


The promotion of health, especially targeted towards younger generations, has become a widely accepted endeavour in Europe. It is considered a form of education for healthy lifestyles, to prevent physical and psychological problems, and to enhance individuals’ sense of well-being. At present, the institutional, health, social and educational policies of the European Union are focusing on the prevention of obesity, a condition which continues to increase in prevalence among European children and adults. According to data published by the WHO in 2010, the percentage of overweight adults in Europe varies between 25 % and 70 %, depending on the country, while 5 % to 30 % of the population is classified as obese( 1 , 2 ). The prevalence of obese adults has tripled since the 1980s and is still increasing( 1 ). In addition, the first study of the European Childhood Obesity Surveillance Initiative( 3 ), carried out in thirteen countries including Italy, reported one-third of children between 6 and 9 years of age as being overweight or obese. Obesity accounts for 8 % of health-care costs and for 10–13 % of deaths in several countries within the European region( 3 ).
The obesity prevalence in Italy is monitored by the Osservatorio del Ministero della Salute ‘Okkio alla Salute’ (Health Ministry Monitor, ‘Watch your Health’). The latest report published by the Osservatorio, dating back to 2010, confirms the noted obesity trend in Europe described in the 2010 WHO report, estimating that 23 % of Italian children between 8 and 9 years old are overweight, while 11 % are obese( Reference Spinelli, Lamberti and Nardone 4 ).
One of the most significant European documents addressing the issue of childhood obesity is the 2007 White Paper entitled ‘A Strategy for Europe on nutrition, overweight and obesity related health issues’( 5 ), inspired by the Seventh Framework Programme for Research of the European Union (2007–2013)( 6 ). In this White Paper, the European Union aims to provide an integrated approach to nutrition and consumer policies in the areas of sports, education and transportation in order to reduce health problems related to unhealthy dietary habits. Specifically, the European Commission invites Member States of the European Union to develop ‘scientific information and education campaigns to raise awareness of the health problems related to poor nutrition, overweight, and obesity. These campaigns should particularly be addressed to vulnerable groups, such as children, deeming that locally focused actions, (...) targeting 0–12 year-olds will be effective in changing behaviour in the long run.’
In order to comply with guidelines outlined in the White Paper of the European Commission( 5 ), Italian political and institutional agencies have established the ‘Scuola e Cibo – Piano di Educazione Scolastica Alimentare, 2009–2015’ (‘School and Food – Nutrition Education Plan, 2009–2015’) with the purpose of developing and promoting initiatives for nutrition education and food safety in schools( 7 ). Through this initiative, nutrition education is introduced in schools as an interdisciplinary subject, employing teaching methods inspired by social cognitive and constructivist approaches and communication technologies, as described by the new ‘Linee guida per l’educazione alimentare nella scuola italiana’ (‘Guidelines for nutrition education in Italian schools’)( 8 ). Initiatives for nutrition education in schools recommended by the Italian government also include a media education approach because Italian children between 8 and 10 years old tend to eat foods advertised on television, which have a high caloric value( Reference Pira and Marrali 9 ). Even though the Ministry of Health recommends eating at least three portions of fruits and two portions of vegetables daily to prevent obesity, data show that at least 23 % of children do not eat any vegetables or fruit on a given day( 10 ). Thus, as it has in other countries, the promotion of fruit and vegetable consumption among children attending primary schools has become an important aim in Italy (11) .
According to several international researchers, effective interventions aimed at increasing children’s fruit and vegetable intake are those which: (i) are incorporated in regular school lessons( Reference Anderson, Porteus and Foster 12 – Reference Delgado-Noguera, Tort and Martínez-Zapata 17 ); (ii) involve parents and stakeholders( Reference Baranowski and Stables 18 – Reference Knai, Pomerleau and Lock 21 ); (iii) include taste tasting( Reference Wardle, Herrera and Cooke 22 , Reference Thomson, McCabe-Sellers and Strickland 23 ); and (iv) include the teaching of media literacy skills( Reference Baranowski, Baranowski and Cullen 24 – Reference Harris and Bargh 28 ).
Because research has found that the media’s images of food have a significant influence on children’s food preferences( Reference Livingstone and Helsper 29 – Reference Strasburger, Jordan and Donnerstein 33 ), our intervention specifically focused on the influences of food advertising. Media education/media literacy workshops that promote critical thinking about food advertising( Reference Milett and Bellotti 34 – Reference Messina and Grassi 37 ) are a recommended way to face the obesity issue. According to literature reviews and agencies such as the American Academy of Pediatrics, media literacy education is considered a key factor for health promotion, with recognized efficacy in countering the strong influence of communication media( 38 – Reference Bergsma and Carney 42 ).
The theoretical framework for the present study was based on the Health Promoting Media Literacy Education framework( Reference Bergsma and Ferris 43 ). This model involves constructs from the Theory of Reasoned Action( Reference Ajzen and Madden 44 ), in which a causal chain of Beliefs, Attitudes and Behavioural Intentions drives health behaviour at the individual level; and Social Cognitive Theory( Reference Bandura 45 ), which includes the constructs of Reciprocal Determinism, Behavioural Capability, Expectations, Self-efficacy, Observational Learning and Reinforcement; and four components of Media Literacy Education, namely Health and Media Knowledge, Critical Analysis and Expression Skills, Habits of Inquiry and Empowerment( Reference Buckingham 46 – Reference Pieter, Fröhlich and Emrich 48 ).
The purpose of the present study was to measure the effect of a school-based health and media education intervention on fruit and vegetable consumption and related variables among a sample of 10-year-old Italian children using a mixed-methods approach.
Method
Design
The research study utilized a mixed-methods approach with a quasi-experimental study as the main study and a qualitative study as the supplementary study. The quasi-experimental study involved an experimental group (children and one of their parents, referred to as the ‘index parent’ in the current paper) and a control group (children and an index parent). Data collection occurred at three points in time: pre-, post- (directly upon completion of the intervention) and delayed post-test (3 months after completion of the intervention). Self-reported data were collected from children and the index parents. Children completed self-administered surveys, which included items and scales measuring fruit and vegetable consumption, and motivation, self-efficacy and perceived parental social support related to fruit and vegetable consumption. Parents completed measures about their motivation and social support related to their children’s fruit and vegetable intake and the availability and accessibility of fruit and vegetables at home. The qualitative study involved three focus groups with children in the experimental group only. Open-ended focus group questions measured children’s health and media beliefs and knowledge, critical thinking and expression skills, intentions of behaviour and reinforcement/obstacles with regard to fruit and vegetable consumption, and their satisfaction with the intervention.
Participants
Children took part in the research after informed consent was obtained from their parents. Four different elementary schools in Treviso (Veneto Region of Italy) agreed to participate in the research. Students enrolled in the 5th grade class of each elementary school (four classes in total) were invited to participate in the research. Two classes were assigned to the intervention group and two classes were assigned to the control group. A total of sixty students agreed to participate. Twenty-seven children and index parents participated in the intervention group and thirty-three children and index parents participated in the control group. All students and their index parent completed baseline measures, post-test and delayed post-test measures (Table 2 presents descriptive information for child participants). Students and parents in the intervention group participated in the school intervention. Students and parents in the control group did not receive an intervention or activity or lesson about nutrition during the period of the research study.
Description of the intervention
The intervention consisted of a school-based programme for 5th grade students, which was completed during twelve 2 h sessions over the span of 10 weeks (from October to December 2012). The implementers of the intervention were a media educator (one of the researchers) and a dietitian of Treviso Ulss 9 Public Health District. The intervention was adapted from an intervention created for children in the USA( Reference Evans, Dave and Tanner 26 , Reference Tanner, Duhe and Evans 27 ).
The three components of the programme were: (i) health promotion, which included interactive activities promoting the consumption of fruits and vegetables (i.e. competition among different groups of children in the ‘quiz game on healthy eating’); (ii) media education, which included interactive activities on how to critically analyse food advertisements (i.e. change slogan and photos of famous advertising of junk food); and (iii) a health communication media-based campaign (eight sessions once weekly), during which children created different media products related to fruits and vegetables targeting their parents. The media campaign productions included one poster (to put in the kitchen), six weekly newsletters (to send to the parents’ email inbox) and one video commercial (to watch on television with the parents). During the intervention the children also completed with their parents two different homework tasks: (i) a week-long fruit and vegetable food log; and (ii) a list of different coloured fruits and vegetables. The poster was made on the fourth week of the intervention and parents were asked to display it in their kitchen for 6 weeks. The weekly newsletters were sent to the parents and the video commercial was watched by the parents on the last week of the intervention.
All children participated in the creation of all media products, which had different slogans. The slogan of the poster was ‘If you eat fruits and vegetables, you will live longer’; the slogan of one newsletter was ‘Red fruits make you happy and protect you from diseases’; and the slogan of the video was ‘Eating fruits and vegetables is important, be it at a restaurant or during a trip’ (in Italian language every slogan was made in rhyme).
The intervention targeted the children directly (through their attendance at the twelve sessions and their involvement in the development of the media campaign) and the parents indirectly (through their exposure to the campaign developed by their children).
Data collection
Data for the quasi-experimental design were collected from children and index parents at three points in time: (i) 1 week before the beginning of the intervention (pre-test); (ii) 1 week immediately upon completion of the intervention (post-test); and (iii) 3 months after completion of the intervention (delayed post-test). Children completed the questionnaires in class and parents filled out their questionnaires during a special meeting organized for data collection (parents who could not attend this meeting received the questionnaires at home from their children). Data for the qualitative study were collected from children in the intervention group during three focus groups after the collection of the post-test data. The focus groups were led by one researcher with the collaboration of an assistant.
Description of measures
For the quasi-experimental study, we used self-report measures that were validated in countries other than Italy. These items and scales were translated into the Italian language, culturally adapted for Italian food habits and tested in a pilot study before utilization in the main study. The pilot study involved 100 children aged 10 years (i.e. fifty-five males and forty-five females) and one parent of each child. Thirty-six of the 100 participants completed the re-test after 7 d. Values of Cronbach’s α for all scales on the child and parent surveys were >0·65. Pearson correlations for test–retest reliability for all scales were >0·55. No changes were made to the items on the instruments as individual items seemed to be clear to all participants. Table 1 presents summary information for the scales and items included on the child and parent questionnaires.
Table 1 Descriptive information for scales measuring child and parent constructs

NA, not applicable.
Child questionnaire
Children’s fruit and vegetable consumption was measured with the validated Pro-Children FFQ on fruit and vegetables( Reference Yngve, Wolf and Poortvliet 49 ) and completed by the children. This questionnaire is composed of five items (e.g. ‘How often do you usually eat fresh fruit?’). Response options range from 1 (‘never’) to 8 (‘every day, more than twice a day’).
Children’s self-efficacy for eating fruit and vegetables was measured with the self-efficacy scale developed by Sallis et al.( Reference Sallis, Grossman and Pinski 50 ). This scale is composed of thirty items ranging from 1 (‘very unsure I can’) to 6 (‘very sure I can’) about participants’ confidence on participating in healthy eating behaviours (e.g. ‘How sure are you that you can eat fruit and vegetables instead of chips?’). In the present study, Cronbach’s α for this scale was >0·90.
Children’s motivation for healthy eating was measured using a motivation scale developed by Wilson et al.( Reference Wilson, Teasley and Friend 51 ). This scale consists of twenty items that assess participants’ internal motivation for healthy eating (e.g. ‘Eating healthy is a priority of my life’), ranging from 1 (‘strongly agree’) to 6 (‘strongly disagree’). Cronbach’s α for this scale was >0·90 in the present study.
Children’s perceived parental support for fruit and vegetable intake was measured using two scales: (i) the Emotional Social Support scale by Sallis et al.( Reference Sallis, Grossman and Pinski 52 ); and (ii) the Instrumental Social Support scale, which was adapted from the scales by Barrera and Ainlay( Reference Barrera and Ainlay 53 ) and Stokes and Wilson( Reference Stokes and Wilson 54 ). The Perceived Parental Instrumental Social Support scale consists of seventeen items and the Perceived Parental Emotional Social Support scale consists of sixteen items assessing parental behaviours to improve their child’s fruit and vegetable intake during the last month. The Perceived Parental Instrumental Social Support scale and the Perceived Parental Emotional Social Support scale range from 1 (‘not at all’) to 5 (‘about every day’). Cronbach’s α for the Perceived Parental Instrumental Social Support scale in the present study was >0·80; for the Perceived Parental Emotional Social Support scale, Cronbach’s α was >0·70.
Parent questionnaire
Parents’ motivation for healthy eating was measured with the same scale used for measuring children’s motivation( Reference Wilson, Teasley and Friend 51 ). Cronbach’s α for the Motivation scale was >0·80.
Parents’ social support for their children’s fruit and vegetable intake used a scale developed by Dave et al.( Reference Dave, Evans and Condrasky 55 ) and was based on scales used to assess the children’s perceived social support. This scale was composed of thirty-three items measuring parents’ engagement in behaviours to improve their child’s fruit and vegetable intake. Response options range from 1 (‘not at all’) to 5 (‘about every day’). Cronbach’s α for the Parental Instrumental Social Support scale was >0·70. Cronbach’s α for the Parental Emotional Social Support scale was >0·65.
Fruit and vegetable availability and accessibility at home were measured with nine items. The items were based on a five-item index developed by Kratt et al.( Reference Kratt, Reynolds and Shewchuk 56 ) on availability of fruits and vegetables at home and a four-item index developed by Hearn et al.( Reference Hearn, Baranowski and Baranowski 57 ) on accessibility of fruits and vegetables at home. Items included ‘Did you have fresh fruit in your kitchen last week?’ Response options range from 1 (‘yes, every day’) to 4 (‘never’).
Demographics
A short self-administered survey containing demographic questions was completed by parents. The variables included their child’s sex, height, weight, age and birth nation, number of children and adults at home, parent’s educational attainment and parent’s employment status.
Focus group study
The semi-structured focus groups were conducted using a questioning protocol based on the questioning protocol used by Evans and Tanner( Reference Evans, Dave and Tanner 26 , Reference Tanner, Duhe and Evans 27 ) and Dixey et al.( Reference Dixey, Sahota and Atwal 58 ) about children’s fruit and vegetable consumption and healthy eating. The focus groups were guided by questions focusing on five topics: (i) behaviour and behavioural change upon completion of the intervention; (ii) healthy eating reinforcement; (iii) beliefs and knowledge about health and media; (iv) critical analysis and expression skills; and (v) opinions on the intervention.
Data analysis
Psychometric analyses were conducted for all scales included on the study surveys. Values of Cronbach’s α were calculated separately for each of the scales to evaluate the internal consistency of the scales for this specific sample. Factorial validity of the scales was examined using the extraction method of principal components analysis and the rotation method of Varimax with Kaiser normalization.
Analyses of the psychometric properties of some of the scales on the survey instruments indicated that some of the scales needed to be divided into subscales. The Perceived Parental Instrumental Social Support scale and the Parental Instrumental Social Support scale were each divided into Action and Information subscales, the Perceived Parental Emotional Social Support scale was divided into Positive and Negative subscales, and the Parental Emotional Social Support scale was divided into an Encouragement subscale, a Negative Modelling subscale and a Discouragement subscale. All of the subscales were treated independently in the subsequent analyses. Cronbach’s α analyses for the scales and subscales indicated adequate internal consistency (Table 1).
Initial data analysis procedures included descriptive analyses. Descriptive statistics were obtained for both the intervention group and the control group for the different variables of interest, including demographic, confounder and outcome measures at baseline. Mean, standard deviation and the range of scores were reported for all continuous variables. Frequencies were obtained for categorical variables. The demographic variables and the baseline levels for each of the study constructs were compared across the two study conditions, using the t test for continuous variables and the χ 2 test for categorical variables, to evaluate if the two groups were equivalent at baseline.
To test for the magnitude of the intervention effect on key outcomes, gain scores (i.e. within-subject changes in the level of outcome from baseline to post-test, as well as from baseline to delayed post-test) were computed for each subject in both the treatment and control conditions. Effect size was estimated as the difference in the magnitude of the gain scores across treatment and control conditions (i.e. a difference-in-difference approach). The distribution of gain scores was compared across conditions using an independent-samples t test to assess if the computed effect size was significantly different from zero, assuming a threshold for significance at P<0·05 and a two-tailed test. All analyses were conducted using the statistical software package IBM SPSS Statistics for Windows, Version 19.
For the focus group study, content analysis using Atlas.ti version 5 was carried out to find the family of codes. A co-occurrence analysis was completed to determine the relationships between families of codes.
Results
Quasi-experimental study
The demographic characteristics of the participants in each group are reported in Table 2. The recruitment rate for the intervention group and the control group was 67·5 % and 82·5 %, respectively. The students and parents who did not take part in the study either did not sign the informed consent form or were not able to complete the questionnaires because they were non-Italian speakers. The χ 2 test or Fisher’s exact test indicated no significant differences in demographic variables between the intervention and control groups (Table 2).
Table 2 Descriptive information for participants (n 60); 10-year-old Italian children and their parents, Treviso (Veneto Region of Italy), October–December 2012
The intervention was effective in significantly increasing children’s fruit and vegetable intake (Table 3). Results of the t-test analyses showed significant differences between the intervention and control group between pre-test and post-test scores on all food frequency index items (P=0·000). The results of the t tests measuring differences between pre-test and delayed post-test on food frequency items indicated that the intervention was effective in increasing children’s intakes of fresh fruit, raw vegetables and 100 % fruit juice three months after intervention completion (P<0·001; Table 4). In addition, results from the t tests on the difference between pre- and post-test results indicated significant differences on all psychosocial determinant scales for children (P=0·000) except for Perceived Parental Emotional Social Support–Negative (Table 3). Significant differences between the intervention and control group were also found between pre- and delayed post-test for Self-efficacy, Motivation, Perceived Parental Instrumental Social Support and Perceived Parental Emotional Social Support–Positive (P values ranging from 0·000 to 0·043; Table 4).
Table 3 Differences in pre-test and post-test scores for child constructs (difference-in-difference scores); 10-year-old Italian children, Treviso (Veneto Region of Italy), October–December 2012

Significant P values are indicated in bold font.
* Lower scores indicate higher level.
Table 4 Differences in pre-test and delayed post-test scores for child constructs (difference-in-difference scores); 10-year-old Italian children, Treviso (Veneto Region of Italy), October–December 2012
Significant P values are indicated in bold font.
* Lower scores indicate higher level.
The intervention was not effective in increasing parents’ psychosocial variables and availability and accessibility of fruits and vegetables at home (Table 5). Similar non-significant results were found between pre- and delayed post-test (Table 6) except for Parental Emotional Social Support–Negative Modelling.
Table 5 Differences in pre-test and post-test scores for parent constructs (difference-in-difference scores); parents of 10-year-old Italian children, Treviso (Veneto Region of Italy), October–December 2012
Significant P values are indicated in bold font.
* Lower scores indicate higher level.
Table 6 Difference in pre-test and delayed post-test scores for parent constructs (difference-in-difference scores); parents of 10-year-old Italian children, Treviso (Veneto Region of Italy), October–December 2012
Significant P values are indicated in bold font.
* Lower scores indicate higher level.
Results from focus group study
The focus group study involved twenty-one among the twenty-seven children of the intervention group because one child was ill and five other children were occupied in other unavoidable school activities on the day that the focus groups were conducted. The children were divided into three subgroups (consisting of six, seven and eight children). Each of the three focus groups was 45 min long. The focus groups were recorded and transcribed verbatim for content analyses on the five main topics of investigation: (i) behaviour and behavioural change upon completion of the intervention; (ii) healthy eating reinforcement; (iii) health and media beliefs and knowledge; (iv) critical analysis and expression skills; and (v) opinions on the intervention. These specific topics were derived from the study’s Health Promoting Media Literacy Education framework (Fig. 1).
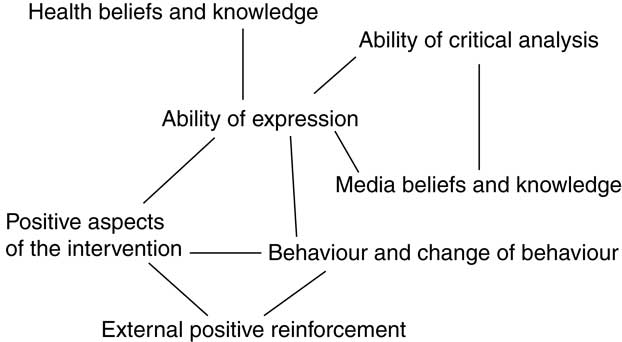
Fig. 1 Health Promoting Media Literacy Education framework applied in the present study
Results indicated fifteen families of codes which emerged from the content analyses (Table 7): (i) Behaviour; (ii) Changes of behaviour; (iii) Health knowledge; (iv) Media knowledge; (v) Health beliefs; (vi) Media beliefs; (vii) External positive reinforcement; (viii) External negative reinforcement; (ix) Internal positive reinforcement; (x) Internal negative reinforcement; (xi) Ability of critical analysis; (xii) Ability of expression; (xiii) Intervention’s positive aspects; (xiv) Intervention’s negative aspects; and (xv) Intervention’s recommended changes.
Table 7 Themes and families of codes emerging from the focus group content analysis; 10-year-old Italian children, Treviso (Veneto Region of Italy), October–December 2012
Results from qualitative data analysis increased the understanding of the quantitative data results. The quantitative data revealed the strength of effects (change in variables) that the intervention produced, while the focus group content analysis results revealed how the intervention produced these effects. During the focus groups, children reported behavioural changes such as eating more fruits and vegetables and less junk food, eating some fruits they didn’t like before, and eating more fruit while participating in sports. They also reported having learned how to follow a healthy diet and asking their parents to buy more fruits and vegetables. Moreover, they reported that they offer fruits and vegetables to friends and encourage others to eat healthy foods, becoming a sort of ‘healthy eating promoter’.
The external positive reinforcements reported by the children were internal, social (parents, relatives and friends) and environmental (newsletters and posters, availability of healthy food, unavailability of junk food). Similarly, the external negative reinforcements were internal, social (parents, relatives and friends) and environmental (parties and availability of junk food). Children indicated as an internal positive reinforcement ‘knowing that fruits and vegetables make you healthier’ and as an internal negative reinforcement ‘fear of not being able to resist junk food’.
In terms of their thoughts about the intervention, they especially appreciated the media component of the intervention because they had the opportunity to be creative and develop different products for the media campaign. Related to this, they reported several important critical analysis and expression skills learned during the intervention: ‘advertising is different from reality’ and ‘advertising shows happiness to influence us’.
The content analyses revealed that a lot of quotations pertained to more than one family of codes. For example, the quote ‘In order to create a great newsletter we needed to eat the fruits that we had to describe in the newsletter’ pertains to both the code family of ‘ability of expression’ and the code family of ‘behaviour’. The co-occurrences analysis was suitable for determining the relationships between families of codes in the study because the analysis revealed which codes of different families co-occurred in the same quotations. Co-occurrence analysis results suggested that ‘ability of expression’ became the central core of the relationships among almost all of the other theoretical constructs investigated. Specifically, it co-occurred with: health beliefs and health knowledge, media beliefs and media knowledge, critical analysis, positive aspects of the intervention, and behaviour and change of behaviour (Fig. 1).
Discussion
The purpose of the present study was to measure the effect of a school-based health and media education intervention on fruit and vegetable consumption and related variables among a sample of 10-year-old Italian children using a mixed-methods approach. A unique strength of the study was the mixed-methods approach. The mixed-methods approach allows researchers to bridge quantitative and qualitative research. More specifically, it allows researchers to explain the quantitative results at a much deeper level( Reference Tashakkori and Teddlie 59 – Reference Johnson and Onwuegbuzie 61 ). For example, in the present study it underscored the importance of measuring a specific construct (e.g. ‘ability of expression’) which is not a construct typically measured in these types of study.
Quantitative results indicate that this intervention was effective for changing almost all of the psychosocial and behavioural constructs of the intervention children measured for the present study. In addition, the parental constructs of Parental Instrumental Social Support–Information and Parental Emotional Social Support–Positive increased significantly as well and maintained their significance in the delayed post-test. Given that the children were the direct target of the intervention and parents the indirect target (through the media products that were brought home by the children), the results are congruent with the dose of the intervention received by children v. parents( Reference Evans, Dave and Tanner 26 , Reference Teufel, Perry and Story 62 – Reference McGarvey, Keller and Forrester 65 ). Nevertheless, the involvement of parents in the intervention was important because parental social support is considered a crucial determinant for children’s engagement in healthy behaviours( Reference Bandura 45 , Reference Reynolds, Hinton and Shewchuk 66 – Reference Tildesley and Andrews 71 ).
Parental pre-test scores were high for both the social support and availability and accessibility of fruits and vegetables variables. These results indicate that the children had positive food environmental conditions and strong support from their parents before the start of the intervention. Several past studies indicated that the availability and accessibility of fruits and vegetables is a fundamental condition to develop healthy eating habits( Reference Reynolds, Franklin and Binkley 19 , Reference Baranowski, Baranowski and Cullen 24 , Reference Evans, Dave and Tanner 26 , Reference Kratt, Reynolds and Shewchuk 56 , Reference Cullen, Baranowski and Owens 72 – Reference Fitzgerald, Heary and Nixon 76 ), but the results of that previous research also suggest that availability and accessibility is likely not enough without the improvement of psychosocial variables such as motivation( Reference Reynolds, Hinton and Shewchuk 66 ), self-efficacy( Reference De Bourdeaudhuij, Klepp and Due 77 – Reference O’Dea and Wilson 79 ) and perceived parental social support( Reference Baranowski, Davis and Resnicow 80 , Reference Young, Fors and Hayes 81 ).
The intervention was created following the recommendations of several previous studies( Reference Knai, Pomerleau and Lock 21 , Reference Harris and Bargh 28 , Reference Buttriss, Stanner and McKevith 82 ) on the effects of media education interventions on healthy eating behaviours of children. These studies indicated that the intervention should be conducted during school lessons, involve the parents, include healthy food intake during the sessions, be conducted with interactive methods, include media education workshops, focus especially on healthy eating and focus in general on healthy lifestyle behaviours. The intervention most likely increased perceived parental support because it included some media products targeting the parents, similar to the ‘Gimme 5’ study by Baranowski et al.( Reference Baranowski, Davis and Resnicow 80 ), and the involvement of parents in helping their children to do the homework, similar to a study conducted by Davis et al.( Reference Davis, Baranowski and Resnicow 83 ).
In the field of study on health-promoting media literacy education, there are some researchers focusing on effective media education interventions targeted to children on fruit and vegetable intake promotion( Reference Evans, Dave and Tanner 26 , Reference Tanner, Duhe and Evans 27 ). These researchers chose the media literacy production approach to promote healthy eating. The ‘production’ approach consisted of the creation of media messages, after a stage of critical thinking development, through a reflexive analysis of the products transmitted by the media (language, contents, purpose)( Reference Buckingham 46 – Reference Pieter, Fröhlich and Emrich 48 ). In particular, studies conducted by Kupersmidt et al.( Reference Kupersmidt, Scull and Austin 84 ) and Pinkleton et al.( Reference Pinkleton, Austin and Chen 85 ) report the effectiveness of the media education production approach in improving healthy behaviours and self-efficacy. For our intervention’s third component we adopted the ‘production’ approach, which consisted of the creation of different media messages for a television commercial, some newsletters and a poster, as described above.
The focus group content analysis confirmed the results of the quantitative data analysis. The children reported that they increased their fruit and vegetable intake. According to the children, they changed their food habits because during the intervention they had the opportunity to taste some fruits that they had never tried before and liked them. This is similar to results found in previous studies( Reference Wardle, Herrera and Cooke 22 , Reference Thomson, McCabe-Sellers and Strickland 23 , Reference Tanner, Duhe and Evans 27 , Reference Domel and Thompson 86 ) which suggest that children’s exposure to fruits and vegetables at school can increase preference, which can then lead to increased consumption. Children also reported that they were more motivated to eat fruits and vegetables because they were aware of the positive effects of fruits and vegetables on health and they had a chance to establish their personal health goals. These results are similar to those of the studies by Cullen et al.( Reference Cullen, Zakeri and Pryor 87 ) and Anderson et al.( Reference Anderson, Porteus and Foster 12 ).
The co-occurrence analysis of the qualitative data put ‘ability of expression’ in the central core of the relationship between most of the theoretical constructs investigated. ‘Ability of expression’ is one of the main skills stimulated by the media education production approach( Reference Bergsma and Ferris 43 , Reference Buckingham 46 , Reference Galliani 88 – Reference Ardizzone and Rivoltella 90 ), so this result pertains especially to the ‘pedagogical approach’ as recent studies on media literacy education recommend( Reference Bergsma and Carney 42 , Reference Bergsma and Ferris 43 ). Some authors( Reference Buckingham 46 , Reference Messina 89 , Reference Falcinelli 91 ) consider the media education production approach to be highly motivating for children because the children are intimately involved in the creation process. This pedagogical method simulates ‘significant’ learning because its activities are organized as ‘optimally challenging tasks’( Reference Harter 92 ) for children, corresponding to children’s objectives and expectations and being especially interesting for their usefulness in real life. In addition, the production of media messages develops competency in communication( Reference Ardizzone and Rivoltella 90 ) and stimulates a direct involvement in the creative process( Reference Mantovani, Bissoli and Barison 36 , Reference Burn and Durran 93 ).
As with any study, the present study had several limitations. The first limitation is the small sample size. The sample included a total of sixty students who were divided between an intervention group and a control group. However, that statistically significant findings were found even with this small sample size is very encouraging. The second limitation is the small period of time between the post-test and the delayed post-test (i.e. 3 months). However, many studies do not include a delayed post-test at all; so even though the time frame was short, a study strength is the inclusion of a delayed post-test. A third limitation is the measurement of fruit and vegetable intake. Ideally, this would have been measured using multiple 24 h dietary recalls. However, given the limited funding for the study, this was not feasible. Using a validated FFQ that was previously used with European children was a satisfactory alternative method of measuring dietary intake.
Conclusions
The present study results confirm the efficacy of a school-based health and media education intervention to address the children’s obesity issue and, in particular, to increase children’s fruit and vegetable intake( Reference Evans, Dave and Tanner 26 , Reference Tanner, Duhe and Evans 27 , Reference Bergsma and Carney 42 , Reference Baranowski, Davis and Resnicow 80 ). Although the study was small it opens a new perspective on the theoretical constructs investigated, because the development of ‘ability of expression’ could be considered one of the most important factors to determine the efficacy of the intervention. We recommend, following Bergsma( Reference Bergsma 94 ), that future research focuses more intensely on the ‘media literacy core concepts/skills’( Reference Bergsma and Carney 42 ). Another recommendation for future studies is to find other strategies to reach the parents so that they receive a greater dose of intervention, because parents are the gatekeepers to the food environment at home (and to a limited extent in the community). A third recommendation for future research is to extend the delayed post-test to determine the sustainability of the noted changes in the children’s behavioural and psychosocial variables.
Lastly, an important collateral result of the present research could be considered the creation of a collaboration among different stakeholders at the following levels: university (Doctoral School of Padua University and University of Texas School of Public Health); health district (Dipartimento di Prevenzione della Ulss 9 – Treviso); fruit and vegetable farmers (Azienda OPO Veneto – Organizzazione Produttori Ortofrutticoli di Zero Branco) who delivered fruits and vegetables during the intervention; and (iv) school district (Treviso ‘Serena’, Treviso ‘De Amicis’, Oderzo and Fontanelle). This collaboration could open several future developments; for example, the creation of a ‘didactic standard format’ based on the media education production workshop to increase children’s fruit and vegetable intake with a specific training for teachers, or the inclusion of the current intervention in a multicomponent project to prevent childhood obesity. In conclusion, we can consider the present study an attempt to establish a rich dialogue between educational research and medical research, which is strongly invocated especially in Italy( Reference Bergsma 94 , Reference Bertolini 95 ).
Acknowledgements
The authors would like to acknowledge Sian – Dipartimento di Prevenzione della Ulss 9 – Treviso, OPO Veneto – Organizzazione Produttori Ortofrutticoli di Zero Branco (TV), Istituti comprensivi di Treviso ‘Serena’, Treviso ‘De Amicis’, Oderzo e Fontanelle, and the Michael and Susan Dell Center for Healthy Living for their involvement in the research. The authors would also like to thank Sarah Bentley for all her help in editing the manuscript. Financial support: This research received no grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: None. Authorship: E.G. contributed by designing and conducting the study, and wrote the first draft of the paper. A.E. contributed by assisting with all aspects of study design, implementation and evaluation, and assisted in the writing of the manuscript. N.R. contributed by assisting with all statistical analyses and reviewing the manuscript. S.D.P. contributed by helping implement the intervention and reviewing the manuscript. L.M. contributed by assisting E.G. with funding for travel to the USA for internship and reviewing the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the University of Padova, Department of Humanities: Philosophy, Sociology, Education, and Applied Psychology, respecting the ethical principles currently adopted. Being a non-medical department, no formal regulation to conduct research with human subjects exists. Written informed consent was obtained from all subjects/patients. Verbal consent was witnessed and formally recorded.








