


After more than 150 years of research on the subject, it is now well established that mental disorders are associated with excess mortality. Reference Brown1–Reference Alstrom3 The association between depression and excess mortality has been shown in several hundreds of studies in many different populations, including community samples, heart disease patients, cancer patients, stroke patients and patients with diabetes. Reference Cuijpers and Smit4–Reference Lin, Heckbert, Rutter, Katon, Ciechanowski and Ludman15 It is not yet clear, however, whether the increased mortality rates only exist in major depressive disorder, or also extend to subthreshold depression. Many studies examining excess mortality in depression have used a cut-off score on self-report instruments to indicate the presence of depressive symptoms. It is possible that the increased mortality rate in these samples can be fully attributed to the people with major depression. However, it is also possible that the increased mortality rate exists not only in major depression but also in subthreshold depression. Many studies have shown that subthreshold depression in itself is a clinically relevant condition, with decreased levels of health-related quality of life, increased use of health services and increased economic costs when compared with healthy controls. Reference Cuijpers and Smit16–Reference Goldney, Fisher, Dal Grande and Taylor19 When people with subthreshold depression are compared with those who have a major depressive disorder, however, it is typically found that on an individual level health-related quality of life, health service use and economic costs are more affected in major depression than in subthreshold depression. From this perspective it would be expected that if there is an association between excess mortality and subthreshold depression it would be less strong than in major depression. Because the prevalence of subthreshold depression is higher than that of major depression, earlier research has found that the impact of subthreshold depression on (for example) economic costs is comparable with the costs of major depression. Reference Cuijpers, Smit, Oostenbrink, de Graaf, ten Have and Beekman20 The same may be true for the impact of subthreshold and major depression on mortality. In order to examine these questions, a meta-analysis of studies in which participants with major depression as well as those with subthreshold depression were included would be most informative. These studies allow comparison of major and subthreshold depression directly with each other and establish whether excess mortality is higher in major depression than in subthreshold depression. We decided to conduct such a meta-analysis.
Method
Studies were traced by several methods. First, we conducted comprehensive literature searches (up to November 2011) in three bibliographic databases (PubMed, PsycINFO and EMBASE). In these searches we combined words indicating depression (such as major depression, mood disorder, depression, depressive), mortality (such as death, survival), and prospective design (such as incidence, follow-up studies, longitudinal studies, prospective studies). Both text and keywords were used. We also checked the references of included studies, as well as the references of earlier meta-analyses examining the association between depression and mortality. Reference Saz and Dewey5–Reference Pan, Sun, Okereke, Rexrode and Hu13,Reference Cole21–Reference Van den Akker, Schuurman, Ensinck and Buntinx27 We retrieved the full text of papers reporting studies that possibly met inclusion criteria. Full-text papers were examined by two independent raters for possible inclusion. Disagreements were solved by discussion and if necessary a third rater was involved.
Studies were includedif theyexaminedtwo groups: participants with a major depressive disorder (established with a diagnostic interview; either major depression alone or combined with dysthymia); and participants with subthreshold depression (established through a self-report depression measure or a diagnostic interview) but no major depressive disorder. Studies also had to have a prospective design and report all-cause mortality at follow-up, for both groups. We included studies in any target group (community samples and specific patient groups), as well as case–control studies. Studies were excluded when insufficient data were presented to calculate the relative risk of dying in the group with major depression compared with subthreshold depression (main analysis). We also excluded studies based on trials examining the effects of an intervention, studies in children and adolescents, and studies in languages other than English, German and Dutch.
Data extraction and quality assessment
We rated the number of deaths in the group with major depression, the group with subthreshold depression and the non-depressed control group. When these data were not reported in the papers, we contacted the first authors of the studies. If no answer was received within 2 weeks, a reminder was sent. Additional data on six studies were received from the researchers (see Acknowledgements). For the subgroup (moderator) analyses we rated several characteristics of the included studies: target population (community sample, heart disease patients, other patient group); percentage of women in the target population (<40%, 40–60%, >60%); definition of subthreshold depression (scoring above a cut-off on self-report measure v. fulfilling diagnostic DSM–IV criteria for minor depression); follow-up period (<2 years, 2–5 years, >5 years); and country where the study was conducted (USA, Europe, other).
In order to assess the validity of the studies we used a quality rating scale that was based on the instrument developed by Hayden et al. Reference Hayden, Cote and Bombardier28 We adapted the specific items for use with the studies in this field, but retained five of the six basic areas of potential bias that are assessed with this instrument: study participation (the study sample represents the population of interest on key characteristics), study attrition, adequate outcome measurement, adequate measurement of confounding variables and adequate statistical analysis. The sixth area of potential bias (the prognostic factor of interest is adequately measured) was not used because an adequate measure of depression (major and subthreshold) was an inclusion criterion for this study. The rating instrument is presented online in Appendix DS1, and the ratings for the included studies are presented in online Table DS1.
Meta-analyses
For each study we calculated the relative risk of dying during the study in the group with major depression compared with the group with subthreshold depression. This was the main comparison for each study. However, all studies also included a non-depressed control group. We also calculated the relative risks of dying for the groups with major depression and subthreshold depression compared with the non-depressed group. Because we did not collect all studies that compared major depression or subthreshold depression with non-depressed controls, these comparisons should be considered with caution; we conducted these analyses only to confirm that earlier associations between depression and excess mortality were also found in our sample of studies.
Because all studies reported the exact number of deaths in the depressed and non-depressed groups, unadjusted relative risks (RRs) were calculated for all studies. None of the studies reported RRs (comparing major depression with subthreshold depression) that were adjusted for demographics or other variables. Therefore, all analyses were conducted with unadjusted RRs. To calculate pooled RRs we used the computer program Comprehensive Meta-analysis for Windows version 2.2.021. As we expected considerable heterogeneity among the studies, we decided to calculate the pooled RR using a random effects model. Because the actual heterogeneity we found was low, we additionally conducted the meta-analyses according to the fixed effects model.
In order to examine heterogeneity we calculated the I 2 statistic, which is an indicator of heterogeneity in percentages. A value of 0% indicates no observed heterogeneity, and larger values show increasing heterogeneity (25% low, 50% moderate, 75% high). Reference Higgins, Thompson, Deeks and Altman29 We calculated 95% confidence intervals around I 2, Reference Ioannidis, Patsopoulos and Evangelou30 using the non-central χ2-based approach within the ‘heterogi’ module for Stata/MP11.0 for Mac. Reference Orsini, Higgins, Bottai and Buchan31 To test for significant heterogeneity we also calculated the Q statistic, but only report whether this was significant or not. Subgroup analyses were conducted according to the mixed effect model, in which studies within subgroups are pooled with the random effects model, whereas tests for significant differences between subgroups are conducted with the fixed effects model. Because the actual heterogeneity we found was low in most analyses, we also conducted the subgroup analyses using the fixed effects model to examine both within-group and between-group differences.
Publication bias was tested by inspecting the funnel plot and by Duval & Tweedie's trim and fill procedure, Reference Duval and Tweedie32 which yields an estimate of the effect size after the publication bias has been taken into account (as implemented in Comprehensive Meta-analysis for Windows version 2.2.021). We also conducted Egger's test of the intercept to quantify the bias captured by the funnel plot and tested whether it was significant.
We expected that the mortality rate in subthreshold depression would be lower than in major depression, but that the prevalence of subthreshold depression would be higher. This would make it possible that the overall impact of subthreshold depression on mortality rates is comparable to or higher than the impact of major depression. In order to examine this we calculated the population attributable fraction (PAF) of major depression and subthreshold depression. The PAF indicates the potential reduction in mortality if the adverse effect of depression were to be completely blocked. Reference Smit, Ederveen, Cuijpers, Deeg and Beekman33,Reference Rothman and Greenland34 We based the overall PAF of subthreshold depression and major depression on the pooled prevalence rates and the pooled mortality rates. Although the PAF assumes that the excess mortality is fully caused by depression, which is not the case (see Discussion), it does give an indication of the relevance of subthreshold and major depression from a public health perspective.
Results
Having examined 6694 abstracts (5919 after removal of duplicates), we retrieved 975 full-text papers for further consideration. We excluded 953 of the retrieved papers (Fig. 1). Twenty-two studies examined both major and subthreshold depression and were included in this meta-analysis. Reference Penninx, Geerlings, Deeg, Van Eijk, Van Tilburg and Beekman35–Reference Winkley, Stahl, Chalder, Edmonds and Ismail56
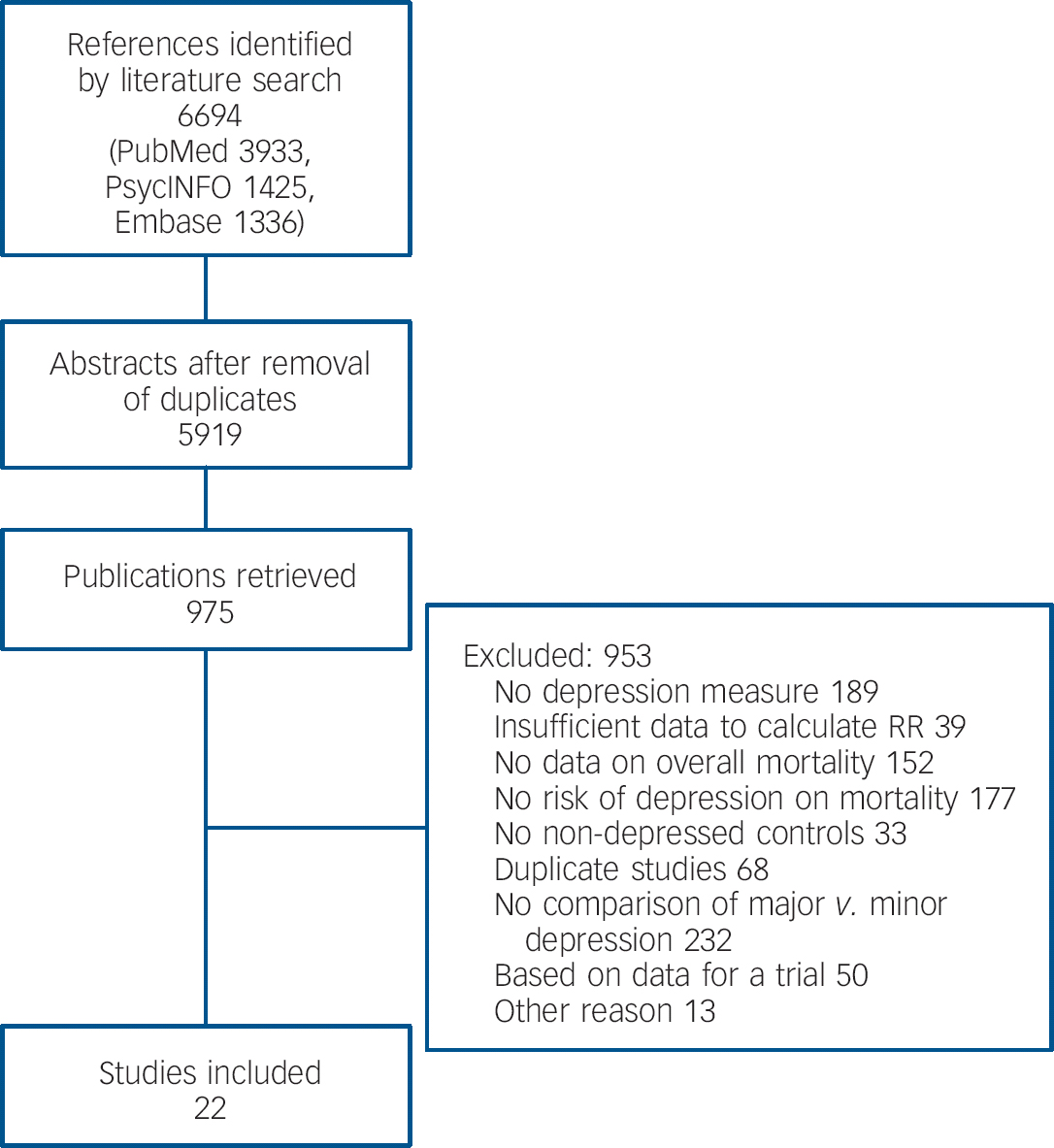
Fig. 1 Flowchart of inclusion of studies: RR, relative risk.
Characteristics of included studies
Selected characteristics of the 22 included studies are presented in online Table DS2. These studies included 18 705 participants (1147 had a diagnosed depressive disorder, 3238 had subthreshold depression and 14 320 had no depression), of whom 2881 died during follow-up. Seven studies were conducted among community samples, six among heart disease patients and nine in other patient groups (two on stroke patients, two on cancer patients, two on medical in-patients with diverse diagnoses, one on dementia patients, one on nursing home residents and one on patients with their first diabetic foot ulcer). Seven studies included less than 40% women, six 40–60% women and seven more than 60% women. Thirteen studies used a cut-off score on a self-report questionnaire to define subthreshold depression, whereas the other nine studies used diagnostic criteria for minor depression (such as Research Diagnostic Criteria or the criteria given in DSM-IV). Nine studies had a follow-up period of less than 2 years, eight studies had a follow-up period of 2–5 years and in four studies the follow-up was more than 5 years. Nine studies were conducted in the USA, seven in Europe and six in other countries. Nine studies scored positive on at least four of the five quality criteria, whereas the remaining 13 studies scored lower (online Table DS1).
Mortality in major v. subthreshold depression
We examined the relative risk of dying in patients with major depression compared with those with subthreshold depression (Table 1, Fig. 2). The risk was 1.13 (95% CI 0.98–1.30, random effects model), indicating a somewhat increased risk of dying for major depression compared with subthreshold depression. This RR was not significant, although there was a trend (P = 0.10 in the random effects model and P = 0.06 in the fixed effects model) indicating an increased mortality risk in major depression. Heterogeneity was low and not significant (P>0.1). The RR after adjustment for publication bias was exactly the same as the unadjusted RR (one trimmed study), and Egger's test of the intercept was not significant (P>0.1). We found no significant difference between any of the subgroups with the random effects model or with the fixed effects model (Table 1). Because the differences between the models were small, we report only the results according to the random effects model, which is the optimal model.
Table 1 Meta-analyses of studies examining mortality in participants with major depression, subthreshold depression or no depression: relative risksFootnote a
| n | RR | 95% CI | I 2 Footnote b | 95% CI | |
|---|---|---|---|---|---|
| Major v. subthreshold depression | 22 | 1.13 | 0.98–1.30 | 13.32 | 0–48 |
| Subgroup analyses Footnote c | |||||
| Population | |||||
| Community | 7 | 1.04 | 0.85–1.27 | 0 | 0–71 |
| Heart disease | 6 | 1.05 | 0.66–1.67 | 24.19 | 0–68 |
| Other patient group | 9 | 1.24 | 0.95–1.64 | 41.23 | 0–73 |
| Subthreshold depression | |||||
| Self-reported | 13 | 1.15 | 0.97–1.36 | 8.12 | 0–46 |
| Diagnostic criteria | 9 | 1.07 | 0.78–1.45 | 27.72 | 0–66 |
| Country | |||||
| USA | 9 | 1.12 | 0.82–1.54 | 41.62 | 0–73 |
| Europe | 7 | 1.01 | 0.79–1.30 | 0 | 0–71 |
| Other | 6 | 1.18 | 0.98–1.43 | 0 | 0–75 |
| Follow-upFootnote d | |||||
| <2 years | 9 | 1.08 | 0.68–1.72 | 47.79 | 0–76 |
| 2–5 years | 8 | 1.11 | 0.94–1.31 | 0 | 0–68 |
| >5 years | 4 | 1.06 | 0.84–1.35 | 0 | 0–85 |
| Quality score | |||||
| 4 or higher | 9 | 1.19 | 0.95–1.48 | 36.25 | 0–71 |
| Lower than 4 | 13 | 1.06 | 0.88–1.29 | 0 | 0–57 |
| Proportion of womenFootnote e | |||||
| <40% | 7 | 1.16 | 0.70–1.91 | 23.93 | 0–66 |
| 40–60% | 6 | 1.01 | 0.81–1.28 | 0 | 0–75 |
| >60% | 7 | 1.19 | 0.96–1.48 | 24.96 | 0–67 |
| Other comparisons | |||||
| Major depression v. non-depressed | 22 | 1.58 | 1.31–1.89Footnote *** | 52.87Footnote ** | 52–80 |
| Subthreshold depression v. non-depressed | 22 | 1.33 | 1.11–1.61Footnote ** | 69.13Footnote *** | 23–71 |
a. All reported results are based on the random effects model.
b. The P values in this column indicate whether the Q statistic is significant.
c. None of the differences between the effect sizes in the subgroups was significant.
d. The study of von Ammon Cavanaugh et al Reference Von Ammon Cavanaugh, Furlanetto, Creech and Powell55 did not report the exact follow-up period and was excluded from these analyses.
e. Two studies in which the percentage of female participants was not reported were excluded (Jorm et al, 1991; Reference Jorm, Henderson and Kay42 von Ammon Cavanaugh et al, 2001 Reference Von Ammon Cavanaugh, Furlanetto, Creech and Powell55 ).
** P<0.01
*** P<0.001.
Comparisons with participants without depression
We compared the mortality rates in major and subthreshold depression respectively with the rate in participants without depression. As indicated, we did this only to verify that the two forms of depression were associated with a higher mortality rate compared with participants without depression in our sample of studies, as suggested in earlier meta-analyses. We found that the relative risk of dying in major depression compared with participants without depression was 1.58 (95% CI 1.31–1.89, P<0.001) in the random effects model, with moderate to high heterogeneity (I 2 = 56%, P<0.01). The RR of dying in subthreshold depression compared with participants without depression was smaller than in major depressive disorders (RR = 1.33, 95% CI 1.11–1.61, random effects model) with high heterogeneity (I 2 = 69%, P<0.001). The results of the fixed effects models were comparable (not presented in Table 1).

Fig. 2 Studies directly comparing mortality rates in major and subthreshold depression: relative risks.
Population attributable fraction
The pooled prevalence rate of subthreshold depression was 0.17 (95% CI 0.10–0.28, random effects model) which was somewhat higher than the pooled prevalence rate of major depressive disorder (0.10, 95% CI 0.06–0.16); the case–control study by Sharma et al was excluded from the latter prevalence estimate. Reference Sharma, Copeland, Dewey, Lowe and Davidson52 To examine the overall impact of major depression and subthreshold depression on mortality in the population, we calculated the population attributable fraction of major depression and subthreshold depression. We found that the PAF of major and subthreshold depression together was 0.137, indicating that the overall mortality would be reduced by 14% if the adverse effects of depression could be blocked completely. The PAF of subthreshold depression was 0.065 and that of major depression was 0.072, indicating that the impact on mortality of the two types of depression are comparable.
Discussion
Direct comparisons between the mortality rates in major depression and subthreshold depression showed that there was a trend (P<0.1) indicating that the mortality rate in people with major depression may be somewhat higher than in people with subthreshold depression (RR = 1.13). We also found that both major depression (RR = 1.58) and subthreshold depression (RR = 1.33) were associated with a significantly increased risk of mortality compared with non-depressed samples (P<0.001). This is in agreement with the findings of most earlier meta-analyses. Together, these findings suggest that both major and subthreshold depression are associated with increased mortality rates, but that there is not much difference between the rates in the two types of depression. This is further strengthened by the findings on the PAF. We found that the PAFs of both major and subthreshold depression are about 0.07. This indicates that mortality would decline by 7% if we could block the adverse effects of major depression, and by another 7% if we could block the adverse effects of subthreshold depression. Although the risk of dying is somewhat higher in major depression the prevalence of major depression is lower, resulting in comparable PAFs. This is in agreement with other research showing that the impact of subthreshold depression on quality of life, service use and economic costs is lower than in major depression on an individual level, Reference Cuijpers and Smit16,Reference Cuijpers, Smit, Oostenbrink, de Graaf, ten Have and Beekman20 but that it is comparable with major depression on the population level because of the higher prevalence.
The relative risks we found for major and subthreshold depression compared with non-depressed controls were somewhat lower than in most other meta-analyses. Reference Cuijpers and Smit4,Reference Barth, Schumacher and Herrman-Lingen7,Reference Satin, Linden and Phillips25 Although higher RR was not confirmed in all meta-analyses, Reference Van den Akker, Schuurman, Ensinck and Buntinx27 this could indicate that our sample of studies was not representative of all studies examining the association between depression and mortality. However, because there is no clear consensus between the different meta-analyses it is not possible to verify this, and further research is needed to confirm it.
Limitations
This study has several limitations. First, although the number of studies was relatively large, the number of participants with major or subthreshold depression was not. Because we were interested in the differential mortality rates in these two conditions, we may not have had sufficient statistical power to detect smaller differences between the two groups. On the other hand, the 95% confidence interval of the RR ranged from 0.98 to 1.30, which indicates that it is unlikely that the ultimate risk is larger than 1.30. This would still only be an association of limited strength. A second limitation is that the quality of the studies was not optimal in all cases. This may have influenced our results, although we did not find significant differences between higher- and lower-quality studies. Third, we were only capable of examining unadjusted associations between major v. subthreshold depression and mortality. There is much evidence showing that a large part of the association between depression and excess mortality can be explained by lifestyle, behavioural and illness-related factors, although it is unclear whether this is also relevant for the comparison between major and subthreshold depression. Nonetheless, it is possible that had we adjusted for these factors the association between major v. subthreshold depression and mortality might have changed, although the direction of such a change cannot be predicted. More research is certainly warranted to explore this issue further. Fourth, in the included studies depression was measured only once (at baseline). It is highly possible that participants with subthreshold depression met criteria for major depression at some time in their past or during the follow-up period, that participants without depression had had a depressive disorder at some point in their life, and that participants with major depression did not meet diagnostic criteria 1 month earlier. This might well have distorted our outcomes. Because of these limitations the results of our studies have to be considered with caution.
Implications
It is not yet clear what the exact causes are of the increased mortality rates in people with depressive disorders. There is evidence that part of the excess mortality can be explained by an increased risk of suicide in people with depression, Reference Botswick and Pankratz57 by hazardous health behaviours such as physical inactivity, Reference Whooley, de Jonge, Vittinghoff, Otte, Moos and Carney58 increased smoking rates, Reference Dierker, Avenevoli, Stolar and Merikangas59 more alcohol consumption and unhealthy eating patterns, Reference Penninx, Geerlings, Deeg, Van Eijk, Van Tilburg and Beekman35,Reference Holahan, Moos, Holahan, Cronkite and Randall60,Reference Luppino, de Wit, Bouvy, Stijnen, Cuijpers and Penninx61 and by biological dysregulation, including hyperactivity of the hypothalamic–pituitary–adrenal axis, neuroimmune dysregulation and sympathoadrenergic dysregulation. Reference Cesari, Penninx, Newman and Kritchevsky62–Reference Cuijpers and Schoevers64 However, it remains unclear for most of these explanatory mechanisms what the causal direction is. It is possible that depressive disorders lead to hazardous health behaviours and biological dysregulation, but it is also possible that these factors have a role in the development of depressive disorders, or that both are explained by a third, underlying factor.
This study has made it clear that the association between depression and excess mortality is not limited to major depression. Apparently, the mechanisms through which depression is associated with mortality are also working in less severe forms of depression. It makes sense that unhealthy lifestyles as well as biological pathways are responsible for the excess mortality in major as well as subthreshold depression. These findings suggest that depression should not be seen as a distinct category with unique characteristics, but rather as a continuum ranging from no depression on the one hand to severe depression on the other, with subthreshold depression in between. Reference Solomon, Haaga and Arnow65,Reference Cuijpers, De Graaf and Van Dorsselaer66 Another implication of our findings is that the effects of subthreshold depression might be less severe than those of major depression in individual cases, but because of its high prevalence the impact on public health is comparable with that of major depression. This could be seen as an indication that subthreshold depression is a clinically relevant condition that does require treatment. Although there is no evidence that antidepressants and benzodiazepines are effective for this condition, Reference Barbui, Cipriani, Patel, Ayuso-Mateos and van Ommeren67 brief psychological treatments have been shown to be effective. Reference Cuijpers, van Straten and Smit68
Future research
We found little evidence that excess mortality is much higher in major depression than in subthreshold disorder, and in terms of population impact the two are comparable. More research on the exact mechanisms through which depression is associated with excess mortality might help in further understanding and possibly reducing this excess mortality.
Acknowledgements
We thank the following researchers for their kind collaboration and for providing additional data on their studies: Dr Nancy Frasure-Smith, Dr Joan Ryan, Dr Kirsty Winkley, Dr Reijo Tilvis, Dr Jane McCusker, Dr Kapil Parakh and Dr Naoki Nakaya.





eLetters
No eLetters have been published for this article.