



Introduction
Partisanship remains a dominant explanation for the differential outcomes from the COVID-19 pandemic (Druckman et al. Reference Druckman, Klar, Krupnikov, Levendusky and Ryan2021; Grossman et al. Reference Grossman, Kim, Rexer and Thirumurthy2020). Striking red and blue hued maps followed narratives about climbing death counts, vaccine distribution, and economic suffering. Within these accounts, however, major discrepancies remain that partisanship alone cannot explain. Why did Mississippi and West Virginia, two largely rural and conservative states, experience such different death rates (13.8% versus 4.6% excess deaths)? Why did New York and Massachusetts, both wealthier and liberal states hit early in the pandemic, have different excess death rates (13.1% versus 2.5%)? We propose that differences in state capacity – not simple partisanship – drive these unequal results.Footnote 1
State capacity is the ability of a state’s executive branch to implement legislative and executive policy decisions. Given that democratically elected political leaders must respond to the basic needs of constituents in order to stay in power, we assume that all state governments at least minimally tried to mitigate harm from COVID-19. Governments in states with superior capacity should therefore demonstrate greater harm mitigation in relation to the COVID-19 pandemic. Although a role for state capacity in pandemic response has been invoked in the comparative literature, it has not been evaluated in the American context, particularly at the state level. In this study, we employ a new measure of subnational state capacity as a latent trait to evaluate the effects.
We begin by describing existing knowledge on state capacity and pandemics, including historical studies and recent work on COVID-19 policies. This is followed by our theory of state capacity and pandemic response. Namely, higher state capacity would allow states to more effectively implement COVID-19 mitigation protocols, leading to reduced morbidity and mortality. Next, we introduce our latent measure of state capacity and demonstrate that it leads to lower excess deaths and increased vaccination rates during the high-demand phase of COVID-19 vaccination. Our results show that state capacity significantly influenced these outcomes in the expected directions, and the relationship is robust to several measures of partisanship, social capital, geography, and demographics. When accounting for state capacity, partisanship of the executive in office at the start of the crisis is not significantly associated with crisis outcomes.
We further demonstrate the role of state capacity in achieving better health outcomes by incorporating state-level anti-COVID policies. While all states created regulations intended to reduce disease transmissions (e.g., safer-at-home orders), they did not all have the same enforcement capacity to make the public comply with these policies, which would be necessary to secure improved outcomes. Health outcomes can only be improved if the policies are actually implemented. This requires state capacity. State governments that were capable of enforcing their will were more successful at turning these regulations into lives saved. We demonstrate that these anti-COVID policies only significantly reduced death rates in higher-capacity states. Thus, our work links the literature on US state politics to comparative literature on state capacity and to research on the politics of pandemics.
State capacity and pandemics
Since the start of the COVID-19 pandemic, social scientists have explored the socio-political causes and consequences of the disease across countries. This research has examined government responses to the pandemic and their effectiveness based on factors such as previous pandemic experience, wealth, regime type, globalization, political trust, culture, and state structures (Bickley et al. Reference Bickley, Chan, Skali, Stadelmann and Torgler2021; Capano et al. Reference Capano, Howlett, Jarvis, Ramesh and Goyal2020; Capano Reference Capano2020; Greer et al. Reference Greer, King, da Fonseca and Peralta-Santos2020; Hartley and Jarvis Reference Hartley and Jarvis2020; Knutsen and Kolvani Reference Knutsen and Kolvani2022; Petridou Reference Petridou2020; Shvetsova et al. Reference Shvetsova, Zhirnov, VanDusky-Allen, Adeel, Catalano, Catalano, Giannelli, Muftuoglu, Riggs and Sezgin2020; Wang Reference Wang2021). Researchers also considered US Senators’ propensity to credit-claim on COVID-related legislation (Bianco et al. Reference Bianco and Schmidt2020) and the influence of campaign money and lobbying on state policy decisions (Crosson et al. Reference Crosson and Parinandi2021; Furnas et al. Reference Furnas, Crosson and Lorenz2021).
COVID-19 is not the first pandemic to be tied to politics. High death tolls from the Black Death, for instance, increased laborers’ negotiating power and promoted more inclusive political institutions, liberal politics, and better public goods provisioning (Dittmar et al. Reference Dittmar and Meisenzahl2020; Gingerich & Vogler Reference Gingerich and Vogler2021). Infectious disease patterns also drove colonialism (Acemoglu et al. Reference Acemoglu, Johnson and Robinson2012), global population growth and development, and the formation of government health agencies (Gray et al. Reference Gray and Jenkins2021). Into the 20th century, infectious disease has impacted marriage patterns, job markets, and insurance coverage (Olivarius Reference Olivarius2022), as well as state aid (Napolio et al. Reference Napolio2020). States and cities have responded to plagues in several ways (Holman et al. Reference Holman, Farris and Sumner2020), which determined how well they stemmed the pandemics and their effects (Olivarius Reference Olivarius2022; Gingerich & Vogler Reference Gingerich and Vogler2021; Capano Reference Capano2020). Citizens, particularly those living in democracies, expect their governments to forestall deadly diseases. Not all governments, however, are capable of doing so.
Scholars agree that political institutions and governance quality affected the toll caused by the COVID-19 pandemic. However, the heterogeneity of country contexts, as well as the interactive effects of specific institutional designs and the efficacy of these institutions, make it difficult to generalize. For instance, Capano (Reference Capano2020) argues that political gamesmanship and health-system design determined the course of the disease across Italy, an early-hit, low-state-capacity country. Cross-national research has found both positive and negative effects of federalism on COVID-19 responses (Shvetsova et al. Reference Shvetsova, Zhirnov, VanDusky-Allen, Adeel, Catalano, Catalano, Giannelli, Muftuoglu, Riggs and Sezgin2020; Greer et al. Reference Greer, King, da Fonseca and Peralta-Santos2020; Toshkov et al. Reference Toshkov, Carroll and Yesilkagit2022). These effects depend in part on how slowly or inefficiently individual governors and legislators respond. Some argue that cities could also act before or until governors or legislators acted (McDonald III et al. Reference McDonald, Goodman and Hatch2020; Brandtner et al. Reference Brandtner, Bettencourt, Berman and Stier2021; Owens et al. Reference Owens and Johnson2020; Holman et al. Reference Holman, Farris and Sumner2020).
Because of the US federal system, state governments had substantial control over the early COVID-19 response policies, which resulted in substantial disparities between the states. Multiple sources of these disparities have been considered, from citizen attitudes, partisanship, media exposure, and public actions, to governmental inaction (Adolph et al. Reference Adolph, Amano, Bang-Jensen, Fullman and Wilkerson2021; Pedersen and Favero Reference Pedersen and Favero2020; Grossman et al. Reference Grossman, Kim, Rexer and Thirumurthy2020; Druckman et al. Reference Druckman, Klar, Krupnikov, Levendusky and Ryan2021). Immormino & Stowell (Reference Immormino and Stowell2022) argue that greater “relative political extraction” – the share of the GDP that the government collects in tax revenue – allowed Canada and Canada’s provinces to respond more effectively to COVID-19’s effects than the US and American states did in the first year.Footnote 2 We focus on the role that differences in state capacity played in the efficacy of their responses.Footnote 3
In June 2020, Greer et al. (Reference Greer, King, da Fonseca and Peralta-Santos2020) included state capacity in their list of factors that would eventually influence relative outcomes among different countries: “State capacity, including control over health care systems as well as public administration, matters to all elements of response and shapes what policymakers perceive as available options.” This interest in the role of state capacity does not mean, however, that researchers have established protocols to measure it; more is said about this in the data section. Furthermore, COVID-19 is so new that the role of state capacity in stemming the pandemic’s effects has not yet been established empirically. Cross-national studies have examined the role of good governance using the World Bank’s government effectiveness index. Liang et al. (Reference Liang, Tseng, Ho and Wu2020), Nabin et al. (Reference Nabin, Chowdhury and Bhattacharya2021), and Serikbayeva et al. (Reference Serikbayeva, Abdulla and Oskenbayev2021)Footnote 4 find a positive relationship between good governance and better pandemic outcomes, while Toshkov et al. (Reference Toshkov, Carroll and Yesilkagit2022) find a negative relationship. Although the World Bank’s index includes measures of state capacity, it also includes other measures that are politically motivated and thus deviate from the central concept. This measurement issue could contribute to the inconsistency in the results. Similarly, Knutsen and Kolvani (Reference Knutsen and Kolvani2022) use a rule of law indicator to proxy state capacity, which also does not measure the true concept. Most importantly for our purposes, these studies use metrics that can only explain cross-national variation.Footnote 5 Our subnational design overcomes these empirical challenges to examine the differences in outcomes among US states.
Theory and hypotheses
As the ability to execute a policy, capacity is separate from the formation of the policy goal. Given the policy goal formed, higher capacity will mean superior execution. We posit that state leaders across the US were against mass public death, at least in a de minimus sense. They need not do anything and everything possible to save lives, and arguably constituents would not want them to do so (e.g., states do not drop speed limits to 25 miles per hour to avoid traffic fatalities or ban smoking). Some harms that state leaders sought to mitigate during the pandemic, for instance, were economic. States therefore needed to weigh economic concerns against public health concerns. We address economic factors in Supplementary Appendix Tables 14 and 15, which show that our results are robust to accounting for states’ economic dependence on the service and recreation sectors, which might pull against policies mitigating COVID-19 transmission. Our assumption therefore acknowledges that state governments did not have uniform policy preferences in regard to mitigating COVID-19-related deaths, nor did they necessarily have the same implicit valuations of civilian lives, nor did they make the same trade-offs in regard to adopting costly life-saving policies. However, we contend that no state government has a pro-death agenda during a pandemic.Footnote 6 More is said on this assumption in Supplementary Appendix 2.2. Thus, we anticipate that high state capacity states will achieve greater amelioration from the COVID-19 pandemic than low capacity states. We can link this to states’ success at averting deaths and implementing vaccination.
Hypothesis 1: Higher capacity states should have lower rates of excess deaths in 2020.
Hypothesis 2: High capacity states should have higher rates of vaccination in early 2021.
The opposition to mass public death can be witnessed in the prevalence of mitigation strategies that state legislatures and governors employed. For instance, schools were closed, gathering was restricted, and non-essential businesses were closed. In keeping with our assumption that legislators wanted to reduce the harms of the pandemic, every state adopted at least some pandemic mitigation policies.Footnote 7
In theory, these policies were enacted with the goal of reducing deaths. However, for these policies to work effectively, states need the capacity to enforce them. Consider the argument that masks work but mask mandates do not; if the mandate is not enforced, it cannot prevent infections or save lives. Thus, we posit that state-level COVID-19 mitigation policies will lower mortality when they are joined with higher levels of state capacity by causing people to follow safer practices (e.g., no mass gathering), even if public support is imperfect. For instance, Immormino and Stowell (Reference Immormino and Stowell2022) find a relationship between “policy stringency” and high-tax provinces in reducing deaths, while Stowell et al. (Reference Stowell, Immormino, Salazar, Zeng and Arbetman-Rabinowitz2022, 8) find that policy stringency’s efficacy depends on “the degree to which the government is involved in the economic activities of the population, relative to expectations, given the education and employment levels of the populace.” Our examination focuses state capacity – the ability to enforce policies – as opposed to economic extraction. State capacity improves public health outcomes as the mechanism for converting public health policy into popular compliance.
Hypothesis 3: State restrictions will lead to lower rates of excess deaths in 2020 in states with higher state capacity.
We do not include a hypothesis about vaccination here because the state policies targeted reducing contact and thereby spread. These state policies did not seek to enforce vaccination. Thus, that analysis instead considers the ability to deliver vaccinations early in their availability when there was substantial and unfilled demand.Footnote 8
Data and design
There are no extant subnational metrics for state capacity in American states. Comparative studies of state capacity often draw on proxy measures that are not applicable to the US case (e.g., tax revenues, military personnel); however, many of these measures are contaminated by political ideology and political will. For example, all American states have tax authority, and they set their tax rates strategically. Previous comparative studies of subnational variation in state capacity have also drawn on techniques that do not apply to the US states, such as colonial infrastructure (Acemoglu et al. Reference Acemoglu, Garca-Jimeno and Robinson2015), age heaping in census reports (Lee and Zhang Reference Lee and Zhang2017), government repression of protest (Sullivan Reference Sullivan2021), or meritocratic recruitment and predictability of bureaucratic careers (Bersch et al. Reference Bersch, Praça and Taylor2017). All American states either have sufficient capacity to address these issues or these domains are handled at the federal level. To measure subnational variations in state capacity for American states, we need a measure that draws on items assessed at the state level and for which there is subnational variation. Pre-existing measures are not suitable for our purpose.
As such, to measure variation in state capacity throughout the US, we introduce a reflective, latent-trait measure based on indicators of states’ relative capacity to enact their will. This approach is comparable to Treier and Jackman (Reference Treier and Jackman2008)‘s latent measure of democracy, which incorporates many different democracy scores but is not indicative of a set of criteria for democracy, and Hanson and Sigman (Reference Hanson and Sigman2021)‘s work on state capacity across countries.
Construct measures are innately either reflective or formative. Reflective measurements are not formed from parts of the construct. Rather, the components of the measurement are caused by the construct itself. The canonical reflective measure is intelligence. Test questions on an intelligence test do not makeup intelligence, but instead, reflect the test takers’ underlying intelligence. Responses (measured with error) indicate the test-takers latent ability. In our case, states have low crime and high literacy rates because of their capacity (all states would have lower crime or higher literacy if capable). Formative or composite measures, on the other hand, are measured by combining the multiple components that constitute the construct. For formative measures, the canonical example is socioeconomic status, which is a combination of education, wealth, and occupational prestige. It is not that these elements of the construct are caused by SES, but rather that SES is the combined influence of these components (Stenner et al. Reference Stenner, Burdick and Stone2008). We do not use a composite measure because the components that comprise state capacity are unknowable in number and thus not accurately measurable. Previous studies have also been unable to empirically validate the mulitidimensionality of state capacity. As such, a reflective measure is the most accurate option. In treating it as a latent trait, we deviate from previous studies that try to focus on one area of capacity, such as revenue extraction, bureaucratic capacity, or coercive capacity, to measure state capacity. Our reflective approach is in line with recommendations from Williams (Reference Williams2021), who argues in favor of a performance-based measure of capacity rather than “hypothetical capacity.” More is said on the distinction between reflective and composite measurements in Supplementary Appendix 2.
To distinguish the capacity to act from the intention to act, we focus on outcomes for which we believe there is a general will to achieve that objective. That is not to say that state governments have uniform preferences or that they agree about the strategies and techniques by which to pursue these goals. However, what it does mean is that leaders of any ideological bent would want the outcomes to move in the same direction. Success in these domains thus marks the state’s ability to fulfill a goal, rather than an assessment of which goals a state actually has. To illustrate this point, high capacity enables a state to do many things, but there are some goals that not all states share. For instance, it not only takes a high capacity to run a generous welfare system but also the political will to have a generous welfare system. By focusing on shared goals, we avoid conflating ideology with capacity for execution. For instance, we consider the choice to expand the size of the state (e.g., the bureaucracy) political, so we do not include direct measures of government size. We are necessarily selective in identifying outcomes that we believe are generally shared in society, including across ideological profiles. However, even if one policy were disputable, the latent-trait modeling framework protects against bias from a single indicator. Because we are using a reflective measure of state capacity, our measure is robust to dropping any single indicator; the modified measures are highly correlated with the metric used in this study (r > 0.95) (Supplementary Appendix 2.1).
Our intention to separate the will to action from the ability for action is not an assertion that ability is entirely removed from politics. States made decisions in the past that contributed to their present level of capacity (e.g., maintaining public records or building public communications systems). Politics may well influence the decision to empower the state. Future research may uncover the political and apolitical drivers of state capacity development. We measure capacity, however, distinctly from the will to any particular action.
We utilize exploratory factor analysis on our selection of indicators that reflect state capacity. Our version is a reflective measurement of the construct (state capacity) insofar as there are many different ways in which state capacity might manifest, and we seek indicators that reflect different levels of capacity, consistent with the definition of reflective measures from Sokolov (Reference Sokolov2018). In forming our reflective measure, we draw on a series of outcomes that have been used by previous scholars studying state capacity around the world. Our project is unique in comparing these health, crime, economic, and education outcomes across American states rather than countries. We favor these over other commonly used proxies for state capacity, such as revenue extraction, which can conflate the desire to extract certain amounts of revenue with the capacity to extract. The list incorporates prior applications of our selected items as proxies for state capacity.
We do not propose that every state wants all of these items equally and vociferously. For instance, some scholars argue that not all states or legislators value life equivalently (Miller Reference Miller2000; Kaplan et al. Reference Kaplan, Lefler and Zilberman2022). Latent-trait modeling addresses this concern. By drawing on multiple policy domains (e.g., health, crime, education), we avoid creating a measure of life-preservation-preference, education support, or crime reduction. We show in Supplementary Appendix 2.1 that there is a very high correlation of latent measures even when dropping any particular indicator (e.g., if we were to drop the infant mortality variable). As the citations below show, cross-national studies regularly use these items in isolation as proxies for capacity. We do not posit that all variation in outcomes on these metrics is entirely the result of state capacity. Private action, demographics, and chance can play a role in outcomes like infant mortality and literacy. However, these random facets would not apply to all of our diverse indicators. Effective states will be more successful at achieving these desired outcomes. The latent trait modeling strategy extracts that element from these multiple cases, and that element is our measure of state capacity.
-
• Infant mortality (Bustikova and Corduneanu-Huci Reference Bustikova and Corduneanu-Huci2017; Cingolani et al. Reference Cingolani, Thomsson and De Crombrugghe2015; Foa & Nemirovskaya Reference Foa and Nemirovskaya2016; Hanson Reference Hanson2015).
-
• Crime (Foa and Nemirovskaya Reference Foa and Nemirovskaya2016; Englehart Reference Englehart2009; Cruz Reference Cruz2011; Richani Reference Richani2010; Herrera & Martinelli Reference Herrera and Martinelli2013; Soifer Reference Soifer2012).
-
• Corruption (Bersch et al. Reference Bersch, Praça and Taylor2017; Bäck and Hadenius Reference Bäck and Hadenius2008; Fortin Reference Fortin2010).
-
• Poverty (Acemoglu et al. Reference Acemoglu, Garca-Jimeno and Robinson2015; Andersen et al. Reference Andersen, Møller, Rørbæk and Skaaning2014; Fearon & Laitin Reference Fearon and Laitin2003; Foa and Nemirovskaya Reference Foa and Nemirovskaya2016)Footnote 9
-
• Primary or secondary education enrollment, literacy (Acemoglu et al. Reference Acemoglu, Garca-Jimeno and Robinson2015; Hanson Reference Hanson2015; Lee and Zhang Reference Lee and Zhang2017).
We argue that state capacity evolves sufficiently slowly that data from recent years strongly indicate the states’ capacities in 2020–2021, which is supported empirically in cross-national research (Fortin Reference Fortin2010; Hanson and Sigman Reference Hanson and Sigman2021). We recognize that states made choices historically that led to different levels of present state capacity. Factors such as demographics and partisanship were implicated in those choices. For instance, populations may have underdeveloped their capacity to avoid redistribution across race lines and instead favored community support mechanisms that omitted the state and equal redistribution. However, these decisions were made decades prior to the pandemic and are pre-treatment as far as the relationship between state capacity and COVID-19 outcomes is concerned. At the moment the exogenous shock struck, the level of state capacity was already established.
This is not to say that states did not attempt to build the capacity to respond to the crisis once it existed. Building an army is doable, after all, but it takes time, resources, and intentionality. For instance, the state governments attempted to purchase healthcare supplies, dragoon medical and security workers into response and enforcement, and direct funding towards harmed sectors. Spending is not, itself, capacity, and capacity cannot merely be immediately purchased; funding is necessary but insufficient for policy implementation in many cases. For instance, Gamm and Kousser (Reference Gamm and Kousser2021) show that states that invested financially in certain domains were more successful.Footnote 10 Some of these resources required organizational infrastructure to implement. Marshaling these resources drew on some level of state capacity (e.g., to collect and collaborate with scientists, to draft the healthcare and security sectors into participation, to identify and disburse needed resources), so the higher capacity states could also build additional capacity faster. Purpose-built capacity on short notice would result in delays in policy implementation that would manifest in their differential outcomes. The temporary investments could not create a massive and sudden increase in capacity that would overpower past under-investment; it was evident at the time that states were spread thin in responding to the pandemic’s myriad harms. Overall, the need to build capacity delayed responding to the virus relative to those that already had higher levels of capacity. Thus, the outcomes in the first wave reflected the ex-ante differences, although other states were trying to catch up, and the potential to build capacity in the face of threat is subsumed into our paradigm that initial capacity was crucial to state responses to crises.
Table 1 details the variety of state-level indicators reflecting state capacity. All indicators are measured as a rate or ratio to account for different state population sizes. The latent variable explains 33% of the variation in the indicators.Footnote 11 We also normalize all of our variables before using factor analysis to make our measure less sensitive to the units used in measurement. As mentioned previously, the indicators incorporate a variety of policy goals: fiscal health, human capital, law and order, and public health. While the comparative literature on state capacity has most often linked capacity to better fiscal and public health outcomes, cross-national studies have also posited that democracies with greater state capacities have better primary and secondary education outcomes than low-capacity states (Hanson Reference Hanson2015; Knutsen Reference Knutsen2013). Other comparative work has linked weak capacity to higher violent crime rates (Englehart Reference Englehart2009; Herrera & Martinelli Reference Herrera and Martinelli2013; Richani Reference Richani2010). The diversity of our indicators makes our measurement of the latent trait more reliable. Moreover, this means that we are not merely using health outcomes to predict other health outcomes. As such, the latent trait is not just an ‘ability to save lives,’ a risk that would be posed if we drew only on life preservation policies or outcomes. Instead, the measure incorporates multiple domains of state efficacy.Footnote 12
Table 1. State capacity factor variable loadings

The factor loadings of our state capacity variable are shown in Table 1. Higher state capacity is treated as a positive. Undesirable outcomes, reflecting poor capacity (e.g., infant mortality), load negatively. A map showing the state capacity ratings in the US according to our measure is included (Figure 1). This is the general level of state capacity per state, not a COVID-19-based metric (COVID-19 outcomes by state are shown in the Supplementary Appendix).Footnote 13 High capacity states, such as New Hampshire and Minnesota, are lighter colored. In general, the Northeast and the Upper Midwest show the highest capacity. Low capacity states have darker colors. Mississippi and Louisiana – two exceptionally poor states in the heart of the formerly Jim Crow South – have the lowest capacity. We also provide a density plot of our measure showing a relatively normal distribution for the factor (Supplementary Appendix 3).

Figure 1. State Capacity Factor Map.
Other studies have appealed to notions of legislative capacity – using Squire’s metric or Bowen’s revision of it (Jordan & Grossmann Reference Jordan and Grossmann2020; Squire Reference Squire2007; Bowen & Greene Reference Bowen and Greene2014) – or bureaucratic capacity – the size of the bureaucracy relative to the population. While it makes sense for a larger government to be capable of achieving more goals – or being enlarged for the purpose of enacting an agenda – we do not consider these facts to themselves be state capacity. A state government may have highly-paid legislators, more employees, or legislators in longer sessions due to inefficiency as much as these features might be indicative of capacity. While having many employees could enable state governments to be effective, it would require them to be engaged in appropriate and strategic hiring and firing. More employees could also be related to ineffective or corrupt regimes.Footnote 14 Thus, these measures are not themselves sufficient proxies. The correlation with Squire’s most recent rating (2003) and state capacity is 0.27 and with Bowen’s most recent rating (2013) is 0.06. The robustness tests in Supplementary Appendix 4 show that these proxies are less efficient measurements than the latent measure used here.Footnote 15 The size of the bureaucracy is measured with the number of full-time state employees (in thousands) in 2016 (Jordan and Grossmann Reference Jordan and Grossmann2020) and the ratio of state employees to population size. The former is correlated at 0.18 with our state capacity measure and the latter at −0.17. Ultimately, we do not believe that these alternatives are appropriate proxies for state capacity because the constitutive elements have a limited relationship to the core construct. We hold that legislative professionalism and government size are, therefore, distinct from state capacity.
Our first dependent variable is the average percentage of excess deaths in the state from April 1 to December 31, 2020. It is the increase in deaths in the state relative to the number from 2019. This data comes from the Center for Disease Control’s National Center for Health Statistics.Footnote 16 Percent excess deaths refer to the number of observed excess deaths divided by the average expected count (upper bound estimate expected count is used as a robustness check in Supplementary Appendix 4). CDC data is collected weekly, so we take the average of the weekly percentage of excess deaths over this time period. We choose April 1st as the starting point since it is early in the pandemic, though late enough that COVID-19 had already spread throughout the country. We set January 1st as our cutoff date to avoid confounding this variable with vaccinations, as vaccinations reduce the number of excess deaths and large-scale state vaccination programs came into effect in 2021. We believe that it was in these early stages of the pandemic that state capacity would have the greatest impact in reducing deaths.
In the early weeks of vaccination, states controlled access through supply and availability policies. Capacity is expected to have led to earlier widespread vaccination. The vaccine-based dependent variables are the number of vaccine units distributed per 100,000 people — expressed as a proportion — and the percent of the population that has completed a vaccine series.Footnote 17 The numbers are the CDC-reported state outcomes by April 1, 2021. Vaccine policies subsequent to this date were confounded by federal mandates; our focus on states requires excising federal influence, so we stopped the data count then.
To assess states’ anti-COVID policies, we turn to the dataset, “State-level social distancing policies in response to COVID-19 in the U.S.” (Fullman et al. Reference Fullman, Bang-Jensen, Reinke, Magistro, Castellano, Erickson, Amano, Wilkerson and Adolph2020). We include data on whether or not a state enacted a state-wide mandate for five social distancing policies (gathering restrictions, non-essential business closures, school closures, restaurant restrictions, and stay-at-home orders) by July 1, 2020. All states had had a COVID-19 case by the end of March, so this would have been ample time for response to be appropriate and to materialize. Our discussion will focus on an additive index of these policies. As most policies were widely adopted, the state scores range from 2 to 5. 48 states scored three or higher, so there is not a great deal of variation in COVID-19 mitigation policies that states enacted. This further underscores our point that governments generally do not want their citizens to die.
We chose these five policies because they are policies that the state can introduce and enforce. There exists a limited number of levers states could pull, though political will is certainly a factor in choosing among options. For instance, the states did not have the will to implement a Wuhan-style lockdown in the US, even if they could have done it. In practice, many states did pull the same levers. We introduce the policy index additively first to examine the direct effects of anti-COVID-19 policies. We then interact the policy index with state capacity to demonstrate that these mitigation policies were more effective when they were coupled with capacity.
The widespread interest in COVID-19 mitigation does not show a partisan bias in implementation. In an OLS model with policy index as the dependent variable, states with higher average population age and larger minority populations implemented more policies. This likely reflects the higher death rates among the elderly and non-white Americans early in the pandemic. States with higher average individualism ratings also implemented more policies, possibly because legislators knew that would mean more state influence would be needed. We do not find significant effects from geography, population density, policy liberalism, Republican governor, or 2016 Trump vote share.Footnote 18
We include the interaction models for three of the policies. Gathering restrictions and restaurant restrictions were adopted in 49 and 50 cases respectively, so they do not have separate interaction models. We can speculate why these policies diverge in efficacy. Staying at home is directly related to limiting interpersonal contact, which limits spread. Closing non-essential businesses may reduce some spread, but the definitions of essential business vary across states, and substantial contact was possible in some “essential” spaces. School closures limited contact among the young and many were replaced in whole or in part by “pods” or private schools. As such, it may have done less, as a policy, to reduce contact than legislators would have hoped.
To assuage concerns that the outcomes were affected by partisanship, our models include a dummy for the Republican governor as a partisanship covariate. Adolph et al. (Reference Adolph, Amano, Bang-Jensen, Fullman and Wilkerson2021, Reference Adolph, Amano, Bang-Jensen, Fullman, Magistro, Reinke and Wilkerson2022) posit that Republican-governor-led states were slower to implement social distancing policies and mask mandates. An alternative specification of partisanship based on 2016 Trump vote share and legislature partisanship were examined as robustness checks (Supplementary Appendix 4). We also include the median population age in the state according to the 2019 American Community Survey as a covariate, given that age strongly predicts COVID-19 morbidity. Conditioning on the percentage of white residents in the state population demonstrates the effect is not driven by race and addresses concerns that states are deliberately incompetent when non-white populations are larger. Because of the limited number of cases (there are only 50 states), only a few covariates can be included in the models. Also, because the dependent variables in all our models are fractions, Beta regressions are used. Comparable OLS models and other robustness checks with controlling for different demographic, political, and economic covariates are shown in Supplementary Appendix 4.
Results
In Table 2, we present our regression results. We compare our measure of state capacity with mean excess deaths in 2020, vaccines per 100,000 people, and the percent of the population that was fully vaccinated as of April 1, 2021. We include the Republican governor, population age, and percent of the state population that is white as covariates. Despite the small N, we find consistent, significant effects. The models also explain a sizeable amount of variation in the dependent variables (30%–41%). States with higher capacity experienced fewer excess deaths (Model 1). They also distributed vaccines more successfully, both in terms of the units distributed (Model 2) and the population share that completed their vaccine series (Model 3).
Table 2. State capacity factor and COVID outcomes

All models are Beta regressions.
* p < 0.1.
** p < 0.05.
*** p < 0.01.
Although partisan disparities have dominated media coverage, partisanship does not predict medical outcomes when we account for capacity. The same holds for our multiple other metrics of partisanship. Furthermore, wealth might allow states to generate capacity over time (though they entered the pandemic with a pre-existing level of capacity), and one might fear that poor states would place greater weight on their economies than public health. We tested the models controlling for state wealth (gross state product) and found the results remain robust. The results are also robust considering the share of GSP from the recreation and service sectors of the economy, which might have been particularly impacted by shutdowns and could arguably have particularly motivated the state to re-open despite the health ramifications. Factors like wealth, housing structure, and racial demographics have been combined in attempts to measure localities’ susceptibility to crises. In addition to showing robustness to demographic and wealth covariates, we examined the robustness of the CDC’s Social Vulnerability Index (SVI). We would posit that these are the conditions on the ground when the virus arrives, but SVI does not determine states’ ability to respond to the crisis circumstances upon arrival. In the models, the SVI does not significantly predict COVID-19 outcomes, and the states’ state capacity is still significantly predictive (Supplementary Appendix 4).
Vaccine behavior could also be influenced by generalized vaccine or medical hesitancy. To account for this, we control for the flu vaccination rate from the 2019 to 2020 flu season, which immediately preceded the COVID pandemic (Supplementary Appendix 4), and find comparably significant results. We also introduce controls for population density, state location (latitude and longitude), census region, and state-level individualist culture; we believe that this captures residual potential effects from spatiotemporal considerations as well as potential interstate diffusion. We also ran the models controlling for the number of days since the first US case before the first case in that state. Our results are robust to all of these factors (Supplementary Appendix 4). A summary of all of our robustness checks is available in Supplementary Appendix 4, Table 5.
In theory, states could “borrow” capacity from civil society. For instance, leaders could call on social groups to enforce distancing regulations or turn to groups like Doctors without Borders or Samaritan’s Purse for medical aid. To account for this possibility, we repeat the models including a covariate for state social capital. While the mean excess death rate was lower in areas with higher social capital, the effect of state capacity is evident, even accounting for this parallel social capacity potentiality (Supplementary Appendix 4).
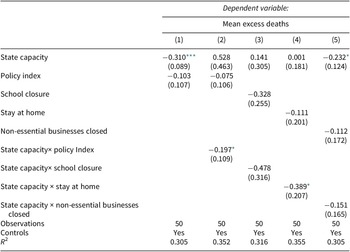
The effects of state policies are shown in Table 3. We include the overall policy index in Model 1, which is not significant and does not appreciably change the magnitude of the effect of state capacity on excess deaths from Table 2. This suggests that states’ mitigation policies were not, on their own, actually mitigating the COVID-19 death toll. This is consistent with policies not being self-enforcing or automatically obeyed by the public. The executive’s ability to enforce compliance is then pertinent to understanding whether state policies would save lives.
Table 3. State capacity, state policies, and COVID outcomes

Note: All models are Beta regressions. Controls are the same as Table 2. They are suppressed here for readability.
* p < 0.1.
** p < 0.05.
*** p < 0.01.
We then interact the additive policy index of COVID mitigation policies with state capacity in Model 2. We do the same with the individual policies in Models 3–5. There is a marginally significant negative interaction with state capacity (p = 0.07). Mitigation policies were effective at lowering excess death rates in the states with the capacity to enforce their policies. Stay-at-home orders seem to be driving the effect. This makes sense, insofar as those being the laws where compliance would be most dependent on enforcement. It would be very hard to defy a school closing order on the individual level; the school is closed. States need enforcement capacity to make people stay at home. Thus, this is a textbook example of state capacity, which is the ability of states to make and enact policies, in action. These states converted the generalized desire to avert mass death into mitigation. This result affirms the third hypothesis.
Figure 2 visualizes the interaction effect between the policy index and state capacity by looking at the predicted mean excess deaths. For visual clarity, we have broken down state capacity between “high capacity” states (the top quartile) and “low capacity” states (the remaining 37 states), but otherwise, this is identical to Model 2 from Table 3. Enacting anti-Covid policies only mitigates excess deaths at the higher levels of state capacity. Among low-capacity states, more policies do not lead to significantly fewer excess deaths; there is, indeed, almost no relationship among the lower-capacity states between policies enacted and predicted mean excess deaths. We find that, for states enacting all five policies in our COVID mitigation policies index, the difference between being low-capacity and high-capacity is equal to a difference in 8% mean excess deaths predicted. This pattern provides direct evidence for how different levels of state capacity translate into differential COVID-19 outcomes and would presumably have a direct effect on other policy outcomes (though that is beyond the scope of this article).

Figure 2. Predicted Mean Excess Deaths as a Function of State Capacity and Covid Policies.
Discussion and conclusion
This article has connected variations in state capacity among the US states to COVID-19 pandemic health outcomes. Our novel measure of state capacity addresses the latent levels of subnational state capacity irrespective of states’ political ideology. We find that higher levels of state capacity led to better performance in stemming excess deaths and vaccinating citizens within their borders. This was particularly manifest in the ability to enforce anti-COVID restrictions. Every state government adopted at least some restrictions in the face of the pandemic. Only governments in states with the capacity to turn their wishes into realities were able to use these policies to lower excess mortality. Without enforcement capacity, the policies were ineffectual.
We can now turn back to our motivating examples of West Virginia versus Mississippi and New York versus Massachusetts. What accounts for the differences in COVID-19 outcomes for these two pairs of states? It is not partisanship since the first two are decidedly Republican states, and the latter two are Democratic states. It is not merely social distancing policies, since they had identical COVID-19 mitigation policies (all four had five out of five on our COVID-19 policy scale). The big difference between the pairs of states is their state capacity: Mississippi is our 50th-ranked state whereas West Virginia is 24th. Similarly, New York is our 26th-ranked state, whereas Massachusetts is our 5th. These differences in capacity allowed them to turn a mutual desire into differential success. The higher capacity states were more successful at mitigating increased death during the COVID-19 pandemic.
Our study also helps to understand why previous research has identified conflicting effects of federalism in countries’ responses to COVID-19 (Shvetsova et al. Reference Shvetsova, Zhirnov, VanDusky-Allen, Adeel, Catalano, Catalano, Giannelli, Muftuoglu, Riggs and Sezgin2020; Greer et al. Reference Greer, King, da Fonseca and Peralta-Santos2020; Toshkov et al. Reference Toshkov, Carroll and Yesilkagit2022). Federalism can give subnational regions, like the US states, the autonomy to act based on their own needs or innovate in response policies. In theory, this would make them more flexible and better able to identify their localized needs. However, our research suggests that federalism can undermine the pandemic response if the states are not able, due to a lack of capacity, to effectively act on their own. As we have noted, eventually, the Biden administration mandated policies like vaccine availability at the federal level, taking the issue from the states. We stop our analysis before this point in order to focus on the states and their responses. Thus where higher levels of government can marshal greater capacity, or the goal is readily shared across the country, the central administration may be more effective than sub-national authorities to achieve uniform response or equal outcomes in the American states. However, as Rocco et al. (Reference Rocco, Béland and Waddan2020) warn, even seemingly uniform national policies that require some degree of implementation at the state level, such as unemployment funding, can lead to unequal implementation and outcomes among states. Between-state or between-region disparities in capacity should therefore be considered before advocating for federalism as a policy solution.
We acknowledge the limitations of our present study. Our measure of state capacity is cross-sectional, and it does not address antecedent policy preferences. Some of the metrics used to identify state capacity are also older than others; this is a function of data availability. We rely on the slowness of change in state capacity for measurement stability (Hanson and Sigman Reference Hanson and Sigman2021). Additionally, we are restricted to observational data. As such, we cannot prove causation. It would certainly be unethical to introduce a multi-state harm in order to test responses. We are confident, nonetheless, that no state anticipated COVID-19 and developed capacity with this pandemic in mind. Some states had already chosen over decades to invest in capacity building to facilitate other policy goals – meaning states had varied levels of capacity before the onset of the pandemic – and higher capacity states were thus better situated to respond to an unanticipated event. Future research could introduce greater time spans and examine the differential effects of state capacity on other US pandemics (e.g., 1918 and 1957 Flu Pandemics).
Furthermore, this study demonstrates that pandemic response is not solely a function of healthcare capacity or health-system structure. Pandemic preparedness indexes based on health-system metrics were not highly predictive of COVID-19 outcomes (Abbey et al. Reference Abbey, Khalifa, Oduwole, Ayeh, Nudotor, Salia, Lasisi, Bennett, Yusuf and Agwu2020; Kachali et al. Reference Kachali, Haavisto, Leskelä, Väljä and Nuutinen2022). This is not to say that health-system capability and structure do not matter (Capano et al. Reference Capano, Howlett, Jarvis, Ramesh and Goyal2020; Capano Reference Capano2020; Gray et al. Reference Gray and Jenkins2021). However, state capacity writ large is also important in pandemic response. Our latent measure, although it reflects some state health metrics, demonstrates that state capacity, not just health-care system structure or ability, is useful for pandemic response.
While there exists a vast comparative, cross-national literature on state capacity, research on state capacity within the American context is more limited. Our analysis therefore makes a substantive and methodological contribution in linking states’ capacity to other developmental and welfare-enhancing outcomes in the US. While this research concludes that state capacity is a stronger predictor of COVID-19 outcomes than simple partisanship, we do not conclude that these are unrelated; it is likely that long-run investments in the building of state capacity is influenced by state-level politics and institutional design. A fruitful extension would be to look at the antecedents of state capacity and the political context through which differential capacities developed in the US states.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/spq.2024.11.
Data availability statement
Replication materials are available on SPPQ Dataverse at https://doi.org/10.15139/S3/PB5UMO (Auerbach Reference Auerbach2024).
Funding statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Competing interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author biographies
Kiran Auerbach is a Postdoctoral Researcher at the University of Zurich. She earned her PhD at University of North Carolina – Chapel Hill.
Joshua Y. Lerner is a data scientist at NORC at the University of Chicago and earned his PhD at Duke University.
Hannah Ridge is an Assistant Professor at Chapman University and earned her PhD at Duke University.







 Open access
Open access