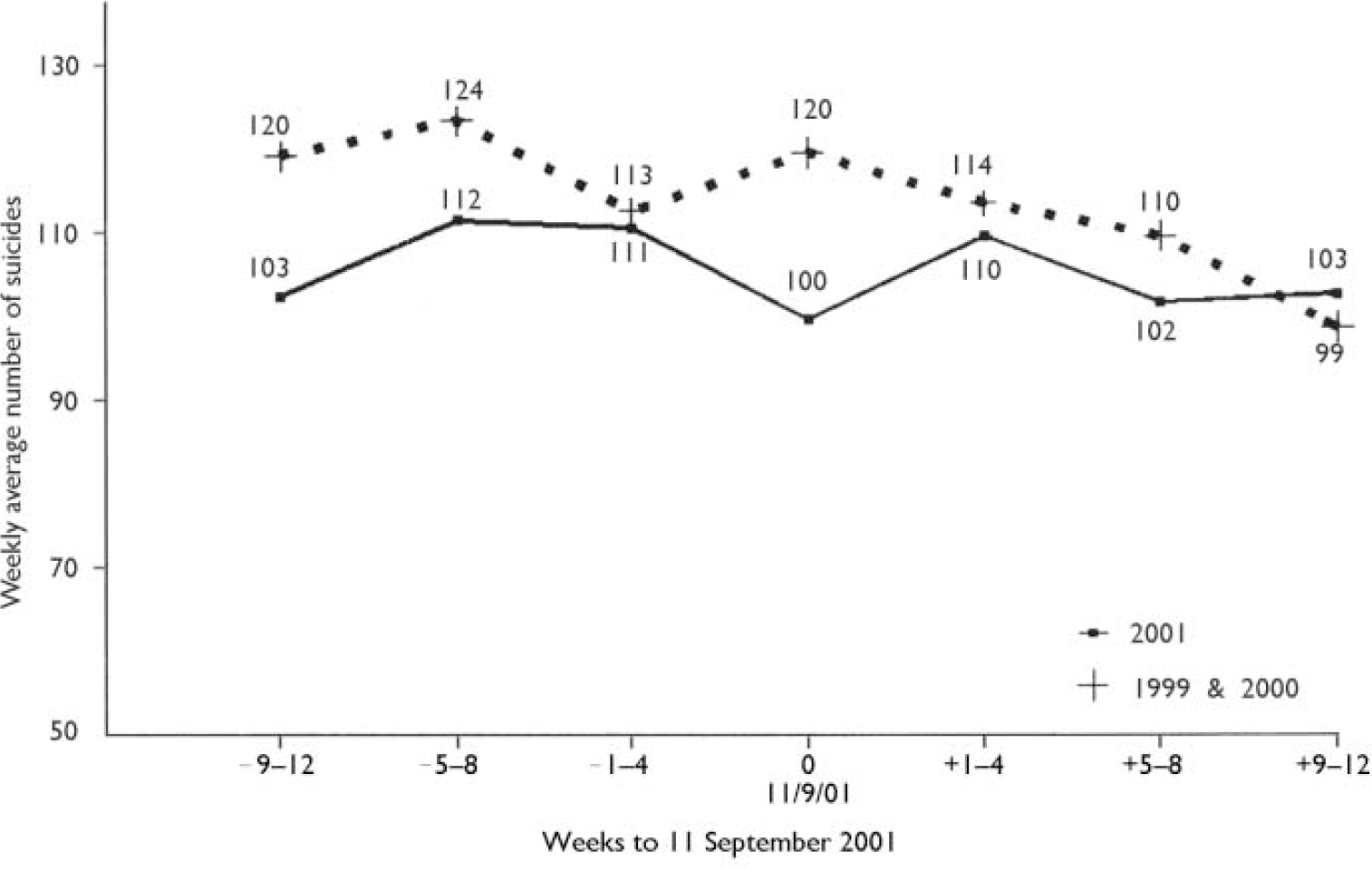
Fig. 4 Weekly mean suicide in England and Wales in 2001 compared with 1999 and 2000.
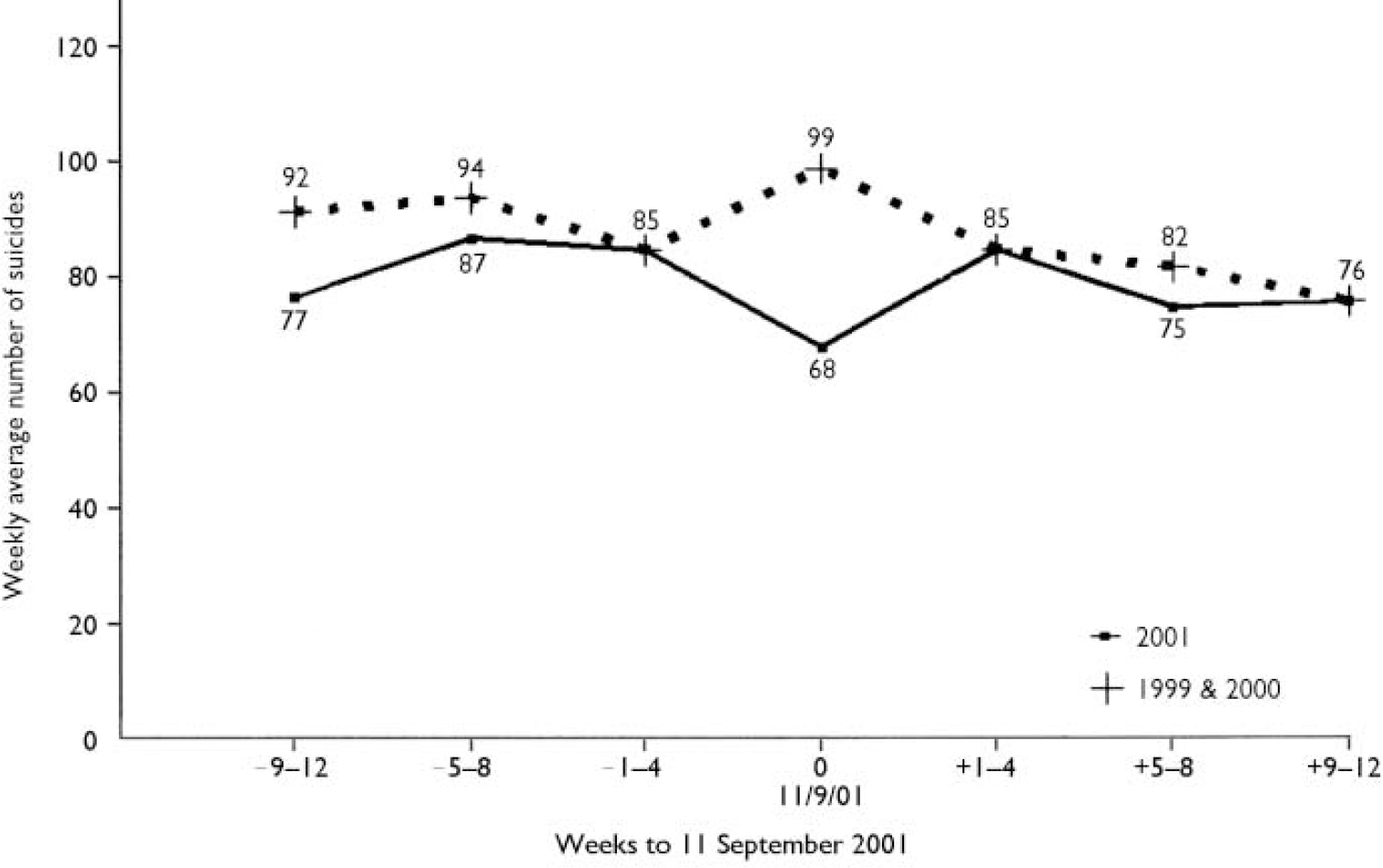
Fig. 5 Male weekly mean suicides in England and Wales in 2001 compared with 1999 and 2000.
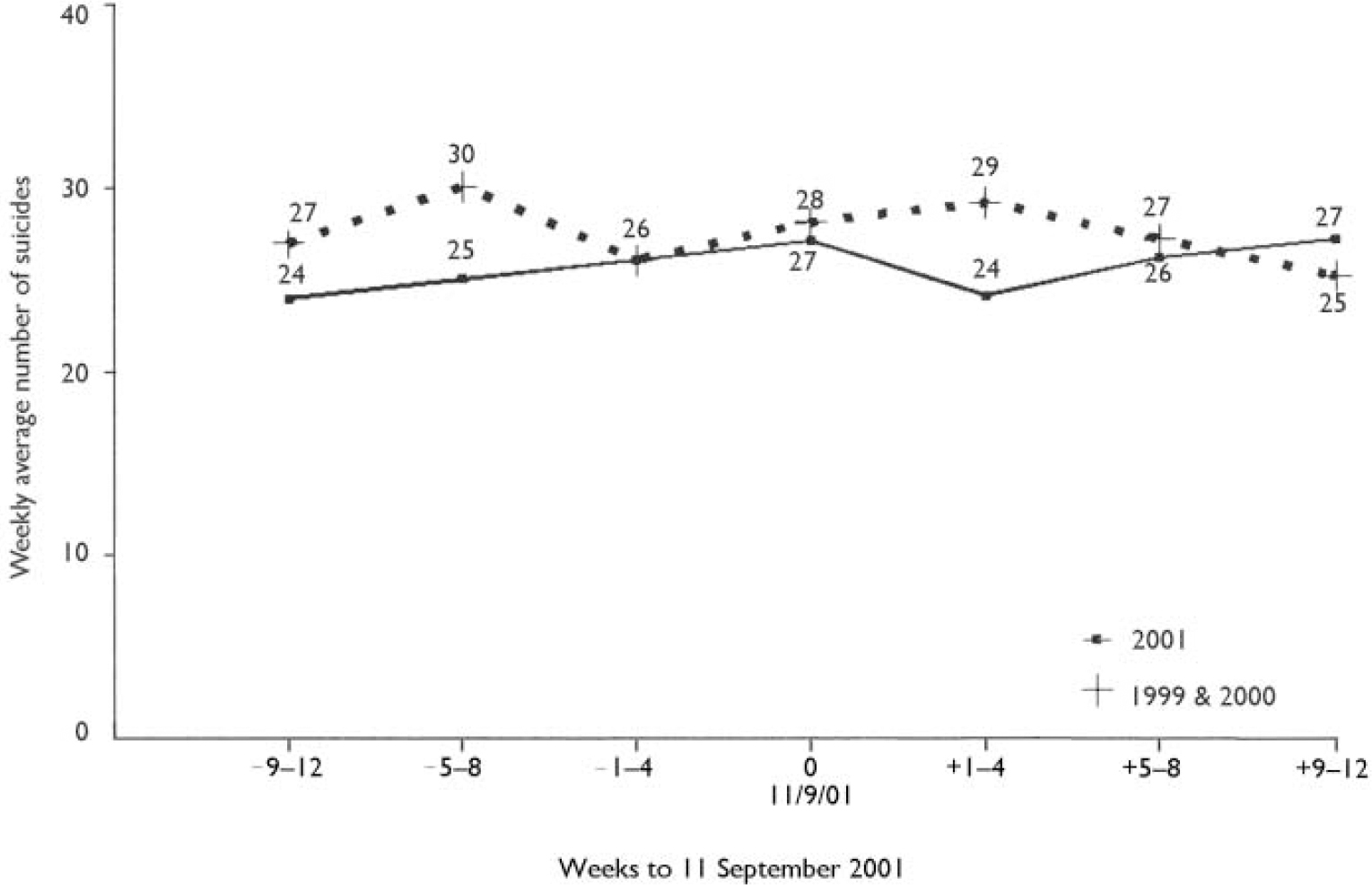
Fig. 6 Female weekly mean suicides in England and Wales in 2001 compared with 1999 and 2000.
The number of male suicides in the week of 11 September 2001 was 68, which is significantly lower than the overall mean in the 12 weeks before and after the event: 82 and 84, respectively (P < 0.05). The number of reported suicides in the week of 11 September 2001 also was significantly lower than the 99 observed during the same week in previous years (P < 0.05) (Fig. 5).
The reduction in male suicides was more evident in men aged less than 50 years but the difference did not reach statistical significance. Over the four weeks after 11 September 2001 the reduced suicide counts appear to have reverted back to the expected level for 2001 before the event. The reduction in male suicides during the week of 11 September did exceed the control chart lower control limit at P < 0.05 (i.e. expected mean — two standard deviations) but was not significant at P < 0.01 (i.e. expected mean — three standard deviations).
The reduction in female suicides did not reach statistical significance and occurred during the four weeks following the attack and not during the same week as in men (Fig. 6).
Homicide
September-reported homicides and total annual homicides in England and Wales between 1979 and 2001 are shown in Table 1. Figure 7 shows the number of homicides in 2001 compared with the monthly means computed for ten years in the 1980s and 1990s, respectively. No significant difference was found regarding the homicides that occurred in September 2001. However, the graph shows a significant trend in the lower rate of homicide after August to December (χ2=32, d.f.=11; P < 0.01), which is evident in 2001, the 1980s and the 1990s. Figure 8 illustrates the same trend for homicide. No significant difference in homicide weekly means was found before or after 11 September 2001. The mean number of weekly homicides was higher in 2001 compared with previous years except for the week of 11 September (Fig. 8). The mean difference, however, did not reach statistical significance.
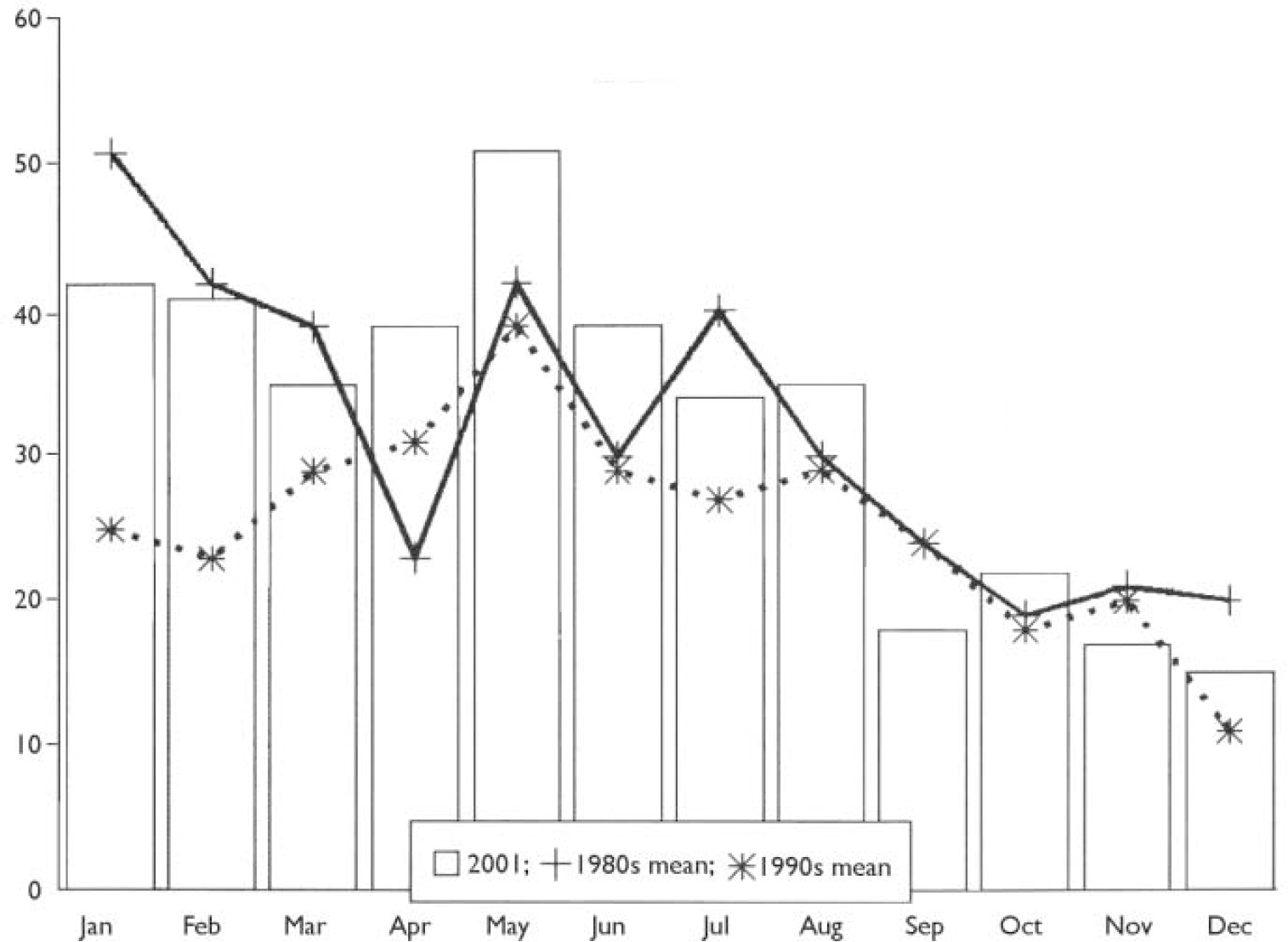
Fig. 7 Mean monthly homicides in England and Wales in the 1980s, 1990s and 2001.
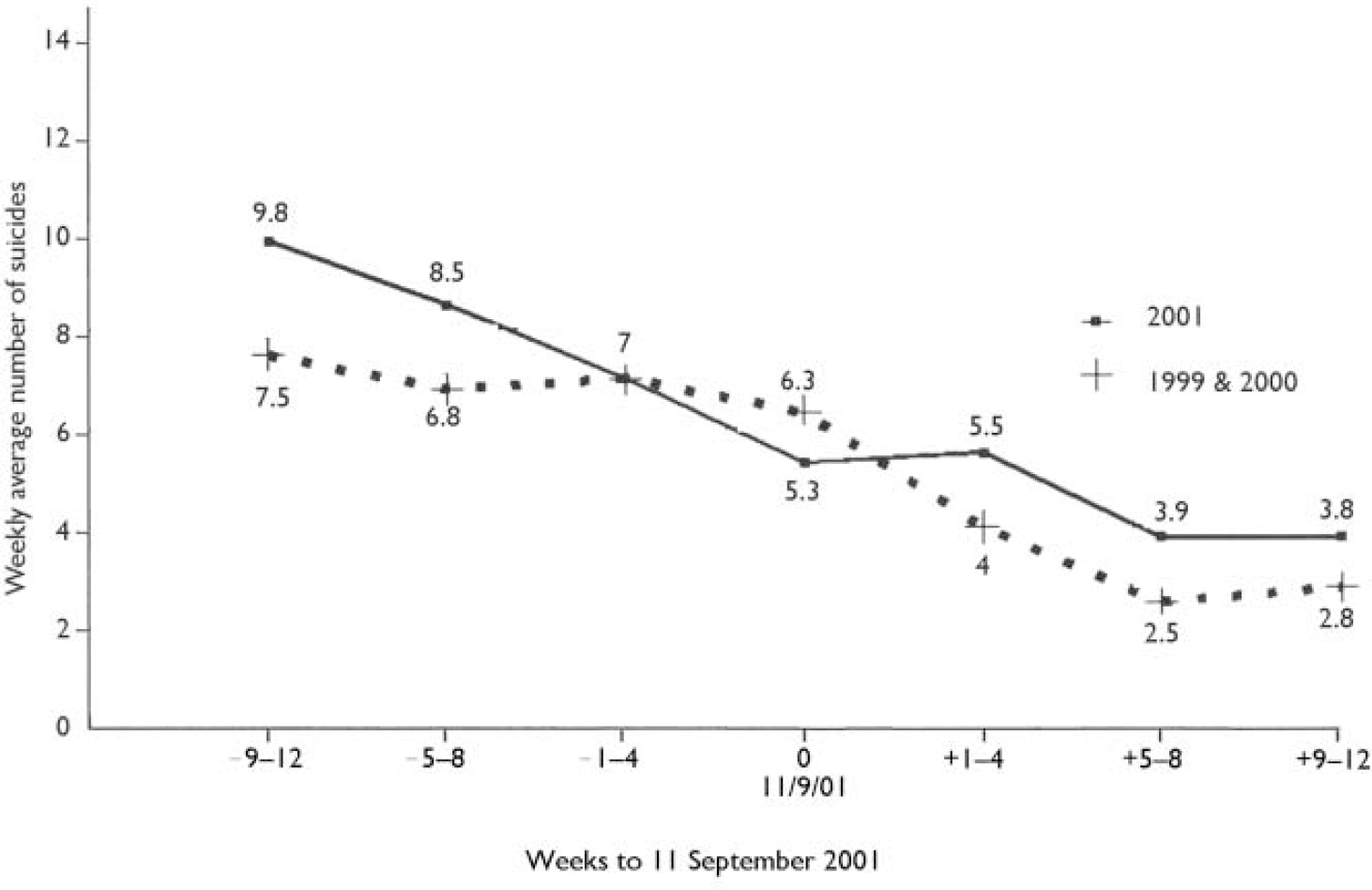
Fig. 8 Weekly mean homicides in England and Wales in 2001 compared with 1999 and 2000.
DISCUSSION
Interpretation of the findings
There is evidence to suggest that the number of suicides reported in the month of September 2001 was significantly lower than in other months in the same year and any September of the previous 22 years in England and Wales after adjusting for seasonal variations and secular trends, including the recent decline in suicide (Reference Kelly and BuntingKelly & Bunting, 1998). The reduction in male suicides occurred in the week starting Tuesday 11 September 2001 and tended to be in middle-aged men. The reduction in female suicides did not reach statistical significance and occurred during the four weeks following the attack and not during the same week as in men, possibly as a delayed effect.
There was no evidence of a similar reduction in reported homicides. Homicide was observed to have a consistent seasonal increase in May and a decline after August but this was unrelated to the events of 11 September.
Although there is an association between suicide and suicidal behaviour and homicide and violence to others (Reference Van PraagVan Praag, 2000), there is no literature currently available detailing the effect of suicide terrorism, particularly the attacks of 11 September, on the rate of suicide and homicide.
Murder and suicide may be inseparable as both assert power over death (Reference Dein and LittlewoodDein & Littlewood, 2000). Individual murderers may seek the death penalty for themselves through suicide. Simultaneous suicide and homicide has become a hallmark of suicide terrorism (Reference SalibSalib, 2003). Suicide terrorism, which is seen by the perpetrators as a mode of warfare, is aimed at causing devastating physical damage and inflicting profound fear on an entire population rather than just the victims of the actual attack, aided by extensive, dramatic and spectacular media coverage (Reference SalibSalib, 2003). There is a need for responsible media reporting of terrorist acts, given the potential mental health impact. Media reporting of deaths and disaster-related television viewing can cause severe distress and also influence the suicide rate (Reference Bollen and PhillipsBollen & Phillips, 1982).
The televised national shock and public display of grief over the death of Diana, Princess of Wales and after her funeral in 1997 was shown to have influenced the rate of suicidal behaviour and deliberate self-harm (Reference Hawton, Harriss and ApplebyHawton et al, 2000). The repeated viewing of the tragic scenes of 11 September – live acts of simultaneous mass homicide and suicide – appears to have had a brief but significant inverse effect on suicide in England and Wales. ‘Imitative suicide’ (Reference Bollen and PhillipsBollen & Phillips, 1982) was reported in one incident shortly after 11 September (the ‘shoe bomber’). It is not clear why the reduction in suicide was only evident in men but this may be related partly to the fact that all the terrorists were men and the visibly distressed fire-fighters and other rescue workers were men. The temporary reduction in suicide associated with 11 September is probably not dissimilar to what has been reported during major wars. Suicide rates declined during the world wars of the 20th century, both in men and women and in participating and non-participating nations (Reference LesterLester, 1995). Also, following the assassination of President John F. Kennedy in 1963 there was a reported reduction in suicide rate in the USA (Reference BillerBiller, 1977).
The finding of this study supports Durkheim's theory that periods of external threat and major events create group integration within society and lower the suicide rate through the impact on social cohesion (Reference DurkheimDurkheim, 1897). It also supports Durkheim's views that ‘imitation’ does not significantly affect suicide rates, a view that is not shared explicitly by modern sociologists (Reference Bollen and PhillipsBollen & Phillips, 1982). Suicide and homicide data for 2002 were not available at the time of writing this paper to assess the effect of the first anniversary of 11 September 2001.
Limitations of the study
One of the main problems associated with using routinely collected data, no matter how reliable and complete, is that of misclassification of data. It must be emphasised that it is impossible to rule out entirely the effect of chance fluctuations in suicide rate or other influences that might explain the findings. The study did not examine whether the observed reduction in male suicides was attributable to a drop in the use of violent methods (particularly explosives, self-immolation and falling from heights) or to a reduction in non-violent deaths. The study did not examine the effect of 11 September on deliberate self-harm behaviour.
Future research
The study findings could be tested by future similar studies from the USA and other countries that may assess the effect of 11 September on suicide and homicide in persons with mental illnesses and also on deliberate self-harm behaviour, areas that the present study did not cover. The effect of ethnic, religious and cultural difference on the rate of suicide after 11 September 2001 within the USA itself and elsewhere also should be explored.
The effect of 11 September anniversaries on suicide and homicide rates, especially with further detailed and dramatic media coverage, may be of interest to future researchers.
Another area for future research is to assess the frequency, targets, locations, groups and outcome of suicide bombing and other forms of suicide–homicide acts after 11 September 2001.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ The number of suicides reported in the month of September 2001 was significantly lower than in other months in the same year and in any September of the previous 22 years in England and Wales.
-
▪ The reduction in male suicide occurred mainly in the week starting Tuesday 11 September 2001. The reduction in female suicide occurred during the four weeks following the attack, possibly as a delayed effect. There was no evidence of a similar effect on homicide.
-
▪ The finding of this study supports Durkheim's theory that periods of external threat create group integration within society that lowers the suicide rate.
LIMITATIONS
-
▪ It is impossible to rule out entirely the effect of chance fluctuations or other influences that might explain the findings.
-
▪ The effect of 11 September 2001 on deliberate self-harm is relevant but was not examined in this study.
-
▪ There could be misclassification in routinely collected data.
Acknowledgements
The author is grateful to Mrs Emma Jones and Miss Katie Spencer from the Beckett Day Unit, Hollins Park, for their help in preparing this manuscript. Thanks also go to Miss Bernadette Hayes and John Bentley at Hollins Park, the 5 Boroughs Partnership Trust and the Office for National Statistics and to Janice Hogan, Sanofi-Synthelabo, for her support.










eLetters
No eLetters have been published for this article.