


BACKGROUND
The related eating disorders anorexia and bulimia nervosa are characterised by a range of abnormal attitudes and behaviours. Chief among these attitudes are concerns about weight and shape, with the typical dieting and purging behaviours appearing to follow these concerns. Are weight and shape concerns necessary for the development of eating disorders, and is there a clear developmental pathway from concern through behaviour to disorder? If concern is the first step on the pathway to an eating disorder, where does this anxiety stem from? This review explores aspects of the development of weight and shape concerns and the evidence for their origins. The relationship between weight and shape concern, pathological eating behaviour and disorder is examined, as an established developmental pathway may point to prevention strategies.
Are weight and shape concerns universal features of eating disorders?
The ICD-10 psychiatric classification system (World Health Organization, 1992) stresses the importance of weight and shape concerns in the diagnosis of both anorexia and bulimia nervosa. In anorexia nervosa, the disorder is described as being “associated with a specific psychopathology whereby a dread of fatness and flabbiness of body contour persists as an intrusive overvalued idea”. Many would see this weight and shape concern as the driving force of the condition, with food restriction, weight loss and the characteristic endocrine changes arising out of this concern. Bulimia nervosa, with its cycle of binge eating and purging, is also said to be characterised by “excessive pre-occupation with control of body shape and weight”. The DSM—IV criteria (American Psychiatric Association, 1994) are in broad agreement on the importance of weight and shape concerns in anorexia nervosa, and for a diagnosis of bulimia nervosa require that “self-evaluation is unduly influenced by body shape and weight”.
In contrast, the feeding disorders of childhood (ICD code 98.2) comprise an assortment of non-organic feeding and eating disorders occurring before the age of 6 years in which weight and shape concerns are not a feature (World Health Organization, 1992). This also appears to be the case for eating disorders that have been described in adolescents, such as food avoidance emotional disorder (Reference Higgs, Goodyer and BirchHiggs et al, 1989) and pervasive refusal (Reference Lask, Britten and KrollLask et al, 1991), in which food restriction is only a part of the picture. This review is therefore confined to the more familiar disorders of anorexia and bulimia nervosa.
Developmental aspects of weight and shape concern
Adolescence is viewed as the stage of greatest risk for the development of eating disorders because of the convergence of physical and psychological challenges at this time. Normal population studies such as that by Marchi & Cohen (Reference Marchi and Cohen1990) suggest that weight and shape worry is rare in young children. This longitudinal study followed up 800 children at three time points and suggested such concerns develop through childhood, becoming common by later adolescence, particularly in girls. More recently, however, reports have appeared of children as young as 5 years expressing fears of becoming fat and having concerns about their body image (Reference Feldman, Feldman and GoodmanFeldman et al, 1998). Shapiro et al (Reference Shapiro, Newcomb and Loeb1997) meanwhile showed that dieting and exercise were used to control weight in as many as 29% of boys and 41% of girls aged 8-10 years. Concerns about fatness then appear to be growing among children of primary school age and have been shown to be associated with low body self-esteem, and to be more common in overweight children and in girls (Reference Hill, Draper and StackHill et al, 1994). Despite these newer findings, the evidence for an increase in these concerns with age is compelling. Cooper & Goodyer (Reference Cooper and Goodyer1997) showed how more strictly defined eating and weight concerns increase in early adolescence and report prevalences in a community sample of 14.5% at age 11-12 years, 14.9% at 13-14 years and 18.9% in girls aged 15-16 years.
ORIGINS OF WEIGHT AND SHAPE CONCERN
There is no doubt that females at all ages show greater weight concern than males. During adolescence boys are commonly dissatisfied with their height and lack of musculature, while girls tend to be unhappy with their weight (Reference Coleman and HendryColeman & Hendry, 1999). What are the influences underlying these concerns?
Biological factors
Genetics
There is some uncertainty about the role of genetic factors in the aetiology of eating disorders in general (Reference KayeKaye, 1999) and of weight and shape concerns in particular. The greater prevalence of bulimia nervosa has resulted in this condition receiving more attention than anorexia nervosa. Kendler and colleagues' twin studies estimated the heritability of bulimia to be around 50% (Reference Kendler, MacLean and NealeKendler et al, 1991), and Kaye (Reference Kaye1999) gives a similar figure for anorexia nervosa. Strober (Reference Strober, Brownell and Fairburn1995) explored the nature of the probable inherited element in these disorders, suggesting that it might largely be based on a personality type that is prone to anxious worry (including worries about weight), unyielding insistence on order and seeking self-validation from external rewards, rather than inheritance of the disorder per se. Wade et al (Reference Wade, Martin and Tiggemann1998) using genetic modelling suggested that shared (and to a lesser extent non-shared) environmental factors are more important than genetic factors in influencing women's attitudes to weight and shape.
Puberty
Adolescence is a complex stage of development in which a number of physical changes and psychosocial challenges converge. The demands of meeting the ‘tasks’ of adolescence will be hard for many and may have a significant impact on confidence and self-esteem. Those who struggle to meet the challenges may feel a sense of being out of control. As dietary restraint and control of eating is valued in our society, weight consciousness may be a non-specific response to the overwhelming demands of puberty. In adolescent girls, the increase in body fat that occurs with puberty results in a change of physical appearance, bodily feelings and reproductive status that requires reorganisation and transformation of the body image (Reference Attie, Brooks-Gunn, Petersen, Lewis and MillerAttie et al, 1990). However, the physical changes of puberty involve significant anabolic growth, so that the notion that this has a direct bearing on weight sensitivity seems logical. In addition, it may go some way to explaining the gender difference in both dieting behaviour and risk of eating disorders in adolescence. Whereas in boys most of the weight gain is explained by an increase in muscle tissue, in girls the physical changes of puberty involve significant deposition of bodily fat on abdomen, buttocks and thighs (Reference TannerTanner, 1989). These are precisely the areas that most ‘normal’ dieters and sufferers with eating disorders are concerned about. The rate of growth during puberty is striking. Boys' mean weight rises from 40.5 kg at their thirteenth birthday to 56 kg at age 15 years, a growth of 38% in 2 years. Girls, meanwhile, grow on average from 34 kg at their eleventh birthday to 47.5 kg by age 13 years, a rise of 40% during their (earlier) 2 years of maximum growth (Reference Tanner and WhitehouseTanner & Whitehouse, 1975). The mean proportion of body fat in females also changes from 8% in middle childhood to 22% after puberty (Reference TannerTanner, 1989). Crisp (Reference Crisp1980) has drawn attention to the timing of puberty as a possible risk factor for the development of eating disorders, probably mediated through weight consciousness. As well as the psychosocial challenges early puberty poses for vulnerable young people, there is an association between fatness in childhood and early puberty. Thus it might be that these young people have a double risk for weight sensitivity. This idea is lent support by the finding of Brooks-Gunn & Warren (Reference Brooks-Gunn and Warren1985), who noted that late-maturing girls were more satisfied with their body and had lower rates of eating disorder than their peers. Koff & Rierdan (Reference Koff and Rierdan1993) in an attempt to disentangle the physical (changes in fatness) from the psychological impact of early puberty concluded that it is the psychological impact that is most powerful in promoting eating disturbance.
De Castro & Goldstein (Reference De Castro and Goldstein1995) compared the eating behaviour and attitudes of pre-pubertal and post-pubertal girls, finding that the latter had significantly more negative body image and body dissatisfaction, but demonstrating the difficulty in disentangling attitude from behaviour.
Obesity
Premorbid obesity has been reported to be more common in those who later develop eating disorders, the rates in anorexia nervosa (7-20%) being lower than in bulimia nervosa (18-40%) (Reference Cooper, Brownell and FairburnCooper, 1995). Being overweight commonly leads to dieting, but the explanation for the link with eating disorders is probably more complex. Children have been found to have negative attitudes to obese people (Reference Harris and SmithHarris & Smith, 1982) and do not like to play with fat children (Reference Strauss, Smith and FrameStrauss et al, 1985). The effects of obesity on self-esteem and body dissatisfaction are therefore likely to be as relevant to the development of eating disorders as their role in promoting dieting behaviour.
Family factors
Family attitudes and beliefs
Hill & Franklin (Reference Hill and Franklin1998) among others have suggested that parents' overconcern with weight and dieting behaviour may be passed on to and adopted by their daughters. They conclude that mothers may have an important role in the transmission of cultural values regarding weight, shape and appearance. These authors cite the work of Pike & Rodin (Reference Pike and Rodin1991), who reported higher levels of disordered eating in the mothers of symptomatic 16-year-olds and suggested an “agreed family agenda of weight concern, drive for thinness and dieting”. Hill & Franklin (Reference Hill and Franklin1998) argue that research into parental promotion of weight concern rarely looks beyond maternal attitudes and behaviour. They suggest that this is primarily because of the presumed central role of mothers in acting out the nature and importance of thinness and to the gender-stereotyped nature of dieting itself. An earlier study from this team (Reference Hill and PallinHill & Pallin, 1995) had confirmed that maternal dieting was much more influential than paternal behaviour.
Clinically, however, comments from male family members are often cited as a precipitant for dieting (Reference Hill and PallinHill & Pallin, 1995), and Hill & Franklin (Reference Hill and Franklin1998) noted that subjects with high weight restraint were twice as likely as their non-restrictive controls to have male siblings. Thus the contribution of male family members to the development of weight and shape concerns should not be overlooked. Smolak et al (Reference Smolak, Levine and Schermer1999) have looked at the relative contribution of mothers' and fathers' direct comments about their child's weight and modelling of weight concerns through their own behaviour, on children's weight concerns and dieting. They found that direct comments — particularly by mothers — were more influential than modelling of behaviour. As in most studies, girls were more affected than boys. Daughters' concerns about fatness were related both to mothers' concerns with their own weight as well as concern about their daughter's weight. Daughters' concerns were also positively correlated with fathers' concerns about their own thinness.
Striegel-Moore & Kearney-Cooke (Reference Striegel-Moore and Kearney-Cooke1994) have suggested that although parents are generally satisfied with their children's appearance, their negative comments increase with the child's age. Mothers may also be more concerned about the weight of their daughters than of their sons, particularly where the mother suffers with an eating disorder herself (Reference Agras, Hammer and McNicholasAgras et al, 1999).
Mothers of daughters with eating disorders have sometimes been found to have unusually high rates of disordered eating attitudes themselves. Pike & Rodin (Reference Pike and Rodin1991), for example, found the mothers had high scores using the Eating Disorder Inventory (Reference Garner and OlmstedGarner & Olmsted, 1983) and also felt their daughters should lose weight more often than did control mothers. Stein et al (Reference Stein, Stein and Walters1995) found that the mothers of younger children being treated for feeding disorders scored highly on nearly every sub-scale of the Eating Disorder Examination. They argue that these findings are consistent with the idea that maternal attitudes play a part in the process of the child acquiring psychopathology.
Parental and sibling eating disorders
Parental (and to a lesser extent, sibling) attitudes to their own body shape may affect children in two ways (Reference Stein, Brownell and FairburnStein, 1995). First, children model themselves on their same-sex parent and elder siblings. Second, parents with eating disorders may influence their children through their attitudes to the children's weight, shape and eating habits and the importance they attach to these.
Stein et al (Reference Stein, Wooley and Cooper1994) identified mothers with eating disorders as more intrusive than controls in their feeding of 12-month-old infants. Infant weight was found to be inversely related to the extent of mothers' concern with their own body shape. In a subsequent study, however, this group found little evidence that mothers with eating disorders preferred smaller children, were dissatisfied with their children's shape or misperceived their children's size (Reference Stein, Murray and CooperStein et al, 1996).
In a controlled, prospective study of 41 mothers with eating disorders and 153 without a history of eating disorder, Agras et al (Reference Agras, Hammer and McNicholas1999) demonstrated that food tended to be used for reward or behavioural control more by the former. Also, the mothers with eating disorders were more concerned about their daughter's weight from the age of 2 years onwards. At 5 years of age, the children of mothers with eating disorders had greater negative affect than controls.
Mothers with bulimia have also been demonstrated to have difficulties with feeding their children (e.g. Reference Fahy and TreasureFahy & Treasure, 1989), and they have also been shown to have excessive concerns about their daughters' weight and shape (Reference Stein and FairburnStein & Fairburn, 1989).
Finally, parental obesity has on occasion been suggested to provide the motivation for a teenager's dieting (Reference Crisp, Harding and McGuinnessCrisp et al, 1974). Rather than the parent modelling dieting behaviour, in some situations the daughter has been seen as providing a model of successful weight restraint for the parent (Reference Weaver and GowersWeaver & Gowers, 1994).
Attachment status
Although there has been only limited work in this area, Sharpe et al (Reference Sharpe, Killen and Bryson1998) in a study of pre-adolescent and adolescent girls aged 9-12 years suggested that those considered insecurely attached (using a single self-report item) had greater weight concerns that those who were securely attached. They suggest that this finding may be explained by low self-esteem or the perceived need to conform to standards set by society in order to gain acceptance.
Feeding practices
Bottle-feeding has been reported to be more common in those subsequently developing eating disorders than in matched controls with neurotic or affective disorders (Reference CrispCrisp, 1969). Mothers who diet or have weight concerns themselves are more likely to bottle-feed (Reference Andrews and BrownAndrews & Brown, 1999). This is likely to be a more important influence than the direct effect of bottle-feeding on infant growth. Although most studies have shown that children of mothers with eating disorders tend to be thinner than controls (Reference Stein, Murray and CooperStein et al, 1996), one group of mothers overfed their children through a belief that infant weight was an important index of health and successful parenting. It is concluded that parents who use food to satisfy their children's emotional needs or to promote good behaviour may interfere with the children's ability to regulate their own body weight and render them vulnerable to obesity or other eating disorders. McCann et al (Reference McCann, Stein and Fairburn1994), in a study of 26 mothers of children with non-organic failure to thrive, found higher rates of dietary restraint compared with controls. Despite their child's low weight, 50% restricted the child's intake of sweet foods and 30% restricted their intake of fattening foods. Although maternal attitudes were thought to have an aetiological role in the non-organic failure to thrive, the risk of these children developing subsequent eating disorders in adolescence is unclear. Whether any effect arises through concern or abnormal eating behaviour is similarly uncertain.
Family functioning
Although family theories on the aetiology of eating disorders abound, the direct influence of family functioning on weight and shape concerns is unclear. Inasmuch as weight concerns probably relate to fears of loss of control, rigid or overprotective styles of parenting (Minuchin et al, Reference Minuchin, Baker and Rosman1975, Reference Minuchin, Rosman and Baker1978) might be expected to undermine children's developing confidence in their own self-control, including over their weight. Vandereycken (Reference Vandereycken, Brownell and Fairburn1995) sees the characteristic family difficulty as being a lack of joint parental authority, expressed as a difficulty striking the right balance between control over the child and the amount of age-appropriate autonomy. Shoebridge & Gowers (Reference Shoebridge and Gowers2000) in a controlled study found that an overprotective or ‘high concern’ style of parenting is common in children who subsequently develop anorexia nervosa, and that this can in a number of cases be explained by an earlier obstetric tragedy. Attie & Brooks-Gunn (Reference Attie and Brooks-Gunn1989) are among those reporting maternal dissatisfaction with family functioning. These authros found that both mothers and symptomatic girls desired greater family cohesion, a finding endorsed by Pike & Rodin (Reference Pike and Rodin1991).
Adverse experience
Severe adverse life events may exert an effect on weight and shape consciousness through an adverse effect on self-esteem. They are not especially common as immediate precipitants of anorexia nervosa compared with other adolescent psychiatric disorders, however, and where negative events have occurred they confer a relatively good prognosis (Reference North, Gowers and ByramNorth et al, 1997).
Sexual abuse
The relationship between eating disorders and past experience of sexual abuse remains a controversial one. Anorexia nervosa commonly arises in adolescence and as weight loss has a direct effect on sex hormone production and loss of postpubertal feminine shape, the increasing awareness of child sexual abuse in the 1980s led many to believe that a specific link with eating disorders would be found. While many researchers (e.g. Reference Welch and FairburnWelch & Fairburn, 1996; Reference Kenardy and BallKenardy & Ball, 1998) have found higher than expected rates of past physical and sexual abuse in those with eating disorders, the rates are probably no higher than in those with other psychiatric disorders (Reference Palmer and OppenheimerPalmer & Oppenheimer, 1992). Nevertheless, the hypothesis that sexual abuse is likely to result in disgust with femininity and sexuality, which then becomes expressed in concern around the subject's own body shape, remains highly plausible.
Bullying
Although there has been little specific research into bullying, anecdotal accounts frequently attest to the perceived importance of negative comments about weight by peers in promoting weight and shape concern. These are often single experiences, however, and as Hill & Pallin (Reference Hill and Pallin1995) point out, these comments are often made by boys.
Dieting
Although weight concern is generally thought to lead to dieting, the reverse is also possible. Clinically, sufferers with anorexia nervosa who are lowest in weight tend to have the greatest weight phobia, while in treatment, contrary to the patient's expectation, fears of fatness frequently reduce with weight gain (Reference CrispCrisp, 1980).
Sociocultural factors
Although eating disorders have been described in the medical literature since the 17th century, they are widely considered to epitomise disorders arising from difficulty in meeting the ever-increasing challenges of adolescence. Crisp (Reference Crisp1980), for example, has drawn attention to adolescence as a stage of development that barely existed as a social phenomenon 150 years ago. The evidence that eating disorders have increased in prevalence over the past 30 years, their predominance in females, and the changing roles of women in Western society has convinced many of the role of sociocultural factors in the aetiology of these disorders. Raphael & Lacey (Reference Raphael and Lacey1992), for example, have argued that it is the difficulty in balancing conflicting roles that is particularly potent. Others have pointed to the changes in the ‘ideal’ female shape over this time, which has become markedly thinner. Szabo (Reference Szabo1996) calculated the body mass index (BMI) of Playboy centrefold models and concluded that 72% had a BMI lower than 18 kg/m2.
Social class
Ogden & Thomas (Reference Ogden and Thomas1999) reported a consistent relationship between social class and weight concern, with higher-class female subjects placing greater importance on physical appearance and especially thinness. These subjects also reported greater body dissatisfaction and bodily distortion than lower-class subjects.
Ethnicity
The certainties about culture-bound attitudes to weight and shape have recently been challenged. Black males and females have been said to value female thinness less than their White counterparts in childhood and adolescence (Reference Powell and KahnPowell & Kahn, 1995). Thompson et al (Reference Thompson, Corwin and Sargent1997) recruited White and Black fourth-grade children into a survey of body image and weight concerns. The Black children tended to select a significantly larger body size ideal for male and female, child and adult sizes. Whites and females experienced more body dissatisfaction and weight concern than males and Blacks. Killen et al (Reference Killen, Taylor and Haward1994) meanwhile found that adolescent Black females were more concerned about becoming over-weight, and Thompson et al (Reference Thompson, Corwin and Sargent1997) showed that in their series Black males selected an image with a higher BMI as an ‘ideal girlfriend size’. However, Striegel-Moore et al (Reference Striegel-Moore, Schreiber and Pike1995) found that while Black females in an American study were plumper than their White counterparts, this increase in adiposity was associated with greater drive for thinness. Williamson (Reference Williamson1998) has suggested that a tendency in American research to focus on White middle-class girls with the exclusion of African Americans has led to an erroneous belief that acceptance in Black communities of women with fuller shapes protects them from eating problems.
Wilfley et al (Reference Wilfley, Schreiber and Pike1996) meanwhile demonstrated that while Black and White females had similar levels of body dissatisfaction, with similar predictive factors, when actual weight was taken into consideration White women were much more dissatisfied, although at a lower weight. Nasser (Reference Nasser1994) has challenged the notion that it is Western women who are especially at risk of pressure to diet. She suggests that women in a range of cultures are vulnerable to societal pressures which contribute to unhealthy eating attitudes.
Media influences
Russell (Reference Russell, Cooper and Stein1992) suggested that the mass media and advertising promote the idea that slim women are more attractive, achieving and successful. The notion that the media somehow ‘cause’ weight and shape concerns seems oversimplistic given that the media primarily reflect beliefs and attitudes in the minds of consumers. Field et al (Reference Field, Cheung and Wolf1999) in an interesting study found that while the majority of pre-adolescent and adolescent girls were unhappy with their shape and weight, these negative attitudes were strongly related to frequency of reading fashion magazines. Baker et al (Reference Baker, Sivyer and Towell1998) meanwhile suggested that evidence that the visual media contribute to negative eating attitudes is provided by research with congenitally blind women, which found that they had less negative body dissatisfaction scores than those with acquired blindness or sighted women. Other researchers have tested the effect of brief exposure to slim or overweight body images on normal subjects, finding that slim images increase body dissatisfaction and overweight images ameliorate it (Reference Ogden and MundrayOgden & Mundray, 1996). The methodologies employed in these studies have, however, been criticised in terms of their brief nature and selection factors (Reference Champion and FurnhamChampion & Furnham, 1999).
Peers
A number of studies have indicated the importance of peer weight and eating concerns in the development of dieting behaviour or weight concerns. Taylor et al (Reference Taylor, Sharpe and Shisslak1998) in study of 523 primary and middle-school children found that peer influences accounted for approximately one-third of the variance in weight concern. Bullying and teasing about weight has been identified as a precipitant of eating concerns and body dissatisfaction in adolescent females (Reference Fabian and ThompsonFabian & Thompson, 1989), and a study of those with established anorexia nervosa (Reference Rabe-JablonskaRabe-Jablonska, 1997) pointed to the importance of changes in the peer group or a change in the subject's position within it.
HOW DO WEIGHT AND SHAPE CONCERNS LEAD TO THE LATER DEVELOPMENT OF EATING DISORDERS?
Weight and shape concerns are extremely prevalent and commonly lead to dieting, but only a minority of dieters go on to develop eating disorders. Patton et al (Reference Patton, Johnson-Sabine and Wood1990) have called into question whether there is a cause and effect sequence between dieting and the development of eating disorders. They argued that dieting is essentially a benign practice without natural progression to eating disorder, and suggested that the influences on dieting behaviour (including those underlying weight and shape concern) are the same in those with and without eating disorders. Killen et al (Reference Killen, Taylor and Haward1994) have attempted to address the relationship between concern and disorder in a longitudinal study. Their community sample of adolescent girls was followed up over a 3-year period, 3.6% showing an onset of eating disorder symptoms in this time, with a significant association with earlier weight concern. A further report from this group (Reference Taylor, Sharpe and ShisslakTaylor et al, 1998) suggested that of those who scored highest at baseline, 12% went on to develop full or partial eating disorders during the 3-year time frame compared with 2% of low scorers. A link between dieting and the subsequent development of a full-blown eating disorder is difficult to demonstrate, given the relative rarity of anorexia nervosa.
ARE WEIGHT AND SHAPE CONCERNS NECESSARY FOR THE DEVELOPMENT OF EATING DISORDERS?
Although weight and shape concerns are required for a diagnosis of anorexia nervosa and bulimia nervosa in both the ICD-10 and DSM-IV systems, these concerns may not be universal and may not necessarily antedate their development. Palmer (Reference Palmer1993) has argued that weight concern should not be seen as a necessary criterion for the eating disorders on three main grounds. First, historical accounts from the 19th century rarely mention weight concern, despite their attention to detail in other respects. Second, apparent cases of anorexia nervosa from non-Western cultures seem not to show concerns with fatness if these preoccupations are not prevalent within that culture. Finally, insistence on weight concern as a diagnostic criterion creates difficulty in the classification and management of ‘atypical’ cases without weight concern, but who are identical to ‘true’ cases in all other respects. Often these cases have merely been assumed to be denying their weight concern (e.g. Reference Lee, Chiu and ChenLee et al, 1989).
We have reviewed the evidence for the role of a range of physical and social factors on weight and shape concern and their relation to the development of eating disorders. There are, however, a number of other commonly proposed risk factors which do not so readily appear to affect weight concern. These include perfectionism, moral and religious belief, and the psychosexual impact of puberty. It is possible that these exert an aetiological effect through a different route, namely a belief in the value of restraint. Figure 1 proposes a model for the impact of these various influences, from which it can be seen that restraint is presumed to lead to dieting. Dieting may then result in the development of an eating dis-order through a vicious circle of growing weight and shape concern. However, this model also allows for an aetiological route without weight and shape concern. Bulimia nervosa appears to sometimes develop with binge eating as the starting point, with weight concern and then dieting behaviour ensuing. Eating disorders have long been considered to have a multi-factorial origin. It is probable, however, that most factors in the aetiology of eating disorders are mediated through weight and shape concern or need for restraint. It is suggested that it is these cognitions that lead to dieting behaviour and thence to anorexia nervosa and often to bulimia nervosa. As weight and shape concerns are very rare in pre-school children and almost universal in late adolescent females who are most at risk of eating disorders, further clarification of the resilience and vulnerability factors operating between primary aetiological factors and weight concern may point to potential intervention strategies.
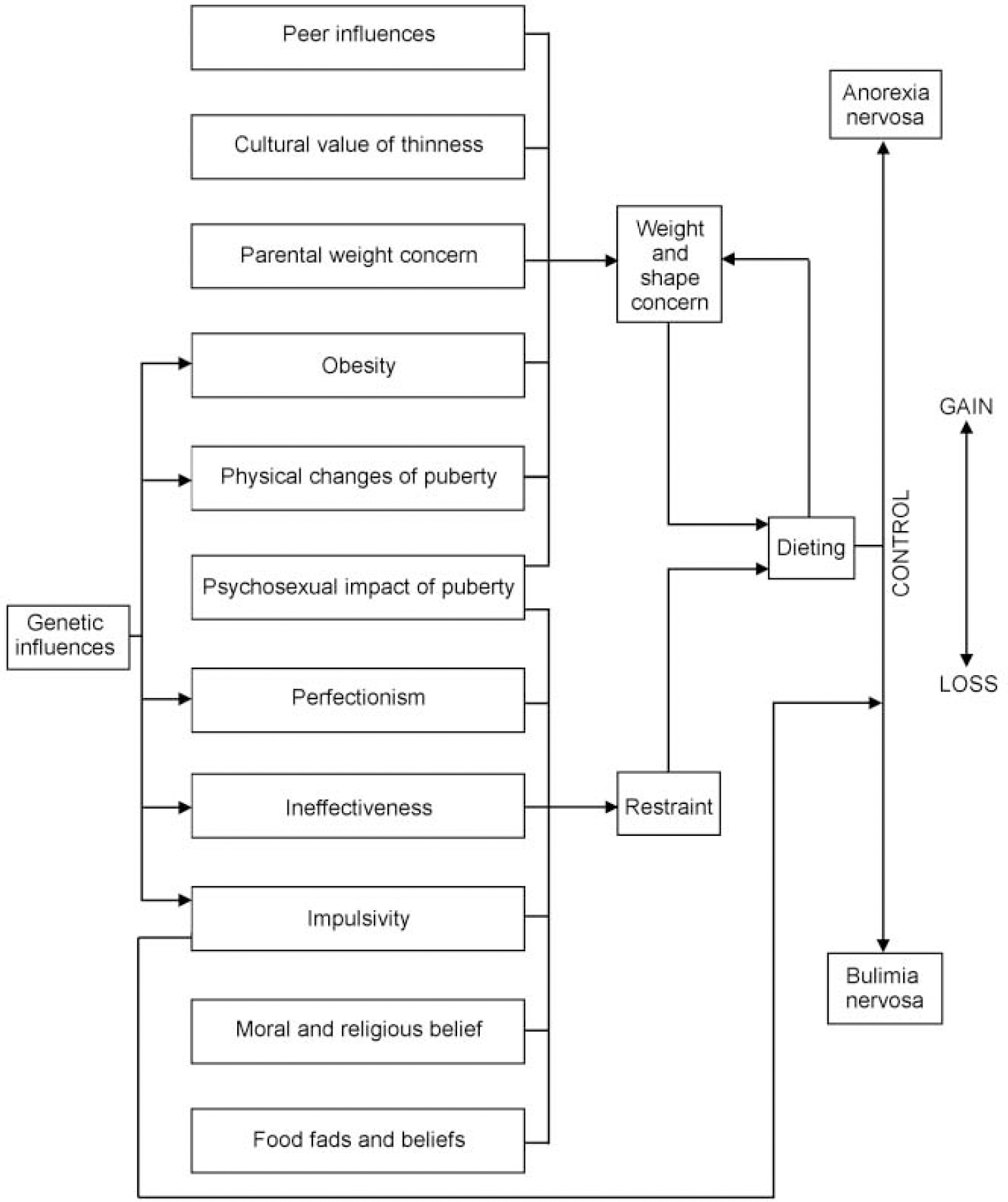
Fig. 1 The origins of weight and shape concern and its relationship to dieting behaviour in eating disorders.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
• Weight and shape concerns commonly develop in late childhood and through puberty.
-
• The origins of these concerns should be an integral part of assessment of those with eating disorders.
-
• Prevention might usefully focus on these concerns rather than on the subsequent dieting behaviour.
LIMITATIONS
-
• Inclusion criteria for this review were not fully systematic.
-
• It is difficult to discriminate between the aetiology of weight and shape concerns and eating disorders themselves.
-
• Weight and shape concerns are very common; uncertainties remain about which young people potentially at risk will go on to develop serious disorders.


eLetters
No eLetters have been published for this article.