


The use of food supplements has increased substantially throughout the developed world, including Europe, where these products are regulated by Directive 2002/46/EC(1). A study undertaken by European Advisory Services for the Directorate-General for Health and Consumers (DG SANCO) of the European Commission estimated the total value of the EU food supplements market in 2005 at about five billion Euros. This comprises food supplements containing vitamins and minerals (50 %), supplements containing ‘other substances’ (43 %), tonics and bottled nutritive drinks (7 %). The four EU Member States with the largest markets in terms of sales of ‘other substances’ are Italy in first place, closely followed by Germany, the UK and France(2, 3).
Various surveys on the use of food supplements and/or functional foods have been carried out in European countries, in which information about the demographic, physical, lifestyle and health characteristics of food supplement users have also been collected(Reference Reinert, Rohrmann and Becker4–Reference Kiely, Flynn and Harrington13). In most cases the variables found to be related to supplement use were age, gender, education, income and lifestyle variables such as drinking, smoking and exercising(Reference Reinert, Rohrmann and Becker4–Reference Knudsen, Rasmussen and Haraldsdóttir10). Significant differences in food consumption were also observed, indicating a tendency for healthier food choices among users of supplements(Reference Reinert, Rohrmann and Becker4, Reference McNaughton, Mishra and Paul6, Reference Beitz, Mensink and Hintzpeter11).
In Italy, to our knowledge, no specific surveys have been carried out on this topic. Therefore the first aim of the present study was to collect data on the consumption of food supplements in a sample of the adult population from different areas of Italy and to characterize the users by demographic, physical and health-related characteristics, lifestyle and behaviour. Moreover, the second purpose was also to obtain information on the use of different categories of food supplements and to investigate if the determinants of usage differ according to product as reported in other studies(Reference de Jong, Ocké and Branderhorst9, Reference Hoggatt, Bernstein and Reynolds14–Reference Kim, Lee and Shin17).
These data are important in light of public health issues and to provide indications to the general population.
Materials and methods
Selection of participants
Sampling was carried out in two stages to select potential participants aged ≥18 years. Specifically, two towns were chosen from each of the five macro-areas of Italy (Northwest, Northeast, Centre, South and Islands), based on data from the National Institute of Statistics (ISTAT) on the resident population at 1 January 2006(18). The towns selected were: (i) the most populous town of the area (‘large’) and (ii) a town randomly selected in the area from those with a total population of between 10 000 and 15 000 inhabitants (‘small’). The ten selected towns (with the numbers of inhabitants aged ≥18 years) were: Milan (1 125 691) and Ovada (10 256) in the Northwest; Bologna (328 593) and Riva del Garda (12 607) in the Northeast; Rome (2 140 153) and Terranuova Bracciolini (9889) in the Centre; Naples (783 859) and Atri (9281) in the South; Palermo (533 315) and Siniscola (9161) in the Islands. In each town the population was stratified according to sex and age (18–25 years, 26–45 years, 46–65 years, ≥66 years). Adults were then selected randomly from lists of residents of the selected towns, furnished by a society that manages telecommunication, in proportion to the size of each sex-by-age stratum, for a total of 1500 adults from each large town and 500 adults from each small town (overall total: 10 000 adults).
Data collection
A six-page questionnaire was sent in May 2008 to potential participants with a covering letter explaining its purpose and a stamped addressed envelope. A second letter with another copy of the questionnaire was sent 1 month later. To guarantee privacy, questionnaires were assigned a numeric code relative to the town and returned anonymously.
All potential participants were asked to fill in the self-administered questionnaire, providing information on the use of food supplements over the previous 2 years and on some determinants of usage. The definition of food supplements was that used in Directive 2002/46/EC(1):
foodstuffs the purpose of which is to supplement the normal diet and which are concentrated sources of nutrients or other substances with a nutritional or physiological effect, alone or in combination, marketed in dose form (such as capsules, pastilles, tablets, pills, ampoules of liquids etc) designed to be taken in measured small unit quantities
and additional clarification was also provided. The present study considered both regular and occasional food supplement users.
The information gathered related to sociodemographic and physical characteristics, lifestyle, health status and dietary habits. The use of eight categories of food supplements (products containing (i) vitamins and/or minerals, (ii) dietary fibre, (iii) fatty acids, (iv) antioxidants, (v) probiotics, (vi) botanicals and botanical extracts, products targeted to (vii) sportsmen or (viii) postmenopausal women) was also investigated, together with selected behavioural characteristics (see Table 1).
Table 1 General structure of the questionnaire

The reliability of the questionnaire was tested on a sample of 102 men and women(Reference Giammarioli, Boniglia and Carratù19). The data obtained relating to their characteristics, such as sociodemographic and physical data, lifestyle, dietary habits and most health characteristics, showed very good agreement between the two questionnaires (baseline and 1-month re-administration). The reliability of the information concerning the use of food supplements was satisfactory on the whole, and in any case similar to the values found in other studies.
Statistical analysis
The age brackets used for participants were the same as those used to stratify the population before the selection of the sample (18–25 years, 26–45 years, 46–65 years, ≥66 years). BMI was calculated from self-reported height and weight and categorized according to the WHO as underweight (BMI < 18·5 kg/m2), normal weight (BMI = 18·5–24·9 kg/m2), overweight (BMI = 25·0–29·9 kg/m2) or obese (BMI ≥ 30·0 kg/m2)(20). Alcohol consumption was categorized as never/occasionally, ≤2 glasses/d or >2 glasses/d, on the basis of the Italian Guidelines for Healthy Nutrition(21), which indicates a moderate consumption of alcohol (<2–3 glasses/d for men and 1–2 glasses/d for women). Consumption of fruit and vegetables was arbitrarily categorized as <2·5, ≥2·5 to ≤5 and >5 times/d, taking into consideration that many institutions(21–23) suggest an intake of five portions daily for this food category.
Differences between groups for frequency of food supplement use were assessed in the contingency tables using the Pearson χ 2 test. The effect of demographic and physical characteristics, lifestyle, dietary habits, health status and medical conditions on the use of food supplements was also evaluated by univariate and multivariate logistic regression. For any potential predictor variable, effect size was estimated by crude (univariate logistic regression) and adjusted (multivariate logistic regression) odds ratios with 95 % confidence intervals. Adjustment was performed according to two different models. In the first model only gender, age group and macro-area were considered as covariates in a fixed model; when evaluating the effect of area, odds ratios were also adjusted for education and income to avoid bias due to the possible differences between areas for these parameters.
In the second model, in addition to gender, age group and macro-area, which were forced into the model, other covariates were selected from among all the potential predictors considered in the analysis using a stepwise backward procedure. The effect of the same variables on the use of different categories of food supplements was also evaluated by multivariate logistic regression. Adjustment was performed considering gender, age group, macro-area and supplement categories as covariates in a fixed model. In this analysis it was not possible to take all potential predictors into account using a stepwise backward procedure, because of the relatively low number of users for the different categories of food supplements. All analyses were performed with the STATA statistical software package release 8·0.
Results
Sample characteristics and prevalence of food supplement use
Of the 10 000 adults selected, 1177 (11·8 %) were not traceable (deceased or moved) and 8823 (88·2 %) received the questionnaire. Of these, 1723 returned the questionnaire, corresponding to a response rate of 19·5 %. Participants’ characteristics are shown in Tables 2–4. Forty-nine per cent of participants were users of food supplements; only one participant failed to indicate use or non-use and was excluded from the study. The distribution of participants by town size is similar to that of the original population selected, as is the distribution by gender of the sample as a whole, although not for each individual town (data not shown). However, different response rates were observed by age and geographical area. In particular, more participants than expected were aged 45–65 years (43 % observed v. 30 % expected) and were living in the North of Italy (53 % observed v. 40 % expected). Participants generally had a medium–high level of education, an average income and were mainly either housewives/pensioners or public/private employees. Most participants were of normal weight or overweight, did not smoke, practised sports and declared a moderate consumption of alcohol. With regard to dietary habits, the study showed that some participants had a very low intake (never/occasionally) of some food categories, i.e. milk and yoghurt (17 % of participants), eggs (11 %), pulses (11 %) and fish (9 %). However, with the exception of fruit and vegetables, the intakes of different food categories were not included in the statistical analysis as, on the whole, the results seemed to be affected by a degree of under-reporting. With regard to medical conditions, most participants reported no specific disease and considered their health status good or fair, with no or low levels of stress. Among those who reported diseases, high blood pressure, anxiety/depression, high cholesterol and joint diseases were the main declared diseases; less frequently declared were osteoporosis, CVD and diabetes.
Table 2 Demographic and physical characteristics of the sample Italian adult population aged ≥18 years, 2008

†P value: statistical analysis by the χ 2 test between users and non-users.
Table 3 Lifestyle and dietary habits of the sample Italian adult population aged ≥18 years, 2008

†P value: statistical analysis by the χ 2 test between users and non-users.
Table 4 Health status and medical conditions of the sample Italian adult population aged ≥18 years, 2008

†P value: statistical analysis by the χ 2 test between users and non-users.
Characteristics of food supplement users and non-users
Tables 2–4 show also the characteristics of non-users and users of food supplements. As already noted, the percentage of food supplement users was 49 % (Table 2); there was a significantly higher prevalence of use among women than men and in those aged 18–45 years than in older age groups. The use of food supplements was significantly higher in the Northeast and Centre of Italy and in large towns; in participants with a lower BMI value in men but not in women; and in participants with higher levels of education and income. The highest percentage of consumers of food supplements was among students, followed by managers/professionals and public/private employees, while the lowest percentage was among housewives/pensioners and farmers/workers, with differences between the genders. All of these data were confirmed by crude OR, and by adjusted OR, except for BMI and income (Table 5a).
Table 5a Use of food supplements in relation to demographic and physical characteristics of the sample Italian adult population aged ≥18 years, 2008 (logistic regression)

Ref., reference category.
*P < 0·05, **P < 0·01.
†Adjusted for gender, age group and area; when evaluating the effect of area, OR was also adjusted for education and income.
Lifestyle and dietary habits also differed between users and non-users (Table 3). The use of food supplements was significantly more frequent in participants who practised sports and, in men but not in women, in current or non-smokers. No differences were observed in food supplement use with regard to alcohol or fruit and vegetable consumption, while a significant high prevalence was evident in regular consumers of wholemeal cereal-based foods. This general trend was confirmed for all variables by the values of crude OR and by adjusted OR, except for smoking status (Table 5b).
Table 5b Use of food supplements in relation to lifestyle and dietary habits of the sample Italian adult population aged ≥18 years, 2008 (logistic regression continued)

Ref., reference category.
*P < 0·05, **P < 0·01.
†Adjusted for gender, age group and area.
With regard to health status and medical conditions (Table 4), while the perception of health seemed not to affect food supplement use, participants reporting some level of stress used supplements more frequently than unstressed participants (P < 0·001). Furthermore, participants affected by hypertension or diabetes, on pharmacologic therapy, reported a significant lower use of food supplements than in those not affected by these diseases, with differences for gender. These data were confirmed by logistic regression analysis (Table 5c), which also highlighted a significantly higher consumption of food supplements in participants affected by cardiovascular or joint diseases who were not taking medication. Stepwise logistic regression confirmed all the associations described with the exception of age, occupation and medical conditions such as hypertension, diabetes and CVD. However, the trends for these variables were maintained (data not shown).
Table 5c Use of food supplements in relation to health status and medical conditions of the sample Italian adult population aged ≥18 years, 2008 (logistic regression continued)

Ref., reference category.
*P < 0·05, **P < 0·01.
†Adjusted for gender, age group and area.
Forty-four per cent of users (Fig. 1) used only one category of food supplement and 54 % were multiple users; in particular, 29 % used two different categories and 25 % three or more, with no significant differences between men and women. Vitamin and/or mineral supplements were the most commonly used (Fig. 2), by 61 % of users, followed by supplements with botanicals and botanical extracts (28 %), dietary fibre supplements (23 %), supplements for sports (22 %), probiotics (20 %), antioxidants (19 %), fatty acids (14 %) and supplements for postmenopausal women (11 %). Men and women differed significantly in the categories of food supplements used. In particular, women consumed more supplements with botanicals and botanical extracts, dietary fibre and probiotics than did men, while men used supplements for sports more than did women.

Fig. 1 Number of different categories of food supplements used ( $$$\raster="fx1"$$$, three or more;
$$$\raster="fx1"$$$, three or more;  $$$\raster="fx1"$$$, two;
$$$\raster="fx1"$$$, two;  $$$\raster="fx1"$$$, one;
$$$\raster="fx1"$$$, one;  $$$\raster="fx1"$$$, not indicated) in a sample Italian adult population aged ≥18 years, 2008. Results are relative to users (n users 527, 313 and 842 for women, men and total population, respectively) and expressed as percentages
$$$\raster="fx1"$$$, not indicated) in a sample Italian adult population aged ≥18 years, 2008. Results are relative to users (n users 527, 313 and 842 for women, men and total population, respectively) and expressed as percentages
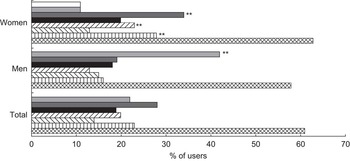
Fig. 2 Use of different categories of food supplements ( $$$\raster="fx1"$$$, for postmenopausal women;
$$$\raster="fx1"$$$, for postmenopausal women;  $$$\raster="fx1"$$$, for sports;
$$$\raster="fx1"$$$, for sports;  $$$\raster="fx1"$$$, botanicals;
$$$\raster="fx1"$$$, botanicals;  $$$\raster="fx1"$$$, antioxidants;
$$$\raster="fx1"$$$, antioxidants;  $$$\raster="fx1"$$$, probiotics;
$$$\raster="fx1"$$$, probiotics;  $$$\raster="fx1"$$$, fatty acids;
$$$\raster="fx1"$$$, fatty acids;  $$$\raster="fx1"$$$, dietary fibre;
$$$\raster="fx1"$$$, dietary fibre;  $$$\raster="fx1"$$$, vitamin and/or mineral) in a sample Italian adult population aged ≥18 years, 2008. Results are relative to users (n users 527, 313 and 842 for women, men and total population, respectively) and expressed as percentages. Percentage of users was significantly different between women and men: **P < 0·01
$$$\raster="fx1"$$$, vitamin and/or mineral) in a sample Italian adult population aged ≥18 years, 2008. Results are relative to users (n users 527, 313 and 842 for women, men and total population, respectively) and expressed as percentages. Percentage of users was significantly different between women and men: **P < 0·01
Table 6 shows the adjusted OR relative to the effect of the variables associated with the use of food supplements in the whole sample (gender, town size, education, sports practice, regular use of wholemeal cereal-based foods, self-assessed stress level) on the use of the different food supplement categories.
Table 6 Use of different categories of food supplements in relation to selected variables relative to demographic characteristics, lifestyle and dietary habits, and health status of the sample Italian adult population aged ≥18 years, 2008 (logistic regression performed on users)

Ref., reference category.
*P < 0·05, **P < 0·01.
†Adjusted for gender, age group, area and use of other supplements.
Female gender was significantly associated with the use of vitamin and/or mineral, dietary fibre, probiotic and botanical supplements, but not with use of supplements for sports, for which a negative association existed. A higher consumption of food supplements in large towns was confirmed only for fatty acids and for supplements for sports; instead, for probiotics and botanicals, the association was reversed. A higher education level (high school and/or degree) was confirmed as a significant determinant of usage for most supplements with the exception of probiotics, botanicals and supplements for postmenopausal women. Also sports practice was associated with the use of most supplement categories but showed a significant negative association for vitamins and/or minerals. The regular use of wholemeal cereal-based foods showed a significant positive association with probiotics and botanical supplements and a tendency for vitamins/minerals, dietary fibre and fatty acids. Finally, a low level of stress remained a determinant of usage for most food supplements (statistical significance for vitamin and/or mineral, dietary fibre, fatty acids and supplements for postmenopausal women, and a tendency for probiotics and botanicals), with the exception of antioxidants and supplements for sports (for the latter a negative association existed).
Regarding the information collected relative to behaviours, because the reliability of this section of the questionnaire was not totally satisfactory(Reference Giammarioli, Boniglia and Carratù19), we decided to consider these data with caution and not to show them in the current paper.
Discussion
Other surveys carried out in Europe(Reference Reinert, Rohrmann and Becker4–Reference Kiely, Flynn and Harrington13) have used different tools to assess food supplement use, such as mailed questionnaires and telephone or face-to-face interviews. Some studies focused specifically on the use of food supplements while others were wider-ranging surveys that also included questions regarding the use of food supplements, often within FFQ or food diaries or other methodologies. In addition, the definitions of supplement users and of food supplements, and the categories of food supplements taken into consideration, were very different. Finally, the statistical evaluation of the data also differed between studies. On account of the different methodologies used, is it not easy to compare the results of the different studies.
The response rate obtained in the current survey was about 20 %, which is lower than that obtained with mailed questionnaires in some European countries (Belgium 37 %, UK 71 %, France 84 %)(Reference Harrison, Holt and Pattison5, Reference Mullie, Guelinckx and Clarys7, Reference Touvier, Kesse and Volatier24), but similar to that obtained in USA (21 %) in the Vitamins and Lifestyle (VITAL) Study(Reference Satia-Abouta, Kristal and Patterson25, Reference Gunther, Patterson and Kristal26).
The prevalence of food supplement use in the population examined was 49 %, and significantly higher in women than in men. The prevalence of use reported in other European countries varies considerably: about 25–44 % in some studies carried out in Germany(Reference Reinert, Rohrmann and Becker4, Reference Beitz, Mensink and Hintzpeter11), 28 % in Ireland(Reference Kiely, Flynn and Harrington13), 31–39 % in Sweden(Reference Messerer, Johansson and Wolk8, Reference Nilsson, Trehn and Asplund12), 35 % in the UK(Reference Harrison, Holt and Pattison5, Reference McNaughton, Mishra and Paul6) and 59 % in Denmark(Reference Knudsen, Rasmussen and Haraldsdóttir10). However, in all cases a higher prevalence was found in women than in men, as in the present study.
The use of food supplements on the whole was significantly higher in the Northeast of Italy and in large towns compared with small towns. After adjustment for gender, age and area, the use was associated with higher education levels (high school or degree) and sports activities. These positive associations were found also in other European countries(Reference Reinert, Rohrmann and Becker4, Reference McNaughton, Mishra and Paul6, Reference Knudsen, Rasmussen and Haraldsdóttir10, Reference Nilsson, Trehn and Asplund12, Reference Marques-Vidal, Pécoud and Hayoz27) and in the USA(Reference Satia-Abouta, Kristal and Patterson25, Reference Gunther, Patterson and Kristal26, Reference Radimer, Bindewald and Hughes28).
An inverse association was instead observed for age, which became significant for older participants (≥66 years). A low consumption of food supplements by older individuals was not found in other surveys, in which the use of food supplements either increased with(Reference Reinert, Rohrmann and Becker4, Reference Harrison, Holt and Pattison5, Reference Messerer, Johansson and Wolk8, Reference Knudsen, Rasmussen and Haraldsdóttir10, Reference Kiely, Flynn and Harrington13, Reference Satia-Abouta, Kristal and Patterson25, Reference Marques-Vidal, Pécoud and Hayoz27, Reference Radimer, Bindewald and Hughes28) or was unrelated to age(Reference Nilsson, Trehn and Asplund12).
No associations were found with smoking status, consumption of alcohol or fruit and vegetable consumption. The absence of any statistical relationship between these variables and the use of dietary supplements was found in some studies but not in others(Reference Reinert, Rohrmann and Becker4–Reference McNaughton, Mishra and Paul6, Reference Messerer, Johansson and Wolk8, Reference Knudsen, Rasmussen and Haraldsdóttir10).
With respect to health status and medical conditions, after adjustment for gender, age and area, no association was found in the present study for self-assessed health status and the use of food supplements. In some studies carried out in Europe the self-perceived health status of participants was related significantly to the consumption of food supplements in different ways. In a survey conducted in the UK the use of any type of dietary supplements was positively associated with self-rated health(Reference Harrison, Holt and Pattison5), while in Sweden and in Denmark the use of food supplements was related to a poor self-perceived health status(Reference Messerer, Johansson and Wolk8, Reference Knudsen, Rasmussen and Haraldsdóttir10).
Furthermore, in the present study, food supplement use was directly associated with a low stress level and the presence of cardiovascular or joint diseases in participants who were not on medication. An inverse association was instead found between the use of food supplements and the presence of hypertension and diabetes in those taking medication for these pathologies. A possible explanation for the associations highlighted could be that individuals taking medication for hypertension and diabetes may not be inclined to add food supplements to their therapeutic schedule, while individuals suffering from cardiovascular or joint diseases who declared not to take medication may consider it useful to consume specific food supplements.
Very few studies have considered stress levels or specific pathologies and food supplement use and the results obtained were heterogeneous. A study conducted in a large cohort of French women(Reference Touvier, Kesse and Volatier24) showed that users of vitamin/mineral supplements more often perceived their work as stressful. In another study carried out in the UK(Reference Harrison, Holt and Pattison5) it was found that people with a history of angina, hypertension, diabetes, heart attack or stroke were less likely to be taking antioxidant, vitamin and/or mineral supplements than those who did not report these conditions. The use of fish-oil supplements was found to be positively associated with arthritis and inversely with angina, diabetes, heart attack or stroke. A study conducted in Switzerland(Reference Marques-Vidal, Pécoud and Hayoz27) showed that the use of vitamin/mineral supplements was positively related to anxiety/depression or osteoporosis and the use of other food supplements to anxiety/depression or arthritis. A third study on the use of complementary and alternative medicine remedies (vitamins, minerals or biological remedies such as fish oil, ginseng and coenzyme Q10) carried out in Sweden(Reference Nilsson, Trehn and Asplund12) showed that the use of these remedies was nearly identical in people with or without a medical history of hypertension, stroke, myocardial infarction or diabetes.
The majority of the present participants (54 %) used more than one category of food supplements, in agreement with the US population in the National Health and Nutrition Examination Survey (NHANES) carried out in 1999–2000, in which multiple users accounted for 53 % of the population examined(Reference Radimer, Bindewald and Hughes28), and with the National Complementary and Alternative Medicine Use Survey (NCAMUS) 2006, carried out in South Korea, where about 57 % of the participants consumed more than one supplement(Reference Ock, Hwang and Lee29). However, other studies have shown different situations; for example, in the population examined in the NHANES 2003–2006(Reference Bailey, Gahche and Lentino30) and in a sample of adults participating in the Danish Investigation on Iodine Intake and Thyroid Diseases 1997–1998(Reference Knudsen, Rasmussen and Haraldsdóttir10), most respondents reported taking only one food supplement, but these studies took into consideration a very limited period of consumption (the last month and the time of the survey, respectively). In the present population vitamin and/or mineral supplements were the most used category (61 %) followed by supplements with botanicals and botanical extracts (28 %). These findings are similar to those obtained in the NHANES 2003–2006, which showed that, of the three categories analysed, the prevalence of use of multi-vitamin/multi-mineral supplements was highest, followed by the use of botanical supplements(Reference Bailey, Gahche and Lentino30). Other studies have highlighted the prevailing consumption of vitamin/mineral supplements over other categories(Reference Reinert, Rohrmann and Becker4, Reference Knudsen, Rasmussen and Haraldsdóttir10, Reference Kiely, Flynn and Harrington13), but different patterns also exist. For example, the supplement most commonly reported to be used by South Korean adults(Reference Ock, Hwang and Lee29) was ginseng, and in the 1946 British Birth Cohort(Reference McNaughton, Mishra and Paul6) it was fish-oil supplements.
To evaluate if the determinants of usage differed for the different categories of food supplements, it was decided to calculate, on the whole sample of users, the OR adjusted considering as covariates not only gender, age group and area but also the different categories of supplements, to take into account the effect of the simultaneous use of different supplements. Few studies have been completed to detect the determinants of usage for specific categories of food supplements and data were limited in most cases to vitamin/mineral and herbal supplements. Some of the associations shown in the present study for vitamin and/or mineral supplements were also found in other studies carried out in the USA and Europe, in particular the positive association with female gender and a higher education level(Reference Reinert, Rohrmann and Becker4, Reference de Jong, Ocké and Branderhorst9, Reference Touvier, Kesse and Volatier24, Reference Satia-Abouta, Kristal and Patterson25, Reference Marques-Vidal, Pécoud and Hayoz27, Reference Radimer, Bindewald and Hughes28, Reference Balluz, Kieszak and Philen31, Reference Rock32). The positive association between physical activity and the use of this type of supplement found in some papers(Reference Reinert, Rohrmann and Becker4, Reference Touvier, Kesse and Volatier24, Reference Marques-Vidal, Pécoud and Hayoz27, Reference Radimer, Bindewald and Hughes28, Reference Rock32) was reversed in our study. In our study users of supplements with botanicals and botanical extracts were more likely to be women; this finding is in agreement with other studies conducted in different countries(Reference Messerer, Johansson and Wolk8, Reference Gunther, Patterson and Kristal26, Reference Harnack, Rydell and Stang33–Reference Harrison, Holt and Pattison36). The positive relationship between increased use of this type of supplement and physical activity(Reference Messerer, Johansson and Wolk8, Reference Gunther, Patterson and Kristal26, Reference Kennedy34, Reference Harrison, Holt and Pattison36) found in some studies was not found in our population.
There is very little information in the literature regarding the other categories of food supplements considered here. For fatty acid supplements our results are somewhat similar to those of a study performed in Norway on the use of cod-liver oil supplements by women(Reference Brustadt, Braaten and Lund37). As in our sample, the use of these supplements increased with higher education levels and physical activity. The positive association between the use of probiotics and female gender found in the present study was also found in a study carried out in South Korea(Reference Ock, Hwang and Lee29). With regard to antioxidants, some of the associations highlighted here, such as the higher use with higher education levels and physical activity, were also reported in specific clinical trials(Reference Shikany, Patterson and Agurs-Collins38, Reference Neuhouser, Kristal and Patterson39). Finally, to our knowledge, no data regarding the determinants of use of dietary fibre supplements or supplements for sports or postmenopausal women in general populations are present in the literature.
Our study has some limitations. The principal limit is that, due to the relatively low response rate (about 20 %), the study sample is not representative of the general population. Indeed, the adults who agreed to participate in our survey had a higher level of education than the general population (30 % graduates v. 11 % )(40) and may be more health-conscious than the non-participants, which would lead to an overestimation of the true prevalence of food supplement use. Finally, a high proportion of participants (43 %) came from a single age group; nevertheless, adjustment for age did not modify the effects described by univariate analyses. For these reasons the results obtained should be regarded as preliminary to further studies introducing strategies to increase the response rate.
Despite these limitations, the present study provided important information for surveillance purposes, given the paucity of data on this topic in Italy. In particular, the study showed that gender, town size, education level, sports practice, regular use of wholemeal cereal-based foods and the presence of low stress levels, although associated with an increased use of food supplements, are not determinants of usage for all categories of supplements. These results support previous observations that the associations between demographic, dietary and lifestyle characteristics, and the use of different categories of food supplements, differ according to products and cannot be accounted for simply by dichotomizing individuals as users or non-users(Reference de Jong, Ocké and Branderhorst9, Reference Hoggatt, Bernstein and Reynolds14–Reference Kim, Lee and Shin17).
To confirm these findings, it would be desirable for other research to be carried out on the same topic; however, these preliminary data are useful for conducting more focused studies and for the national authorities to develop policies regarding the use of food supplements.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sector. None of the authors has any conflicts of interest. Ethical approval was not required. S.G. and E.S. were involved in study design, data management, and manuscript design and writing. C.F. was involved in statistical analysis and interpretation, and manuscript design and writing. C.B., B.C. and M.M. were involved in data analysis and data interpretation. M.C. was involved in acquiring the data. All co-authors have reviewed and approved the paper.










